v
¡Í§ºÃóҸԡÒÃ
ª×Í-Ê¡ØÅ
è ´ÒÃÒÇÃó ǹЪÔǹÒÇÔ¹
Çز¡ÒÃÈÖ¡ÉÒ
Ô ¾.º., ».ªÑ¹ÊÙ§ (ÍÒÂØÃÈÒʵÃ), Ç.Ç. µ¨ÇÔ·ÂÒ,
é
Í.Ç. ¾ÂÒ¸ÔÇ·ÂÒ¤ÅÔ¹¡
Ô Ô
µíÒá˹‹§·Ò§ÇÔªÒ¡Òà ÃͧÈÒʵÃÒ¨ÒÃÂ
˹‹Ç§ҹ ÊÒ¢ÒÇÔªÒâ»Ã⵫ÑÇ ÀÒ¤ÇÔªÒ»ÃÊÔµÇÔ·ÂÒ
ʶҺѹ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ÔÔ
ª×Í-Ê¡ØÅ
è Á³Õ Ãѵ¹äªÂÒ¹¹·
Çز¡ÒÃÈÖ¡ÉÒ
Ô ¾.º., ».ªÑ¹ÊÙ§ (ÊÙµÈÒʵÃ-¹ÃÕàǪÇÔ·ÂÒ), Ç.Ç. ÊÙµÈÒʵÃ-¹ÃÕàǪÇÔ·ÂÒ,
é Ô Ô
Cert. .ellow in Reproductive Biology,
Ç.Ç. àǪÈÒʵáÒÃà¨ÃԾѹ¸Ø, Í.Ç. àǪÈÒʵäÃͺ¤ÃÑÇ,
Ç·.Á. (¡ÒþѲ¹ÒÊØ¢ÀÒ¾)
µíÒá˹‹§·Ò§ÇÔªÒ¡Òà ÈÒʵÃÒ¨ÒÃÂ
˹‹Ç§ҹ ˹‹Çµ‹ÍÁäÃŒ·Í·Ò§¹ÃÕàǪ ÊÒ¢ÒÇÔªÒàǪÈÒʵáÒÃà¨ÃԾѹ¸Ø
‹
ÀÒ¤ÇÔªÒÊÙµÈÒʵÃ-¹ÃÕàǪÇÔ·ÂÒ
Ô
ʶҺѹ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ÔÔ
ª×Í-Ê¡ØÅ
è ÇÒ³Õ ÇÔÊ·¸ÔàÊÃÕǧÈ
Ø ì
Çز¡ÒÃÈÖ¡ÉÒ
Ô ¾.º., ».ªÑ¹ÊÙ§ (¡ØÁÒÃàǪÈÒʵÃ), Ç.Ç. ¡ØÁÒÃàǪÈÒʵÃ,
é
Dip. of Dermatology, Cert. in Ped. Dermatology,
Í.Ç. (àǪÈÒʵäÃͺ¤ÃÑÇ), Í.Ç. (¡ØÁÒÃàǪÈÒʵà µ¨ÇÔ·ÂÒ)
µíÒá˹‹§·Ò§ÇÔªÒ¡Òà ÃͧÈÒʵÃÒ¨ÒÃÂ
˹‹Ç§ҹ ÊÒ¢Òâä¼ÔÇ˹ѧ ÀÒ¤ÇÔªÒ¡ØÁÒÃàǪÈÒʵÃ
ʶҺѹ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ÔÔ
ª×Í-Ê¡ØÅ
è ÇÔ·Ã ªÔ¹ÊÇ‹Ò§ÇѲ¹¡ØÅ
Ù
Çز¡ÒÃÈÖ¡ÉÒ
Ô ¾.º., Ç.Ç.(ÈÑÅÂÈÒʵÃ), Ph.D. (London)
µíÒá˹‹§·Ò§ÇÔªÒ¡Òà ÍÒ¨ÒÃÂ
˹‹Ç§ҹ ÊÒ¢ÒÇÔªÒÈÑÅÂÈÒʵ÷Çä» ÀÒ¤ÇÔªÒÈÑÅÂÈÒʵÃ
Ñè
ʶҺѹ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ÔÔ
7.
vi
ª×Í-Ê¡ØÅ
è ÁÒ¹¾ ¾Ô·¡ÉÀÒ¡Ã
Ñ
Çز¡ÒÃÈÖ¡ÉÒ
Ô ¾.º., Í.Ç.(ÍÒÂØÃÈÒʵÃ)
Diplomate, American Board of Internal Medicine
Diplomate, American Board of Medical Genetics
.ellowship in Clinical Genetics and Clinical Molecular Genetics
µíÒá˹‹§·Ò§ÇÔªÒ¡Òà ¼ÙªÇÂÈÒʵÃÒ¨ÒÃÂ
Œ ‹
˹‹Ç§ҹ ÊÒ¢ÒÇÔªÒàǪ¾Ñ¹¸ØÈÒʵà ÀÒ¤ÇÔªÒÍÒÂØÃÈÒʵÃ
ʶҺѹ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ÔÔ
8.
vii
ÃÒ¹ÒÁ¼ÙŒ¹Ô¾¹¸
Wei Mei Ching ¡Ñ·Í§ ·Í§ãË‹
Doctor ÍÒ¨ÒàᾷÂËÔ§ ËÁ‹ÍÁËÅǧ
Viral and Rickettsial Diseases Department ÀÒ¤ÇÔªÒâʵ ¹ÒÊÔ¡ ÅÒÃÔ§«Ç·ÂÒ
Ô
Naval Medical Research Center, MD, USA ¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
¡¹¡ÇÃó ºØ¾ÔÊ®°ŠÔ
ÃͧÈÒʵÃÒ¨ÒàᾷÂËÔ§ à¡ÃÕ§ÈÑ¡´Ôì ¨ÕÃÐá¾·Â
ÀÒ¤ÇÔªÒÍÒÂØÃÈÒʵà ÈÒʵÃÒ¨Òà¹ÒÂá¾·Â
¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ ÀÒ¤ÇÔªÒ¡ØÁÒÃàǪÈÒʵÃ
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å ¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
¡ÁŷԾ ËÒ¼´Ø§¡Ô¨
ÃͧÈÒʵÃÒ¨ÒàᾷÂËÔ§ ¤íÒÁØ¡ ¤ÃͧÂØ·¸
ÀÒ¤ÇÔªÒàǪÈÒʵÿ¹¿Ù
„œ ¹Ò§ÊÒÇ
¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ ÀÒ¤ÇÔªÒÃѧÊÕÇ·ÂÒ
Ô
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å ¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
¡ÅÕºÊäº ÊÃþ¡Ô¨
¼ÙªÇÂÈÒʵÃÒ¨ÒàᾷÂËÔ§
Œ ‹ ¨Ñ¹¨ÔÃÒ à¾ªÃÊØ¢ÈÔÃÔ
ÀÒ¤ÇÔªÒ¡ØÁÒÃàǪÈÒʵà ¼ÙªÇÂÈÒʵÃÒ¨ÒàᾷÂËÔ§
Œ ‹
¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ ÀÒ¤ÇÔªÒÃѧÊÕÇ·ÂÒ
Ô
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å ¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
¡ŒÍ§à¢µ àËÃÕÂÊØÇÃó
¼ÙªÇÂÈÒʵÃÒ¨Òà¹ÒÂá¾·Â
Œ ‹ ¨Ñ¹·¹ÃÑÈÁ ¨Ñ¹·¹Âԧ§
è
ÀÒ¤ÇÔªÒÈÑÅÂÈÒʵÃÍÍÃ⸻´Ô¤ÊáÅÐ ÍÒ¨ÒàᾷÂËÔ§
¡ÒÂÀÒ¾ºíҺѴ ÀÒ¤ÇÔªÒÈÑÅÂÈÒʵÃÍÍÃ⸻´Ô¤ÊáÅÐ
¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ ¡ÒÂÀÒ¾ºíҺѴ
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å ¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
xxv
68 Traumatic CerebrovascularInjury: Neurosurgical Perspective 489
àÍ¡ÇØ²Ô ¨Ñ¹á¡ŒÇ, ·ÇÕÈ¡´Ôì àÍ×ͺØÒÇѲ¹, ÍѪÅÕ ªÙâè¹
Ñ é
69 Interventional Radiology Management in Traumatic Patient 497
(Body and Peripheral Artery)
ÊÁÃÒª ¸ÃÃÁ¸ÃÇѲ¹
ÀÒÇмԴ»¡µÔ¢Í§¡Òù͹ËÅѺ
70 ¹Í¹¡Ã¹áÅÐÀÒÇÐËÒÂ㨼Դ»¡µÔ¢³ÐËÅѺª¹Ô´ÍØ´¡Ñ¹
é 505
ÇÔª ºÃóËÔÃ
Ñ
71 Narcolepsy 523
ÇѲ¹ªÑ ⪵ԹÂÇѵáØÅ
Ñ
72 Surgical Treatment for Sleep Disordered Breathing 529
ÇÔª ºÃóËÔÃ
Ñ
ÀÒÇмԴ»¡µÔ¢Í§¡ÒáÅ×¹
73 Management for Dysphagia Patients 535
⪤ªÑ àÁ¸ÕäµÃÃѵ¹, ๵ÃÒ ºÑÇ¡¹¡, ÀÒÇÔ¹ à¡É¡ØÅ, ÇÃصÁ ¾§ÈÒ¾Ôª, Êع¹· ͧÍÒ¨
Ñ
ÀÒÇÐàÅ×Í´ÍÍ¡ã¹·Ò§à´Ô¹ÍÒËÒÃʋǹº¹
74 ÀÒÇÐàÅ×Í´ÍÍ¡ã¹·Ò§à´Ô¹ÍÒËÒÃʋǹº¹ 543
ÇÃÒÂØ »ÃѪ¡ØÅ
75 Management of Esophageal Varices and Esophageal Variceal Hemorrhage 555
ÈÔÇоà äªÂ¹Øǵ,Ô ¹¹·ÅÕ à¼‹ÒÊÇÑÊ´Ô,ì Êؾ¨¹ ¹ÔÁ͹§¤
Ñ è
76 Embolization for Upper Gastrointestinal Hemorrhage 565
ÇÅÑÂÅѡɳ ªÑÂÊÙµÃ
¡ÒÃÇÔ¨ÑÂáÅÐÇÔ·ÂÒÈÒʵþ×é¹°Ò¹·Ò§¡ÒÃá¾·Â
77 General Aspects of Tumor Microenvironment 569
»‚µÔ ¸ØǨԵµ
78 Cancer-associated .ibroblasts in Tumor Progression 573
ª¹ÔµÃÒ ¸ØǨԵµ
27.
xxvi
79 Digital ImageProcessing and Data Management for Clinical 579
Registry and Clinical Research
»ÃоѲ¹ ÊØüÅ
Ô
80 Research and Road to Innovation and Business 587
ÇÃóРÁËÒ¡ÔµµÔ¤³, ¾ÔÁ¾»ÃÐä¾ ¸ÕÃЪվ, ¸ÒÃÔ¹ àÍÕÂÁྪÃÒ¾§È, ¸¹¾Å ÇÕÃÒÊÒ
Ø è
¡¯ËÁÒ·ҧ¡ÒÃá¾·Â
81 Transplantation: Medico-legal Investigation 595
»ÃÕªÒ ÈÔ÷ͧ¶ÒÇÃ
Ô
82 ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ÊÒÂàÊÕ§ 597
侺ÙÅ ÊØþ§É
Õ
83 Hearing Loss in Children: 120 year Evolution in Management 601
ÊØǨ¹Ò ͸ÔÀÒÊ
Ñ
´Ñª¹Õ
´Ñª¹Õ 605
4 Childhood Seizure and Epilepsy
Partial seizure (.ocal seizure) (4)
Partial ËÃ×Í focal seizure ໚¹ÍÒ¡Òêѡ«Ö§à¡Ô´¨Ò¡¡Ò÷ÕÁ¡ÃÐáÊä¿¿‡Ò·ÕÁÒ¡¼Ô´»¡µÔà¡Ô´¢Ö¹
è è Õ è é
¨Ò¡ÊÁͧʋǹã´Ê‹Ç¹Ë¹Ö§ â´Â¡ÃÐáÊä¿¿‡Ò´Ñ§¡Å‹ÒÇÍÒ¨¤§ÍÂÙ·à´ÔÁËÃ×Í ÍÒ¨à¤Å×͹价ÕÊÁͧʋǹÍ׹䴌
è ‹ Õè è è è
«Ö§¨ÐÁռŵ‹ÍÅѡɳСÒêѡ¢Í§¼Ù»Ç ÍÒ¡ÒêѡẺ¹Õẋ§ä´ŒÍ¡à»š¹ 2 ª¹Ô´Â‹Í¤×Í
è Œ † é Õ
1. Simple partial seizure (SPS) ã¹¢³ÐªÑ¡¼Ù»Ç¨ÐÂѧÃÙÊ¡µÑÇ (consciousness) ·Õ´ÍÂÙ‹
Œ † ŒÖ è Õ
ÅѡɳСÒêѡ¢Í§¼ÙŒ»†Ç¹Ñ鹨ТÖé¹ÍÂÙ‹¡ÑºÇ‹ÒÊÁͧʋǹ㴶١¡Ãе،¹â´Â¡ÃÐáÊä¿¿‡Ò·Õè¼Ô´»¡µÔ
¼Ù»ÇÂÍÒ¨¨ÐÁÕÍÒ¡ÒÃà¤Å×͹äËǢͧËҧ¡Ò·ռ´»¡µÔ (motor seizure) ઋ¹ à¡Ãç§ ¡Ãеء ʋǹ˹֧
Œ † è è Ô è
ʋǹ㴢ͧËҧ¡Ò ઋ¹ãºË¹ŒÒ äËÅ‹ ᢹ Á×Í ¢ÒËÃ×Íà·ŒÒ ¢ŒÒ§ã´¢ŒÒ§Ë¹Ö§ ºÒ§ÃÒÂÍÒ¨¨ÐÁÕÍÒ¡Ò÷ҧ è
¤ÇÒÁÃÙÊ¡ËÃ×Í »ÃÐÊÒ·ÊÑÁ¼ÑʾÔàÈÉÍ×¹æ (somatosensory or special-sensory seizure) ઋ¹ ªÒᢹ
ŒÖ è
¢Ò¢ŒÒ§ã´¢ŒÒ§Ë¹Ö§ àËç¹áʧ 䴌¹àÊÕ§ ËÃ×Íä´Œ¡ÅÔ¹µ‹Ò§æ ·Õ¼´»¡µÔ
è Ô è è Ô
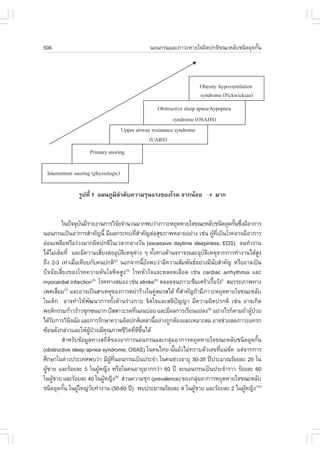
2. Complex partial seizure (CPS) ¼ÙŒ»†Ç¨ÐÁÕ impairment of consciousness «Öè§
consciousness ·Õ㪌¡¹ã¹âäÅÁªÑ¡¹Ñ¹»ÃСͺ´ŒÇ 2 ʋǹ¤×Í responsiveness (¡Òõͺʹͧµ‹Í
è Ñ é
ÊÔ§àÃŒÒ ËÃ×Í·íÒµÒÁ¤íÒÊѧÍ‹ҧÁÕ¤ÇÒÁËÁÒÂ) áÅÐ awareness (¡ÒÃÃѺÃÙáÅÐÊÒÁÒö¨´¨íÒà˵ءÒó
è è Œ
µ‹Ò§æ ·Õèà¡Ô´¢Öé¹ã¹¢³Ð·ÕèÁÕÍÒ¡Òêѡ) ¼ÙŒ·Õ辺àË繡Òêѡ¢Í§¼ÙŒ»†ÇÂÍÒ¨¨Ð͸ԺÒÂÇ‹Ò¼ÙŒ»†ÇÂÁÕÍÒ¡ÒÃ
àËÁèÍ à»ç¹ÅÁ ËÁ´ÊµÔ ËÃ×ͺҧ¤ÃѧÍÒ¨¨Ð´ÙàËÁ×͹ÃÙÊ¡µÑÇ´ÕáµèäÁè·ÓµÒÁ¤ÓÊѧ ã¹¢³Ð·Õª¡¹Ñ¹ ¼Ù»ÇÂ-
é éÖ è è Ñ é é è
ºÒ§ÃÒÂÍÒ¨¨ÐÁÕ¡ÒÃà¤Å×è͹äËǢͧËҧ¡Ò«éíÒæ àÃÕÂ¡Ç‹Ò automatism «Ö觼ٌ»†ÇÂÍÒ¨¨Ð¢ÂѺ»Ò¡
àËÁ×͹à¤ÕÂÇ ËÃ×Í¡Å×¹ (lips smacking, swallowing) ¨ÑºÁ×ÍËÃ×ÍËÂÔº¨ÑºÊÔ§¢Í§µ‹Ò§æ ËÃ×Íà´Ô¹ä»ÁÒ
é è
«Ö§à»š¹¾ÄµÔ¡ÃÃÁ·ÕäÁ‹Á¤ÇÒÁËÁÒ â´Â·ÑÇä»ÃÐÂÐàÇÅÒ·Õª¡»ÃÐÁÒ³ 2-3 ¹Ò·Õ (30 ÇÔ¹Ò·Õ – 10 ¹Ò·Õ)
è è Õ è è Ñ
¹Í¡¨Ò¡¹ÕÍÒ¨¾ºÍÒ¡ÒùíÒ pre-ictal symptom (aura) «Ö§à»š¹¤ÇÒÁÃÙÊ¡·Õ¼»Çºҧ¤¹ÍÒ¨¨Ð͸ԺÒÂ
é è Œ Ö è ÙŒ †
ä´Œ¡Í¹ÁÕÍÒ¡Òêѡ ´Ñ§·Õ¾ºã¹ SPS ËÅѧ¨Ò¡ªÑ¡ (post-ictal state) ¼Ù»ÇÂÁÑ¡¨ÐÁÕÍÒ¡ÒÃÊѺʹ䴌µÍ
‹ è Œ † ‹
໚¹¹Ò·Õ
¼ÙŒ»†Ç·ÕèàÃÔèÁµŒ¹¡Òêѡ´ŒÇ SPS ËÃ×Í CPS ¹Ñé¹ÍÒ¨¨ÐÁÕ¡ÒÃà¡Ãç§ËÃ×Í¡Ãеء¢Í§Ã‹Ò§¡ÒÂ
·Ñ§µÑǵÒÁÁÒ ¨ÐàÃÕÂ¡Ç‹Ò partial seizure evolving to secondarily generalized seizure ´Ñ§¹Ñ¹¼Ù»Ç·Õè
é é Œ †
ÁÕ¼¾ºÇ‹ÒÁÕÍÒ¡ÒÃà¡Ã秡Ãеء·Ñ§µÑǹѹÍÒ¨¨Ð໚¹¡ÒêѡẺ focal ¹íÒÁÒ¡‹Í¹¡çä´Œ
ÙŒ é é
Generalized seizure (4)
Generalized seizure ໚¹ÍÒ¡Òêѡ·Õà¡Ô´¢Ö¹¨Ò¡¡ÒÃà»ÅÕ¹á»Å§¢Í§¡ÃÐáÊä¿¿‡Ò·Õè¡Ãеع
è é è Œ
ÊÁͧ·ÑèÇæ仾ÌÍÁ¡Ñ¹·Ñé§Êͧ¢ŒÒ§ ·íÒãËŒÁռŵ‹Í¤ÇÒÁÃÙŒÊÖ¡µÑÇáÅÐ ¡ÒÃà¤Å×è͹äËǢͧ¡ÅŒÒÁà¹×éÍ
·ÕäÁ‹¨Òà¾Òзբҧ㴢ŒÒ§Ë¹Ö§¢Í§Ã‹Ò§¡Ò generalized seizure ẋ§Í͡໚¹ 4 ¡ÅØÁãË‹æ 䴌ᡋ
è í è Œ è ‹
1. Tonic-clonic seizure (grand mal) ¼Ù»Ç¨ÐÁÕ¤ÇÒÁÃÙÊ¡µÑÇ·ÕŴŧ ËÇÁ¡ÑºÍÒ¡ÒÃà¡Ãç§ áÅÐ/
Œ † ŒÖ è
ËÃ×Í¡Ãеء¢Í§ÅíÒµÑÇ, ᢹ¢Ò â´Â·ÑèÇä»ÍÒ¡Òêѡ¨ÐàÃÔèÁµŒ¹´ŒÇÂÍÒ¡ÒÃà¡Ãç§ (tonic phase) áÅŒÇ
µÒÁÁÒ´ŒÇÂÍÒ¡ÒáÃеء (clonic phase) ª‹Ç§·ÕèÁÕÍÒ¡Òêѡ¼ÙŒ»†ÇÂÍÒ¨ÁÕÍÒ¡Ò÷ҧÃкº»ÃÐÊÒ·
Íѵâ¹ÁѵÃÇÁ´ŒÇ¤×Í ÁÕÁÒ¹µÒ¢ÂÒÂ, ¹éÒÅÒ¿ÙÁ»Ò¡, à˧×ÍÍÍ¡, »˜ÊÊÒÇÐ Íب¨ÒÃÐÃÒ´ ËÅѧ¨Ò¡ªÑ¡
Ô‹ ‹ í è
¼Ù»ÇÂÁÑ¡¨ÐÁÕÍÒ¡ÒÃà¾ÅÕ ÊѺʹ ËÅÑºä» ÍÒ¡Òêѡª¹Ô´¹Õé ¼Ù¤¹·ÑÇä»ÁÑ¡ÃÙ¨¡ã¹ª×Í ÅÁºŒÒËÁÙ ¼Ù»ÇÂ
Œ † Œ è ŒÑ è Œ †
àǪÈÒʵ÷¹Âؤ 2553
Ñ 9
1. àÅ×Í¡ÂÒ·ÕàËÁÒÐÊÁ¡ÑºÍÒ¡Òêѡ¢Í§¼Ù»ÇÂ
è Œ †
.irst line drug in partial seizure : Phenytoin, phenobarbital,carbamazepine,
valproic acid
Primary generalized tonic-clonic seizure : Phenytoin, phenobarbital, carbamazepine,
valproic acid
Absence, myoclonic, atonic seizure : Valproic acid
Infantile spasm : Vigabatrin, ACTH
2. ¤ÇÃàÃÔÁÂҡѹªÑ¡´ŒÇÂÂÒª¹Ô´à´ÕÂÇ¡‹Í¹ (monotherapy)
è
3. ¡ÒÃàÃÔÁÂÒ¤ÇÃãËŒÂÒã¹¢¹Ò´µèÒ à¾×ÍãËŒ¼»ÇÂÊÒÁÒö·¹µ‹Í¼Å¢ŒÒ§à¤Õ§·ÕÍÒ¨à¡Ô´¢Ö¹ áÅÐ
è í è ÙŒ † è é
»ÃѺ¢¹Ò´ ÂÒãˌʧ¢Ö¹Í‹ҧªŒÒæ ¨¹¡Ç‹Ò¼Ù»Ç¨ÐäÁ‹ÁÍÒ¡ÒêѡËÃ×ÍàÃÔÁÁռŢŒÒ§à¤Õ§¢Í§ÂÒ ¢¹Ò´áÅÐ
Ù é Œ † Õ è
¤ÇÒÁ¶Õ¢Í§¡ÒÃãËŒÂҡѹªÑ¡·Õ㪌ºÍÂã¹»ÃÐà·Èä·ÂáÊ´§änj㹵ÒÃÒ§·Õè 3
è è ‹
4. ºÃÔËÒÃÂÒµÒÁÅѡɳТͧàÀÊѪ¨Å¹ÈÒʵâͧÂÒᵋÅЪ¹Ô´
5. ¤Ç÷ÃÒº¶Ö§¼Å¢ŒÒ§à¤Õ§¢Í§ÂÒᵋÅЪ¹Ô´ áÅзÃÒº¶Ö§àÇÅҷըлÃÐàÁÔ¹¼Å¡ÒÃÃÑ¡ÉҢͧ è
ÂÒª¹Ô´¹Ñ¹æ ÃÇÁ·Ñ§¢ŒÍº‹§ªÕ㹡ÒÃÊ‹§µÃǨáÅÐá»Å¼ÅÃдѺÂҡѹªÑ¡ã¹àÅ×Í´
é é é
6. àÁ×ͼٻÇÂä´ŒÂҡѹªÑ¡ã¹¢¹Ò´·ÕàËÁÒÐÊÁ ᵋÍÒ¡ÒêѡÂѧäÁ‹ÊÒÁÒö¤Çº¤ØÁä´Œ´Õ ËÃ×ÍÁÕ
è Œ † è
¼Å¢ŒÒ§à¤Õ§¢Í§ÂÒª¹Ô´áá·Õ㪌 ¤ÇþԨÒóÒàÃÔÁÂҡѹªÑ¡ª¹Ô´·Õè 2 â´Â¤íÒ¹Ö§¶Ö§¡ÒÃÍÍ¡Ä·¸Ô¢Í§ÂÒ
è è ì
¡Ñ¹ªÑ¡áÅÐ drug interaction ´ŒÇÂ
7. ã¹àǪ»¯Ôºµ·Ç仹ÔÂÁãËŒÂҡѹªÑ¡á¡‹¼»ÇµԴµ‹Í¡Ñ¹à»š¹ÃÐÂÐàÇÅÒ¹Ò¹ 2 »‚¡Í¹¾Ô¨ÒóÒ
Ñ Ô Ñè ÙŒ † ‹
ËÂØ´ÂҡѹªÑ¡¶ŒÒ¼Ù»ÇÂäÁ‹ÁÍÒ¡Òêѡ«éÒ »˜¨¨Ñ·շÒãËŒÁâÍ¡Òʪѡ«éÒÍÕ¡ÊÙ§¢Ö¹¡ç¤Í ÊÒà˵آͧ¡Òêѡ
Œ † Õ í è í Õ í é ×
¤ÇÒÁ¼Ô´»¡µÔ¢Í§¤Å×¹ÊÁͧ áÅÐÍÒÂØ·àÃÔÁÁÕÍÒ¡Òêѡ 㹡óշ¾¨ÒóÒáÅŒÇÇ‹ÒÊÁ¤ÇÃËÂØ´ÂÒ
è Õè è (14)
Õè Ô
¡Ñ¹ªÑ¡¹Ñ¹¤ÇÃÅ´ÂҡѹªÑ¡Å§Í‹ҧªŒÒæ «Ö§â´Â·ÑÇä»ÁÑ¡¨Ð¤‹ÍÂæ ËÂØ´ÂҡѹªÑ¡â´Â㪌ÃÐÂÐàÇÅÒ»ÃÐÁÒ³
é è è
2-3 à´×͹
37.
