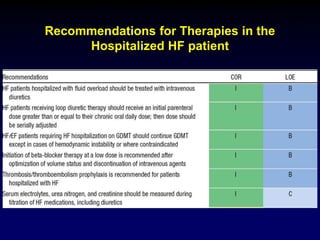
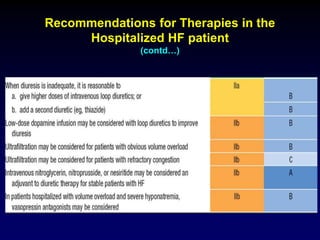
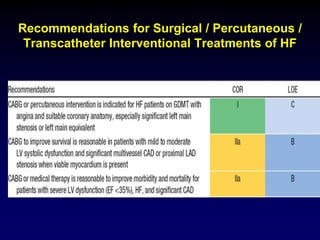
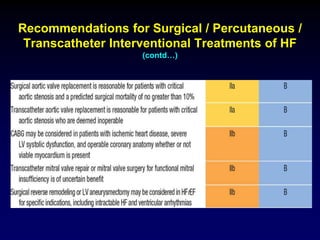
1. Management of Heart Failure Guideline 2013 provides recommendations for treating heart failure based on evidence from clinical trials and guidelines.
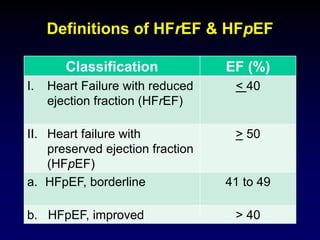
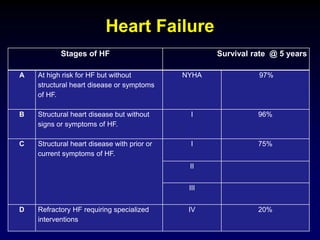
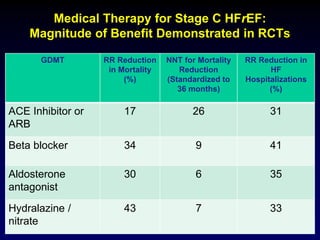
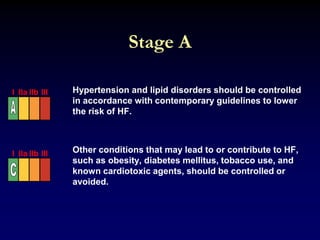
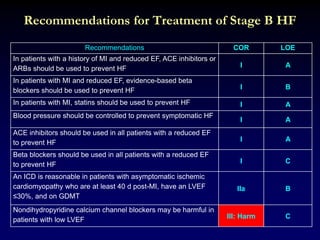
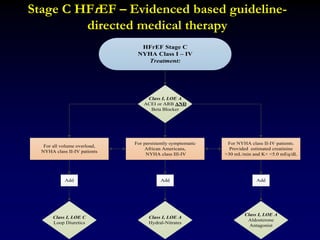
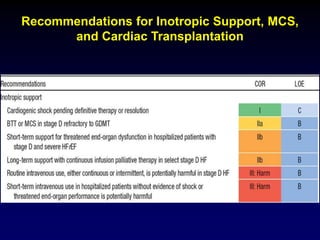
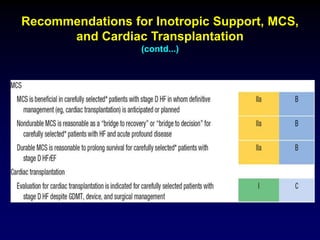
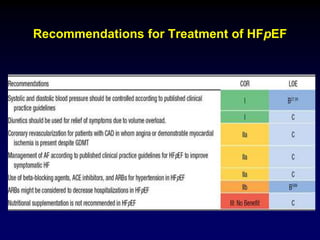
2. Heart failure is classified into stages based on symptoms and ejection fraction. Recommended treatments include drugs that have been shown to decrease mortality such as beta blockers, ACE inhibitors, and aldosterone antagonists.
