Download to read offline


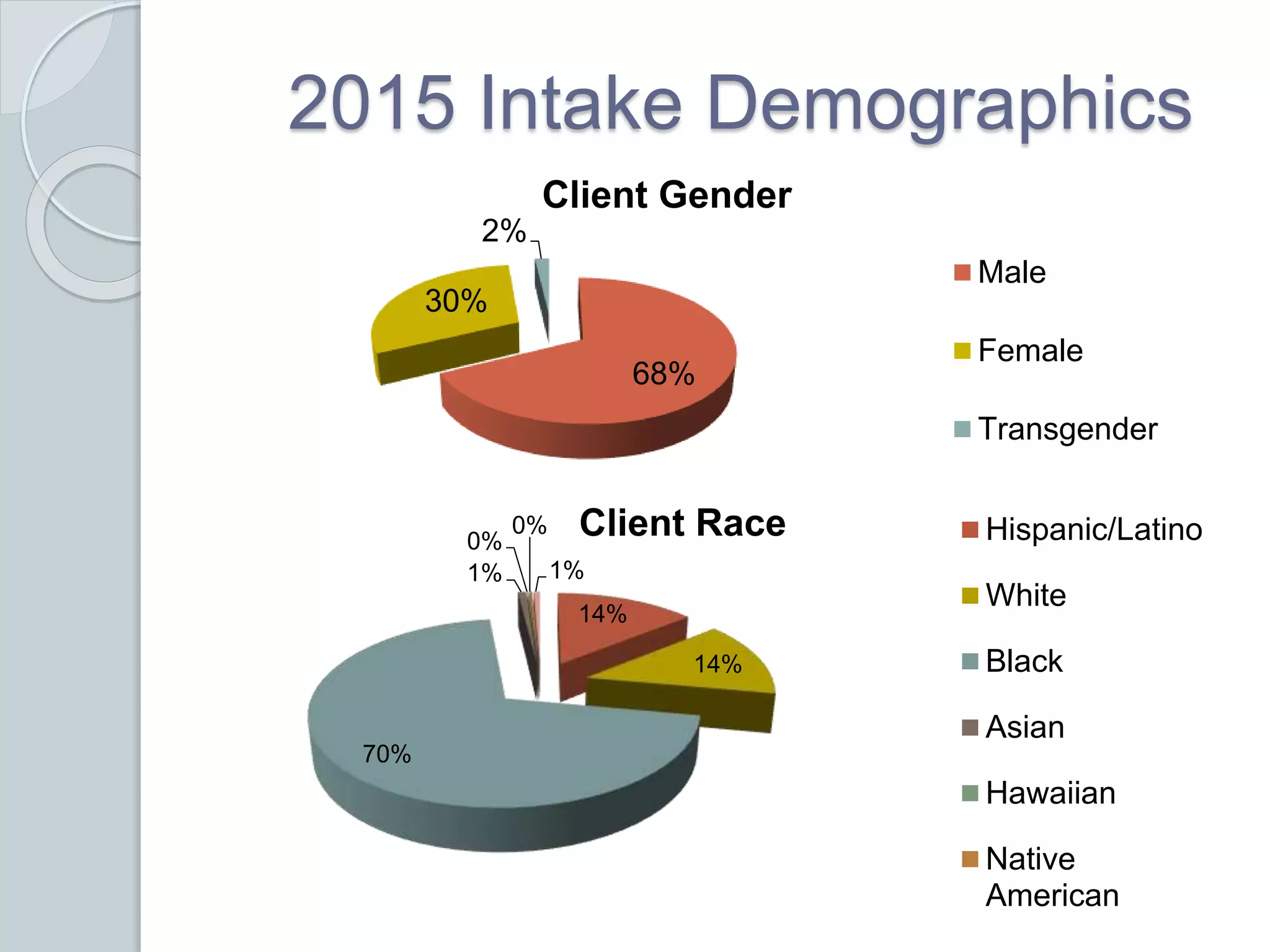
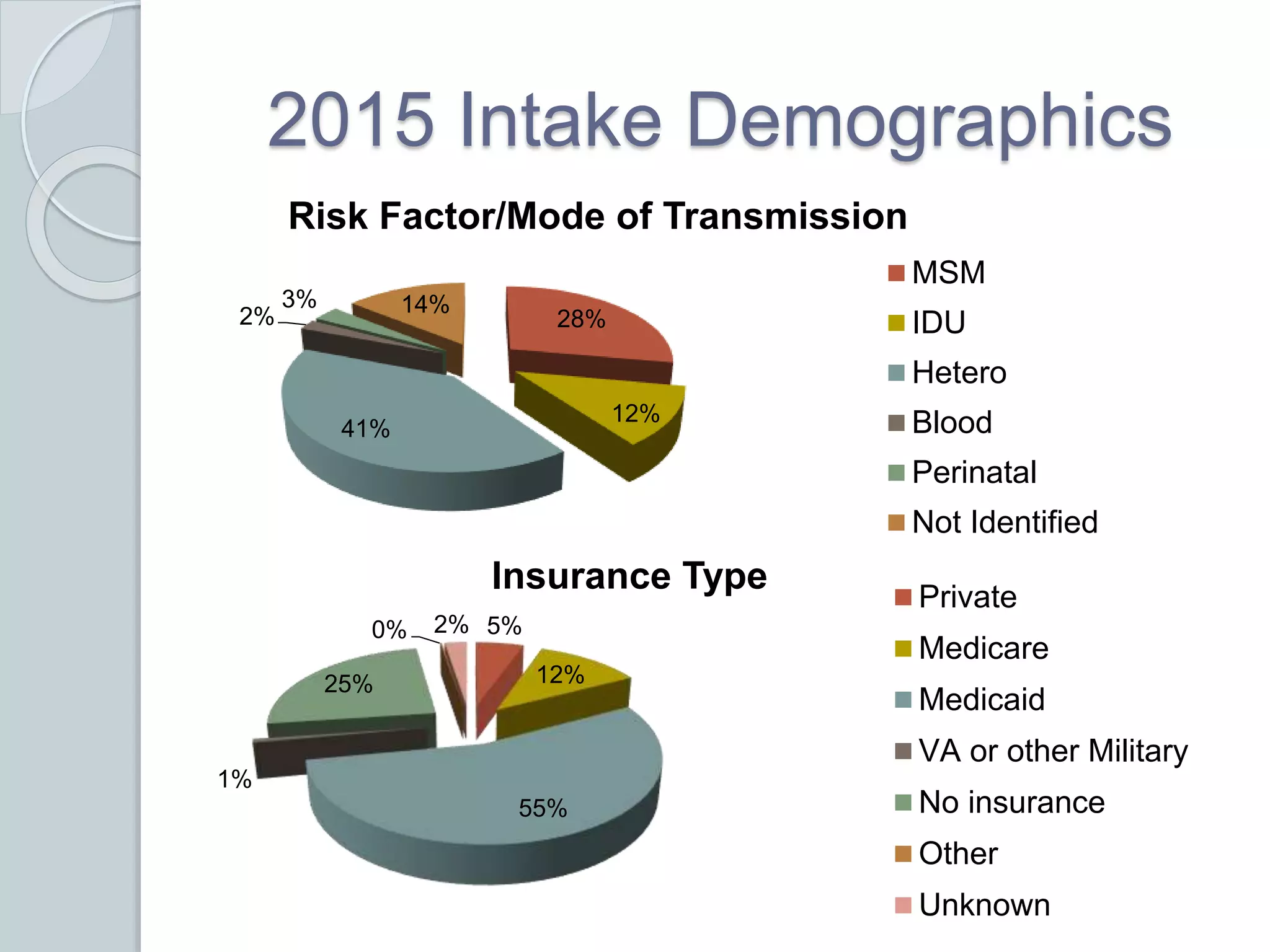
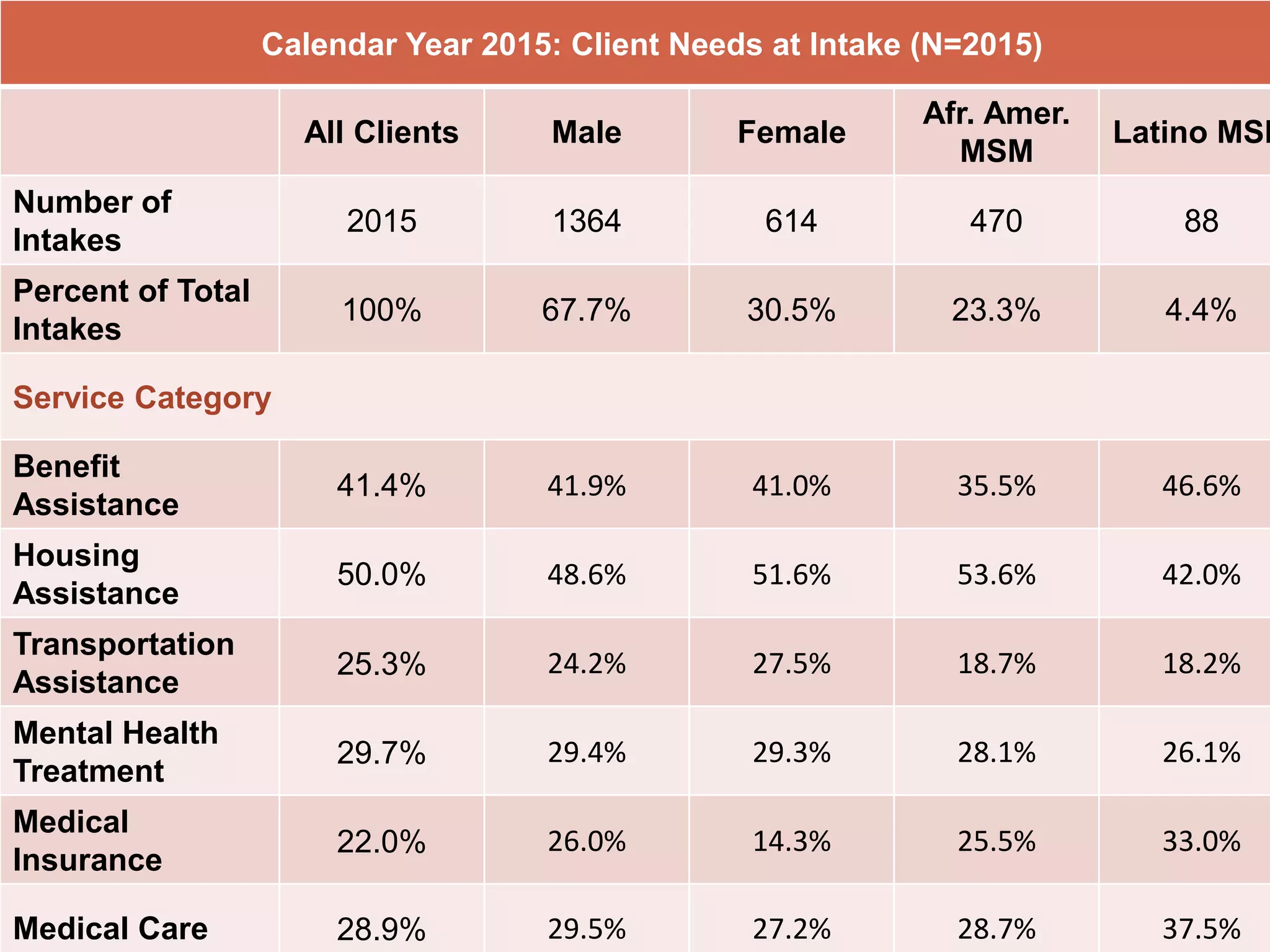