10 Childhood Seizure and Epilepsy
µÒÃÒ§·Õè 3 ¢¹Ò´áÅФÇÒÁ¶Õè¢Í§¡ÒÃãËŒÂҡѹªÑ¡·Õè㪌º‹ÍÂã¹»ÃÐà·Èä·Â
Drug Initial dose Maintenance dose .requency Therapeutic level Metabolism
(mg/kg/day) (mg/kg/day) (mg/L)
Phenobarbital 3-5 3-8 bid, hs 10-40 Hepatic
Phenytoin 5 5-8 bid, hs 10-20 Hepatic
Carbamazepine 10-15 10-30 tid, bid (CR) 4-12 Hepatic
Valproic acid 10-15 30-60 tid, bid (chrono) 50-120 Hepatic
Topiramate 1 5-9 bid - Renal 70%
Levetiracetam 10 20-60 bid - Renal 70%
Lamotrigine 0.5 5-10 bid - Renal 70%
Oxcarbazepine 10 20-50 bid - Renal 70%
ÊÃØ»
âäÅÁªÑ¡ã¹à´ç¡à»š¹âä·Ò§ÊÁͧ·Õ¾ºä´ŒºÍÂã¹àǪ»¯ÔºµÔ ᾷ¤ÇÃÁÕ¤ÇÒÁÃÙ·à¡ÕÂÇ¢ŒÍ§¡Ñº
è ‹ Ñ Œ Õè è
ÍÒ¡Òêѡ áÅÐâäÅÁªÑ¡ãËŒ´Õ ÁÕ¤ÇÒÁÊÒÁÒö·Õ¨Ð«Ñ¡»ÃÐÇÑµÔ µÃǨËҧ¡Ò àÅ×Í¡Ê‹§¡ÒõÃǨ¾ÔàÈÉ
è
Í×¹æ 䴌͋ҧàËÁÒÐÊÁà¾×ÍÇÔà¤ÃÒÐËÇÒ¼Ù»ÇÂÁÕÍÒ¡ÒêѡËÃ×ÍäÁ‹ ¶ŒÒÁÕÍÒ¡Òêѡ໚¹ÍÒ¡Òêѡª¹Ô´ã´
è è ‹ Œ †
¨Óà»ç¹µéͧãËé¡ÒÃÃÑ¡ÉÒËÃ×ÍäÁè ËÃ×ͨѴà¢éÒà»ç¹¡ÅØÁ epileptic syndrome ª¹Ô´ã´ä´éËÃ×ÍäÁè ¤ÇÃÁÕ¤ÇÒÁ-
è
ÃÙ㹡ÒÃàÅ×Í¡ÂҡѹªÑ¡·ÕàËÁÒÐÊÁ¡ÑºÍÒ¡Òêѡ·Õ¼»ÇÂÁÕ ¤Ç÷ÃÒº¶Ö§¼Å¢ŒÒ§à¤Õ§¢Í§ÂÒµ‹Ò§æ·ÕÍÒ¨¨Ð
Œ è è ÙŒ † è
à¡Ô´¢Ö¹ áÅФÇÃ͸ԺÒÂâäàº×ͧµŒ¹ãˌᡋ¼»Ç à¾×ÍãËŒ¼»ÇÂËÃ×ͼٻ¡¤ÃͧàË繶֧¤ÇÒÁÊíÒ¤Ñ㹡ÒÃ
é é ÙŒ † è ÙŒ † Œ
ÃÑ¡ÉÒ áÅШÐä´Œ»¯ÔºµµÇãËŒ¶¡µŒÍ§µ‹Íä»
Ñ Ô Ñ Ù
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Obeid M, Mikati MA. Expanding spectrum of paroxysmal events in children: Potential mimickers of epilepsy.
Pediatr Neurol. 2007;37:309-16.
2. Baulac M. Epilepsy. In: Schapira AHV, Byrne E, editors. Neurology and clinical neuroscience. Philadelphia:
Mosby Elsevier; 2007. p.673-718
3. The Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for
revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia. 1981;22:489-501.
4. Holmes GL, Nordli DR. Generalized, focal and multifocal seizure. In: Swaiman K., Ashwal S, .erriero DM,
editors. Pediatric neurology: principles and practice. Philadelphia: Mosby Elsevier; 2006. p. 1019-54.
5. The Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for
revised classification of epilepsies and epileptic syndromes. Epilepsia. 1989;30:389-99.
6. Roger J, Bureau M, Dravet C, Genton P, Tassinari CA, Wolf P. Epileptic syndromes in infancy, childhood and
adolescence. 3rd ed. London: John Libbey; 2002.
7. Arzimanoglou A, Guerrini R, Aicardi J. Aicardi’s epilepsy in children. 3rd ed. Philadelphia: Lippincott William &
Wilkins; 2004.
38.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 11
8. Hirtz D, Ashwal S, Berg A, et al. Practice parameter: evaluating a first nonfebrile seizure in children: report of
the quality standards subcommittee of the American Academy of Neurology, The Child Neurology Society,
and The American Epilepsy Society. Neurology. 2000;55:616-23.
9. Browne TR, Holmes GL. Epilepsy. N Engl J Med. 2001;344:1145-51.
10. Hirtz D, Berg A, Bettis D, et al. Practice parameter: treatment of the child with a first unprovoked seizure:
Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice
Committee of the Child Neurology Society. Neurology. 2003;60:166-75.
11. Shinnar S, Berg AT, Moshe SL, et al. The risk of seizure recurrence after a first unprovoked afebrile seizure in
childhood: an extended follow-up. Pediatrics. 1996;98:216-25.
12. Brodie M, Dichter M. Antiepileptic drugs. N Engl J Med. 1996;334(3):168-75.
13. Dichter M, Brodie M. New antiepileptic drugs. N Engl J Med. 1996;334(24):1583-90.
14. Practice parameter: a guideline for discontinuing antiepileptic drugs in seizure-free patients – summary statement.
Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 1996;47(2):
600-2.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 19
4. American Academy of Pediatrics, American College of Obstetricians and Gynecologists. Guidelines for perinatal
care. 6th ed. Elk Grove Village, IL:AAP; Washington DC: ACOG; 2007: 235-7.
5. American Academy of Pediatrics Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics.
2005;115:496–506.
6. Lester BM. Definition and diagnosis of colic. In: Sauls HS, Redfern DE, eds. Colic and excessive cry. Report
of the 105th Ross Conference on Pediatric Research. Columbus: Abbot Laboratories, 1997.
7. World Health Organization. Evidence for the ten steps to successful breastfeeding. Geneva: World Health
Organization, Division of Child Health and Development, 1998. http://www.who.int/nutrition/publications/
evidence_ten_step_eng.pdf
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 35
4
Cultivated Epithelial Cell in Ophthalmology, When and How?
ÃͧÈÒʵÃÒ¨ÒàᾷÂËÔ§ÀÔ¹ÔµÒ µÑ¹¸ØǹԵÂ
¼ÙŒª‹ÇÂÈÒʵÃÒ¨ÒàᾷÂËÔ§³Ñ°¾Ã à·ÈÐÇÔºØÅ
ÀÒ¤ÇԪҨѡÉØÇ·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ÔÔ
ÃͧÈÒʵÃÒ¨Òà´Í¡àµÍû˜·ÁÒ à͡⾸Ôì
ÀÒ¤ÇÔªÒÇÔ·ÂÒÀÙÁ¤Á¡Ñ¹ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ØŒ ÔÔ
¼ÙŒª‹ÇÂÈÒʵÃÒ¨Òà¹ÒÂá¾·ÂÁ§¤Å ÍØ»ÃÐàÊÃÔ°¡ØÅ
ÀÒ¤ÇÔªÒ¾ÂÒ¸ÔÇ·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ÔÔ
WHEN? àÁ×èÍäè֧¨íÒ໚¹µŒÍ§·íÒ¡ÒÃÃÑ¡ÉÒ´ŒÇ cultivated epithelial cell
Background
Corneal limbal epithelial stem cell ËÃ×Í à«Åŵ¹¡íÒà¹Ô´¢Í§¼ÔÇ¡ÃШ¡µÒ໚¹à«ÅÅ··Ò˹ŒÒ·Õè
Œ Õè í
ÊÌҧà«ÅżǡÃШ¡µÒ (corneal epithelial cell) à«ÅŹ¾ºÍÂÙ·ºÃÔàdzÃ͵‹Í¢Í§µÒ´íҡѺµÒ¢ÒÇ
Ô Õé ‹ Õè
(limbus; áÊ´§ã¹ÀÒ¾·Õè 1) áÅÐ໚¹»˜¨¨ÑÂ˹֧·ÕÊÒ¤Ñ㹡Ò䧤ÇÒÁãʢͧ¡ÃШ¡µÒ (cornea) â´Â
è èí
¨Ð¤Í¡ѹäÁ‹ãËŒà«ÅŢͧàÂ×ÍºØµÒ (conjunctiva) ÃءࢌÒÁÒ㹡ÃШ¡µÒ(1)
é è
ÀÒ¾·Õè 1 áÊ´§µíÒá˹‹§¢Í§ limbus «Öè§ÁÕ corneal epithelial stem cell ÍÂÙ‹
ÍÒ¡Ò÷ҧ¤ÅÔ¹¡
Ô
ËÒ¡ corneal limbal stem cell àÊ×ÍÁÊÀҾ仨зíÒãËŒà¡Ô´ÀÒÇÐ corneal limbal stem cell
è
deficiency(1,2) «Ö§ÁռŷíÒãËŒÁàÊŒ¹àÅ×Í´áÅÐà«ÅŢͧàÂ×ͺصÒÃءࢌÒÁÒã¹¼ÔǢͧ¡ÃШ¡µÒ à¡Ô´á¼ÅËÅØ´
è Õ è
Å͡໚¹æ ËÒÂæ ¡ÃШ¡µÒ¢Ø¹ áÅеÒÁÑÇŧ «Ö§¾ºä´Œã¹ÀÒÇÐÀÙÁᾌ·µÒÍ‹ҧÃعáç ¡ÅØÁÍÒ¡ÒÃ
‹ è Ô Õè ‹
Stevens Johnson ÍѹµÃÒ¨ҡÊÒÃà¤ÁÕ àª‹¹ ¡Ã´ ËÃ×Í´‹Ò§à¢ŒÒµÒ ¡ÒõԴàª×Í·Õ¡ÃШ¡µÒ µÒ·Õ䴌ú
é è è Ñ
63.
36 Cultivated Epithelial Cell in Ophthalmology, When and How?
¡Òü‹ÒµÑ´ËÅÒÂæ ¤Ãѧ(3) ¼Ù»Ç¨ÐÁÕÍÒ¡ÒõÒÁÑÇŧ ᾌáʧ äÁ‹ÊºÒÂµÒ «Ö§ËÒ¡à¡Ô´ÀÒÇдѧ¡Å‹ÒǹÕé
é Œ † è
¡ÒÃÃÑ¡ÉÒâ´Â¡Òü‹ÒµÑ´à»ÅÕ¹¡ÃШ¡µÒµÒÁ»¡µÔà¾Õ§Í‹ҧà´ÕÂÇ (corneal transplantation ËÃ×Í
è
penetrating keratoplasty) ¨ÐäÁ‹ÁâÍ¡ÒÊ»ÃÐʺ¼ÅÊíÒàÃç¨ÃÐÂÐÂÒÇä´ŒàÅ ´Ñ§¹Ñ¹¨Ö§¨íÒ໚¹µŒÍ§·íÒ¡ÒÃ
Õ é
ÃÑ¡ÉÒºÒ§»ÃСÒÃà¾×Í¿„¹¿ÙÊÀÒ¾¢Í§¡ÃШ¡µÒ¡‹Í¹
è œ (4)
¡ÒÃÃÑ¡ÉÒᵋà´ÔÁ
㹼ٻǷÕ໚¹ corneal limbal stem cell deficiency â´ÂÃͺ¡ÃШ¡µÒ ᵋà´ÔÁ¨Ð·íÒ¡ÒÃ
Œ † è
ÃÑ¡ÉÒâ´ÂÇÔ¸Õ»ÅÙ¡¶‹ÒÂà«ÅŵŒ¹¡íÒà¹Ô´ (stem cell) â´ÂµÃ§ (in vivo corneal limbal stem cell
transplantation)(2, 4) «Ö§ÍҨ㪌à«ÅŢͧ¼Ù»ÇÂàͧËÃ×ͨҡ¼ÙºÃÔ¨Ò¤ ´Ñ§¹Õé
è Œ † Œ
1. Autograft ã¹ÃÒ·Õ໚¹ corneal limbal stem cell deficiency ¢Í§µÒ¢ŒÒ§à´ÕÂÇ ÂѧÁÕà«ÅÅ·Õè
è
»¡µÔã¹µÒÍÕ¡¢ŒÒ§Ë¹Ö§ ¨ÐÊÒÁÒö㪌à«Åŵ¹¡íÒà¹Ô´¨Ò¡µÒ¢ŒÒ§·Õ»¡µÔ¢Í§¼Ù»ÇÂàͧ â´ÂàÍÒà¹×ÍàÂ×Í
è Œ è Œ † é è
ºÃÔàdzÃ͵‹Í¢Í§µÒ´íÒáÅеҢÒÇ (limbus) ÁÒ»ÅÙ¡¶‹ÒÂâ´ÂµÃ§
2. Allograft ã¹ÃÒ·յҷѧÊͧ¢ŒÒ§à»š¹ corneal limbal stem cell deficiency ÍҨ㪌à«ÅÅ
è é
¨Ò¡ÒµÔ àÃÕÂ¡Ç‹Ò living related corneal limbal allograft ËÃ×ͨҡµÒ¼ÙºÃÔ¨Ò¤ (allograft) â´Â¹íÒʋǹ
Œ
·Õ໚¹Ã͵‹Í¢Í§µÒ´íҡѺµÒ¢ÒÇÁÒ»ÅÙ¡¶‹ÒÂâ´ÂµÃ§
è
WHY? ·íÒäÁµŒÍ§ãªŒ cultivated epithelial cell 㹡ÒÃÃÑ¡ÉÒ·Ò§µÒ
¡Ò÷íÒ in vivo corneal limbal stem cell transplantation »˜ËÒ·Õ¾º¤×Í ËÒ¡¹íÒà«Åż͹
è ÙŒ ×è
ÁÒ»ÅÙ¡¶‹Ò (allograft) ¨ÐÁÕâÍ¡ÒÊà¡Ô´»¯Ô¡ÃÂÒµ‹ÍµŒÒ¹ (rejection) ÊÙ§ áÅеŒÍ§ÃѺ»ÃзҹÂÒ¡´
ÔÔ
ÀÙÁµÒ¹·Ò¹ (immunosuppressive drug) Í‹ҧµ‹Íà¹×ͧà¾×Í»‡Í§¡Ñ¹äÁ‹ãËŒà¡Ô´»¯Ô¡ÃÂҴѧ¡Å‹ÒÇ ã¹¡Ã³Õ
Ô Œ è è ÔÔ
¼Ù»ÇÂ໚¹âä·ÕµÒ¢ŒÒ§à´ÕÂÇ «Ö§¨Ð㪌à«ÅŨҡµÒ¢ŒÒ§·Õ»¡µÔ¢Í§¼Ù»ÇÂÁÒ»ÅÙ¡¶‹Ò ËÃ×ͼٻÇ·Õ໚¹âä
Œ † è è è Œ † Œ † è
·ÕµÒ·Ñ§Êͧ¢ŒÒ§áÅеŒÍ§¡ÒÃ㪌à«ÅŨҡµÒ¢Í§ÒµÔ ᾷ¨ÐäÁ‹ÊÒÁÒö¹íÒà«ÅŨҡµÒ¢ŒÒ§·Õ»¡µÔ
è é è
ÍÍ¡ÁÒ䴌㹻ÃÔÁÒ³ÁÒ¡æ ºÒ§¤Ãѧ»ÃÔÁÒ³¢Í§à«ÅŨ§äÁ‹à¾Õ§¾Í·Õ¨Ð»ÅÙ¡¶‹ÒÂà¾×Í»‡Í§¡Ñ¹¾Ñ§¼×´·Õ¨Ð
é Ö è è è
ÃءࢌҡÃШ¡µÒä´Œ ã¹ÃÐÂÐÂÒÇ
ä´ŒÁÕ¤ÇÒÁ¾ÂÒÂÒÁ㹡Ò䌹ËÒÇÔ¸ÕãËÁ‹ã¹¡ÒûÅÙ¡¶‹ÒÂà«ÅŵŒ¹¡íÒà¹Ô´¢Í§¼ÔÇ¡ÃШ¡µÒ
á·¹¡ÒÃ㪌à¹×éÍàÂ×èÍä»»ÅÙ¡¶‹ÒÂãˌᡋ¼ÙŒ»†ÇÂâ´ÂµÃ§ ᵋ¨Ð¹íÒà«ÅÅ·Õ赌ͧ¡ÒÃÁÒà¾ÒÐàÅÕé§ã¹ËŒÍ§
»¯Ôºµ¡Òá‹Í¹ ¨¹ä´Œ»ÃÔÁÒ³áÅÐÅѡɳеÒÁ·ÕµÍ§¡Òà ËÅѧ¨Ò¡¹Ñ¹¨Ö§¹íÒà«ÅÅ´§¡Å‹ÒÇÁÒ»ÅÙ¡¶‹ÒÂ
Ñ Ô è Œ é Ñ
ãˌᡋ¼»ÇÂÀÒÂËÅѧ 㹡ÒäѴàÅ×Í¡à«ÅÅ·¨Ð¹íÒÁÒà¾ÒÐàÅÕ§ ã¹»˜¨¨Øº¹ÁÕ 2 ª¹Ô´¤×Í
ÙŒ † Õè é Ñ
1. à«ÅŢͧ¡ÃШ¡µÒ (corneal epithelium)
2. à«ÅŢͧàÂ×ͺØã¹Ã‹Ò§¡Ò (mucosal epithelium)
è
64.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 37
HOW? ¨Ð㪌 cultivated epithelial cell ÁÒÃÑ¡ÉÒ䴌͋ҧäÃ
Corneal epithelial cell culture
¡ÒÃà¾ÒÐàÅÕ§â´Â㪌 corneal limbal stem cell à¾×Íà¾ÔÁ¨íҹǹ¢Í§ stem cell ¡‹Í¹¹íÒä»
é è è
»ÅÙ¡¶‹ÒÂãËŒÁÕ»ÃÔÁÒ³ÁÒ¡¾Í¡Ñº¤ÇÒÁµŒÍ§¡ÒÃáÅÐÅ´âÍ¡ÒÊ¡ÒÃà¡Ô´»¯Ô¡ÔÃÔÂÒµ‹ÍµŒÒ¹à¹×éÍàÂ×èÍ â´Â
·íÒ¡ÒÃà¾ÒÐàÅÕ§à«ÅÅã¹ËŒÍ§»¯Ôºµ¡Òú¹àÂ×ÍááŌǨ֧¹íÒ¡ÅѺ任ÅÙ¡¶‹ÒÂãˌᡋ¼»Ç ÊÒÁÒö
é Ñ Ô è ÙŒ †
à¾ÒÐàÅÕ§à«ÅŨҡ¢¹Ò´ 2 ÁÁ. ໚¹ 2 «Á. ã¹àÇÅÒ 2 - 4 ÊÑ»´ÒË ·íÒãËŒ¡Ò÷íÒ¼‹ÒµÑ´ª¹Ô´ autograft
é
໚¹ä»Í‹ҧÁÕ»ÃÐÊÔ·¸ÔÀÒ¾ÁÒ¡¢Ö¹ â´ÂÊÒÁÒöà¾ÔÁ»ÃÔÁÒ³à«ÅÅãËŒà¾Õ§¾Í·Õ¨Ð¤ÅØÁ¼ÔÇ¡ÃШ¡µÒ
é è è
·Ñ§ËÁ´ä´Œ áÅÐã¹¡Ã³Õ allograft ¡ÒÃà¾ÒÐàÅÕ§à«Åš͹¹íÒä»»ÅÙ¡¶‹Ò¨зíÒãËŒâÍ¡ÒÊà¡Ô´»¯Ô¡ÃÂÒ
é é ‹ ÔÔ
µ‹ÍµŒÒ¹ (graft rejection) ¹ŒÍ¡NjҡÒü‹ÒµÑ´áººà´ÔÁ à¹×ͧ¨Ò¡à«ÅÅ·¹ÒÁÒ»ÅÙ¡¶‹ÒÂÁÕà¾Õ§à«ÅÅ
è Õè í
ªÑ¹¼ÔÇ෋ҹѹ
é é
¡ÒÃà¾ÒÐàÅÕé§áÅлÅÙ¡¶‹ÒÂà«ÅÅÁÕÃÒ§ҹ¤ÃÑé§áá㹻‚ ¤.È. 1997 ·Õè»ÃÐà·ÈÍÔµÒÅÕ
¨Ò¡ÃÒ§ҹµ‹Ò§»ÃÐà·È¾ºÇ‹Ò»ÃÐʺ¼ÅÊíÒàÃ稻ÃÐÁҳÌÍÂÅÐ 75(5) áÅÐãËŒ¼Å´Õ¡Ç‹Ò¡ÒûÅÙ¡¶‹ÒÂ
à«ÅÅâ´ÂµÃ§ ʋǹ㹻ÃÐà·Èä·Â ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅâ´Â¤ÇÒÁËÇÁÁ×ͧ͢ÀÒ¤ÇÔªÒ
ÔÔ
¨Ñ¡ÉØÇ·ÂÒ ÀÒ¤ÇÔªÒÇÔ·ÂÒÀÙÁ¤Á¡Ñ¹ ÀÒ¤ÇÔªÒ¾ÂÒ¸ÔÇ·ÂÒ áÅÐÈÙ¹Âà¹×ÍàÂ×ͪÕÇÀÒ¾¡ÃØ§à·¾Ï ä´Œ·Ò¡ÒÃ
Ô Ô ØŒ Ô é è í
à¾ÒÐàÅÕ§ corneal limbal stem cell ã¹ËŒÍ§»®Ôºµ¡ÒÃáÅлÅÙ¡¶‹ÒÂãˌᡋ¼»Ç·ѧ allograft áÅÐ
é Ñ Ô ÙŒ † é
autograft ÊíÒàÃç¨à»š¹¤Ãѧáá㹻ÃÐà·Èä·Âã¹»‚ ¾.È. 2550 â´Âä´Œ¼ÒµÑ´·íÒ cultivated corneal epithelial
é ‹
transplantation ·Ñ§ËÁ´ÃÇÁ 14 ÃÒÂ
é
¨Ò¡¡ÒõÃǨµÔ´µÒÁ¼ÙŒ»†Ç¾ºÇ‹ÒÁÕ¡ÒÃÍÑ¡àʺ¢Í§µÒŴŧ à«ÅÅ·Õè»ÅÙ¡¶‹ÒÂÊÒÁÒö
¤§ÊÀÒ¾ÍÂÙä´Œâ´ÂäÁ‹ËÅØ´ÅÍ¡ ¼Å¡ÒõÃǨÊͺ·Ò§¾ÂÒ¸ÔÇ·ÂÒ·Õè 1 à´×͹ËÅѧ¼‹ÒµÑ´ ¾ºÇ‹ÒäÁ‹Áà«ÅÅ
‹ Ô Õ
¢Í§àÂ×ͺصÒÃØ¡ÅéÒࢌÒÁÒ㹺ÃÔàdz¢Í§¡ÃШ¡µÒ ¡Ò÷íÒઋ¹¹Õ໚¹¡ÒÃàµÃÕÂÁ¤ÇÒÁ¾ÃŒÍÁãËŒ¡ÃШ¡µÒ
è í é
à¾×Íà¾ÔÁâÍ¡Òʷըм‹ÒµÑ´à»ÅÕ¹¡ÃШ¡µÒãËŒ»ÃÐʺ¤ÇÒÁÊíÒàÃç¨ã¹Í¹Ò¤µÊÙ§¢Ö¹
è è è è é
Mucosal epithelial cell culture
㹼ٻǷÕÁ¾ÂÒ¸ÔÊÀÒ¾¢Í§µÒ·Ñ§Êͧ¢ŒÒ§ ઋ¹¡ÅØÁÍÒ¡Òà Stevens Johnson ËÃ×͵ҷѧÊͧ
Œ † è Õ é ‹ é
¢ŒÒ§ä´ŒÃºÍѹµÃÒ¨ҡÊÒÃà¤ÁÕ ËÒ¡¨íÒ໚¹µŒÍ§·íÒ cultivated corneal epithelial transplantation á¾·Â
Ñ
¨ÐäÁ‹ÊÒÁÒö·íÒâ´Â㪌à«ÅŢͧ¼Ù»ÇÂàͧ䴌 µŒÍ§ãªŒà»š¹ allograft «Ö§¾º»˜ËÒÇ‹ÒÂѧ¨íÒ໚¹µŒÍ§ãªŒÂÒ
Œ † è
¡´ÀÙÁµÒ¹·Ò¹ áÅÐÂѧÁÕâÍ¡ÒÊà¡Ô´ graft rejection ä´Œ ´Ñ§¹Ñ¹ ¨Ö§ÁÕ¤ÇÒÁ¾ÂÒÂÒÁ·Õ¨Ð¹íÒà«ÅÅ͹
Ô Œ é è ×è
¢Í§¼Ù»ÇÂÁÒ㪌᷹à«ÅÅ¡ÃШ¡µÒà¾×ÍËÅÕ¡àÅÕ§»˜ËÒ¹Õé
Œ † è è
à«ÅŢͧàÂ×ͺػҡ (oral mucosal epithelium) ¾ºÇ‹Ò໚¹à«ÅÅ·àËÁÒÐÊÁ à¹×ͧ¨Ò¡ÁÕšɳÐ
è Õè è Ñ
¢Í§ differentiation µèÒ áº‹§à«ÅÅàÃçÇ äÁ‹ÁÕ keratin áÅÐÁÕ¤ÇÒÁªØÁª×¹àÁ×͹íÒÁÒà¾ÒÐàÅÕ§º¹àÂ×Íá
í ‹ é è é è
ÅѡɳРrugae ¢Í§ mucosa ¨ÐËÒÂä» áÅÐÁÕšɳÐà«ÅŤŌÒ corneal epithelium ´Ñ§¹Ñ¹ Kinoshita
Ñ é
áÅФ³Ð ¨Ö§ä´Œ¹Òà«ÅŢͧàÂ×ͺػҡÁÒ㪌»ÅÙ¡¶‹Ò·յҼٻÇ àÃÕÂ¡Ç‹Ò cultivated oral mucosal
(6)
í è è Œ †
epithelial transplantation (COMET) «Ö§ÃÒÂ§Ò¹Ç‹Ò ÊÒÁÒö·íÒãˌŴ¡ÒÃÍÑ¡àÊºã¹µÒ Å´àÊŒ¹àÅ×Í´·Õè
è
¡ÃШ¡µÒ ÃÑ¡ÉÒÊÀÒ¾¼ÔÇãËŒ¤§·¹ äÁ‹à¡Ô´á¼Å¶ÅÍ¡ ᵋÍ‹ҧäáçµÒÁ à¹×ͧ¨Ò¡à«ÅŢͧàÂ×ͺػҡ¹Õé
è è
65.
