A practical aproach
•
4 likes•6,936 views

This document discusses vestibulitis, a condition characterized by focal erythema and sometimes erosion at the junction of the hymen and vestibule. Women with vestibulitis experience pain with sexual intercourse or tampon insertion due to tenderness in the vestibular area. A careful examination looking for erythema or fissures at the hymenal-vestibular junction can help diagnose vestibulitis. Medical therapies for vestibulitis are generally ineffective as the condition renders the vestibular epithelium more susceptible to damage.

More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (11)
More from Luis Carlos Murillo Valencia
More from Luis Carlos Murillo Valencia (20)
Recently uploaded
Recently uploaded (20)
A practical aproach
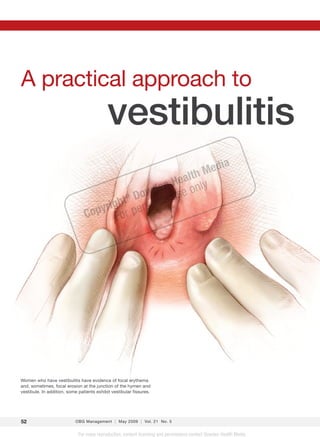
- 1. A practical approach to vestibulitis ed ia a lt hM e n He only owd se ht D rsonal u ® ig Copyr For pe Women who have vestibulitis have evidence of focal erythema and, sometimes, focal erosion at the junction of the hymen and vestibule. In addition, some patients exhibit vestibular fissures. 52 OBG Management | May 2009 | Vol. 21 No. 5 For mass reproduction, content licensing and permissions contact Dowden Health Media.
- 2. and vulvodynia Draw a few basic distinctions and apply simple strategies to aid your diagnosis and management of these all-too-common conditions CASE David Soper, MD No relief, despite multiple therapies Dr. Soper is Professor of Obstetrics and Gynecology and Vice Chairman A 20-year-old woman is referred to your practice for evalu- for Clinical Affairs at the Medical ation of persistent dyspareunia. She describes the pain as University of South Carolina in “excruciating” and reports that it occurs with attempted IN THIS Charleston, SC. ARTICLE penile insertion. The author reports no financial Her symptoms began 1 year ago when she noted some Cyclic vulvovaginitis relationships relevant to this article. postcoital soreness at the introitus, as well as external dys- can lead to uria. The symptoms have become so pronounced that she dyspareunia now avoids sexual intercourse altogether. She experiences page 54 similar pain when she inserts a tampon, wears tight jeans, or rides a bicycle. She has no history of recurrent vaginitis. One, simple question So far, she has tried, sequentially, topical steroids, vitamin D ointment, topical gabapentin, and oral amitripty- can aid the diagnosis line—without improvement. of vestibulitis What is the differential diagnosis? And what can you page 56 do to ease her pain? Essential vulvodynia responds to medical A lthough vulvar pain has many causes, women who have a chronic vulvar pain syndrome gen- therapy MOLLY BORMAN FOR OBG MANAGEMENT erally fall into one of three diagnostic categories page 60 (i.e., McKay’s patterns): • cyclic vulvovaginal candidiasis ›› SHARE YOUR COMMENTS How would you diagnose and • vestibulitis manage the patient described on • essential vulvodynia.1 this page? Drop us a line and let In this case, the diagnosis is vestibulitis, which is us know. marked by focal erythema and, in some cases, focal ero- E-MAIL obg@dowdenhealth.com sion at the junction of the hymen and vestibule. Clinical FAX 201-391-2778 findings in women who have vestibulitis are often subtle, but can be detected with careful examination. CONTINUED ON PA GE 54 o b g m a n a ge me n t .c om Vol. 21 No. 5 | May 2009 | OBG Management 53
- 3. Vestibulitis and vulvodynia TABLE How vulvar pain Anatomy of the vulva is classified The first step in adopting a practical approach to vulvar pain is developing familiarity with Generalized vulvar anatomy. I find it useful to divide the Involvement of the entire vulva vulvovaginal anatomy into three discrete areas: • Provoked (sexual contact, nonsexual contact, or both) • vulva • Unprovoked (spontaneous) • vestibule • Mixed (provoked and unprovoked) • vagina. The vulvar integument is keratinized and Localized Involvement of a portion, or component, contains hair follicles and apocrine glands. of the vulva, e.g., vestibulodynia, clitorodynia, The epithelium of the vestibule, on the other hemivulvodynia, etc. hand, is similar to the buccal mucosa: non- • Provoked (sexual contact, nonsexual keratinized and usually moist, with no ad- contact, or both) nexal structures. This highly innervated area • Unprovoked extends from the hymenal ring to Hart’s line • Mixed (provoked or