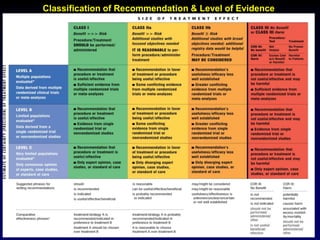
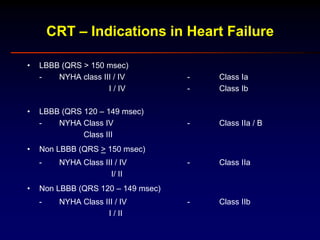
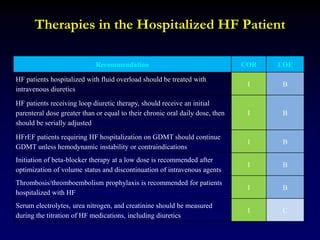
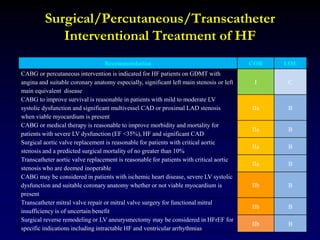
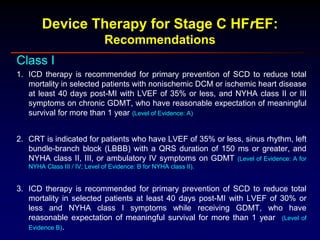
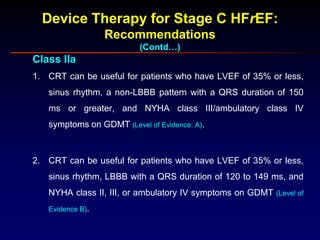
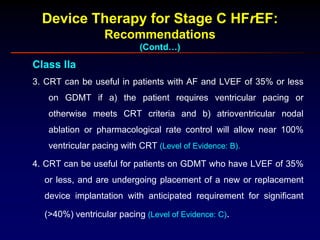
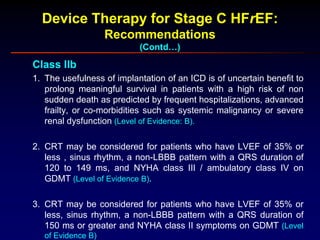
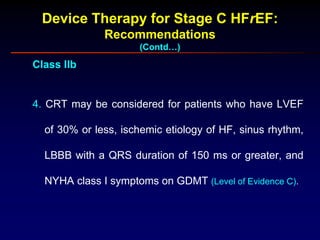
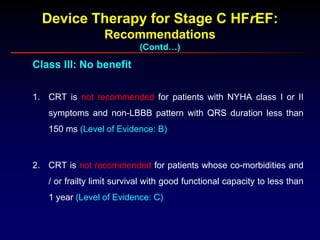
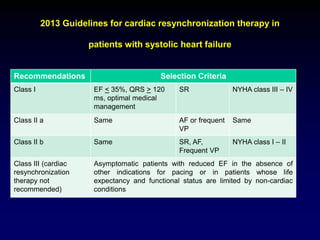
3. Device therapies such as implantable cardioverter defibrillators and cardiac resynchronization therapy are recommended for selected patients to reduce mortality and hospitalizations based on results from major clinical trials.

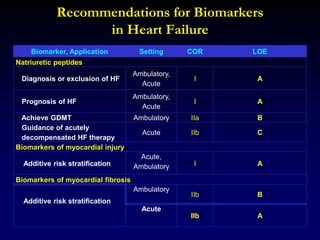
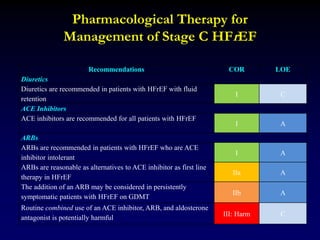
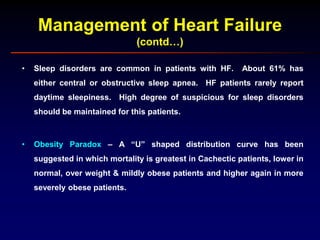
![Selected clinical trials establishing the benefit of angiotensin-
converting enzyme inhibitors in symptomatic and
asymptomatic LV systolic function
Trial (Ref) (No. of
patients; average
follow up)
Study
population
ACE inhibitor
and dose
Key results
CONSENSUS I [22] (n = 253; 6
mo)
NYHA IV Enalapril vs Placebo 2.5
mg twice daily titrated to
20 mg twice daily
6 month mortality decreased 40%
1-year mortality decreased 31%
Improvement in NYHA class
Decrease in cardiac size
V-HeFT II [24]
(n=804; 2.5 y)
NYHA II – IV
LVEF < 45%
Target enalapril 10 mg
twice daily vs
hydralazine 75 mg four
times daily + isosorbide
dinitrate 40 mg four
times daily
2 year mortality decreased 28%
No difference in HF hospitalization
Lesser improvement in exercise
capacity and ventricular function with
enalapril
SOLVD Treatment Trial [65]
(n = 2569; 41 mo)
NYHA II – IV (90% II
– III)
LVEF < 35%
Enalapril vs placebo 2.5
mg twice daily titrated to
10 mg twice daily
16% decrease in mortality
22% decrease in progressive HF
mortality
26% decrease in either death or HF
hospitalization
8.6 month increase in median life
expectancy [76]
SOLVD Prevention Trial [29]
( n = 4228; 37.4 month)
NYHA I
LVEF < 35%
Enalapril vs placebo 2.5
mg twice daily titrated to
10 mg twice daily
20% decrease in either death or HF
hospitalization
29% decrease in either death or
development of HF](https://image.slidesharecdn.com/11472874-221214182337-5e0ae0a2/85/11472874-ppt-15-320.jpg)
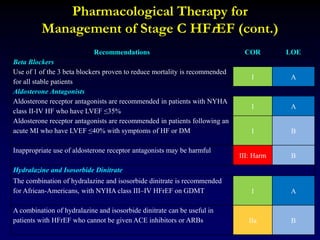
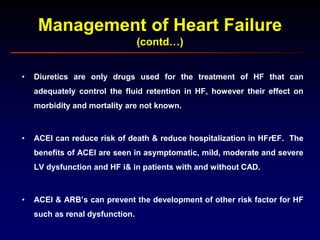
![Summary of Implantable cardioverter defibrillator
trials in patients with a cardiomyopathy due to CAD
Ischemic
Cardiomyopathy