38 Cultivated Epithelial Cell in Ophthalmology, When and How?
äÁ‹ãª‹à«ÅŢͧ¡ÃШ¡µÒàÁ×èÍ»ÅÙ¡¶‹ÒÂà«ÅÅáÅŒÇ ÊÑ¡ÃÐÂÐ˹Ö觨ÐÁÕàÊŒ¹àÅ×Í´¡ÅѺࢌÒÁÒã¹µÒã¹Ê‹Ç¹
periphery 䴌
ÀÒ¤ÇԪҨѡÉØÇ·ÂÒ ÀÒ¤ÇÔªÒÀÙÁ¤Á¡Ñ¹ áÅÐÀÒ¤ÇÔªÒ¾ÂÒ¸ÔÇ·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª
Ô Ô ØŒ Ô ÔÔ
¾ÂÒºÒÅ ä´ŒàÃÔÁ§Ò¹ÇԨ¹յ§áµ‹»‚ ¾.È. 2552 ä´Œ·Ò¡Òü‹ÒµÑ´ãˌᡋ¼»Ç 䴌¼ÒµÑ´·Ñ§ËÁ´ 6 ÃÒÂ
è Ñ é Ñé í ÙŒ † ‹ é
7 µÒ
¡ÒÃà¾ÒÐàÅÕé§à«ÅÅ
¡ÒÃà¾ÒÐàÅÕé§ corneal limbal stem cell
ã¹áµ‹ÅÐÃÒ§ҹÁÕǸà¾ÒÐàÅÕ§·Õᵡµ‹Ò§¡Ñ¹ ẋ§à»š¹ 2 ẺãË‹æ 䴌ᡋ explants culture
ÔÕ é è
system «Ö§¤×Í¡ÒÃÇÒ§ªÔ¹à¹×Í·ÕÁà«ÅÅ·§ªÔ¹º¹àÂ×Íá (amniotic membrane)(7-10) ËÃ×Í substrate Í×¹
è é é è Õ Ñé é è è
ઋ¹ fibrin gel ¡Ñº suspension culture system(11-14) «Ö§¨Ð‹ÍÂà«ÅÅãˌ໚¹à«ÅÅà´ÕÂÇæ ¡‹Í¹ áŌǨ֧
è è
ÇÒ§à«Åź¹ substrate ËÃ×Í amniotic membrane «Ö§ã¹ºÒ§ÃÒ§ҹ¨Ð㪌 3T3 feeder layer ໚¹µÑÇ
è
¡ÃеعãËŒà«ÅÅâµä´ŒàÃçÇ ¡ÒùíÒ amniotic membrane ÁÒ㪌 à¹×ͧ¨Ò¡ amniotic membrane ÁÕ growth
Œ è
factor µ‹Ò§æ ·ÕªÇÂãËŒà«ÅÅà¨ÃÔàµÔºâµä´Œ´Õ
è ‹ (15)
·Õ褳Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒŠʋǹ¡ÒÃà¾ÒÐàÅÕé§à«ÅŹÑé¹à¾ÒÐàÅÕ駺¹ amniotic
membrane áÅÐÁÕ¢¹µÍ¹´Ñ§µ‹Í仹Õé
Ñé
¡ÒÃà¾ÒÐàÅÕé§ corneal limbal stem cell
໚¹¡ÒÃàÅÕ§à«ÅÅẺ explants â´Â¹íÒ limbal tissue ·ÕÂÍ´ŒÇ dispase ÁÒàÅÕ§º¹àÂ×Í
é è ‹ é è
á amniotic membrane (AM) ·Õ¢´ epithelium cell ÍÍ¡ËÁ´ àÅÕ§ã¹ÍÒËÒÃàÅÕ§à«ÅÅ (keratinocyte
è Ù é é
growth medium: KGM) à¾ÒÐàÅÕ§㹠CO2 incubator ÍسËÀÙÁÔ 37 C ÀÒÂ㵌ÊÀÒÇзÕÁ¡Ò«¤Òú͹
é í è Õ
ä´ÍÍ¡ä«´ÃÍÂÅÐ 5 ໚¹àÇÅÒ 2-3 ÊÑ»´ÒË
Œ
¡Ò÷´Êͺ¤Ø³ÊÁºÑµ¤ÇÒÁ໚¹à«Åŵ¹¡íÒà¹Ô´¢Í§à¹×ÍàÂ×Í·Õà¾ÒÐàÅÕ§¹Õ´ÇÂÇÔ¸·Ò§¾ÂÒ¸ÔÇ·ÂÒ
Ô Œ é è è é é Œ Õ Ô
â´Â ¡ÒÃÂŒÍÁÊÕ hematoxylin & eosin (H&E) áÅÐÈÖ¡ÉҤسÊÁºÑµ¢Í§ epithelial differentiation marker
Ô
(cytokeration K (CK) 12 and CK3) áÅÐ stem cell marker (ABCG2) ´ŒÇÂÇÔ¸Õ reverse transcription-
polymerase chain reaction (RT-PCR) áÅÐ immunoperoxidase áÅŒÇÈÖ¡ÉÒÇ‹Òà«ÅÅ·àÅÕ§䴌Á¤³ÊÁºÑµÔ
Õè é Õ Ø
¢Í§â¤Ã§ÊÌҧáÅÐá͹µÔਹ¤ÅŒÒ¡Ѻ corneal limbal stem cell ËÃ×ÍäÁ‹ «Ö§Åѡɳдѧ¡Å‹ÒǤ×Í
è
1. à«ÅÅÁûËҧ¤‹Í¹¢ŒÒ§¡ÅÁ¶Ö§àËÅÕÂÁ «ÑÂâµ¾ÅÒÊÁµÔ´ÊÕá´§ ¹ÔÇà¤ÅÕÂʵԴÊÕ¹Òà§Ô¹â»Ã‹§
ÕÙ è éí
àÁ×ÍÂŒÍÁ´ŒÇÂÊÕ H&E (ÀÒ¾·Õè 2)
è
2. ÂŒÍÁµÔ´á͹µÔਹ p63, AE1/AE5 «Ö§áÊ´§Ç‹Òà«ÅÅÁ¤³ÊÁºÑµà»š¹ stem cell áÅÐÂŒÍÁ
è Õ Ø Ô
µÔ´ CK12 㹪ѹº¹¢Í§à«ÅÅ áÊ´§Ç‹Òà«ÅÅ·à¾ÒÐàÅÕ§໚¹à«ÅŢͧ corneal epithelium(16-18)
é Õè é
3. à«ÅÅ·à¾ÒÐàÅÕ§ÀÒÂ㵌ÊÀÒÇдѧ¡Å‹ÒÇàÁ×Í·´ÊͺÇÔ¸Õ RT-PCR ¾ºÇ‹ÒÁÕ¡ÒÃáÊ´§ÍÍ¡¢Í§
Õè é è
ABCG2 CK 3 áÅÐ CK12 «Ö§Â×¹ÂѹNjÒ໚¹à«ÅŢͧ¡ÃШ¡µÒ·Õ·Ò˹ŒÒ·Õ໚¹ stem cell
è è í è
66.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 39
ÀÒ¾·Õè 2 áÊ´§ÀÒ¾·Ò§¾ÂÒ¸ÔÇÔ·ÂÒ ¢Í§¡ÒÃà¾ÒÐàÅÕé§ Corneal Limbal stem cell : (A) ÂŒÍÁÊÕ
H&E, (B) ÂŒ Í Á immunohistochemistry áÊ´§¶Ö § á͹µÔ à ¨¹·Õè á Ê´§ÍÍ¡ áÅÐ
äÁ‹áÊ´§ÍÍ¡º¹¼ÔÇà«ÅÅ ÂŒÍÁ p63 áÊ´§¶Ö§¡ÒÃ໚¹ stem cell, (C) ÂŒÍÁ CK12
µÔ ´ à«ÅÅ ªÑé ¹ º¹ áÊ´§¶Ö § à«ÅÅ ·Õè á º‹ § µÑ Ç à¨ÃÔ àµÔ º âµä´Œ à »š ¹ à«ÅÅ ¢ ͧ corneal
epithelium
¡ÒÃà¾ÒÐàÅÕé§ oral mucosal epithelium
´íÒà¹Ô¹¡ÒÃà¾ÒÐàÅÕ§ human oral mucosal epithelial cell ã¹ÍÒËÒÃàÅÕ§à«ÅÅã¹ÊÀÒÇзÕäÁ‹
é é è
ÁÕ serum áÅÐ feeder cell ໚¹àÇÅÒ 2-3 ÊÑ»´ÒË áÅŒÇÈÖ¡ÉҤسÊÁºÑµ¢Í§ epithelial differentiation
Ô
marker (cytokeration K (CK) 12 and CK3) áÅÐ stem cell marker (ABCG2) ´ŒÇÂÇÔ¸Õ reverse
transcription-polymerase chain reaction (RT-PCR) à«ÅÅ·à¾ÒÐàÅÕ§ÀÒÂ㵌ÊÀÒÇдѧ¡Å‹ÒÇÁÕ¡ÒÃ
Õè é
áÊ´§ÍÍ¡¢Í§ CK3 áÅÐ ABCG2 ᵋäÁ‹áÊ´§ÍÍ¡¢Í§ CK12 «Ö§áÊ´§Ç‹Ò໚¹à«ÅÅ·¤ÅŒÒ¡ÃШ¡µÒ
è Õè
ᵋäÁ‹ãª‹à«ÅŢͧ¡ÃШ¡µÒ
¡Ò÷íÒ¼‹ÒµÑ´á¡‹¼ÙŒ»†ÇÂ
¡Ò÷íÒ¼‹ÒµÑ´ CCET áÅÐ COMET ÁÕËÅÑ¡¡ÒÃà´ÕÂǡѹ¤×Í ÅÍ¡¾Ñ§¼×´·Õ¤ÅØÁ ocular surface
è
ÍÍ¡ ·Ñ§ã¹Ê‹Ç¹¢Í§ cornea áÅÐ conjunctiva ÇÒ§¹éÒÂÒ 0.02% mitomycin C à¾×Í»‡Í§¡Ñ¹¡ÒáÅѺ
é í è
໚¹«éҢͧ¾Ñ§¼×´ ¨Ò¡¹Ñ¹ÇÒ§àÂ×Íá·ÕÁà«ÅŢͧ corneal epithelium ËÃ×Í oral mucosal epithelium
í é è è Õ
ÍÂÙ‹ àÂ纵Դ¡Ñº sclera áÅÐ cornea ʋǹ·ÕÅÍ¡¾Ñ§¼×´ÍÍ¡áÅŒÇ(6-8, 10, 19,20) «Ö§¨Ð¾ºÇ‹ÒÊÒÁÒö·íÒãËŒÁÕ
è è
à«ÅŤÅØÁá¼Åä´Œ·§ËÁ´ËÃ×Íà¡×ͺ·Ñ§ËÁ´µÑ§áµ‹ËÅѧ¼‹ÒµÑ´ ã¹ÃÒ·Õà¹×Í¡ÃШ¡µÒ¢Ø¹ ËÅѧ¨Ò¡á¼ÅµÔ´´Õ
Ñé é é è é ‹
¡ÒÃÍÑ¡àʺŴŧ ᵋ¡ÃШ¡µÒÂѧ¢Ø¹ÍÂÙ‹ ¨Ð·íÒ¡ÒÃà»ÅÕ¹¡ÃШ¡µÒµ‹Íä»
‹ è
àǪÈÒʵ÷¹Âؤ 2553
Ñ 41
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Li DQ, Tseng SC. Differential regulation of keratinocyte growth factor and hepatocyte growth factor/scatter
factor by different cytokines in human corneal and limbal fibroblasts. J Cell Physiol. 1997;172(3):361-72.
2. Dua HS, Azuara-Blanco A. Limbal stem cells of the corneal epithelium. Surv Ophthalmol. 2000;44(5):415-25.
3. Puangsricharern V, Tseng SC. Cytologic evidence of corneal diseases with limbal stem cell deficiency.
Ophthalmology. 1995;102(10):1476-85.
4. Prabhasawat P. Corneal limbal stem cells. Siriraj Med J. 2006;58:728-9.
5. Shortt AJ, Secker GA, Notara MD, Limb GA, Khaw PT, Tuft SJ, et al. Transplantation of ex vivo cultured limbal
epithelial stem cells: a review of techniques and clinical results. Surv Ophthalmol. 2007;52(5):483-502.
6. Nakamura T, Inatomi T, Sotozono C, Amemiya T, Kanamura N, Kinoshita S. Transplantation of cultivated
autologous oral mucosal epithelial cells in patients with severe ocular surface disorders. Br J Ophthalmol. 2004
;88(10):1280-4.
7. Koizumi N, Inatomi T, Suzuki T, Sotozono C, Kinoshita S. Cultivated corneal epithelial stem cell transplantation
in ocular surface disorders. Ophthalmology. 2001;108(9):1569-74.
8. Nakamura T, Inatomi T, Sotozono C, Koizumi N, Kinoshita S. Successful primary culture and autologous
transplantation of corneal limbal epithelial cells from minimal biopsy for unilateral severe ocular surface disease.
Acta Ophthalmol Scand. 2004;82(4):468-71.
9. Grueterich M, Espana EM, Touhami A, Ti SE, Tseng SC. Phenotypic study of a case with successful
transplantation of ex vivo expanded human limbal epithelium for unilateral total limbal stem cell deficiency.
Ophthalmology. 2002;109(8):1547-52.
10. Sangwan VS, Matalia HP, Vemuganti GK, .atima A, Ifthekar G, Singh S, et al. Clinical outcome of autologous
cultivated limbal epithelium transplantation. Indian J Ophthalmol. 2006;54(1):29-34.
11. Daya SM, Watson A, Sharpe JR, Giledi O, Rowe A, Martin R, et al. Outcomes and DNA analysis of ex vivo
expanded stem cell allograft for ocular surface reconstruction. Ophthalmology. 2005;112(3):470-7.
12. Nakamura T, Inatomi T, Sotozono C, Ang LP, Koizumi N, Yokoi N, et al. Transplantation of autologous serum-
derived cultivated corneal epithelial equivalents for the treatment of severe ocular surface disease. Ophthalmology.
2006;113(10):1765-72.
13. Pellegrini G, Traverso CE, .ranzi AT, Zingirian M, Cancedda R, De Luca M. Long-term restoration of damaged
corneal surfaces with autologous cultivated corneal epithelium. Lancet. 1997;349(9057):990-3.
14. Rama P, Bonini S, Lambiase A, Golisano O, Paterna P, De Luca M, et al. Autologous fibrin-cultured limbal
stem cells permanently restore the corneal surface of patients with total limbal stem cell deficiency. Transplantation.
2001;72(9):1478-85.
15. Prabhasawat P, Tseng SC. Impression cytology study of epithelial phenotype of ocular surface reconstructed
by preserved human amniotic membrane. Arch Ophthalmol. 1997;115(11):1360-7.
16. Kawasaki S, Tanioka H, Yamasaki K, Connon CJ, Kinoshita S. Expression and tissue distribution of p63
isoforms in human ocular surface epithelia. Exp Eye Res. 2006;82(2):293-9.
17. Paladino G, Marino C, La Terra Mule S, Civiale C, Rusciano D, Enea V. Cytokeratin expression in primary
epithelial cell culture from bovine conjunctiva. Tissue Cell. 2004;36(5):323-32.
18. Kasper M, Moll R, Stosiek P, Karsten U. Patterns of cytokeratin and vimentin expression in the human eye.
Histochemistry. 1988;89(4):369-77.
69.
42 Cultivated Epithelial Cell in Ophthalmology, When and How?
19. Tsai RJ, Li LM, Chen JK. Reconstruction of damaged corneas by transplantation of autologous limbal
epithelial cells. N Engl J Med. 2000;343(2):86-93.
20. Kinoshita S, Koizumi N, Nakamura T. Transplantable cultivated mucosal epithelial sheet for ocular surface
reconstruction. Exp Eye Res. 2004;78(3):483-91.