unprovoked) (FIGURE 1) and is the primary site of concern International Society for the Study of Vulvar Diseases13 in women who have a vulvar pain syndrome. The vagina begins at the hymenal ring and extends proximally to the cervix. The FIGURE 1Physical findings may vagina is uniformly normal in patients who be subtle complain of chronic vulvar pain unless yeast vaginitis is one of the causes. Areas of erythema Cyclic vulvovaginitis can lead to dyspareunia When they relapse, Women who have cyclic vulvovaginal can- women who have didiasis initially complain of symptoms of cyclic vulvovaginitis yeast vaginitis, e.g., vulvovaginal itching and tend to experience a cheesy white vaginal discharge. Most wom- en experience infrequent episodes of yeast mild irritative Hart’s line vaginitis, but those who have cyclic candidi- symptoms and asis relapse after a short course of topical or a new complaint of When vestibulitis is suspected, look for areas of systemic antifungal therapy. When they re- entry dyspareunia erythema or fissuring at the junction of the hymen lapse, they tend to experience mild irritative and vestibule and explore the entire vestibule out to Hart’s line. symptoms and de novo entry dyspareunia. PHOTO COURTESY OF DAVID SOPER, MD Many of these women will have been treated with intermittent antifungal medica- tion and antibiotics because their clinician This article outlines the diagnosis and assumed that a bacterial infection was pres- management of vestibulitis and essential ent when the antifungal therapy did not solve vulvodynia, including a basic classification the problem. Another challenge in evaluating of vulvar pain (TABLE). In the process, it also these women is the inability of point-of-care sheds light on the tricky diagnosis of cyclic vul- testing to guide the diagnosis—or the omis- vovaginal candidiasis, which can provoke ves- sion of such testing altogether. tibulitis in some cases. The basic profile of these patients re- A careful history, focused physical exami- mains the same, however: relapsing introital nation of the vulva and vagina, and microsco- symptoms that are relatively mild but lead to py of the vaginal secretions are the foundation worsening entry dyspareunia, a sign of vestib- of diagnosis of any vulvar pain syndrome. ulitis. The patient may also report postcoital 54 OBG Management | May 2009 | Vol. 21 No. 5
- 4. Vestibulitis and vulvodynia topical or systemic antimicrobial. When she An overlooked and underestimated affliction returns, vulvovaginal candidiasis can usually be diagnosed by microscopy and confirmed As an official entity, the term vulvodynia has been around only 25 by vaginal yeast culture to rule out non-albi- years. The International Society for the Study of Vulvar Diseases cans Candida. Patients who have recurrent (ISSVD) defined vulvodynia in 1984 as chronic vulvar discomfort, not- vulvovaginal candidiasis tend to flare pre- ing that it is characterized in particular by the patient’s complaint of menstrually. burning, stinging, irritation, or rawness. Vulvodynia didn’t originate in 1984, of course. But its definition Treatment may be lengthy was an important first step in identifying a clinical entity that had Treatment of cyclic vulvovaginal candidiasis long been ignored by clinicians, primarily because of their inability to involves an initial course of oral fluconazole determine a cause, establish a diagnosis, and recommend a specific course of therapy. In addition, the magnitude of the problem was (150 mg every 3 days for three doses), fol- woefully underestimated. lowed by suppressive therapy with weekly flu- A population-based study of 4,915 women in Boston found that conazole (150 mg).2 This treatment is effective 16% of respondents reported either chronic vulvar burning or pain in more than 90% of cases, easing the cyclicity with contact.11 Hispanic women were more likely than Caucasian and of the patient’s symptoms. However, she may African-American women to acknowledge such a complaint. be left with some residual vestibulitis and dis- Similarly, Goetsch found that 15% of patients in her gynecologic comfort with coitus, which may take as long as practice had vestibular pain and tenderness on examination.12 2 months to resolve. Biweekly application of a topical steroid of modest strength may help, such as triamcinalone 0.1% ointment. soreness and burning after micturition when the urine drops onto the vestibule (“splash