Entry Criteria EF (%) Overall
mortality
(control;
ICDs [%])
Mortality
reduction
(relative;
absolute
[%])
MADIT 2 – year
analysis
EF 35%, nonsustained
or inducible VT
26 + 7 32; 13 59; 19
MUSTT 5 –year
analysis
EF < 40%, inducible
VT
30 (21-
35)
55; 24 58; 31
MADIT II 2 – year
analysis
EF < 30% 23 + 5 22; 16 28; 6
SCDHeFT 5 – year
analysis
EF < 35%, NYHA II, III,
52% CAD – CHF
25 (20 –
30)
36; 29 23; 7](https://image.slidesharecdn.com/11472874-221214182337-5e0ae0a2/85/11472874-ppt-22-320.jpg)
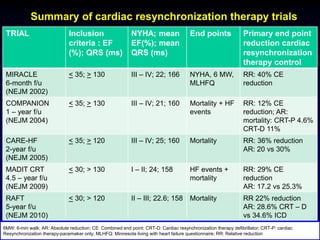
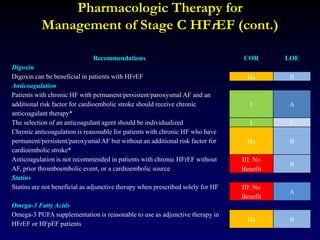
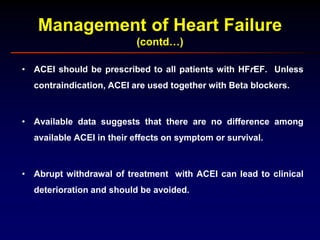
![Summary of Implantable cardioverter defibrillators trials
in patients with a nonischemic cardiomyopathy
Nonischemic
Cardiomyopathy
Entry Criteria EF %
(mean)
Overall
mortality
(control;
ICD [%])
DEFINITE 2 – year
analysis
EF < 36%, NSVT or >
10 PVCs / h
21.4 14.1; 7.9
SCDHeFT 5 – year
analysis
EF < 35%, NYHA II –
III; 48% nonischemic
CM
25 36; 29](https://image.slidesharecdn.com/11472874-221214182337-5e0ae0a2/85/11472874-ppt-23-320.jpg)
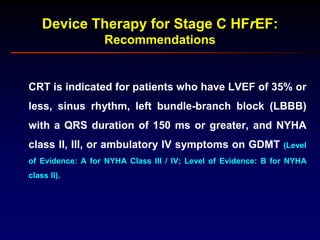
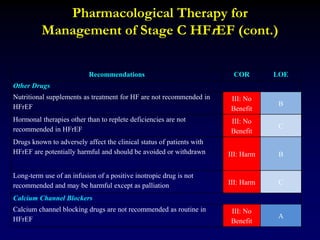
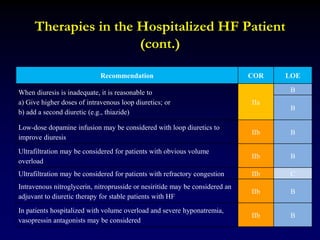









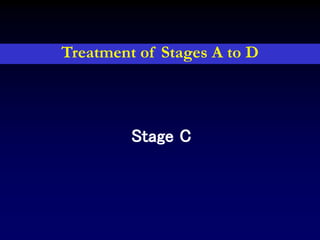

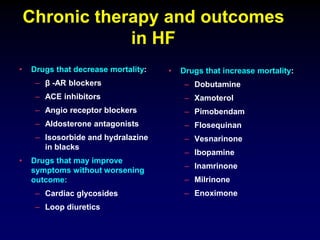
![Pharmacological Treatment for
Stage C HFrEF (cont.)
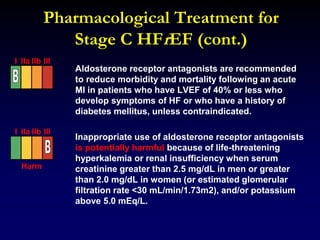
Aldosterone receptor antagonists [or mineralocorticoid
receptor antagonists (MRA)] are recommended in
patients with NYHA class II-IV and who have LVEF of
35% or less, unless contraindicated, to reduce morbidity
and mortality. Patients with NYHA class II should have a
history of prior cardiovascular hospitalization or elevated
plasma natriuretic peptide levels to be considered for
aldosterone receptor antagonists. Creatinine should be
2.5 mg/dL or less in men or 2.0 mg/dL or less in women
(or estimated glomerular filtration rate >30
mL/min/1.73m2) and potassium should be less than 5.0
mEq/L. Careful monitoring of potassium, renal function,
and diuretic dosing should be performed at initiation and
closely followed thereafter to minimize risk of
hyperkalemia and renal insufficiency.
I IIa IIb III](https://image.slidesharecdn.com/11472874-221214182337-5e0ae0a2/85/11472874-ppt-98-320.jpg)



![Heart failure – an update [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/heartfailureanupdateautosaved-110321012825-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)