70.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 43
5
¡ÒÃÃÑ¡ÉÒÀÒÇÐÊÒµҼԴ»¡µÔ´ŒÇ LASIK :
ÊÔ觹‹ÒÃÙŒ¹Í¡à˹×ͨҡ¡Ò÷íÒàÅÊÔ¡
(Beyond Lasik)
¼ÙŒª‹ÇÂÈÒʵÃÒ¨Òà¹ÒÂᾷ³ѰÇØ²Ô Ãʹ͹ѹµ
ÃͧÈÒʵÃÒ¨Òà¹ÒÂá¾·Âʺ§ ÈÃÕÇÃóºÙó
ÃͧÈÒʵÃÒ¨Òà¹ÒÂᾷ¹ÃÔÈ ¡Ô¨³Ã§¤
ÀÒ¤ÇԪҨѡÉØÇ·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ÔÔ
ÀÒÇÐÊÒµҼԴ»¡µÔ
ÀÒÇÐÊÒµҼԴ»¡µÔ ໚¹ÊÒà˵ØãËŒà¡Ô´ÍÒ¡ÒõÒÁÑÇ ·Õ¾ºä´ŒºÍÂã¹·Ø¡ÍÒÂØ áµ‹ÊÒÁÒö·íÒãËŒ
è ‹
ÁͧàËç¹ä´Œ´¢¹´ŒÇ¡ÒÃÊÇÁáÇ‹¹µÒ ¤Í¹á·¤àÅ¹Ê ËÃ×Í¡Ò÷íÒàÅÊÔ¡ ¡Ò÷ÕàÃÒ¨ÐÁͧàËç¹ä´Œª´à¨¹¹Ñ¹
Õ Öé è Ñ é
áʧ·ÕÊͧࢌҵҵŒÍ§¶Ù¡ÃÇÁáʧ¼‹Ò¹¡ÃШ¡µÒáÅÐàÅ¹ÊµÒ ËÃ×Íâ¿¡ÑÊáŌǵ¡Å§¾Í´Õ·¨ÍµÒ ¶ŒÒ¡ÒÃ
è‹ Õè
ÃÇÁáʧäÁ‹¾Í´Õ áʧ¨ÐäÁ‹ÃÇÁ·Õ¨ÍµÒ·íÒãËŒà¡Ô´ÀÒÇÐÊÒµҼԴ»¡µÔµÒ§æ 䴌ᡋ ÀÒÇÐÊÒµÒÊѹ ÊÒÂ
è ‹ é
µÒÂÒÇ áÅÐÊÒµÒàÍÕ§
ÊÒµÒÊÑé¹ (Myopia) à¡Ô´¨Ò¡¡íÒÅѧ¡ÒÃÃÇÁáʧ¢Í§µÒ·Õ·ÒãËŒ¨´â¿¡Ñʢͧáʧµ¡Å§Ë¹ŒÒ¨Í
è í Ø
µÒ ÍÒ¨à¡Ô´¨Ò¡ÅÙ¡µÒÂÒÇËÃ×Í¡ÃШ¡µÒÁÕ¤ÇÒÁ⤌§ÁÒ¡à¡Ô¹ä» ¼Ù·ÁÊÒµÒÊѹ¨Ö§ÁͧàËç¹ä´Œã¹ÃÐÂÐ
Œ Õè Õ é
ã¡ÅŒ ᵋ¨ÐÁͧäÁ‹ª´ã¹ÃÐÂÐä¡Å
Ñ
ÊÒµÒÂÒÇ (Hyperopia) à¡Ô´¨Ò¡¡íÒÅѧ¡ÒÃÃÇÁáʧ¢Í§µÒ ·Õ·ÒãËŒ¨´â¿¡Ñʢͧáʧµ¡Å§ËÅѧ
è í Ø
ËÃ×ÍàÅÂ¨ÍµÒ ÍÒ¨à¡Ô´¨Ò¡ÅÙ¡µÒÊѹËÃ×Í¡ÃШ¡µÒÁÕ¤ÇÒÁ⤌§áº¹à¡Ô¹ä» ¼Ù·ÁÊÒµÒÂÒǨ֧ÁͧäÁ‹ª´
é Œ Õè Õ Ñ
·Ñ§ã¹ÃÐÂÐã¡ÅŒËÃ×Íä¡Å ÀÒÇÐÊÒµÒÂÒǹÕäÁ‹ãª‹ª¹Ô´à´ÕÂǡѺÊÒµÒÂÒÇã¹¼ÙʧÍÒÂØ
é é ŒÙ
ÊÒµÒàÍÕ§ (Astigmatism) à¡Ô´¨Ò¡¡Ò÷աÒÅѧ¡ÒÃÃÇÁáʧ¢Í§µÒã¹á¡¹µ‹Ò§æäÁ‹à·‹Ò¡Ñ¹
è í
·íÒãËŒ¨´â¿¡ÑʢͧáʧäÁ‹¡ÅÁËÃ×ÍÁÕËÅÒ¨ش à¡Ô´¨Ò¡¡ÃШ¡µÒäÁ‹¡ÅÁ ÀÒÇйÕÍÒ¨à¡Ô´Ã‹ÇÁ¡ÑºÀÒÇÐÊÒÂ
Ø é
µÒÊѹ ËÃ×ÍÂÒÇä´Œ
é
ÊíÒËÃѺÀÒÇÐÊÒµÒÂÒÇã¹¼ÙʧÍÒÂØ (Presbyopia) äÁ‹ãª‹ÀÒÇÐÊÒµÒÂÒÇ»¡µÔ à¹×ͧ¨Ò¡à»š¹
Œ Ù è
ÀÒÇзÕà¡Ô´¨Ò¡¡ÒÃàÊ×ÍÁ¢Í§¡ÅŒÒÁà¹×Íã¹µÒ·Õ㪌㹡ÒûÃѺÃÐÂÐÁͧã¡ÅŒ-ä¡Å ·íÒãËŒÁͧã¡ÅŒäÁ‹ª´ «Ö§
è è é è Ñ è
ÀÒÇÐÊÒµÒÂÒÇã¹¼ÙʧÍÒÂع¨ÐàÃÔÁÁÕÍÒ¡ÒÃã¹¼Ù·ÁÍÒÂØ»ÃÐÁÒ³ 40 »‚¢¹ä»
ŒÙ Õé è Œ Õè Õ Öé
àǪÈÒʵ÷¹Âؤ 2553
Ñ 45
¼Ù·Á»ÃÐÇѵàË繨ش´íÒÅÍÂä»ÁÒ àËç¹áʧ¤ÅŒÒ¿‡Òáź ËÃ×Íà¤ÂÁը͵ÒËÅØ´ÅÍ¡ÁÒ
Œ Õè Õ Ô
¡‹Í¹ã¹µÒÍÕ¡¢ŒÒ§
- ÀÒÇШ͵ÒÅÍ¡µÑÇ «Ö§äÁ‹àËÁÒСѺ¡Ò÷íÒàÅÊÔ¡
è
- ÀÒÇТͧ¨ÍµÒÍ×¹æ ·ÕÍÒ¨à¡ÕÂÇ¢ŒÍ§¡Ñº¨ÍµÒÅÍ¡µÑÇ àª‹¹ white without pressure,
è è è
cobble stone degeneration
¡ÒÃà¾ÔÁ¤ÇÒÁ´Ñ¹µÒã¹ÃÐËÇ‹Ò§¢Ñ¹µÍ¹¡Ò÷íÒàÅÊÔ¡ÍÒ¨·íÒãËŒÁ¡ÒÃË´ËÃ×Í¢ÂÒµÑǢͧÇعµÒ
è é Õ Œ
(vitreous) «Ö§ÍÒ¨·íÒãËŒÁ¡Òô֧Ãѧ¨ÍµÒáÅÐà¡Ô´¤ÇÒÁ¼Ô´»¡µÔ·¨ÍµÒä´Œ
è Õ é Õè
ÀÒÇФÇÒÁ´Ñ¹µÒÊÙ§ áÅÐâ䵌ÍËÔ¹
µŒÍËÔ¹¤×Í¡ÅØÁâä·Õ·ÒãËŒà¡Ô´¤ÇÒÁ¼Ô´»Ã¡µÔ¢Í§¢ÑÇ»ÃÐÊÒ·µÒ (optic disc) â´Âà¡ÕÂÇ¢ŒÍ§¡Ñº
‹ è í é è
¤ÇÒÁ´Ñ¹µÒ (intraocular pressure) ËÃ×Í¡ÒÃÊÙàÊÕÂÅÒ¹ÊÒÂµÒ (visual field) ¤ÇÒÁ´Ñ¹µÒ¢Í§¤¹»¡µÔ
¨ÐäÁ‹à·‹Ò¡Ñ¹ áÅÐÁÕ¡ÒÃà»ÅÕ¹á»Å§¢Ö¹Å§ä´ŒµÒÁàÇÅÒµ‹Ò§æ ¢Í§Çѹ (diurnal variation) â´Â·ÑÇ令ÇÒÁ
è é è
´Ñ¹µÒ¨ÐäÁ‹à¡Ô¹ 21 ÁÔÅÅÔàÁµÃ»ÃÍ· ᵋ¤¹»¡µÔºÒ§¤¹ÍÒ¨ÁÕ¤ÇÒÁ´Ñ¹µÒÊÙ§¡Ç‹Ò¹Õé ᵋäÁ‹ä´Œ·ÒãËŒà¡Ô´ í
¤ÇÒÁ¼Ô´»¡µÔ¢Í§¢ÑÇ»ÃÐÊÒ·µÒËÃ×ÍÅÒ¹ÊÒµҡç¨ÐäÁ‹¶ÍÇ‹Ò໚¹â䵌ÍËÔ¹ ᵋ໚¹ÀÒÇФÇÒÁ´Ñ¹µÒÊÙ§
é ×
(ocular hypertension) áÅÐÂѧÁÕ¼»ÇÂÍÕ¡¡ÅØÁ·ÕáÁŒ¤ÇÒÁ´Ñ¹µÒÂѧäÁ‹Ê§à¡Ô¹¤‹Ò»¡µÔᵋ¢Ç»ÃÐÊÒ·µÒ
ÙŒ † ‹ è Ù Ñé
¡ç¶Ù¡·íÒÅÒ ÅÒ¹ÊÒµÒ᤺ŧ ¼ÙŒ»†ÇµŒÍËÔ¹¡ÅØ‹Á¹ÕéàÃÕÂ¡Ç‹Ò à»š¹â䵌ÍËÔ¹ª¹Ô´¤ÇÒÁ´Ñ¹µÒäÁ‹ÊÙ§
(normal tension glaucoma) »˜¨¨ÑÂàÊÕ§¢Í§â䵌ÍËÔ¹»ÃСͺ´ŒÇ¼ٷÁ»ÃÐÇѵÁÒµÔ໚¹µŒÍËÔ¹ ¼Ù·Õè
è Œ Õè Õ Ô Õ Œ
ÁÕÊÒµÒÊѹËÃ×ÍÂÒÇÁÒ¡æ ¼Ù»ÇÂàºÒËÇÒ¹ áÅмÙʧÍÒÂØ ¹Í¡¨Ò¡¹Õ§ÁÕµÍËÔ¹ª¹Ô´·ØµÂÀÙÁÔ (secondary
é Œ † ŒÙ éÑ Œ Ô
glaucoma) ¤×Í µŒÍËÔ¹·Õà¡Ô´¨Ò¡ÊÒà˵Ø͹ 䴌ᡋ ÀÒÇÐàºÒËÇÒ¹¢Ö¹¨ÍµÒ (proliferative diabetic
è ×è é
retinopathy) Íغµà˵طҧµÒµ‹Ò§æ ¡ÒõԴàª×ÍËÃ×Í¡ÒÃÍÑ¡àÊºã¹µÒ (uveitis) ¡ÒÃ㪌ÂÒ¡ÅØÁÊàµÕÂÃÍ´
Ñ Ô é ‹
(steroid induced glaucoma) µÅÍ´¨¹â䵌͡ÃШ¡ (phacomorphic glaucoma, phacolytic glaucoma)
¼Ù·ÁÀÒÇФÇÒÁ´Ñ¹µÒÊÙ§ ËÃ×Íâ䵌ÍËÔ¹ äÁ‹àËÁÒзըзíÒàÅÊÔ¡ à¹×ͧ¨Ò¡ã¹ÃÐËÇ‹Ò§¡Ãкǹ
Œ Õè Õ è è
¡Ò÷íÒàÅÊÔ¡·Õ¨Ð·íÒ¡ÒÃᡪѹ¡ÃШ¡µÒ·Ñ§´ŒÇÂãºÁÕ´ (microkeratome) ËÃ×Í .emtoSecond Laser
è é é
¨Ð·íÒãËŒ¤ÇÒÁ´Ñ¹ÀÒÂã¹µÒÊÙ§¢Ö¹ªÑǤÃÒÇ ªÖ§ÍÒ¨·íÒãËŒÁ¡Ò÷íÒÅÒ¢ÑÇ»ÃÐÊÒ·µÒÁÒ¡¢Ö¹ä´Œ Í‹ҧäÃ
é è è Õ é é
¡çµÒÁ¡ÒÃᡪѹ¡ÃШ¡µÒ´ŒÇ .emtoSecond Laser ÍÒ¨à¾ÔÁ¤ÇÒÁ´Ñ¹µÒ¹ŒÍ¡NjÒàÁ×Íà·Õº¡Ñº¡ÒÃ
é è è
㪌 microkeratome ÀÒÂËÅѧ¡Ò÷íÒàÅÊÔ¡¡ÃШ¡µÒ¨ÐºÒ§Å§·íÒãËŒ¡ÒÃÇÑ´¤‹Ò¤ÇÒÁ´Ñ¹µÒà»ÅÕ¹á»Å§ è
ä´Œ â´Â¨Ðä´Œ¤Ò¤ÇÒÁ´Ñ¹µÒµèÒ¡Ç‹Ò¤ÇÒÁ໚¹¨ÃÔ§ ´Ñ§¹Ñ¹¡ÒõԴµÒÁ¡ÒÃÃÑ¡ÉÒµŒÍËԹ㹼ٷ·ÒàÅÊÔ¡¨Ð
‹ í é Œ Õè í
·íÒä´ŒÂÒ¡¢Ö¹ é
73.
46 ¡ÒÃÃÑ¡ÉÒÀÒÇÐÊÒµҼԴ»¡µÔ´Ç Lasik : ÊÔ§¹‹ÒÃٹ͡à˹×ͨҡ¡Ò÷íÒàÅÊÔ¡
Œ è Œ
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Hyams SW, Neumann E. Peripheral retina in myopia. With particular reference to retinal breaks. Br J Ophthalmol
1969;53(5):300-6.
2. Mirshahi A, Schopfer D, Gerhardt D, et al. Incidence of posterior vitreous detachment after laser in situ
keratomileusis. Graefes Arch Clin exp Ophthalmol 2006;244:149-53.
3. Hernandez-Verdejo JL, Teus MA, Roman JM, Boliver G. Porcine model to compare real-time intraocular
pressure during LASIK with a mechanical microkeratome and femtosecond laser. Invest Ophthalmol Vis Sci
2007;48:68-72.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 49
3. Murphree AL. Intraocular retinoblastoma: The case for a new group classification. Ophthalmol Clin North Am
2005;18:41–53.
4. Chantada G, Doz ., Antoneli CB, et al. A proposal for an international retinoblastoma staging system. Pediatr
Blood Cancer 2006;47:801-5.
5. Atchaneeyasakul LO, Wongsiwaroj C, Uiprasertkul M, Sanpakit K, Thephamongkhol K, Trinavarat A. Prognostic
factors and treatment outcomes of retinoblastoma in pediatric patients: a single-institution study. Jpn J Ophthalmol
2009;53:35-9.
6. Murphree AL, Villablanca JG, Deegan W. 3rd, et al. Chemotherapy plus local treatment in the management
of intraocular retinoblastoma. Arch Ophthalmol 1996;114:1348-56.
7. RamaChandran S, Ariffin H. Secondary acute myeloid leukemia after etoposide therapy for haemophagocytic
lymphohistiocytosis. Pediatr Blood Cancer 2009;53:488-90.
8. Chan HS, DeBoer G, Thiessen JJ, et al. Combining cyclosporin with chemotherapy controls intraocular
retinoblastoma without requiring radiation. Clin Cancer Res 1996;2:1499-508.
9. Colombo D, .lori L, Altomare G, Aste N, Sgarbi S. Clinical outcome evaluation following cyclosporine a
treatment in moderate to severe psoriasis: a retrospective study. Int J Immunopathol Pharmacol 2010; 23:363-
7.
10. Kaneko A, Suzuki S. Eye-preservation treatment of retinoblastoma with vitreous seeding. Jpn J Clin Oncol
2003; 33:601-7.
11. Abramson DH, .rank CM, Dunkel IJ. A phase I/II study of subconjunctival carboplatin for intraocular
retinoblastoma. Ophthalmology 1999; 106:1947-50.
12. Yamane T, Kaneko A, Mohri M. The technique of ophthalmic arterial infusion therapy for patients with
intraocular retinoblastoma. Int J Clin Oncol 2004; 9:69-73.
64 âäàª×ÍÃÒ·Õ¼Ç˹ѧªÑ¹ÅÖ¡
é è Ô é
1. ÃÍÂâäÅѡɳÐ໚¹¡ŒÍ¹ (tumefaction)
2. à¡Ô´ÃÙ·ÐÅØÁ˹ͧÍÍ¡ÁÒ·ÕºÃÔàdz¼ÔǢͧÃÍÂâä (sinus drainage)
Õ è
3. µÃǨ¾º¡ÅØÁ¢Í§ÊÒÂÃÒ (grains) »¹ÁҡѺ˹ͧ¨Ò¡ÃÙᵡ·ÐÅØ
‹
ÃÍÂâäÁÑ¡¾ºä´Œº‹Í·ÕèºÃÔàdz à·ŒÒ, ¢Ò ËÃ×ÍÁ×Í «Öè§à»š¹µíÒá˹‹§·Õèà¡Ô´ºÒ´á¼Åä´Œº‹ÍÂ
ã¹ÃÍÂâä·Õ໚¹¹Ò¹æ ¨ÐÁÕ¡ÒÃÅÒÁä»·Õ¡Ãд١à¡Ô´à»š¹ osteomyelitis «Ö§¹íÒä»ÊÙ¤ÇÒÁ¾Ô¡ÒÃä´Œ ¼Ù»ÇÂ
è è è ‹ Œ †
ÁÑ¡äÁ‹ÁÍÒ¡ÒÃà¨çº ¹Í¡¨Ò¡¨ÐÁÕ¡ÒÃᵡ໚¹á¼Å·ÕºÃÔàdz¼ÔÇ˹ѧ«Ö§·íÒãËŒ¼»ÇÂÁÕÍÒ¡ÒÃà¨çºä´Œ
Õ è è ÙŒ † (1,3)
ÃÙ»·Õè 4 Åѡɳзҧ¤ÅÔ¹Ô¡¢Í§ mycetoma
¡ÒõÃǨ·Ò§ËŒÍ§»¯Ôºµ¡ÒÃ
Ñ Ô
ÊÒÁÒöµÃǨ¾º grain ·Õ»¹ÍÂÙã¹Ë¹Í§ºÃÔàdzÃÙà»´¢Í§á¼Å¨Ò¡µíÒá˹‹§ÃÍÂâä «Ö§ÊÒÁÒö
è ‹ è
àËç¹ä´Œ´ÇµÒà»Å‹ÒáÅжŒÒ¹íÒä»´Ù´Ç¡Ōͧ¨ØÅ·ÃÃȹ ¡ç¨ÐàË繡ÅØÁ¡ŒÍ¹¢Í§ÊÒÂÃÒ ¡ÒõÃǨªÔ¹à¹×Í
Œ Œ ‹ é é
¨Ò¡ºÃÔàdzÃÍÂâä à¾×Í´Ùšɳзҧ¨ØžÂÒ¸ÔÇ·ÂҨоº grain »¹ÍÂÙã¹Ê‹Ç¹¢Í§à¹×͵Ò ·ÕÁ¡ÒÃ
è Ñ Ô ‹ é è Õ
ÍÑ¡àʺẺá¡Ã¹ÙâÅÁÒËÇÁ¡ÑºÁÕ¹ÇâµÃ¿ÅÁÒÃÇÁ¡Ñ¹ (ÃÙ»·Õè 5) áÅÐÁÕ¾§¼×´ÅŒÍÁÃͺºÃÔàdz·ÕÁ¡ÒÃ
Ô Ñ è Õ
ÍÑ¡àʺ㹪ѹ˹ѧ᷌ â´Â¨ÐàËç¹ÊÒÂÃҪѴਹ¨Ò¡¡ÒÃÂŒÍÁ H&E áÅÐÊÒÁÒöŒÍÁ¾ÔàÈÉ´ŒÇ GMS
é
à¾×ÍáÊ´§ÊÒÂÃÒä´Œª´à¨¹¢Ö¹ ¡ÒÃà¾ÒÐàª×ͨЪ‹ÇÂ㹡ÒèíÒṡÊÒ¾ѹ¸Ø¢Í§àª×ÍÃÒ¡‹Íâä
è Ñ é é é
ÃÙ»·Õè 5 ÅѡɳСÅØ‹Á¢Í§ÊÒÂÃÒ (grain) ·ÕèµÃǨ¾ºã¹ÃÍÂâä;H&E x 100
àǪÈÒʵ÷¹Âؤ 2553
Ñ 73
¡ÒÃà¡Ô´»¯Ô¡ÃÂÒÃÐËÇ‹Ò§ÂÒ·Õ㪌·Ò§¨ÔµàǪ
ÔÔ è
âä·Ò§¨Ô µ àǪ໚ ¹ âä·Õè ÁÑ ¡ ¨ÐÁÕ ¡ ÒÃ㪌  ÒËÅÒª¹Ô ´ Ë Ç Á¡Ñ ¹ ઋ ¹ ÂÒµŒ Ò ¹«Ö Á àÈÃŒ Ò
(antidepressant) ËÇÁ¡ÑºÂÒ·Õ㪌áÉÒÍÒ¡Ò÷ҧ¨Ôµ (antipsychotics) ËÃ×ÍËÇÁ¡ÑºÂÒ¤ÅÒ¡ѧÇÅ¡ÅØÁ
è Ñ ‹
benzodiazepines ÂҴѧ¡Å‹ÒÇÍÒ¨à¡Ô´»¯Ô¡ÃÂÒÃÐËÇ‹Ò§ÂÒä´Œ¤Í¹¢ŒÒ§ÁÒ¡ µÑÇÍ‹ҧઋ¹ ÂÒ fluoxetine
ÔÔ ‹ (5)
·Õ໚¹ÂÒµŒÒ¹ÍÒ¡ÒëÖÁàÈÃŒÒ㹡ÅØÁ selective serotonin reuptake inhibitors (SSRIs) ·ÕÁ¡ÒÃ㪌¡¹
è ‹ è Õ Ñ
¤‹Í¹¢ŒÒ§ÁÒ¡ ᵋÂÒ¹ÕÁ¤³ÊÁºÑµà»š¹µÑÇÂѺÂѧ¡Ò÷íÒ§Ò¹¢Í§à͹ä«Á CYP2D6 ·Õ¤Í¹¢ŒÒ§áç áÅÐ
é Õ Ø Ô é è ‹
ÂѧÂѺÂÑ駡Ò÷íÒ§Ò¹¢Í§ CYP2C9 ÍÕ¡´ŒÇ àÁ×èÍ㪌ËÇÁ¡Ñº antipsychotics ઋ¹ haloperidol,
fluphenazine, perphenazine ¨Ð·íÒãËŒÃдѺÂÒ antipsychotics ã¹àÅ×Í´ÊÙ§¢Ö¹ÁÒ¡ ¨¹à¡Ô´ÍѹµÃÒÂá¡‹
é
¼Ù»ÇÂä´Œ
Œ †
º·ÊÃØ»
¡ÒÃà¡Ô´»¯Ô¡ÃÂÒÃÐËÇ‹Ò§ÂÒ·ÕÁ¤ÇÒÁÊíҤѷҧ¤ÅÔ¹¡¹Ñ¹ ÊÒÁÒöà¡Ô´ä´Œã¹¼Ù»Ç·ء»ÃÐàÀ·
ÔÔ è Õ Ô é Œ †
ºÒ§¤ÃÑé§ÍÒ¨ÁÕ¤ÇÒÁÃعá稹ÍҨ໚¹ÍѹµÃÒ¶֧ᡋªÕÇÔµ ᾷ¼ٌ㪌ÂÒ¤§äÁ‹ÊÒÁÒö·Õè¨Ð¨´¨íÒ
¤Ø³ÊÁºÑµ¢Í§ÂÒä´Œ·§ËÁ´ ᵋ¤ÇÃÃÐÁÑ´ÃÐÇѧàÁ×͵ŒÍ§ãªŒÂÒ㹡óմ§¹Õé
Ô Ñé è Ñ
1. ¼Ù»ÇÂÊÙ§ÍÒÂØ à¹×ͧ¨Ò¡¼Ù»Ç¡ÅØÁ¹ÕÁâÍ¡ÒÊ䴌úÂÒËÇÁ¡Ñ¹ËÅÒª¹Ô´ áÅФÇÒÁÊÒÁÒö
Œ † è Œ † ‹ é Õ Ñ
㹡ÒÃà»ÅÕ¹á»Å§áÅТ¨Ñ´ÂÒÅ´¹ŒÍÂŧ
è
2. ¼ÙŒ»†Ç·Õè㪌ÂÒËÅÒª¹Ô´Ã‹ÇÁ¡Ñ¹ ¼ÙŒ»†ÇºҧÃÒÂÁÕâä»ÃШíÒµÑÇËÅÒÂâä µŒÍ§¾ºá¾·Â
ËÅÒ·‹Ò¹ ËÅÒÂá¼¹¡ ·íÒãˌ䴌úÂÒËÅÒª¹Ô´ ´Ñ§¹Ñ¹¨Ö§¤ÇÃÁÕ¡Ò÷º·Ç¹ÂÒ·Õ㪌ÃÇÁ¡Ñ¹ÍÂÙÍ‹ҧÊÁèÒ
Ñ é è ‹ ‹ í
àÊÁÍ
3. ÂÒ·ÕÁ´ª¹Õ¡ÒÃÃÑ¡ÉÒ᤺ (narrow therapeutic index) ÂÒ㹡ÅØÁ¹Õé ËÒ¡ÁÕÃдѺÂÒ·Õʧ¡Ç‹Ò
è Õ Ñ ‹ èÙ
ÃдѺ¡ÒÃÃÑ¡ÉÒà¾Õ§àÅ硹ŒÍ¡çÍÒ¨·íÒãËŒà¡Ô´ÍѹµÃÒÂá¡‹¼»ÇÂä´Œ ઋ¹ warfarin, digoxin, theophylline
ÙŒ †
4. ÂÒ·ÕÁ¤³ÊÁºÑµ¨º¡Ñºâ»ÃµÕ¹ÊÙ§ ઋ¹ NSAIDs, warfarin
è Õ Ø ÔÑ
5. ÂÒ·ÕÁ¤³ÊÁºÑµà»š¹ strong enzyme inducer or inhibitor
è Õ Ø Ô
6. ÂÒ·ÕÁ¤³ÊÁºÑµã¹¡Òâ¨Ñ´ÂÒẺ saturation kinetics ËÃ×Í zero-order kinetics «Ö§ÁÕ͵ÃÒ
è Õ Ø Ô è Ñ
¡Òâ¨Ñ´ÂÒ¤§·Õè áÁŒÇÒÃдѺÂÒã¹àÅ×Í´¨ÐÊÙ§ÁÒ¡¨¹¶Ö§ÃдѺà¡Ô´¾ÔÉ ¡çäÁ‹ÊÒÁÒöà˧¢¨Ñ´ÍÍ¡¨Ò¡Ã‹Ò§
‹
¡ÒÂä´Œ ઋ¹ ÂÒ phenytoin, theophylline
7. ÂÒ·Õ¨Ò໚¹µŒÍ§ãªŒà»š¹àÇÅÒ¹Ò¹æ áÅеŒÍ§¡ÒÃãËŒÃдѺÂÒã¹àÅ×Í´¤§·Õè à¾×ͤǺ¤ØÁâä
èí è
ઋ¹ÂҡѹªÑ¡ (antiepileptic drugs) ÂÒµŒÒ¹¡ÒÃൌ¹¼Ô´¨Ñ§ËÇТͧËÑÇ㨠(antiarrhythmic drugs)
101.