dysuria”). These symptoms may reflect the Vestibulitis is most common presence of small vestibular fissures. among young women Women who have vestibulitis tend to be pre- Young women Evaluation can be tricky menopausal and young—typically, in their who have vestibulitis The key to evaluation of a patient with these 20s. They usually complain of worsening tend to complain complaints is to schedule her appointment pain with coitus, as well as pain with tampon of progressively once she has been off therapy for at least 2 insertion and tenderness when riding a bike weeks and has not used any intravaginal or wearing tight jeans, suggesting that touch worsening pain with medication during that interval. This drug to the vestibule provokes the pain. coitus as well as holiday serves two functions: Despite these other symptoms, however, other symptoms that • It eliminates adverse reactions to medi- it is the inability to have vaginal sexual inter- suggest that touch cations from the differential diagnosis. course that usually brings the patient to the to the vestibule • It allows adequate evaluation of vaginal physician. I generally ask a simple question: provokes the pain secretions, including a reliable vaginal “If you did not engage in sexual intercourse, culture for Candida species. would you be normal?” In other words, would During this initial encounter, the exam she avoid the pain if she avoided touch to the may well be normal. Ask the patient to grade vestibule? Patients who have vestibulitis in- her vulvovaginal symptoms on a scale of 0 to evitably answer, “Yes!” 10, with 10 representing the worst symptoms experienced and 0 being a complete lack of “The eye doesn’t see what symptoms. Many patients at the initial en- the mind doesn’t know” counter will grade their symptoms as mini- This caveat is important as you examine the mal, in the range of 2 to 3 out of 10. patient (FIGURE 1, page 54). When vestibulitis If the exam is normal, ask the patient is present, clinical findings are often subtle; to return for a repeat evaluation when her careful examination, however, can elicit the symptoms reach 8 or greater on the 10-point source of the tenderness. Inspect the vulvar scale, and instruct her not to self-treat with a vestibule carefully circumferentially, and 56 OBG Management | May 2009 | Vol. 21 No. 5
- 5. Vestibulitis and vulvodynia Vestibulitis and vulvodynia Improving exert pressure at the junction of the hymen and contraceptive vestibule using a moistened cotton swab. As I mentioned earlier, women who have vestibulitis have evidence of focal erythema and, success: sometimes, focal erosion at the junction of the hymen and vestibule. They also experience ex- quisite tenderness as the cotton swab presses against this junction, with the pain most intense Facilitating choice of in the 3 to 9 o’clock region. Yeast vaginitis should be ruled out by microscopy and yeast culture. appropriate and Most patients have avoided coitus for some time before they see a physician, so vestibular acceptable contraceptive fissures may not be obvious. The diagnosis of vestibulitis can be based on Friedrich’s criteria: methods • severe pain at the vestibule upon touch or attempted vaginal entry 1.0 • tenderness to pressure localized within the CME vulvar vestibule CREDIT • physical findings confined to vestibular ery- OVERVIEW FREE Nonuse and misuse of contraception result in the vast majority of unplanned pregnancies in the United States. The selection of appropriate and acceptable contraceptive methods can improve adherence. This supplement examines 1.0 CME CREDIT thema of various degrees.3 the factors that contribute to inconsistent contraceptive behavior and offers S U P P L E M E N T TO strategies for assisting patients in the selection and use of methods that best suit their individual needs and preferences. EDUCATIONAL OBJECTIVES Medical therapy is ineffective At the conclusion of this activity, participants should be better able to: ❚ Discuss factors associated with nonuse/misuse of contraception and implications for improving adherence ❚ Review the latest safety, efficacy, tolerability, and sustainability data for current and emerging contraceptive methods ❚ Develop strategies for counseling patients about appropriate and acceptable contraceptive methods Vestibulitis is a disease that renders the vestibu- TARGET AUDIENCE JANUARY 2009 This activity has been designed to meet the