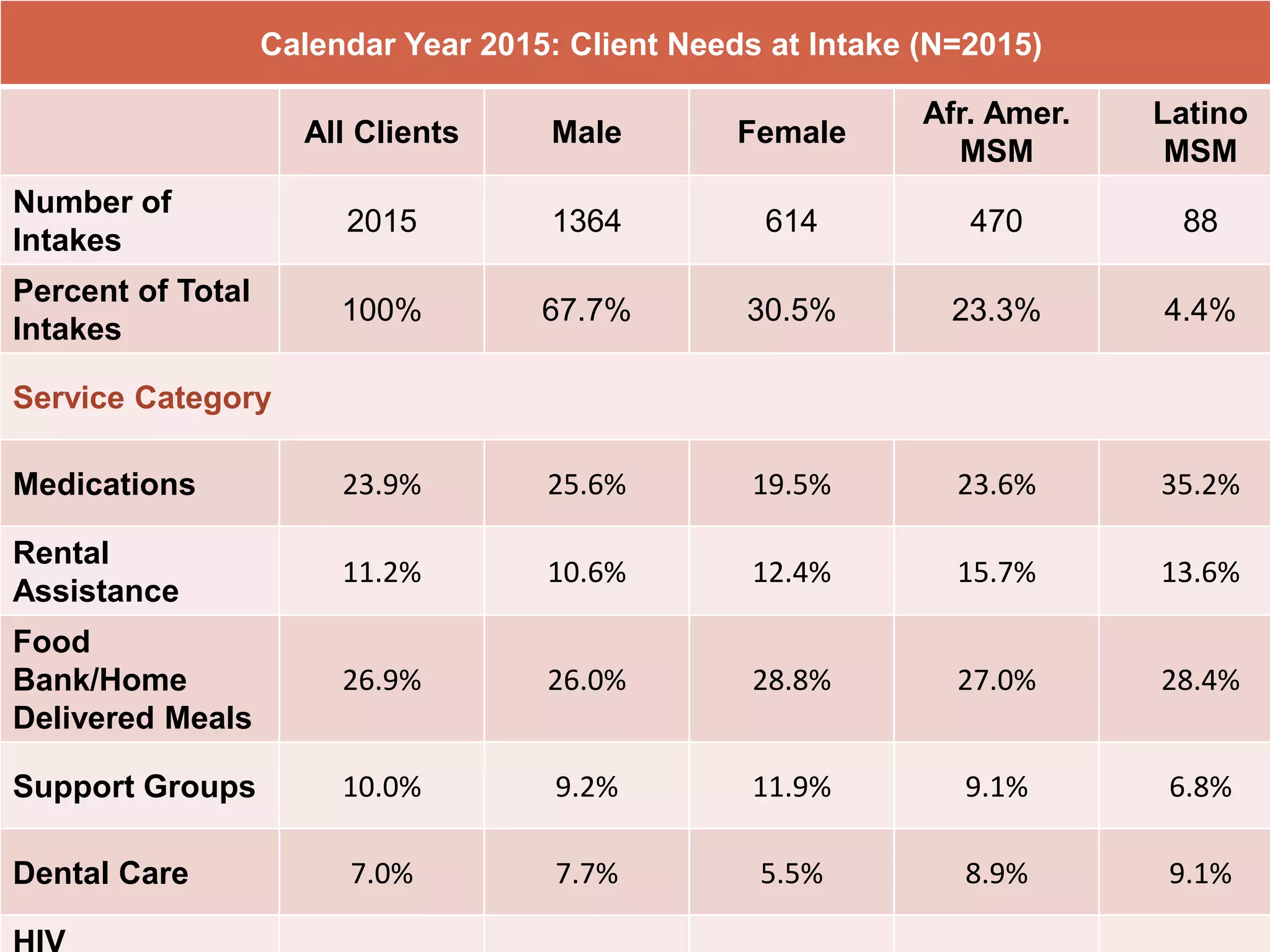
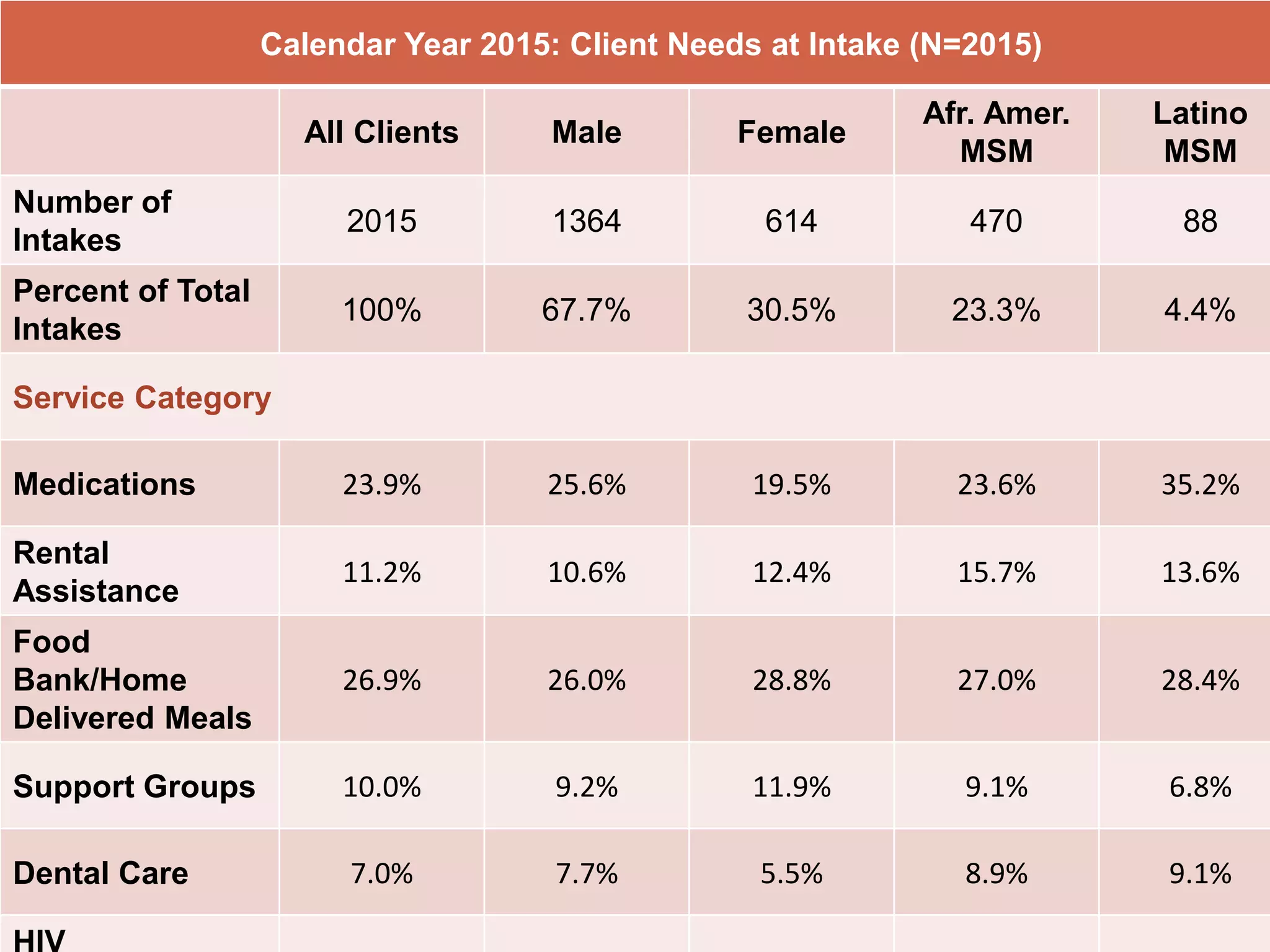



The Philadelphia Department of Public Health held a meeting on April 14, 2016, focusing on medical case management (MCM) services for HIV/AIDS, which aim to improve health outcomes through client-centered activities. Key activities include initial assessments, care plan development, and ongoing client monitoring, with an emphasis on quality improvement initiatives to enhance service delivery. The meeting also highlighted funding details and demographic information of clients benefitting from these services in the region.





























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)