74 ¡ÒÃà¡Ô´»¯Ô¡ÃÂÒÃÐËÇ‹Ò§ÂÒ·ÕÁ¤ÇÒÁÊíҤѷҧ¤ÅÔ¹¡
ÔÔ è Õ Ô
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Manzi S., Shannon M. Drug interaction-a review. Clin Ped Emerg Med. 2005;6:93-102.
2. Piscitelli CS, Gallicano DK. Interaction among drugs for HIV and opportunistic infections. N Engl J Med.
2001;344:984-96.
3. Ray AW, Murray TK, Meredith S, Narasimhulu SS, Hall K, Stein MC. Oral erythromycin and the risk of
sudden death from cardiac cause. N Engl J Med. 2004;351:1089-96.
4. Trujillo CT, Nolan EP. Antiarrhythmic agents: drug interactions of clinical significant. Drug Safety. 2000;28:509-
32.
5. Spina E, Scordo GM. Clinically significant drug interactions with antidepressants in the elderly. Drugs Aging.
2002;19:299-20.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 79
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Dart RC, Stark Y, .ulton B, Koziol-McLain J, Lowenstein SR. Insufficient stocking of poisoning antidotes in
hospital pharmacies. JAMA 1996;276 (18):1508-10.
2. Juurlink DN, McGuigan MA, Paton TW, Redelmeier DA. Availability of antidotes at acute care hospitals in
Ontario. CMAJ 2001;165 (1):27-30.
3. Gorman SK, Zed PJ, Pursell RA, Brubacher J, Willis GA. Antidote stocking in British Columbia hospitals. CJEM
2003;5 (1):12-7.
4. Bailey B. Are there teratogenic risks associated with antidotes used in the acute management of poisoned
pregnant women?. Birth Defects Res A Clin Mol Teratol 2003;67:133-40.
5. Dart RC, Borron SW, Caravati EM, Cobaugh DJ, Curry SC, .alk JL, et al. Expert consensus guidelines for
stocking of antidotes in hospitals that provide emergency care. Ann Emerg Med 2009; 54 (3): 386-94.
6. Betten DP, Vohra RB, Cook MD, Matteucci MJ, Clark R.. Antidote use in the critically ill poisoned patient. J
Intensive Care Med 2006;21 (5):255-77.
102 ¡ÒÃ㪌 TriggerTool 㹡Ò䌹ËÒáÅÐÇÑ´ÍѵÃÒà˵ءÒóäÁ‹¾§»ÃÐʧ¤¨Ò¡¡ÒÃ㪌ÂÒã¹âç¾ÂÒºÒÅ
Ö
9. Jick H. Drugs-remarkably toxic. N Engl J of Med 1974;291(16):824-8.
10. Institute for Healthcare Improvement. Trigger Tool for Measuring Adverse Drug Events. Cambridge,
Massachusetts: IHI; 2004.
11. Griffin .A, Resar RK. IHI Global Trigger Tool for Measuring Adverse Events. IHI Innovation Series white paper.
Cambridge, Massachusetts; 2007. (Available on www.IHI.org).
12. Bates DW, Boyle DL, Vander Vliet MB. Relationship between medication errors and adverse drug events. J
Gen Intern Med 1995;10:199-205.
13. National Coordinatin Council for Medication Error Reporting and Prevention (NCC MERP) Index for Categorizing
Errors. Available from: http://www.nccmerp.org/medErrorCatIndex.html. Accessed June 10, 2010.
130.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 103
15
PET/CT for Cancer in Head and Neck Region:
Thyroid and Nonthyroid Carcinoma
ÍÒ¨ÒàᾷÂËԧຨÒÀÒ à¢ÕÂÇËÇÒ¹
ÀÒ¤ÇÔªÒÃѧÊÕÇ·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ÔÔ
ÁÐàÃ秺ÃÔàdzÈÕÃÉÐ áÅÐÅíÒ¤Í໚¹ÁÐàÃ秷ÕèÁÕ¤ÇÒÁÊíÒ¤ÑáÅоºä´Œº‹Í â´Â¾º»ÃÐÁÒ³
ÃŒÍÂÅÐ 5 ¢Í§ÁÐàÃ秷ѧËÁ´ ÁÕ¼»ÇÂÁÐàÃç§ÃÒÂãËÁ‹»ÃÐÁÒ³ 550,000 ÃÒµ‹Í»‚ áÅÐ໚¹ÊÒà˵آͧ
é ÙŒ †
¡ÒÃàÊÕªÕǵ»ÃÐÁÒ³ 300,000 ÃÒµ‹Í»‚ ª¹Ô´¢Í§à«ÅÅÁÐàÃ秷վºÁÒ¡·Õʴ໚¹à«ÅŪ¹Ô´ squamous
Ô è èØ
cell carcinoma ¹Í¡à˹×ͨҡÁÐàÃ秺ÃÔàdzÈÕÃÉÐáÅÐÅíҤͷվºä´Œ·Çä»ã¹àǪ»¯ÔºµÍ¹ä´Œá¡‹ ÁÐàÃç§
è Ñè Ñ ÔÑ
¢Í§â¾Ã§¨ÁÙ¡, paranasal sinus, lip and oral cavity, nasopharynx, oropharynx, hypopharynx,
salivary gland áÅÐ larynx áÅŒÇ ÂѧÃÇÁ¶Ö§ malignant melanoma, invasive skin cancer áÅÐ soft
tissue sarcoma (rhabdomyosarcoma áÅÐ osteosarcoma) 㹺ÃÔàdzÈÕÃÉÐáÅÐÅíÒ¤Í «Ö§ÃÇÁÁÐàÃç§ è
¢Í§ä·ÃÍ´ áÅоÒÃÒä·ÃÍ´´Ç Íغµ¡Òó¢Í§ÁÐàÃç§ä·ÃÍ´¾º»ÃÐÁÒ³ 4-9 ÃÒ µ‹Í 100,000
Œ Ñ Ô
ÃÒµ‹Í»‚ ¡ÒÃÃÑ¡ÉÒÁÐàÃç§ÈÕÃÉÐáÅÐÅíÒ¤Íâ´Â·ÑÇä» »ÃСͺ´ŒÇ¡Òü‹ÒµÑ´ ÃѧÊÕáÉÒ áÅÐà¤ÁպҺѴ
è Ñ í
µ‹Ò§¨Ò¡¡ÒÃÃÑ¡ÉÒÁÐàÃç§ä·ÃÍ´«§»ÃСͺ´ŒÇ ¡Òü‹ÒµÑ´áÅСÒÃãËŒÊÒÃÃѧÊÕäÍâÍ´Õ¹ (radioiodine)
Öè
໚¹ËÅÑ¡ ¡ÒÃÃÑ¡ÉÒ¼Ù»ÇÂÁÐàÃ秢ͧä·ÃÍ´ ¨íÒ໚¹µŒÍ§ÁÕ¡ÒûÃÐàÁÔ¹ÃÐÂТͧâä â´Â¾Ô¨ÒóҡÒÃ
Œ †
ÅØ¡ÅÒÁ¢Í§ÁÐàÃç§ä»ºÃÔàdz¢ŒÒ§à¤Õ§ µ‹ÍÁ¹éÒàËÅ×ͧ áÅСÒÃá¾Ã‹¡ÃШÒ¢ͧÁÐàÃç§ä»ÍÇÑÂÇÐË‹Ò§ä¡Å
í
«Ö§Áռŵ‹Í¡ÒÃÃÑ¡ÉÒáÅСÒþÂҡóâä¤ÅŒÒ¤ÅÖ§¡Ñº¡ÒÃÃÑ¡ÉÒÁÐàÃ秢ͧÍÇÑÂÇÐÍ×¹ ¡ÒûÃÐàÁÔ¹
è è
ÃÐÂÐ (staging) ¢Í§ÁÐàÃç§ÈÕÃÉÐáÅÐÅíÒ¤Í ÍÒÈÑ¡Òëѡ»ÃÐÇÑµÔ ¡ÒõÃǨËҧ¡Ò ¡ÒõÃǨ¼‹Ò¹¡ÅŒÍ§
(endoscopy) ¡ÒõÃǨÀÒ¾ÃѧÊÕ CT ËÃ×Í MRI áÅеŒÍ§ÍÒ¨¨íÒ໚¹µŒÍ§ÍÒÈÑ¡Ò÷íÒÍÑŵÃÒ«Òǹ´
ËÇÁ¡ÑºµÃǨªÔ¹à¹×Í (fine needle aspiration biopsy) »ÃСͺ¡Ñº¼Å·Ò§¾ÂÒ¸ÔÇ·ÂÒ㹼ٻǺҧÃÒÂ
é é Ô Œ †
ÊíÒËÃѺ¡ÒûÃÐàÁÔ¹ÃÐÂТͧÁÐàÃç§ä·ÃÍ´ ÍÒÈÑ¡Òëѡ»ÃÐÇÑµÔ ¡ÒõÃǨËҧ¡Ò ¼Å·Ò§
¾ÂÒ¸ÔÇ·ÂÒáÅСÒõÃǨ·Ò§àǪÈÒʵùÇà¤ÅÕÂà total body scan ¡ÒõÃǨÀÒ¾¶‹Ò·ҧÃѧÊÕ¨§ÁÕ
Ô Ô Ö
º·ºÒ·ÊíҤѵ‹Í¡Òú͡ÃÐÂТͧâäÁÐàÃ秺ÃÔàdzÈÕÃÉÐáÅÐÅíÒ¤Í áÅÐÁÐàÃç§ä·ÃÍ´ ÃÇÁ·Ñé§
¡ÒûÃÐàÁÔ¹¼Å¡ÒÃÃÑ¡ÉÒáÅСÒûÃÐàÁÔ¹¡ÒáÅѺ໚¹«éíҢͧâä
¡ÒõÃǨÀÒ¾ÃѧÊÕ´Ç CT áÅÐ MRI ãËŒ¢ÍÁÙÅ´ŒÒ¹¡ÒÂÇÔÀҤ䴌´Õ ÁÕ¤ÇÒÁàËÁÒÐÊÁ㹡ÒÃ
Œ Œ
»ÃÐàÁÔ¹ÃÐÂТͧâä à¾×ÍÇҧἹ¡ÒÃÃÑ¡ÉÒàÃÔÁµŒ¹ ᵋÁ¡¾º»˜ËÒ㹡ÒûÃÐàÁÔ¹à¹×ͧ͡·ÕàËÅ×ÍÍÂÙ‹
è è Ñ é è
(residual tumor) ËÃ×Íà¹×ͧ͡·Õ¡ÅѺ໚¹«éÒ (recurrent tumor) ÀÒÂËÅѧ¡ÒÃÃÑ¡ÉÒ ã¹»˜¨¨Øº¹¡ÒõÃǨ
é è í Ñ
110 PET/CT for Cancer in Head and Neck Region : Thyroid and Nonthyroid Carcinoma
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Wahl RL. Targeting glucose transporters for tumor imaging: “sweet” idea, “sour ” result. J Nucl Med 1996;
37:1038-41.
2. Kostakoglu L, Agress H Jr, Goldsmith SJ. Clinical role of .DG PET in evaluation of cancer patients. Radiographics
2003;23(2):315-40.
3. Warburg O, Posener K, Negelein E. On the metabolism of cancer cells. Biochem Z 1924;152:319-44.
4. Wong RJ, Lin DT, Sch?der H, Patel SG, Gonen M, Wolden S, et al. Diagnostic and prognostic value of
[(18).]fluorodeoxyglucose positron emission tomography for recurrent head and neck squamous cell carcinoma.
J Clin Oncol 2002;20(20):4199-208.
5. Sch?der H, Yeung HW. Positron emission imaging of head and neck cancer, including thyroid carcinoma.
Semin Nucl Med 2004;34(3):180-97.
6. Sch?der H, Yeung HW, Gonen M, Kraus D, Larson SM. Head and neck cancer: clinical usefulness and
accuracy of PET/CT image fusion. Radiology 2004;231(1):65-72.
7. Blide A, Von Buchwald C, Mortensen J, Marving J, Therkidsen MH, Kirkegaard J, et al. The role of SPECT-
CT in the lymphoscintigraphic identification of sentinel nodes in patients with oral cancer. Acta Otolaryngol
2006;1269(10):1096-103.
8. Haerla SK, Strobel K, Hany T., Sidler D, Stoeckli SJ. (18).-.DG-PET/CT versus panendoscopy for the detection
of synchronous second primary tumors in patients with head and neck squamous cell carcinoma. Head Neck.
2010;32(3):319-25.
9. Yamamoto Y, Wong TZ, Turkington TG, Hawk TC, Coleman RE. Head and neck cancer: dedicated .DG
PET/CT protocol for detection-phantom and initial clinical studies. Radiology 2007;244(1):263-72.
10. Yen R., Hung RL, Pan MH, Wang YH, Huang KM, Lui LT, et al. 18-fluoro-2-deoxy-glucose positron emission
tomography in detecting residual/recurrent nasopharyngeal carcinomas and comparison with magnetic resonance
imaging. Cancer 2003;98(2):283-7.
11. Kao CH, Shiau YC, Shen YY, Yen R.. Detection of recurrent or persistent nasopharyngeal carcinomas after
radiotherapy with technetium-99m methoxyisobutylisonitrile single photon emission computed tomography and
computed tomography: comparison with 18-fluoro-2-deoxyglucose positron emission tomography. Cancer
2002;94(7):1981-6.
12. Kao CH, Tsai Sc, Wang JJ, Ho YJ, Yen R., Ho ST. Comparing 18-fluoro-2-deoxyglucose positron emission
tomography with a combination of technetium 99m tetrofosmin single photon emission computed tomography
and computed tomography to detect recurrent or persistent nasopharyngeal carcinomas after radiotherapy.
Cancer 2001;92(2):434-9.
13. Isles MG, McConkey C, Mehanna HM. A systematic review and meta-analysis of the role of positron emission
tomography in the follow up of head and neck squamous cell carcinoma following radiotherapy or
chemoradiotherapy. Clin Otolaryngol 2008;33(3):210-22.
14. Chen AY, Vilaseca I, Hudgins PA, Schuster D, Halkar R. PET-CT VS contrast-enhanced CT: what is the role
for each after chemoradiation for advanced oropharyngeal cancer? Head Neck 2006;28 (6):487-95.
15. Andrade RS, Heron DE, Degirmenci B, .ilho PA, Branstetter B., Seethala RR, et al. Posttreatment assessment
of response using .DG-PET/CT for patients treated with definitive radiation therapy for head and neck cancers.
Int J Radiat Oncol Biol Phys 2006;65(5):1315-22.
138.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 111
16. Ong Sc, Sch?der H, Lee NY, Patel SG, Carlson D, .ury M, et al. Clinical utility of 18.-.DG PET/CT in
assessing the neck after concurrent chemoradiotherapy for locoregional advanced head and neck cancer.
JNM 2008;49 (4):532-40.
17. Kim SY, Lee SW, Nam SY, Im KC, Kim JS, Oh SJ, et al. The feasibility of 18.-.DG PET scans 1 month after
completing radiotherapy of squamous cell carcinoma of the head and neck. J Nucl Med 2007;48 (3):373-8.
18. Yao M, Smith RB, Graham MM, Hoffman HT, Tan H, .unk G., et al. The role of .DG PET in management
of neck metastasis from head-and-neck cancer after definitive radiation treatment. Int J Radiat Oncol Biol Phys
2005;63(4):991-9.
19. Liu SH, Chang JT, Ng SH, Chan SC, Yen TC. .alse positive fluorine-18-fluorodeoxy-D-glucose positron emission
tomography finding caused by osteoradionecrosis in a nasopharyngeal carcinoma patient. Br J Radiol
2004;77(915):257-60.
20. Troost EG, Bussink J, Hoffmann AL, Boerman OC, Oyen WJ, Kaanders JH. 18.-.LT PET/CT for early
response monitoring and dose escalation in oropharyngeal tumors. J Nucl Med 2010;51(6):866-74.
21. Ciemik I., Dizendorf E, Baumert BG, Reiner B, Burger C, Davis JB, et al. Radiation treatment planning with
an integrated positron emission and computed tomography (PET/CT): a feasibility study. Int J Radiat Oncol
Biol Phys 2003;57(3):853-63.
22. Chung MK, Jeong HS, Park SG, Jang JY, Son YI, Choi JY, et al. Metabolic tumor volume of (18.)-
fluorodeoxyglucose positron emission tomography/computed tomography predicts short-term outcome to
radiotherapy with or without chemotherapy in pharyngeal cancer. Clin Cancer Res. 2009; 15(18):5861-5868.
23. Kole AC, Nieweg OE, Prium J, Hoekstra HJ, Koops HS, Roodenburg JL, et al. Detection of unknown occult
primary tumors using positron emission tomography. Cancer 1998;82(6):1160-6.
24. Graven KM, Keyes JW Jr, Williums DW 3rd, McGuirt W., Joyce WT 3rd. Occult primary tumors of the head and
neck: lack of benefit from positron emission tomography imaging with 2- (.18)fluoro-2-deoxy-D-glucose. Cancer
1999;86(1):114-8.
25. Wartski M, Le Stanc E, Gontier E, Vilain D, Banal A, Tainturier C, e al. In search of an unknown primary tumor
presenting with cervical metastases: performance of hybrid .DG-PET-CT. Nucl Med Commun 2007;28(5):365-
71
26. Miller .R, Karnad AB, Eng T, Hussey DH, Stan McGuff H, Otto RA. Management of the unknown primary
carcinoma: lone-term follow-up on a negative PET scan and negative panendoscopy. Head Neck 2008;30(1);
28-34.
27. Rajendren JG, Hendrickson KR, Spence AM, Muzi M, Krohn KA, Mankoff DA. Hypoxia imaging-directed
radiation treatment planning. Eur J Nucl Med Mol Imaging 2006;33 (Suppl 1):44-53.
28. Myerson RJ, Singh AK, Bigott HM, Cha B, Engelbach JA, Kim J, et al. Monitoring the effect of mild
hyperthermia on tumour hypoxia by Cu-ATSM PET scanning. Int J Hyperthermia 2006;22(2):93-115.
29. Grosu AL, Piert M, Weber WA, Jeremic B, Picchio M, Schratzenstaller U, et al. Positron emission tomography
for radiation treatment planning. Strahlenther Onkol 2005;181(8):483-99.
30. Bloom AD, Adler LP, Shuck JM. Determinatiom of malignancy of thyroid nodules with positron emission
tomography. Surgery 1993;114(4):728-34.
31. Kim JM, Ryu JS, Kim TY, Kim WB, Kwon GY, Gong G, et al. 18.-fluorodeoxyglucose positron emission
tomography does not predict malignancy in thyroid nodules cytologically diagnosed as follicular neoplasm. J
Clin Endocrinol Metab 2007;92(5):1630-4.
139.
112 PET/CT for Cancer in Head and Neck Region : Thyroid and Nonthyroid Carcinoma
32. Singer PA, Cooper DS, Daniels GH, Ladenson PW, Greenspan .S, Levy EG, et al. Treatment guidelines for
patients with thyroid nodules and well-differentiated thyroid cancer. American Thyroid Association. Arch Intern
Med 1996;156(19):2165-72.
33. Wang W, Macapinlac H, Larson SM, Yeh SD, Akhurst T, .inn RD, et al. [18.]-2-fluoro-2-deoxy-D-glucose positron
emission tomography localized residual thyroid cancer in patients with negative 131I whole body scans and
elevated serum thyroglobulin levels. J Clin Endocrinol Metab 1999;84:2291-302.
34. Grunwald ., Schomburg A, Bender H, Klemm E, Menzel C, Bultmann T, et al. .luorine-18 fluorodeoxyglucose
positron emission tomography in the follow-up of differentiated thyroid cancer. Eur J Nucl Med 1996;23:312-9.
35. Chung JK, So Y, Lee JS, Choi CW, Lim SM, Lee DS, et al. Value of .DG PET in papillary thyroid carcinoma
with negative I-131 whole-body scan. J Nucl Med 1999;40(6):986-92.
36. Lind P, Kresnik E, Kumnig G, Gallowitsch HJ, Igerc I, Matschnig S, et al. 18.-.DG-PET in the follow-up of thyroid
cancer. Acta Med Austrica 2003;30(1):17-21.
37. Wang W, Larson SM, .azzari M, Tickoo SK, Kolbert K, Sgouros G, et al. Prognostic value of (18.)
fluorodeoxyglucose positron emission tomographic scanning in patients with thyroid cancer. J Clin Endocrinol
Metab 2000;85(3):1107-13.
38. Phan HT, Jager PL, Plukker JT, Wolffenbuttel BH, Dierckx RA, Links TP. Detection of bone metastases in
thyroid cancer patients: bone scintigraphy or 18.-.DG PET? Nucl Med Commun 2007;28(8):597-602.
39. Ito S, Kato K, Ikeda M, Iwano S, Makino N, Tadokoro M, et al. Comparison of 18.-.DG PET and bone
scintigraphy in detection of bone metastases of thyroid cancer. J Nucl Med 2007;48(6):889-95.
40. Bombardieri E, Buscombe J, Lucignani G, Schober O, editors. Advances in Nuclear Oncology: Diagnosis and
Therapy.1st ed. United kingdom: Informa UK Ltd; 2007.
41. Lin EC, Alavi A, editors. PET and PET/CT: A clinical guide.2nd ed. New York: Thieme Medical Publishers, Inc.;
2009.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 115
¤Ãͺ¤ÅØÁ¡ŒÍ¹ÁÐàÃç§ Å´¼Å¢ŒÒ§à¤Õ§µ‹ÍÍÇÑÂÇзÕÊÒ¤Ñã¡ÅŒà¤Õ§ áÅÐÁÕ¤ÇÒÁáÁ‹¹ÂíÒÁÒ¡¢Ö¹ à¾×ÍËÇѧ
èí é è
¼Å㹡ÒäǺ¤ØÁâäáÅÐÅ´¼Å¢ŒÒ§à¤Õ§·Õà¡Ô´¨Ò¡¡ÒÃÃÑ¡ÉÒ
è
ÃÙ»·Õè 1 ¡ÒÃÇҧἹ¡ÒÃÃÑ¡ÉÒ¼ÙŒ»†ÇÂÁÐàÃç§â¾Ã§ËÅѧ¨ÁÙ¡ (nasopharyngeal carcinoma)
´ŒÇÂÃѧÊÕÊÒÁÁÔµÔá»Ã¤ÇÒÁࢌÁ (IMRT) «Öè§áÊ´§ãËŒàËç¹Ç‹ÒÊÒÁÒöŴ»ÃÔÁÒ³ÃѧÊÕ
ä»·ÕèÍÇÑÂÇÐÊíÒ¤Ñઋ¹ ¡ŒÒ¹ÊÁͧ áÅÐÃÇÁ件֧¡ÒÃÅ´»ÃÔÁÒ³ÃѧÊÕä»·Õ赋ÍÁ¹éíÒÅÒÂ
¡Å‹Í§àÊÕ§ áÅЪ‹Í§»Ò¡´ŒÇÂ
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Attasara P. Cancer registry 2008. National Cancer Institute. 2009:1-18.
2. .orastiere AA, Goepfert H, Maor M, Pajak T., Weber R, Morrison W, et al. Concurrent chemotherapy and
radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003;349(22):
2091-8.
3. Pignon JP, le Maitre A, Bourhis J. Meta-analyses of chemotherapy in head and neck cancer (MACH-NC): an
update. Int J Radiat Oncol Biol Phys. 2007;69(2 Suppl):S112-4.