educational needs of obstetri- cians, gynecologists, and other health care specialists involved in the man- agement of patients who may benefit from contraception. lar epithelium less resilient and more suscep- ACCREDITATION STATEMENT SciMed is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. tible to fissures upon contact. For this reason, IMPROVING CREDIT DESIGNATION medical therapy is ineffective. SciMed designates this educational activity for a maximum of 1.0 AMA PRA Category 1 Credit™. Physicians should only claim credit commensurate with CONTRACEPTIVE the extent of their participation in the activity. RELEASE DATE: January 6, 2009 EXPIRATION DATE: January 6, 2010 ESTIMATED TIME TO COMPLETE ACTIVITY: 1.0 hour DISCLOSURE AND RESOLUTION OF CONFLICTS OF INTEREST SUCCESS: Although a 6-week trial of a topical steroid SciMed assesses conflicts of interest with its faculty and all individuals who are in a position to control the content of CME activities. All relevant conflicts of interest that are identified are resolved by SciMed to ensure fair balance and scientific objectivity. Facilitating choice of (triamcinalone 0.1% or desoximetasone 0.25% When asked to report any potential conflict(s) of interest, faculty reported the following: appropriate and acceptable ointment twice daily) is commonly prescribed, it Anita L. Nelson, MD ❚ GRANTS/RESEARCH SUPPORT: Barr Pharmaceuticals, Inc. (Duramed Pharma- contraceptive methods ceuticals, Inc.), Bayer HealthCare Pharmaceuticals (Berlex, Inc.), Wyeth Phar- maceuticals ❚ SPEAKERS BUREAU/HONORARIA: Barr Pharmaceuticals, Inc., Bayer HealthCare is rare for a patient to have a response sufficient Pharmaceuticals, Merck & Co., Inc., Schering-Plough Corporation (Organon BioSciences), Ther-Rx Corporation, Wyeth Pharmaceuticals ❚ CONSULTANT/ADVISORY BOARD: Barr Pharmaceuticals, Inc., Bayer Health- Care Pharmaceuticals, Ortho-McNeil Pharmaceutical, Inc., Wyeth Pharma- › ANITA L. NELSON, MD Professor, Department of Obstetrics and Gynecology to restore pain-free coitus.4 ceuticals David Geffen School of Medicine at UCLA Andrew M. Kaunitz, MD ❚ SPEAKERS BUREAU/HONORARIA: Barr Pharmaceuticals, Inc., Bayer HealthCare Pharmaceuticals, Johnson and Johnson (Ortho-McNeil Pharmaceutical, University of California, Los Angeles Los Angeles, California Some patients are adept at applying topi- Inc.), Merck & Co., Inc., Noven Pharmaceuticals, Inc., Organon BioSciences ❚ CONSULTANT/ADVISORY BOARD: Barr Pharmaceuticals, Inc., Bayer Health- Care Pharmaceuticals, Johnson and Johnson (Ortho-McNeil Pharmaceutical, Inc.), Merck & Co., Inc., Noven Pharmaceuticals, Inc., Organon BioSciences › ANDREW M. KAUNITZ, MD cal 5% xylocaine ointment to the vestibule 15 to ❚ STOCKHOLDER: sanofi-aventis Professor and Associate Chair All SciMed personnel involved in the development of content for this activity have no relevant conflicts to report. The materials for this activity were peer reviewed by Ellen Miller, MD, Clinical Department of Obstetrics and Gynecology University of Florida College of Medicine 30 minutes before coitus to ease the discomfort Jacksonville, Florida Associate Professor of Medicine, Albert Einstein College of Medicine. Dr. Miller has no relevant conflicts to report. INSTRUCTIONS FOR OBTAINING CME CREDIT associated with intercourse. Another alterna- There are no fees for participating in and receiving CME credit for this activity. To obtain CME credit for participating in this activity during the period Janu- ary 6, 2009 through January 6, 2010, participants must (1) read the educa- tional objectives and disclosure statements, (2) study the educational activity, tive is injection of interferon into the vestibule, (3) complete the posttest by recording the best answer to each question, (4) complete the evaluation form, and (5) mail or fax the evaluation form with answer key to SciMed per the instructions on the form. A statement of credit will be issued only upon receipt of a complete activ- which can limit the percentage of patients who ity evaluation form and a completed posttest with a score of 80% or better. Supported by an educational grant from Sponsored by Participants will be mailed a certificate or statement of credit within 4 to 6 weeks. DISCLAIMER require vestibulectomy by almost 50%. Howev- er, interferon must be injected into the vestibule The opinions or views expressed in this CME activity are those of the present- ers and do not