4. Cooper JS, Pajak T., .orastiere AA, Jacobs J, Campbell BH, Saxman SB, et al. Postoperative concurrent
radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med.
2004;350(19):1937-44.
5. Bernier J, Domenge C, Ozsahin M, Matuszewska K, Lefebvre JL, Greiner RH, et al. Postoperative irradiation
with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med.
2004;350(19):1945-52.
6. Bernier J, Cooper JS, Pajak T., van Glabbeke M, Bourhis J, .orastiere A, et al. Defining risk levels in locally
advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus
chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck. 2005 Oct;27(10):843-50.
143.
116 ¡ÒÃÃÑ¡ÉÒÁÐàÃç§ÈÕÃÉÐáÅÐÅíҤʹŒÇÂÃѧÊÕáÉÒ
Ñ
7. Bonner JA, Harari PM, Giralt J, Cohen RB, Jones CU, Sur RK, et al. Radiotherapy plus cetuximab for
locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and
relation between cetuximab-induced rash and survival. Lancet Oncol. 2010;11(1):21-8.
8. Bourhis J, Overgaard J, Audry H, Ang KK, Saunders M, Bernier J, et al. Hyperfractionated or accelerated
radiotherapy in head and neck cancer: a meta-analysis. Lancet. 2006;368(9538):843-54.
9. Pow EH, Kwong DL, McMillan AS, Wong MC, Sham JS, Leung LH, et al. Xerostomia and quality of life after
intensity-modulated radiotherapy vs. conventional radiotherapy for early-stage nasopharyngeal carcinoma: initial
report on a randomized controlled clinical trial. Int J Radiat Oncol Biol Phys. 2006;66(4):981-91.
10. Guido A, .uccio L, Rombi B, Castellucci P, Cecconi A, Bunkheila ., et al. Combined 18.-.DG-PET/CT imaging
in radiotherapy target delineation for head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2009;73(3):
759-63.
124 ÀÒ¾¹íÒÇÔ¶Õ ÃѧÊÕáÉÒ¡ŒÒÇä¡Å
Ñ
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Mell LK, Pawlicki T, Jiang SB, Mundt AJ. Image-Guided Radiation Therapy. In: Halperin EC, Perez CA, Brady
LW, eds. Perez and Brady’s Principles and Practice of Radiation Oncology, 5th Edition. Philadelphia: Lippincott
Williams & Wilkins, 2008;263-99.
2. Keall PJ, Vedam SS, George R et al. Respiratory regulatory gated 4D CT acquisition: concept and proof of
principle, Phys. Eng. Sci. Med, A. 2007; 211-20.
3. Jaffray DA, Brock KK, Sharpe M. Advanced Imaging and Guidance System for Use in Intensity Modulated
RT. In: Bortfeld T, Schmidt-Ullrich R, De Neve W and Wazer DE. Image-Guide IMRT. Berlin, Heidelberg,
Springer, 2006;217-27.
4. Létourneau D, Martinez AA, Lockman D, Yan D, Vargas C, Ivaldi G, Wong J. Assessment of residual error
for online cone-beam CT-guided treatment of prostate cancer patients. Int J Radiat Oncol Biol Phys. 2005;
62(4):1239-46.
152.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 125
18
Postoperative Pain Management in Pediatric Patients:
What’s New? What’s Recommendation?
ÈÒʵÃÒ¨ÒàᾷÂËÔ§ÊØÇÃÃ³Õ ÊØÃàÈóÕǧÈ
ÀÒ¤ÇÔªÒÇÔÊÕÇ·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ñ Ô ÔÔ
¤ÇÒÁà¨çº»Ç´ËÅѧ¼‹ÒµÑ´ã¹¼ÙŒ»†ÇÂà´ç¡Âѧ¤§ÁÕÍغѵԡÒóÊÙ§·Ñé§ã¹»ÃÐà·È áÅе‹Ò§»ÃÐà·È
ÊíÒËÃѺã¹âç¾ÂÒºÒÅÈÔÃÃÒªËÅѧ¨Ò¡ÁÕ¡Òúѹ·Ö¡¤Ðá¹¹¤ÇÒÁ»Ç´â´Â㪌à¤Ã×ͧÇÑ´·ÕàËÁÒÐÊÁµÒÁ
Ô è è
ÍÒÂØ໚¹ÊÑÒ³ªÕ¾·Õè 5 ¾ºÍغµ¡Òó¤ÇÒÁ»Ç´ËÅѧ¼‹ÒµÑ´ÃŒÍÂÅÐ 9.7 ã¹·Òáááà¡Ô´, ÃŒÍÂÅÐ 44
Ñ Ô
ã¹·Òá áÅÐÃŒÍÂÅÐ 44 ã¹à´ç¡âµ(2) ´Ñ§¹Ñ¹¤ÇÒÁ¾ÂÒÂÒÁ·Õ¨ÐÅ´ÃдѺ¤ÇÒÁ»Ç´ËÅѧ¼‹ÒµÑ´ã¹à´ç¡
(1)
é è
Âѧ¤§ÁÕÍ‹ҧµ‹Íà¹×ͧ è
¡ÅÂØ·¸·ÕèÊíÒ¤Ñ䴌ᡋ¡ÒþѲ¹ÒÃкº¡ÒôÙáÅÃЧѺ»Ç´µÅÍ´¨¹¡ÒÃãËŒ¤ÇÒÁÃٌᡋᾷÂ
¾ÂÒºÒÅáÅмٻ¡¤Ãͧ ¡ÒÃ㪌෤¹Ô¤áÅÐÂÒá¡Œ»Ç´·ÕàËÁÒÐÊÁ
Œ è
ÂÒ㹡ÅØÁ opioids Âѧ¤§à»š¹ÂÒ·Õ¹ÂÁ㪌ÃЧѺ»Ç´ÊíÒËÃѺ¡Òü‹ÒµÑ´·Õ·ÒãËŒ»Ç´ÃдѺ»Ò¹¡ÅÒ§
‹ è Ô è í
ËÃ×ÍÃعáç ¨Ò¡ÒÃÈÖ¡ÉÒã¹à´ç¡¨íҹǹ 10,762 ¤¹ã¹»ÃÐà·ÈÍѧ¡ÄÉ·Õ䴌ú opioid infusion ¾ºÇ‹ÒÁÕ
è Ñ
cardiac arrest 1 ÃÒ ¨Ò¡ÀÒÇÐ aspiration pneumonitis áÅÐ underlying neurological condition,
ÁÕÀÒÇÐ respiratory depression 14 ÃÒ«֧µŒÍ§ãªŒ naloxone á¡Œä¢ ¨íҹǹ 8 ÃÒÂ(3) ´Ñ§¹Ñ¹¡ÒÃ㪌෤¹Ô¤
è é
áÅÐÂÒá¡Œ»Ç´Í×¹æ àÊÃÔÁẺ multimodal analgesia ¨Ö§à»š¹·Õ¹ÂÁà¾×ͪ‹ÇÂàÊÃÔÁÄ·¸ÔÃЧѺ»Ç´ ª‹ÇÂÅ´
è è Ô è ì
»ÃÔÁÒ³ opioids ·Õ㪌áÅÐÅ´¼Å¢ŒÒ§à¤Õ§¨Ò¡ÂÒŧ
è
¡ÒþѲ¹ÒÃкº¡ÒôÙáÅÃЧѺ»Ç´ÁÕËÅÒÂÇÔ¸Õ ä´Œá¡‹ Ãкº¡ÒôÙáÅÃЧѺ»Ç´â´ÂÇÔÊÕá¾·Â Ñ
áÅÐÃкº¡ÒôÙáÅÃЧѺ»Ç´â´Âá¾·Â áÅоÂÒºÒÅ਌Ңͧ䢌â´ÂÁÕÇÔÊÑÕá¾·Â໚¹·Õè»ÃÖ¡ÉÒ(4)
ÃкºááÊÒÁÒöãËŒ¡ÒÃÃЧѺ»Ç´Í‹ҧÁÕ»ÃÐÊÔ·¸ÔÀÒ¾Ê٧ᵋ´áżٻÇÂä´ŒäÁ‹·Ç¶Ö§ à¹×ͧ¨Ò¡ÁÕÇÊÕ
Ù Œ † Ñè è ÔÑ
á¾·ÂäÁ‹à¾Õ§¾Í ÃкºËÅѧ¨Ð´ÙáżٻÇÂä´Œ¤Ãͺ¤ÅØÁÁÒ¡¡Ç‹Ò ᵋÍÒ¨ÁÕ»ËÒã¹´ŒÒ¹»ÃÐÊÔ·¸ÔÀÒ¾(4,6)
Œ † ˜
«Ö§¤ÇÃÁÕ¡ÒþѲ¹Òã¹ËÅÒÂæ ´ŒÒ¹ä´Œá¡‹
è
1. ¡ÒûÃÐàÁÔ¹¤ÇÒÁà¨çº»Ç´¢Í§¼ÙŒ»†ÇÂà´ç¡áµ‹ÅÐÇÑÂâ´Â㪌à¤Ã×èͧÁ×Í·ÕèàËÁÒÐÊÁµÒÁÍÒÂØ
Í‹ҧ໚¹ÃÙ»¸ÃÃÁ áÅе‹Íà¹×ͧËÅѧ¼‹ÒµÑ´à»š¹ÊÑÒ³ªÕ¾·Õè 5 Í‹ҧ¹ŒÍ 3 Çѹ
è
2. ¡ÒÃ㪌ǸºÒºÑ´¤ÇÒÁ»Ç´·ÕàËÁÒÐÊÁ¡ÑºÃдѺ¤ÇÒÁ»Ç´
ÔÕ í è
3. ¡ÒÃãËŒ¤ÇÒÁÃÙá¡‹á¾·Â áÅоÂÒºÒÅà¡ÕÂǡѺ¡ÒÃãËŒÂÒÃЧѺ»Ç´
Œ è
4. ¡ÒÃ㪌ẺÊѧ¡ÒÃÃÑ¡ÉÒÊíÒËÃѺᾷ«§ÁÕª¹Ô´ÂÒ ¢¹Ò´ÂÒ áÅÐÃÐÂÐˋҧ㹡ÒÃãËŒÂÒ·Õè
è Öè
àËÁÒÐÊÁÊíÒËÃѺà´ç¡µÅÍ´¨¹¡ÒÃÊѧ¡ÒÃÃÑ¡ÉÒẺ nurse controlled analgesia(7)
è
128 Postoperative Pain Management in Pediatric Patients : What’s New? Recommendation?
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Aroonpruksakul N, Suraseranivongse S. Quality of post-operative pain control in infants and neonates. Siriraj
Med J. 2009;61(5):245-8.
2. Suraseranivongse S, Khuvichitsuwan P, Sriverachai P, Boonthitikul S, Homchan W. Quality assessment and
risk factors of postoperative pain in children. Thai J Anesthesiology. 2006;32(4):261-8.
3. Morton N, Errera A. APA national audit of pediatric opioid infusions. Pediatr Anesth. 2010; 20: 119–125.
4. Ready LB, Oden R, Chadwick HS, et al. Development of an anesthesiology-based postoperative pain
management service. Anesthesiology. 1988;68:100-6.
5. Lee A, Chan S, Chen PP, Gin T, Lau AS. Economic evaluations of acute pain service programs: a systematic
review. Clin J Pain. 2007;23(8):726-73.
6. Shapiro A, Edna Z, Kantor M, Memrod J, .redman B. Establishing a nurse-based, Anesthesiologist-supervised
inpatient acute pain service: experience of 4,617 patients. J Clin Anesth. 2004;16:415-20.
7. Howard R, Lloydthomas A, Thomas M, Williams DG, Saul R, Bruce E, Peters J.Nurse-controlled analgesia
(NCA) following major surgery in 10 000 patients in a children’s hospital. Pediatr Anesth. 2010;20:126–34.
8. Willschke H, Marhofer P, B?senberg A, Johnston S, Wanzel O, Cox SG, et al. Ultrasonography for ilioinguinal/
iliohypogastric nerve blocks in children. Br J Anaesth. 2005;95(2):226-30.
9. Weintraud M, Lundblad M, Kettner SC, Willschke H, Kapral S, L?nnqvist PA, et al. Ultrasound versus
landmark-based technique for ilioinguinal-iliohypogastric nerve blockade in children: the implications on plasma
levels of ropivacaine. Anesth Analg. 2009;108(5):1488-92.
10. Walker KJ, McGrattan K, Aas-Eng K, Smith A.. Ultrasound guidance for peripheral nerve blockade. Cochrane
Database Syst Rev. 2009;(4):CD006459.
11. Karthikesalingam A, Walsh SR, Markar SR, Sadat U, Tang TY, Malata CM. Continuous wound infusion of
local anaesthetic agents following colorectal surgery: systematic review and meta-analysis.World J Gastroenterol.
2008;14:5531-5.
12. Krotz ., Schiele TM, Klauss V, Sohn HY. Selective COX-2 inhibitors and risk of myocardial infarction. J Vasc
Res. 2005;42:312–24.
13. Lynn AM, Bradford H, Kantor ED, Seng K, Salinger DH, Chen J, et al. Postoperative ketorolac tromethamine
use in infants aged 6–18 months: the effect on morphine usage, safety assessment, and stereo-specific
pharmacokinetics. Anesth Analg. 2007;104:1040–51.
14. Papacci p, de .rancisci G, Iacobucci T, Giannantonio C, de Carolis MP, Zecca E. Use of intravenous ketorolac
in the neonate and premature babies. Pediatr Anesth. 2004;14:487–92.
15. Tucker A, Kim Y, Nadeson R et al. Investigation of potentiation of analgesic effects of fentanyl by ketamine
in humans: a double blinded, randomized, placebo controlled, crossover study of experimental pain. BMC
Anesthesiol. 2005;5:2–14.
16. Granry JC, Dube L, Turroques H et al. Ketamine: new uses for an old drug. Curr Opin Anaesthesiol.
2000;13:299–302.
17. Grande LA, O’Donnell BR, .itzgibbon DR et al. Ultra-low dose ketamine and memantine treatment for pain in
an opiodtolerant oncology patient. Anesth Analg. 2008;107:1380–83.
18. Hocking G, Cousins MJ. Ketamine in chronic pain management: an evidence-based review. Anesth Analg.
2003;97:1730–39.
19. Gurnani A, Sharma PK, Rautela RS et al. Analgesia for acute musculoskeletal trauma: low-dose subcutaneous
infusion of ketamine. Anaesth Intens Care. 1996;24:32–6.
156.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 129
20. Dal D, Celebi N, Gaye E et al. The efficacy of intravenous or peritonsillar infiltration of ketamine for postoperative
pain relief in children following adenotonsillectomy. Pediatr Anesth. 2007;17:263–9.
21. Aspinall RL, Mayor A. A prospective randomized controlled study of the efficacy of ketamine for postoperative
pain relief in children after adenotonsillectomy. Paediatr Anaesth. 2001;11: 333–6.
22. Palmer GM, Chen SP, Smith KR, Hardikar W. Introduction and audit of intravenous paracetamol at a tertiary
paediatric teaching hospital. Anaesth Intensive Care. 2007;35:702–6
23. Murat I, Baujard C, .oussat C, et al. Tolerance and analgesic efficacy of a new i.v. paracetamol solution in
children after inguinal hernia repair. Paediatr Anaesth. 2005;15:663–70.
24. Capici ., Ingelmo PM, Davidson A, et al. Randomized controlled trial of duration of analgesia following
intravenous or rectal acetaminophen after adenotonsillectomy in children. Br J Anaesth. 2008;100:251–5.
25. Palmer GM , Atkins M, Anderson BJ, Smith KR, Culnane TJ,McNally CM, et al.I.V. acetaminophen
pharmacokinetics in neonates after multiple doses. Br J Anaesth.2008;101(4):523–30.
26. Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43:879–923.
27. Allegaert K, Anderson BJ, Verbesselt R, Debeer A, de Hoon J, Devlieger H,et al. Tramadol disposition in the
very young: an attempt to assess in vivo cytochrome P-450 2D6 activity. Br J Anaesth.2005;95(2):231–9.
28. Kitson R, Carr B. Tramadol and severe serotonin syndrome. Anaesthesia. 2005;60(9):934-5
158.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 131
19
Outcome Improvement in Neuroanesthesia
: Neuro-interventional Perspective
Assistant Professor Anchalee Churojana
Department of Radiology, .aculty of Medicine Siriraj Hospital, Mahidol University
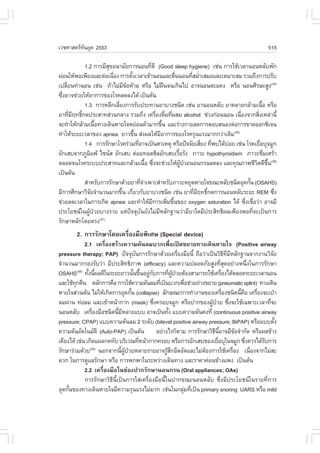
Interventional Neuroradiology is a treatment modality of vascular diseases of central
nervous system (CNS) and head & neck region with certain overlapped aspects with neurosurgery,
head & neck surgery and vascular surgery, by means of endovascular access to deliver
therapeutic agents such as embolic materials, sclerosing and chemotherapeutic drugs including
mechanical devices. The purpose of the procedure is either definite treatment or preoperative
devascularization.
It can be broadly grouped as
1. Embolization procedure: with the purpose to occlude vessels in the diseases with
abnormal vascular channels or high vascularization. Those diseases are arteriovenous
malformations (AVMs), arteriovenous fistulas, carotid-cavernous fistulas, intracranial aneurysms,
traumatic aneurysms and preoperative devascularization of tumors.
Diseases Embolic agent Comment
AVMs N-butyl cyanoacrylate (NBCA
or Glue)
Carotid-cavernous fistulas Detachable balloon
(CC.s)
Aneurysms Detachable coils May need nondetachable
balloon or stent-assisted
coiling
Arteriovenous fistulas NBCA or coils depending on size of fistulas
Dural arteriovenous shunts NBCA and/or fibered coils Usually NBCA using fpr
or detachable coils transarterial feeder occlusion
and coils using for dural sinus
or venous packing
Preoperative tumor Particles (polyvinyl alcohols
embolizations or PVA)
159.
132 Outcome Improvement in Neuroanesthesia : Neuro-interventional Perspective
1. Dilatation procedure: with purpose to open up the narrowed arteries, or perform
angioplasty with or without stenting in the occluded vascular disease including mechanical
thrombectomy or clot retrieval in acute embolic stroke.
2. Transarterial infusion: with the purpose for intraarterial thrombolysis in acute stroke
or chemotherapy in certain cancers such as transophthalmic artery chemo-infusion for
retinoblastoma, palliative transarterial chemo-infusion for nasopharyngeal cancer.
3. Percutaneous or direct puncture: mostly used in AVMs or venous malformations
with extracranial locations for delivering liquid embolic or sclerosing agents directly. In our
practice, NBCA is used in AVMs and Bleomycin is used as sclerosing drug.
Currently, Interventional Neuroradiology is increasingly performed with the administration
of anesthesia. In this point of view, several important concerns from anesthesiologists should
be included1
! Maintenance of the patient’s immobility to reduce motion artifact, general anesthesia
is preferred to facilitate visualization of small vessels and prevent patient movement.
! Proper monitoring: blood pressure, PaCO2 in case of the possibility of unexpected
neurological complications and anaphylactic reactions, particularly from contrast
media.
! Anticoagulant therapy and monitoring.
! Rapid recovery from anesthesia and sedation during the procedure to facilitate
neurological testing, such as in internal carotid artery sacrification.
! Management of sudden unexpected complication such as hemorrhage or vascular
occlusion.
! Guiding the medical care and treatment of critical ill patients during the procedure
and transportation.
! Smooth recovery from anesthesia after procedure to prevent risk of complications
such as balloon displacement during strong coughing, vascular injury at puncture
site during non-purposeful movement.
General care
! Intravenous access should be on the left arm with adequate extension tube from the
image intensifier or when the patient is draped.
! Increased systemic blood pressure in patient whose femoral pulse can’t be palpated
due to hypotension.
160.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 133
! Intraprocedural heparinization and control activated clotting time including
postoperative protamine reversal.
! Awareness of allergic reaction particularly with contrast media.
Special care
! Pediatric patients: keep warm to the patients, contrast medium and drug dose-
limitation, intraarterial & intravenous fluid overload. Post embolization for vein of
Galen malformation and high flow AVM usually need to maintain head in semi-upright
position to minimize venous congestion.
! Controlled systemic hypotension may be required during embolization of high flow
fistulas or intracranial AVMs to reduce the flow across the lesions to achieve good
deposition of embolic agents.2
! The patient must be awake for the balloon occlusion test procedure, as continuous
neurological examination to assess the effects of occlusion. However, rapid wake-up
of the patient is requested in the case of unplanned or accidental arterial occlusion.
! Concerning of sudden hypotension or vago-vagal reflex during carotid balloon
angioplasty
! Adequate heparinization in the case of transarterial device delivery such as coiling
aneurysm or balloon application.
! Preoperative antiplatelet administration for all stenting procedure.
Neurovascular complication management
! Catheter-induced vasospasm: may need transarterial Nimodipine infusion which results
to systemic hypotension.
! Arterial occlusion: may be caused by fly-away of embolic agents to normal arteries,
malposition of device such as coils or stent, and thromboembolism. In this event,
the arterial pressure should be raised to increase collateral blood flow and maintain
normocarbia. Mechanical thrombectomy or infusion of thrombolytic agent may be
needed. Antiplatelet agents, such as Abciximab, have also shown promising results.
However, occlusion from NBCA or glue is always permanent. If arterial luminal
narrowing or occlusion occurred from catheter-induced dissection, systemic
heparinization is recommended and the procedure must be terminated.
161.
134 Outcome Improvement in Neuroanesthesia : Neuro-interventional Perspective
! Venous outlet occlusion: usually results from spillage of glue during embolization of
AVMs or fistula into draining veins. If stasis of contrast media in the venous outlet
is observed in post-embolization angiogram, embolization of feeding arteries as much
as possible is recommended to minimize the venous congestion. During post
procedural period, the patient needs to have maintenance of modest hypotension
and sedation.
! Hemorrhage: results from arterial rupture by catheter or guide-wire perforation or abrupt
rise in mean arterial pressure during test injection in the small artery or fragile
aneurysm. Visualization of extravasation of contrast media is the only clue for the
diagnosis, however, some patients may have sudden onset of bradycardia. Immediate
reversal of heparin is required (1 mg protamine for each 100 units of heparin given).
Lowering of the systemic arterial pressure may be needed. PaCO2 should be
maintained between 4.5 and 5.0 kPa.2 Endovascular treatment should be performed
without hesitation depending on each cause. Aneurysm rupture should be rapidly
packed by coils as much as possible. Arterial perforation can be glued vigorously at
the tip of microcatheter. Intraoperative CT scan is recommended for assessment
and preparing for postoperative management. Emergency craniotomy may be required
if endovascular embolization fails.
In conclusion, interventional neuroradiological procedures have been expanding in the
treatment of CNS, including head and neck, diseases. The type of anesthetic administration,
general anesthesia or intravenous sedation, is determined by the goal of each procedure together
with the experience of the radiology-anesthesia team.3 The anesthesiologists have a crucial role
in facilitating procedures, monitoring of the patients and involvement of complication management.
Thus, understanding of specific interventional neuroradiological procedures and their potential
complications are important. Good relationship with communication and planning between
radiologists and anesthesiologists in the team of interventional neuroradiology are key factors
of smooth procedure with good patient’s outcome.
References
1. Hashimoto T, Gupta DK, Young WL. Interventional neuroradiology-anesthetic considerations. Anesthesiology
Clinics of North America. 2002;20(2):347-59.
2. Varma MK, Price K, Jayakrishnan Y, et al. Anaesthetic considerations for interventional neuroradiology. BJA
2007;99(1):75-85.
3. Derbent A, Oran I, Parildar M, et al. Adverse effects of anesthesia in interventional radiology. Diagn Interv
Radiol 2005;11:109-112.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 141
11. Hall AH, Saiers J, Baud .. Which cyanide antidote? Crit Rev Toxicol 2009;39(7):541-52.
12. Brent J. .omepizole for ethylene glycol and methanol poisoning. N Engl J Med 2009;360(21):2216-23.
13. Kerns W, 2nd. Management of beta-adrenergic blocker and calcium channel antagonist toxicity. Emerg Med
Clin North Am 2007;25(2):309-31; abstract viii.