necessarily reflect the opinions or recommendations of SciMed or the commercial supporter. Participants should critically appraise the infor- mation presented and are encouraged to consult appropriate resources for This supplement was submitted by SciMed and has been edited and peer three times weekly for 4 weeks.5 Side effects in- information surrounding any product, device, or procedure mentioned. reviewed by OBG Management. COPYRIGHT © 2009 DOWDEN HEALTH MEDIA clude the pain of the needlestick and systemic fever and flu-like illness from the interferon. This supplement was sponsored by Vestibulectomy is the SciMed and supported by an educational treatment of choice grant from Schering-Plough. Multiple studies suggest 61% to 94% improve- ment or cure after vestibulectomy.6 A key pre- dictor of surgical failure is constant vulvar pain SUPPLEMENT TO in addition to pain with coitus.7 Such patients should probably be managed by an expert. 58 OBG Management | May 2009 | Vol. 21 No. 5
- 6. PELVIC SURGERY DVD SERIES FIGURE 2 Excision of the vestibule now available THANK YOU FOR ORDERING FROM OWN ONE OR Vestibulectomy involves removal of the entire vestibule except the part just lateral to the urethral meatus. ALL 10 SETS IN THE SERIES PHOTO COURTESY OF DAVID SOPER, MD Review sample clips from these remarkable state-of-the-art DVDs that utilize detailed surgical drawings, extensive video footage of cadaver Before deciding on vestibulectomy, confirm dissections and live surgical demonstrations to that the patient has had persistent symptoms for teach a variety of pelvic surgical procedures. more than 6 months. The reason? Spontaneous More than 15 renowned specialists narrate, remission does sometimes occur within the first covering indications, techniques and how to avoid 6 months of vestibulitis. complications of a variety of pelvic reconstructive In the OR, after induction of anesthesia, ap- procedures. More than 20 hours of video footage. ply downward and lateral pressure to the pos- terior fourchette to bring small fissures to light. DVD Titles: Vestibulectomy entails removal of the hymen • Sling Procedures from A to Z and vestibular skin out to Hart’s line. This usually means removal of all of the vestibule except the • Vaginal Correction of Anterior and Posterior Vaginal part just lateral to the urethral meatus (FIGURE 2). Wall Prolapse With and Without Vaginal Hysterectomy Once this tissue is removed, mobilize the • Techniques to Correct Enterocele and Vaginal Vault vaginal epithelium, as in posterior colporrha- Prolapse phy, and advance it to cover the surgical defect. • Cystourethroscopy and Urologic Surgery for the Gynecologist Postoperative immobilization is required After surgery, the patient should expect to be • Reconstructive Procedures on the Lower Urinary Tract somewhat immobilized for 2 weeks and to re- • Retropubic Procedures quire narcotic analgesia during this time. Heal- • Challenging Cases in Urology and Urogynecology ing should be apparent by 6 postoperative • Evaluation of Women With Lower Urinary Tract weeks, but the suture line at the introitus may Symptoms With and Without Pelvic Organ Prolapse— still be slightly tender. I usually recommend that Including Urodynamic Testing the patient avoid coitus until the 3-month post- operative visit. At this visit, the introitus should • Surgical Management of Congenital, Acquired and no longer be tender. If this is the case, the patient Iatrogenic Lesions of the Vagina and Urethra can be given the green light for coitus. • Surgery for Posterior Pelvic Floor Abnormalities FOR A In older women, look for genital atrophy LIMITED TIME, Postmenopausal women are remaining sexually RECEIVE A FREE DVD active in ever-increasing numbers. When dys- WITH YOUR pareunia occurs in this population, the cause is ORDER For details and to purchase, visit May 2009 | OBG Management 59 www.obgmanagement.com/pelvicdvds