14. Lheureux P, Penaloza A, Gris M. Pyridoxine in clinical toxicology: a review. Eur J Emerg Med 2005;12(2):
78-85.
144 ¡ÒÃÍÍ¡¡íÒÅѧËÅѧ¡Ò÷íÒËѵ¶¡ÒÃËÃ×ͼ‹ÒµÑ´ËÑÇã¨
4. Metabolic equivalent time (MET) ËÁÒ¶֧ ÃдѺ¢Í§àÁµÒºÍÅÔ«Á¢Í§Ã‹Ò§¡ÒÂàÁ×ͤԴ
Ö è
໚¹¨íҹǹ෋ҢͧàÁµÒºÍÅÔ«Á¢³Ð¾Ñ¡ â´Âã¹¢³Ð¾Ñ¡Ã‹Ò§¡ÒÂÁÕ¡ÒÃ㪌ÍÍ¡«Ôਹà¾×ÍãËŒà¡Ô´¾Åѧ§Ò¹
Ö è
3.5 ÁÔÅÅÔŵÃ/¹éÒ˹ѡµÑÇ 1 ¡ÔâÅ¡ÃÑÁ/¹Ò·Õ ¡Å‹ÒÇ ¤×Í ¢³Ð¾Ñ¡Ã‹Ò§¡Ò¨ÐÁÕÃдѺàÁµÒºÍÅÔ«Á 1 MET
Ô í Ö
ËÃ×ÍÁÕ¡ÒÃ㪌ÍÍ¡«Ôਹ 3.5 ÁÔÅÅÔŵÃ/¹éÒ˹ѡµÑÇ 1 ¡ÔâÅ¡ÃÑÁ/¹Ò·Õ ´Ñ§¹Ñ¹ ¨Ö§¹ÔÂÁ㪌 ¨íҹǹ MET ã¹
Ô í é
¡Òú‹§ºÍ¡¶Ö§ ÃдѺ¡ÒÃ㪌ÍÍ¡«Ôਹ¢Í§Ã‹Ò§¡Ò ¾Åѧ§Ò¹ËÃ×ÍÃдѺ¤ÇÒÁ˹ѡ¢Í§¡Ô¨¡ÃÃÁ·Õ·Ò ઋ¹ è í
! ¹Ñ§¾ÔÁ¾§Ò¹ËÃ×Í㪌¤ÍÁ¾ÔÇàµÍÃ
è 1.5 METs
! Â׹Ōҧ¨Ò¹ àµÃÕÂÁÍÒËÒà 2.0-2.5 METs
! ÍÒº¹éíÒ 2-3 METs
! Ōҧö ¡ÇÒ´ºŒÒ¹ 3 - 3.5 METs
! ¡ÒÃà´Ô¹àÃ×ÍÂæ㹺ŒÒ¹ËÃ×Í·Õ·Ò§Ò¹
è è í 2 METs
! à´Ô¹àÃçÇ溹¾×¹ÃÒº (4 äÁÅ/ ªÑÇâÁ§)
é è 5 METs
! ¡ÒÃŧºÑ¹ä´ 2.5 METs
! ¡ÒâֹºÑ¹ä´
é 4.0 METs
5. ÃдѺ¤ÇÒÁà˹×Í (Rate of perceived exertion, RPE) ໚¹ÇÔ¸¡ÒÃÍ‹ҧ˹֧·Õ㪌ºÍ¡ÃдѺ
è Õ è è
¤ÇÒÁ˹ѡ¢Í§¡Ò÷íÒ¡Ô¨¡ÃÃÁ ·Õ¹ÂÁ㪌¡¹ ¤×Í Borg scale ·Õ¡Ò˹´¤ÇÒÁà˹×Í ໚¹ÃдѺµÑÇàÅ¢
è Ô Ñ è í è
µÑ§áµ‹ 6-20 (µÒÃÒ§·Õè 1)
é
µÒÃÒ§·Õè 1 ÃдѺ¤ÇÒÁà˹×èÍ Borg scale
¤Ðá¹¹ ¤ÇÒÁÃÙÊ¡
Œ Ö
6
7 ÃÙʡʺÒÂ
΅ very very light
8
9 äÁ‹à˹×ÍÂ
è very light
10
11 àÃÔÁÃÙÊ¡à˹×ÍÂ
è ŒÖ è fairly light
12
13 ¤‹Í¹¢ŒÒ§à˹×ÍÂ
è somewhat hard
14
15 à˹×ÍÂ
è hard
16
17 à˹×ÍÂÁÒ¡
è very hard
18
19 à˹×Í·ÕÊ´
è èØ very very hard
20
172.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 145
6. Heart rate reserve (HRR) ËÃ×Í Karvonen method ໚¹ÇÔ¸¡ÒáíÒ˹´¤ÇÒÁ˹ѡ¢Í§¡ÒÃ
Õ
ÍÍ¡¡íÒÅѧÍ‹ҧ˹֧ â´Â¡íÒ˹´à»š¹ ÃŒÍÂÅТͧʋǹµ‹Ò§¢Í§ÍѵÃÒ¡ÒÃൌ¹¢Í§ËÑÇ㨠ÊÙ§ÊØ´ (maximal
è
heart rate, HR max ¡ÑºÍѵÃÒ¡ÒÃൌ¹¢Í§ËÑÇ㨠¢³Ð¾Ñ¡ (resting heart rate, HRrest )
THR= %(HRmax- HRrest) + HRrest
à˵ؼŷÕ赌ͧÍÍ¡¡íÒÅѧ
¡ÒÃÍÍ¡¡íÒÅѧÁÕËÅÒª¹Ô´ ᵋ¡ÒÃÍÍ¡¡íÒÅѧ·ÕèÁÕ»ÃÐ⪹áÅÐ㪌à¾×èÍÊ‹§àÊÃÔÁÊØ¢ÀÒ¾áÅÐ
»‡Í§¡Ñ¹âäËÑÇ㨠¤×Í ¡ÒÃÍÍ¡¡íÒÅѧà¾×Íà¾ÔÁ¤ÇÒÁ·¹·Ò¹ËÃ×ͤÇÒÁÊÁºÙó¢Í§ÃкºËÑÇ㨠ËÅÍ´àÅ×Í´
è è
áÅлʹ ËÃ×Í ¡ÒÃÍÍ¡¡íÒÅѧẺáÍâúԤ ¡ÒÃÍÍ¡¡íÒÅѧª¹Ô´¹ÕéÁØ‹§ãËŒà¡Ô´¡ÒûÃѺµÑǢͧËҧ¡ÒÂ
ãËŒÊÒÁÒö´Ö§ÍÍ¡«Ôਹä»ãªŒ»ÃÐ⪹䴌´Õ¢Öé¹ â´Â¾ºÇ‹Ò¡ÒÃÍÍ¡¡íÒÅѧẺáÍâúԤ ÁÕ»ÃÐ⪹
ª‹Ç»‡Í§¡Ñ¹âäËÑÇ㨴ѧáÊ´§ã¹ÃÙ»·Õè 1(1) ´Ñ§¹Ñ¹¡ÒÃÍÍ¡¡íÒÅѧª¹Ô´¹Õ¨§à»š¹¡ÒÃÍÍ¡¡íÒÅѧ·Õá¹Ð¹íÒãËŒ
é éÖ è
·íÒ໚¹»ÃШíÒ㹪‹Ç§·ÕÍÍ¡¨Ò¡âç¾ÂÒºÒÅËÃ×Íá¢ç§áç¢Ö¹áÅŒÇ
è é
¡ÒÃÍÍ¡¡íÒÅѧ¨Ñ´à»š¹à¤Ã×ͧÁ×ÍÊíÒ¤Ñ㹡Òÿ„¹¿ÙÊÁÃöÀÒ¾¼Ù»ÇÂâä CAD â´Â¡Òÿ„¹¿Ù
è œ Œ † œ
ÊÁÃöÀÒ¾·ÕÁ¡ÒÃÍÍ¡¡íÒÅѧ໚¹Í§¤»ÃСͺÁÕ»ÃÐ⪹㹡ÒÃÅ´ÍѵÃÒ¡ÒÃàÊÕªÕǵ¨Ò¡âäËÑÇã¨(2)
è Õ Ô
Å´ÃдѺâ¤àÅÊàµÍÃÍÅ ÃдѺ¤ÇÒÁ´Ñ¹âÅËÔµ«ÔÊâµÅÔ¤ (systolic blood pressure, SBP)(3) áÅÐÂѧª‹ÇÂ
»‡Í§¡Ñ¹¡ÒÃ໚¹«éÒÃÇÁ·Ñ§¨Ðª‹ÇÂÅ´ÍѵÃÒ¡ÒÃà¡Ô´ËÅÍ´àÅ×Í´µÕºµÑ¹ÀÒÂËÅѧ¡Ò÷íÒ PCI
í é
ÃÙ»·Õè 1 áÊ´§¼Å¡Òû‡Í§¡Ñ¹âäËÑÇ㨢ͧ¡Ô¨¡ÃÃÁ·Ò§¡Ò·Õè·íÒÊÁèíÒàÊÁÍ(1)
BP = blood pressure; HR = heart rate
àǪÈÒʵ÷¹Âؤ 2553
Ñ 147
ÃÐÂзÕè 1 ÃÐÂмٌ»†ÇÂã¹ ¨ÐÁاãËŒ¼»ÇÂäÁ‹à¨çº»Ç´ »ÃÒȨҡÀÒÇÐá·Ã¡«ŒÍ¹ ª‹ÇÂàËÅ×Í
‹ ÙŒ †
µ¹àͧ䴌 áÅÐÊÒÁÒö»¯Ôºµµ¹ËÃ×ÍÍÍ¡¡íÒÅѧ·ÕºÒ¹ä´Œ â´Â·ÑÇ仨ÐàÃÔÁãËŒÍÍ¡¡íÒÅѧÃÇÁ·Ñ§Â×¹à´Ô¹
Ñ Ô è Œ è è é
àÁ×ͼٻÇÂÁÕÍÒ¡Ò䧷ÕáÅŒÇ ÊÔ§ÊíÒ¤Ñ ¤×Í ¼Ù»ÇÂäÁ‹ÁÍÒ¡ÒÃà¨çºá¹‹¹Ë¹ŒÒÍ¡ ËÃ×ÍÁÕËÇã¨àµŒ¹¼Ô´»¡µÔ
è Œ † è è Œ † Õ Ñ
·Õà»ÅÕ¹á»Å§ä»¨Ò¡à´ÔÁ áÅеŒÍ§¤íÒ¹Ö§¶Ö§¤ÇÒÁ¾ÃŒÍÁ´ŒÒ¹¨Ôµã¨¢Í§¼Ù»Ç´ŒÇ ÃÇÁ·Ñ§´Ù¡Òõͺʹͧ
è è Œ † é
¢Í§Ã‹Ò§¡Òµ‹Í¡ÒÃÍÍ¡¡íÒÅѧNjÒàËÁÒÐÊÁËÃ×ÍäÁ‹ à¾×ÍËÂØ´ËÃ×Í»ÃѺà»ÅÕ¹â»Ãá¡ÃÁ (µÒÃÒ§·Õè 6)(4) â´Â
è è
·ÑÇ仨ÐãËŒ¢³ÐÍÍ¡¡íÒÅѧÁÕ͵ÃÒ¡ÒÃൌ¹¢Í§ËÑÇã¨ËÃ×ͪվ¨Ãà¾ÔÁ¢Ö¹¨Ò¡¢³Ð¾Ñ¡»ÃÐÁÒ³ 5-20 ¤Ãѧ/
è Ñ è é é
¹Ò·Õ áÅÐã¹ÃÐÂйըÐäÁ‹Á¡Òýƒ¡ÍÍ¡¡íÒÅѧª¹Ô´·ÕÁá経ҹ (resistive exercise training)
é Õ è Õ
! ËÅѧ·íÒ PCI ʋǹãË‹¡Ò÷íÒ PCI ¨Ð·íÒ¼‹Ò¹·Ò§ËÅÍ´àÅ×Í´á´§ femoral ·Õè¢Ò˹պ
㹪‹Ç§áá¼Ù»Ç¨еŒÍ§¹Í¹¹Ô§æ ໚¹àÇÅÒ¹Ò¹ ÁÑ¡ÁÕ»ËһǴàÁ×Í ᵋàÁ×Íà¤Å×͹äËÇä´Œ
Œ † è ˜ è è è
ÍÒ¡ÒûǴàÁ×ͨдբ¹ËÃ×ÍËÒÂä» ¼Ù»Ç¡ÅØÁ¹ÕÊǹãË‹¨Ð¹Í¹âç¾ÂÒºÒÅ໚¹ÃÐÂÐ
è Öé Œ † ‹ é ‹
àÇÅÒÊÑ¹æ »ÃÐÁÒ³ 1-2 Çѹ ¡Ô¨¡ÃÃÁ·Ò§¡Ò·ըнƒ¡ãËŒ¨Ð໚¹¡Ô¨¡ÃÃÁ¾×¹°Ò¹à¾×ÍãËŒªÇÂ
é è é è ‹
µ¹àͧ䴌 ·íÒ¡Ô¨ÇѵûÃШíÒÇѹ䴌àͧ ¡ÒÃÍÍ¡¡íÒÅѧËÃ×Í¡Ô¨¡ÃÃÁ·Ò§¡Ò·Õèá¹Ð¹íÒ ¤×Í
¡ÒÃà´Ô¹ ·Ñ§¹ÕµÍ§ÃÐÇѧ¡ÒÃà¡Ô´ËŒÍàÅ×Í´ËÃ×Í¡ŒÍ¹àÅ×Í´ÍÍ¡¨Ò¡ËÅÍ´àÅ×Í´á´§ femoral ´ŒÇÂ
é é Œ
áÅФÇõÃǨ»ÃÐàÁÔ¹ªÕ¾¨Ã¢Í§ËÅÍ´àÅ×Í´á´§·ÕÍÂÙã¹Ê‹Ç¹»ÅÒ´ŒÇ ¤×Í ËÅÍ´àÅ×Í´á´§
è ‹
dorsalis pedis áÅÐ posterior tibial
! ËÅѧ¼‹ÒµÑ´ CABG ¼Ù»Ç¡ÅØÁ¹ÕÊǹãË‹¨Ð¹Í¹âç¾ÂÒºÒÅ»ÃÐÁÒ³ 5-7 Çѹ ¡ÒÃÍÍ¡¡íÒÅѧ
Œ † ‹ é‹
·Õèá¹Ð¹íÒã¹ÇѹááËÅѧ¼‹ÒµÑ´ ¤×Í ¡ÒÃËÒÂã¨ÅÖ¡áÅСÒáÃе،¹äÍ à¾×èÍ»‡Í§¡Ñ¹ÀÒÇÐ
á·Ã¡«ŒÍ¹·Ò§»Í´áÅÐ ¡ÒâÂѺ¢ŒÍ෌Ңֹŧ (ankle pumping) à¾×Í»‡Í§¡Ñ¹ÀÒÇÐÅÔÁàÅ×Í´
é è è
ÍØ´µÑ¹ã¹ËÅÍ´àÅ×Í´´íÒ (deep vein thrombosis) àÁ×ͼٻÇÂÁÕÍÒ¡Òôբ¹ ¨ÐàÃÔÁãËŒ¹§ áÅÐ
è Œ † Öé è Ñè
Â×¹à´Ô¹µ‹Íä» â´Â·ÑÇ仨ÐàÃÔÁÂ×¹à´Ô¹ä´Œµ§áµ‹Ç¹·Õè 2 ËÅѧ¼‹ÒµÑ´ ·Ñ§¹Õ¨ÐãËŒ¼»ÇÂÍÍ¡¡íÒÅѧ
è è Ñé Ñ é é ÙŒ †
¢ÂѺ¢ŒÍµ‹Í (range of motion exercise) ËÃ×ÍÂ×´àÊŒ¹Â×´ÊÒ (stretching) ¡‹Í¹¡ÒÃÂ×¹à´Ô¹
(µÒÃÒ§·Õè 5) (5) â´Â·ÑÇ仨нƒ¡ãËŒ¼»ÇÂà´Ô¹ÍÍ¡¡íÒÅѧ䴌 10-15 ¹Ò·Õ áŌǨÐËÑ´ãËŒ¢¹Å§
è ÙŒ † Öé
ºÑ¹ä´ ËÃ×Í ·íÒ¡Ô¨¡ÃÃÁä´Œã¹ÃдѺ»ÃÐÁÒ³ 3-4 METs ¡‹Í¹ãËŒ¨íÒ˹‹ÒÂÍÍ¡¨Ò¡
âç¾ÂÒºÒÅËÃ×Í¡ÅѺºŒÒ¹ à¾ÃÒСԨÇѵûÃШíÒÇѹʋǹãË‹¨ÐÁÕÃдѺ¾Åѧ§Ò¹»ÃÐÁÒ³
3 - 4 METs
175.
148 ¡ÒÃÍÍ¡¡íÒÅѧËÅѧ¡Ò÷íÒËѵ¶¡ÒÃËÃ×ͼ‹ÒµÑ´ËÑÇã¨
µÒÃÒ§·Õè 2 áÊ´§à¡³±¡ÒèѴÃдѺ¤ÇÒÁàÊÕ§¢Í§ American Association of Cardiovascular
è
and Pulmonary Rehabilitation (AACVPR)(4)
Low Risk Moderate Risk High Risk
! No significant left ! Moderately impaired left ! Decreased left ventricular
ventricular dysfunction ventricular function function (E. of < 40%)
(E. of > 50%) (E. = 40% - 49%) ! Survivor of cardiac arrest or
! No resting or exercise- ! Signs/symptoms including sudden death
induced complex angina at moderate levels ! Complex ventricular
arrhythmias of exercise (5 – 6.9 METs) arrhythmias at rest or with
! Uncomplicated Ml; CABGs; or in recovery exercise
angioplasty, atherectomy, ! MI or cardiac surgery
or stent; complicated by cardiogenic
! Absence of CH., or shock. CH., and/or
signs/symptoms of signs/symptoms of
postevent ischemia postevent/procedure
! Normal hemodynamics ischemia
with exercise or recovery ! Abnormal hemodynamics
! Asymptomatic including with exercise (especially flat
absence of angina with or decreasing SBP or
exertion or recovery chronotropic incompetence
! .unctional capacity of > 7 with increasing workload)
METs ! Signs/symptoms including
! Absence of clinical angina pectoris at low levels
depression of exercise (< 5.0 METs) or
in recovery
! .unctional capacity of < 5.0
METs
! Clinically significant
depression
Low-risk classification is Moderate risk is assumed for Highest-risk classification is
assumed when each of the patients who do not meet the assumed with the presence of
descriptors in the category is classification of either high or any one of the descriptors
present low risk included in this category
ËÁÒÂà赯 MI = myocardial infarction; CABGs = coronary artery bypass surgery;
CH. = congestive heart failure; SBP = systolic blood pressure
176.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 149
µÒÃÒ§·Õè 3 ¢ŒÍËŒÒÁ㹡ÒÃÍÍ¡¡íÒÅѧ(4)
! Unstable angina
! SBP ¢³Ð¾Ñ¡ > 180 mm Hg ËÃ×Í DBP ¢³Ð¾Ñ¡ > 110 mm Hg ·Ñ§¹ÕµÍ§¾Ô¨ÒóÒ
é é Œ
໚¹ÃÒÂæ´ŒÇÂ
! Orthostatic blood pressure drop > 20 mm Hg ·ÕÁÍÒ¡ÒÃ
è Õ
! Critical aortic stenosis
! Acute systemic illness or fever
! Uncontrolled atrial or ventricular arrhythmias
! Uncontrolled sinus tachycardia (> 120 beats per minute)
! Uncompensated congestive heart failure
! Third-degree A-V block (without pacemaker)
! Active pericarditis or myocarditis
! Recent embolism
! Thrombophlebitis
! Resting ST displacement (> 2mm); > 3 mm if patient is taking digitalis
! Uncontrolled diabetes (resting blood glucose > 400 mg/dL)
! Severe orthopedic problems that would prohibit exercise
! Other metabolic problems such as acute thyroiditis, hypo- or hyperkalemia,
hypovolemia, etc.