- 7. Vestibulitis and vulvodynia usually genital atrophy. Long-term treatment Less is more in the pharmacotherapeutic with systemic or topical estrogen will usually management of essential vulvodynia. Women ease coital pain. Surgery is not a mainstay of who do not respond to a lower dosage tend treatment of dyspareunia in postmenopaus- not to respond to a higher one, either. al women. (For more on this population, see Another option is gabapentin. It usually “Postmenopausal dyspareunia: A problem is administered orally but was recently stud- for the 21st century,” by Alan Altman, MD, in ied in a topical formulation, both of which the March 2009 issue of OBG Management appear to be effective.9,10 at www.obgmanagement.com.) Counsel the patient that improvement, not cure, is the therapeutic goal with these drugs and that her response will be gradual, Essential vulvodynia is more with improvement usually noticed after 2 common among older women weeks of therapy, continuing until her 6- Women who have essential (dysesthetic) week revisit. At that time, the dosage can be vulvodynia tend to be older and postmeno- maintained or increased, depending on the pausal, although premenopausal women are patient’s response. If the patient is happy with sometimes affected. These women complain that response, treatment should continue for of chronic, unremitting, diffuse vulvar burn- 4 months, at which point she can be weaned ing that is usually not limited to the vestibule. from therapy. Relapse is uncommon. They may have similar symptoms in the re- gion of the urethra and rectum. In general, CASE: OUTCOME dyspareunia is not a major problem. Upon examination, the patient exhibits focal In women who have essential vulvo- erythema at the junction of the hymen and dynia, the pelvic examination is absolutely vestibule. Palpation of these areas with a normal other than the presence of mild geni- moist cotton swab causes extreme tender- tal atrophy in the postmenopausal patient. ness, recreating the patient’s introital pain. When the patient There is no evidence of provoked tenderness Microscopy of the vaginal secretions is nor- has essential and no focal erythema or erosion. mal, and a vaginal yeast culture is negative. Because she is an excellent candidate for vulvodynia, the pelvic exam is absolutely Treatment is medical vestibulectomy, the patient undergoes resec- Women who have essential vulvodynia are tion of the vulvar vestibule from the hymenal normal except not candidates for surgery. Optimal treatment ring to Hart’s line, from the 1 o’clock to 11 for the presence of of this neuralgia entails the use of low-dosage o’clock positions, and recovers slowly. mild genital atrophy amitriptyline (25 to 50 mg nightly) or other At her 6-week postoperative checkup, in postmenopausal antidepressants (e.g., venlafaxine, sertraline, the surgical site is healed but tender. At her women duloxetine).8 I prefer low-dosage sertraline 3-month visit, the introitus is no longer ten- (25 mg daily) because it has a low incidence of der, erythema has resolved, and she resumes side effects at this dosage. coital activity. References 1. McKay M. Vulvodynia. Diagnostic patterns. 6. Landry T, Bergeron S, Dupuis MJ, Desrochers CA. Topical gabapentin in the treatment of local- Dermatol Clin. 1992;10:423–433. G. The treatment of provoked vestibulodynia: a ized and generalized vulvodynia. Obstet Gynecol. 2. Sobel JD, Wiesenfeld HC, Martens M, et al. critical review. Clin J Pain. 2008;24:155–171. 2008;112:579–585. Maintenance fluconazole therapy for recurrent vul- 7. Bornstein J, Goldik Z, Stolar Z, Zarfati D, 11. Harlow BL, Stewart EG. A population-based as- vovaginal candidiasis. N Engl J Med. 2004;351:876– Abramovici H. Predicting the outcome of surgical sessment of chronic unexplained vulvar pain: have 883. treatment of vulvar vestibulitis. Obstet Gynecol. we underestimated the prevalence of vulvodynia? J 3. Friedrich EG Jr. Vulvar vestibulitis syndrome. J 1997;89(5 Pt 1):695–698. Am Med Womens Assoc. 2003;58:82–88. Reprod Med. 1987;32:110–114. 8. McKay M. Dysesthetic (“essential”) vulvodyn- 12. Goetsch MF. Vulvar vestibulitis: prevalence 4. Nyirjesy P. Is it vestibulitis? Contemp Ob Gyn. ia. Treatment with amitriptyline. J Reprod Med. and historic features in a general gynecologic prac- 2007;52(1):64–73. 1993;38:9–13. tice population. Am J Obstet Gynecol. 1991;164(6 5. Marinoff SC, Turner ML, Hirsch RP, Richard G. 9. Harris G, Horowitz B, Borgida A. Evaluation of Pt 1):1609–1616. Intralesional alpha interferon. Cost-effective thera- gabapentin in the treatment of generalized vulvo- 13. Moyal-Barracco M, Lynch PJ. 2003 ISSVD ter- py for vulvar vestibulitis syndrome. J Reprod Med. dynia, unprovoked. J Reprod Med. 2007;52:103–106. minology and classification of vulvodynia: a histor- 1993;38:19–24. 10. Boardman LA, Cooper AS, Blais LR, Raker ical perspective. J Reprod Med. 2004;49:772–777. 60 OBG Management | May 2009 | Vol. 21 No. 5