µÒÃÒ§·Õè 4 âäËÃ×ÍÀÒÇзÕè·íÒãËŒà¡Ô´¡ÒÃàºÕè§ູ¢Í§á¹Ç·Ò§ËÃ×Íâ»Ãá¡ÃÁ·ÕèÇÒ§äÇŒ(4)
ÀÒÇÐà¨çº»†Ç·Õ辺ËÇÁ ÀÒÇÐá·Ã¡«ŒÍ¹·Ò§ËÑÇã¨áÅÐËÅÍ´àÅ×Í´
ÊÀҾËҧ¡ÒÂ͋͹áÍ ºÍººÒ§ (frailty) ÀÒÇÐàÅ×Í´ÍÍ¡ËÅѧ¼‹ÒµÑ´
âääµàÃ×ÍÃѧ
é ÀÒÇÐËÑÇã¨àµŒ¹¼Ô´»¡µÔ
âäËÅÍ´àÅ×Í´ÊÁͧ »Í´ÍÑ¡àʺµÔ´àª×Íé
âä¡Ãд١áÅТŒÍ ¡ÅŒÒÁà¹×ÍËÑÇ㨵Òª‹Ç§¼‹ÒµÑ´
é
ÊµÔ»Ò ¡ÒÃÃѺÃÙº¡¾Ã‹Í§
˜ Œ ËÑÇã¨ËŒÍ§Å‹Ò§«ŒÒ·íҧҹŴŧ
âäËÅÍ´àÅ×Í´ÊÁͧ
àǪÈÒʵ÷¹Âؤ 2553
Ñ 151
µÒÃÒ§·Õè 6 ¡Òõͺʹͧµ‹Í¡ÒÃÍÍ¡¡íÒÅѧ·Õ躋§ªÕéãËŒËÂØ´ÍÍ¡¡íÒÅѧã¹ÃÐÂмٌ»†ÇÂã¹(4)
! HR > 130 bpm or > 30 bpm above pre-exercise level
! Diastolic BP > 110 mm Hg
! Decrease in systolic BP > 10 mm Hg
! Significant ventricular or atrial arrhythmias
! Second- or third-degree heart block
! Signs/symptoms of exercise intolerance including angina pectoris and marked dyspnea
ÃÐÂзÕè 2 ª‹Ç§¾Ñ¡¿„œ¹ ໚¹ÃÐÂе‹Íà¹×èͧ¨Ò¡¼ÙŒ»†ÇÂã¹ ¤×Í »ÃÐÁÒ³ 4- 6 ÊÑ»´ÒËáá
ËÅѧÍÍ¡¨Ò¡âç¾ÂÒºÒÅ ÃÐÂйÕéÍÒ¨ãËŒ¼ÙŒ»†ÇÂÍÍ¡¡íÒÅѧ·Õ躌ҹËÃ×Íâç¾ÂÒºÒÅ¡çä´Œ â´Â»¡µÔ
¨Ðá¹Ð¹íÒãËŒ½ƒ¡·Õ躌ҹ ᵋã¹ÃÒ·ÕèÁÕ¤ÇÒÁàÊÕè§ÊÙ§¤ÇÃá¹Ð¹íÒãËŒÁÒ½ƒ¡·Õèâç¾ÂÒºÒŠ໇ÒËÁÒÂ
¢Í§¡Òýƒ¡ ¤×Í ¨ÐÁا์¹ãËŒ¤§ÃдѺ¤ÇÒÁÊÒÁÒö·Õ·Òä´Œ¡Í¹ÍÍ¡¨Ò¡âç¾ÂÒºÒÅ áÅÐàµÃÕÂÁ¼Ù»ÇÂ
‹ è í ‹ Œ †
ࢌÒÊÙÃÐÂзÕè 3 ÇÔ¸¡Òà ¤×Í
‹ Õ
! ¤‹ÍÂæ à¾ÔÁÃÐÂÐàÇÅÒ¡ÒÃÍÍ¡¡íÒÅѧãËŒ¹Ò¹¢Ö¹¨Ò¡ 5-10 ¹Ò·Õ ໚¹ 45 ¹Ò·Õ â´Â·íÒ·Ø¡Çѹ
è é
ËÃ×ÍÊÑ»´ÒËÅÐ 5 ¤Ãѧ ¡Å‹ÒǤ×Í ã¹ª‹Ç§áá·Õ·Òä´ŒäÁ‹¹Ò¹ ÍÒ¨·íÒÇѹÅÐ 2 Ãͺ ᵋàÁ×Í
é è í è
à¾ÔÁàÇÅÒä´Œ¹Ò¹¢Ö¹à»š¹ 45 ¹Ò·Õ ÊÒÁÒö½ƒ¡à¾Õ§ÇѹÅÐ 1 Ãͺ
è é
! ÍѵÃÒ¡ÒÃൌ¹¢Í§ËÑÇã¨ËÃ×ͪվ¨Ã¢³ÐÍÍ¡¡íÒÅѧà¾ÔÁ¢Ö¹¨Ò¡¢³Ð¾Ñ¡»ÃÐÁÒ³ 20 ¤Ãѧ/¹Ò·Õ
è é é
ËÃ×Í RPE »ÃÐÁÒ³ 11-13
! ª¹Ô´¢Í§¡ÒÃÍÍ¡¡íÒÅѧ¡Ò·չÂÁã¹ÃÐÂйÕé ¤×Í ¡ÒÃà´Ô¹ËÃ×Í»˜¹¨Ñ¡ÃÂÒ¹
è Ô ›
㹡óշÕèá¹Ð¹íÒãËŒÍÍ¡¡íÒÅѧʋǹᢹ µŒÍ§¤íÒ¹Ö§¶Ö§¡ÒÃËÒ¢ͧá¼Å¼‹ÒµÑ´ºÃÔàdz
sternum ¢Í§¼Ù»ÇÂ·Õ·Ò CABG ´ŒÇÂáÅÐ㹡óշ¨Ð½ƒ¡ÍÍ¡¡íÒÅѧª¹Ô´·ÕÁá経ҹµŒÍ§á¹Ð¹íÒãËŒ¼»ÇÂ
Œ † è í Õè è Õ ÙŒ †
¡¹éÒ˹ѡËÃ×ÍÍÍ¡áç㹢³ÐËÒÂã¨ÍÍ¡ áÅÐÇÒ§¹éÒ˹ѡŧ㹢³ÐËÒÂã¨à¢ŒÒ
í í
ÃÐÂзÕè 3 ¼ÙŒ»†Ç¹͡ ໚¹ÃÐÂзÕÁ§ãËŒ¼»Ç¡ÅѺÊÙÃдѺ¡Ô¨¡ÃÃÁ»¡µÔ â´Âá¹Ð¹íÒãËŒ½¡ÍÍ¡
è Ø‹ ÙŒ † ‹ ƒ
¡íÒÅѧ·Õ˹‹Ç¿„¹¿ÙËÇã¨áµ‹¡ÊÒÁÒö·íҷպҹ䴌 ໚¹ÃÐÂзս¡ÍÍ¡¡íÒÅѧª¹Ô´ aerobic à¾×Íãˌ䴌¤ÇÒÁ
è œ Ñ ç è Œ è ƒ è
ÊÁºÙóá¢ç§áç¢Í§ÃкºËÑÇã¨áÅÐËÅÍ´àÅ×Í´ 㪌àÇÅÒ»ÃÐÁÒ³ 6–8 ÊÑ»´ÒË áµ‹ã¹¡ÅØÁ¼Ù»Ç·ÕÁÕ ‹ Œ † è
¤ÇÒÁàÊÕ§ÊÙ§ÍҨ㪌àÇÅÒ¹Ò¹¶Ö§ 10-12 ÊÑ»´ÒË ÇÔ¸¡Òà ¤×Í
è Õ
! ÃÐÂÐàÇÅÒ¡ÒÃÍÍ¡¡íÒÅѧ 30 -60 ¹Ò·Õ ·íÒÍ‹ҧ¹ŒÍ ÊÑ»´ÒËÅÐ 3-5 ¤Ãѧ é
! ½ƒ¡·Õ¤ÇÒÁ˹ѡ»ÃÐÁÒ³ 40/50-85% ¢Í§ HRR ËÃ×Í RPE 12-16 ã¹·Ò§»¯ÔºµËÒ¡á¹Ð
è Ñ Ô
¹íÒãËŒ¼»Ç½ƒ¡ÍÍ¡¡íÒÅѧàͧ·ÕºÒ¹ ¨Ðá¹Ð¹íÒãËŒ¼»ÇÂ㪌 RPE »ÃÐÁÒ³ 11-13 à¾×ͤÇÒÁ
ÙŒ † è Œ ÙŒ † è
»ÅÍ´ÀÑÂ
! ª¹Ô´¢Í§¡ÒÃÍÍ¡¡íÒÅѧ¡Ò ¤×Í à´Ô¹ »˜¹¨Ñ¡ÃÂÒ¹ Ç‹Ò¹éÒ
› í
! ¡ÒûÃѺà»ÅÕ¹â»Ãá¡ÃÁ¨Ð¢Ö¹¡ÑºÃдѺ¤ÇÒÁàÊÕ§¢Í§¼Ù»ÇÂ
è é è Œ †
179.
152 ¡ÒÃÍÍ¡¡íÒÅѧËÅѧ¡Ò÷íÒËѵ¶¡ÒÃËÃ×ͼ‹ÒµÑ´ËÑÇã¨
ÃÐÂзÕè 4 ¤§ÊÀÒ¾ªÑèǪÕÇÔµ ໚¹ÃÐÂзռ»ÇµŒÍ§´ÙáÅ»¯Ôºµµ¹ áÅФ§¡ÒÃÍÍ¡¡íÒÅѧà¾×Í
è ÙŒ † Ñ Ô è
ÊØ¢ÀÒ¾·Õ´¢Í§Ã‹Ò§¡ÒÂáÅл‡Í§¡Ñ¹¡ÒÃ໚¹«éÒ (secondary prevention) ·Ñ§¹Õ¼»Ç·ըÐÍÍ¡¡íÒÅѧàͧ
è Õ í é é ÙŒ † è
áÅе‹Íà¹×ͧ¤ÇÃÊÒÁÒö·íÒ¡Ô¨¡ÃÃÁÍ‹ҧ¹ŒÍ 5 METs
è
ÊíÒËÃѺ¡Òýƒ¡ÍÍ¡¡íÒÅѧã¹ÃÐÂзÕè 3 áÅÐ 4 ¢Í§¼Ù»ÇÂâäËÑÇ㨠CAD ·Õ䴌ú¡Ò÷íÒ PCI
Œ † è Ñ
ËÃ×Í CABG ÊÒÁÒö㪌á¹Ç·Ò§¡ÒÃÍÍ¡¡íÒÅѧ·ÑÇä»·Õè American College of Sports Medicine (ACSM)
è
áÅÐ American Heart Association (AHA) á¹Ð¹íÒÊíÒËÃѺºØ¤¤Å·ÑèÇä»ä´Œáµ‹µŒÍ§»ÃѺà»ÅÕè¹ãËŒ
àËÁÒÐÊÁ¡ÑºÊÀÒÇТͧ¼Ù»ÇÂáÅÐãËŒ¤ÇÒÁÊíҤѡѺ warm up áÅÐ cool down ¤íÒá¹Ð¹íҢͧ ACSM
Œ †
áÅÐ AHA ÊíÒËÃѺºØ¤¤Å·ÕÁÍÒÂØ 18-65 »‚ ¤×Í “ãËŒ·Ò¡Ô¨¡ÃÃÁ·Ò§¡ÒÂẺáÍâúԤã¹ÃдѺ¤ÇÒÁáç
è Õ í
»Ò¹¡Åҧ͋ҧ¹ŒÍÂÇѹÅÐ 30 ¹Ò·Õ ÊÑ»´ÒËÅÐ 5 Çѹ ËÃ×Í ·íÒ¡Ô¨¡ÃÃÁ·Ò§¡ÒÂẺáÍâúԤã¹ÃдѺ
¤ÇÒÁáçÁÒ¡Í‹ҧ¹ŒÍÂÇѹÅÐ 20 ¹Ò·Õ ÊÑ»´ÒËÅÐ 3 Çѹ ·Ñ駹Õé ÍÒ¨¼ÊÁ¼ÊÒ¹¡Ô¨¡ÃÃÁ·Ñé§ÊͧẺ
ËÇÁ¡Ñ¹ä´Œ µÑÇÍ‹ҧ ઋ¹ à´Ô¹àÃçÇæ 30 ¹Ò·Õ ÊÑ»´ÒËÅÐ 2 Çѹ ËÇÁ¡Ñº¡ÒÃÇÔ§àËÂÒÐæ 20 ¹Ò·Õ ÊÑ»´ÒËÅÐ
è
2 Çѹ ¹Í¡¨Ò¡¹Õé¤Ç÷íÒ¡Ô¨¡ÃÃÁ·Õ褧ËÃ×ÍàÊÃÔÁÊÌҧ¡íÒÅѧáÅФÇÒÁ·¹·Ò¹¢Í§¡ÅŒÒÁà¹×éÍÍ‹ҧ¹ŒÍÂ
ÊÑ»´ÒËÅÐ 2 Çѹ áÅÐ ¶ŒÒºØ¤¤Å»ÃÒö¹Ò¨ÐÁÕ¤ÇÒÁÊÁºÙóá¢ç§áç¢Í§Ã‹Ò§¡ÒÂÁÒ¡¢Ö¹ ÁÕ¤ÇÒÁàÊÕ§ é è
µ‹Í¡ÒÃà¡Ô´âäàÃ×ÍÃѧ¹ŒÍÂŧ ËÃ×Í »‡Í§¡Ñ¹¹éÒ˹ѡµÑÇà¾ÔÁÁÒ¡¢Ö¹¡ç¤ÇÃÍÍ¡¡íÒÅѧà¾ÔÁÁÒ¡¢Ö¹¨Ò¡à¡³±
é í è é è é
¢Ñ¹µèÒ·Õá¹Ð¹íÒäÇŒà¹×ͧ¨Ò¡»ÃÔÁÒ³¢Í§¡Ò÷íÒ¡Ô¨¡ÃÃÁ·Ò§¡ÒÂÁÕ¤ÇÒÁÊÑÁ¾Ñ¹¸¡ºÀÒÇÐÊØ¢ÀÒ¾”(6) áÅÐ
é í è è Ñ
ä´ŒÁ¡ÒÃá¹Ð¹íÒ¡Ô¨¡ÃÃÁ·Ò§¡ÒÂÅѡɳÐઋ¹à´ÕÂǡѹÊíÒËÃѺ¼ÙʧÍÒÂØ·ÁÍÒÂØÁÒ¡¡Ç‹Ò 65 »‚ ËÃ×Í ºØ¤¤Å
Õ ŒÙ Õè Õ
·ÕÁÍÒÂØ 50-64 »‚ᵋÁÀÒÇÐà¨çº»†ÇÂàÃ×ÍÃѧ·Õ¨Ò¡Ñ´¡Ò÷íÒ¡Ô¨¡ÃÃÁ ᵋÁ»ÃÐà´ç¹·ÕµÍ§¾Ô¨ÒóÒ໚¹¾ÔàÈÉ
è Õ Õ é èí Õ è Œ
¤× Í ÃÐ´Ñ º ¤ÇÒÁË¹Ñ ¡ ¢Í§¡Ô ¨ ¡ÃÃÁ·Õè ·í Ò ¡Ô ¨ ¡ÃÃÁ·Õè ª‹ Ç Â¤§ËÃ× Í à¾Ôè Á ¤ÇÒÁÂ× ´ ËÂØ‹ ¹ (flexibility)
áÅСÒ֍µÑÇ (balance)(7)
ÊÃØ»
¡ÒÃÍÍ¡¡íÒÅѧ¨Ñ´à»š¹ÇÔ¸¡ÒÃÃÑ¡ÉÒ·ÕÊÒ¤ÑÍ‹ҧ˹֧ÊíÒËÃѺ¼Ù»ÇÂâäËÑÇ㨫֧¡ÒÃãËŒ¤Òá¹Ð¹íÒ
Õ èí è Œ † è í
¡ÒÃÍÍ¡¡íÒÅѧ໚¹ÊÔ§·ÕÁ¤ÇÒÁÊíҤѷըЪ‹ÇÂãËŒ¼»ÇÂÁÕ¤³ÀÒ¾ªÕǵ·Õ´¢¹ â´Â¼Ù»ÇÂâäËÑÇã¨ÊÒÁö
è è Õ è ÙŒ † Ø Ô è Õ Öé Œ †
ÍÍ¡¡íÒÅѧ䴌µ§áµ‹ªÇ§·Õ¾¡ÃÑ¡ÉÒµÑÇã¹âç¾ÂÒºÒÅáÅÐÊÒÁÒö·Õ¨ÐÍÍ¡¡íÒÅѧµ‹Íà¹×ͧ仵ÅÍ´ªÕǵ
Ñé ‹ è Ñ è è Ô
à¾×ÍÊØ¢ÀÒÇзÕá¢ç§áçÊÁºÙó¢Í§Ã‹Ò§¡Òµ‹Íä» ª¹Ô´¢Í§¡ÒÃÍÍ¡¡íÒÅѧ·Õá¹Ð¹íÒãËŒ·Òã¹ÃÐÂÐÂÒÇ ¤×Í
è è è í
¡ÒÃÍÍ¡¡íÒÅѧẺáÍâúԤ ¤ÃѧÅÐ 20-60 ¹Ò·Õ¢¹¡ÑºÃдѺ¤ÇÒÁ˹ѡ¢Í§¡ÒÃÍÍ¡¡íÒÅѧ áÅÐÍÍ¡¡íÒÅѧ
é Öé
·íÒÊÑ»´ÒËÅÐ 3-5 ¤Ãѧé
àÍ¡ÊÒÃ͌ҧÍÔ§
1. American College of Sports Medicine. ACSM’s guidelines for exercise testing and prescription. 7th ed. Lippincott
Williams & Wilkins; 2006.
2. Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. Exercise-based rehabilitation for coronary
heart disease. Cochrane Database Syst Rev. 2001(1):CD001800.
180.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 153
3. Taylor RS, Brown A, Ebrahim S, Jolliffe J, Noorani H, Rees K, et al. Exercise-based rehabilitation for patients
with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med
2004;116(10):682-92.
4. American Association of Cardiovascular and Pulmonary Rehabilitation. Guidelines for cardiac rehabilitation and
secondary prevention programs. 3rd ed. Champaign,IL: Human Kinetics; 1999.
5. Pollock ML, Gomes PS. Exercise prescription. In: Wenger NK, Smith LK, .roelicher ES, Comoss PM, editors.
Cardiac rehabilitation: a guide to practice in the 21st century. New York: Marcel Dekker; 1999. p. 49-65.
6. Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, .ranklin BA, et al. Physical activity and public health:
updated recommendation for adults from the American College of Sports Medicine and the American Heart
Association. Circulation 2007;116(9):1081-93.
7. Nelson ME, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, et al. Physical activity and public health
in older adults: recommendation from the American College of Sports Medicine and the American Heart
Association. Circulation 2007;116(9):1094-105.
182.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 155
22
¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂã¹âä¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§
ÍÒ¨ÒÃÂÇÔÅÒÇѳ ¶ÔÃÀѷþ§È
ÀÒ¤ÇÔªÒàǪÈÒʵÿ¹¿Ù ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
„œ ÔÔ
»ÃÐ⪹¢Í§¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂã¹¼ÙŒ·ÕèÁÕ¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§
¡ÒÃÍÍ¡¡íÒÅѧ¡Ò¶×Í໚¹Ê‹Ç¹Ë¹Ö§¢Í§â»Ãá¡ÃÁ¡ÒûÃѺà»ÅÕ¹¾ÄµÔ¡ÃÃÁ áÅСÒôíÒà¹Ô¹ªÕǵ
è è Ô
à¾×èÍ»‡Í§¡Ñ¹ ÃÑ¡ÉÒáÅФǺ¤ØÁ¤ÇÒÁ´Ñ¹âÅËÔµ ·Ñé§ã¹¼ÙŒ·ÕèÁÕ¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§áÅмٌ·ÕèÁÕ¤ÇÒÁ´Ñ¹âÅËÔµ
ÍÂÙ‹ã¹à¡³±»¡µÔ¨Ò¡¡ÒÃÃǺÃÇÁËÅÒ¡ÒÃÈÖ¡ÉÒ Hagberg áÅФ³Ð(1)¾ºÇ‹Ò¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂ
Í‹ҧÊÁèÒàÊÁÍÊÒÁÒöŴ¤ÇÒÁ´Ñ¹«ÕÊâµÅÔ¡áÅФÇÒÁ´Ñ¹ä´áÍÊâµÅԡŧ䴌 11 áÅÐ 8 ÁÔÅÅÔàÁµÃ»ÃÍ·
í
µÒÁÅíҴѺ
ËÅѧÍÍ¡¡íÒÅѧ¡Ò»ÃÐÁÒ³ 10 ÊÑ»´ÒË ¤ÇÒÁ´Ñ¹·Ñ§«ÕÊâµÅÔ¡áÅÐä´áÍÊâµÅÔ¡¨ÐŴŧÍ‹ҧ
é
ÁÕ¹ÂÊíÒ¤Ñ áÅÐàÁ×ÍÍÍ¡¡íÒÅѧ¡ÒÂà¡Ô¹ 20 ÊÑ»´ÒË ¾ºÇ‹Ò¤ÇÒÁ´Ñ¹«ÕÊâµÅÔ¡ÂѧÊÒÁÒöŴŧ䴌͡
Ñ è Õ
¢³Ð·Õè¤ÇÒÁ´Ñ¹ä´áÍÊâµÅÔ¡äÁ‹ÁÕ¡ÒÃŴŧà¾ÔèÁ¢Öé¹ ¼ÙŒ·ÕèÁÕ¤ÇÒÁ´Ñ¹âÅËÔµÍÂÙ‹ã¹à¡³±»¡µÔ¨ÐÁÕ
(1)
¤ÇÒÁ´Ñ¹Å´Å§àÁ×ÍÍÍ¡¡íÒÅѧ¡Ò ᵋ¹Í¡NjÒàÁ×Íà·Õº¡Ñº¼Ù·Á¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§ áÅФÇÒÁ´Ñ¹âÅËÔµ
è Œ è Œ Õè Õ
·ÕŴŧ¹Ñ¹ÂѧÍÂÙã¹à¡³±»¡µÔ
è é ‹ (2, 3)
¼Å¢Í§¡ÒÃÍÍ¡¡íÒÅѧ¡Òµ‹Í¤ÇÒÁ´Ñ¹âÅËÔµ
(Effects of exercise on blood pressure)
1. ¡ÒÃÍÍ¡¡íÒÅѧ¡Òª¹Ô´·ÕÁ¡ÒÃà¤Å×͹äËǢͧ¢ŒÍ (Isotonic exercise)
è Õ è
¼Ù·Á¤ÇÒÁ´Ñ¹âÅËÔµ»¡µÔ cardiac output (CO) ¨Ðà¾ÔÁ¢Ö¹¢³ÐÍÍ¡¡íÒÅѧ¡Ò ʋ§¼Å·íÒãËŒ
Œ Õè Õ è é
ËÑÇã¨àµŒ¹àÃçÇ¢Ö¹ stroke volume (SV) à¾ÔÁ¢Ö¹ áÅÐËÑÇ㨺պµÑÇáç¢Ö¹ à¾×ÍÊ‹§àÅ×Í´ä»àÅÕ§¡ÅŒÒÁà¹×Í·Õè
é è é é è é é
ÍÍ¡¨Ò¡áçà¾ÔèÁ¢Öé¹ ¢³Ð·ÕèÊ‹§àÅ×Í´ä»àÅÕ駡ŌÒÁà¹×éÍ·ÕèäÁ‹ä´ŒÍÍ¡áçáÅÐÍÇÑÂÇÐÀÒÂã¹Å´¹ŒÍÂŧ
¼ÅÊØ·¸Ô¤Í¤ÇÒÁ´Ñ¹«ÕÊâµÅÔ¡à¾ÔÁ¢Ö¹ ¤ÇÒÁ´Ñ¹ä´áÍÊâµÅÔ¡¤§·ÕËÃ×ÍÁÕ¡ÒÃà»ÅÕ¹á»Å§àÅ硹ŒÍ áÅÐ
× è é è è
systemic vascular resistance (SVR) Ŵŧ (4)
¼Ù·Á¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§ÃдѺ¹ŒÍ¶֧»Ò¹¡ÅÒ§ ¶Ö§áÁŒ CO à¾ÔÁ¢Ö¹Í‹ҧ»¡µÔ ᵋ ¤ÇÒÁ´Ñ¹
Œ Õè Õ è é
·Ñ§«ÕÊâµÅÔ¡áÅÐä´áÍÊâµÅÔ¡áÅÐ SVR ¨Ðà¾ÔÁ¢Ö¹àÁ×Íà»ÃÕºà·Õº¡Ñº¼Ù·Á¤ÇÒÁ´Ñ¹âÅËÔµ»¡µÔ ¼Ù·ÁÕ
é è é è Œ Õè Õ Œ Õè
¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§ÃдѺÃعáç CO ¨ÐµèÒ¡Ç‹Ò»¡µÔ·¤ÇèÐ໚¹ à¾ÃÒÐ SV Ŵŧ ʋǹ¤ÇÒÁ´Ñ¹«ÕÊâµÅÔ¡
í Õè
áÅÐä´áÍÊâµÅÔ¡áÅÐ SVR ¨Ðà¾ÔÁ¢Ö¹Í‹ҧÁÒ¡
è é
183.
156 ¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂã¹âä¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§
2. ¡ÒÃÍÍ¡¡íÒÅѧ¡Òª¹Ô´·ÕÁ¡ÒÃà¡Ã秡ŌÒÁà¹×Í â´ÂäÁ‹Á¡ÒÃà¤Å×͹äËǢͧ¢ŒÍ
è Õ é Õ è
(Isometric exercise)
㹤¹»¡µÔ àÁ×ÍÍÍ¡¡íÒÅѧ¡Òª¹Ô´¹Õé ¤ÇÒÁ´Ñ¹âÅËÔµ·Ñ§¤ÇÒÁ´Ñ¹«ÕÊâµÅÔ¡áÅÐä´áÍÊâµÅÔ¡¨Ð
è é
à¾ÔÁ¢Ö¹ «Ö§à»š¹¼ÅʋǹãË‹¨Ò¡ CO à¾ÔÁ¢Ö¹ â´Â·Õè SVR ÁÕ¡ÒÃà»ÅÕ¹á»Å§à¾Õ§àÅ硹ŒÍ µÃ§¡Ñ¹¢ŒÒÁ
è é è è é è
¡Ñº¼ÙŒ·ÕèÁÕ¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§ «Ö觤ÇÒÁ´Ñ¹âÅËÔµ·Õèà¾ÔèÁ¢Öé¹Ê‹Ç¹ãˋ໚¹¼ÅÁÒ¨Ò¡ systemic vascular
resistance ·Õèà¾ÔèÁ¢Öé¹ à¹×èͧ¨Ò¡ËÑÇã¨ËŒÍ§Å‹Ò§«ŒÒÂÁÕ¢¹Ò´âµ (left ventricle hypertrophy) ËÃ×Í
beta-adrenergic system ·íҧҹ䴌äÁ‹àµçÁ·Õè ·íÒãËŒ CO äÁ‹à¾ÔÁ¢Ö¹ËÃ×Íà¾ÔÁ¢Ö¹à¾Õ§àÅ硹ŒÍÂ(4)
è é è é
¼ÙŒà»š¹¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§¨ÐÁÕ¤ÇÒÁ´Ñ¹âÅËÔµà¾ÔèÁ¢Öé¹·Ñ駫ÕÊâµÅÔ¡áÅÐä´áÍÊâµÅÔ¡ÁÒ¡¡Ç‹Ò
¼Ù·Á¤ÇÒÁ´Ñ¹âÅËÔµ»¡µÔ àÁ×ÍÍÍ¡¡íÒÅѧ¡Òª¹Ô´·ÕÁ¡ÒÃà¤Å×͹äËǢͧ¢ŒÍ (isotonic exercise) ËÃ×Í
Œ Õè Õ è è Õ è
ÍÍ¡¡íÒÅѧ¡Òª¹Ô´·ÕèÁÕ¡ÒÃà¡Ã秡ŌÒÁà¹×éÍ â´ÂäÁ‹ÁÕ¡ÒÃà¤Å×è͹äËǢͧ¢ŒÍ (isometric exercise)
·Ø¡ÃдѺ¤ÇÒÁ˹ѡàºÒ áÅСÒÃÍÍ¡¡íÒÅѧ¡Òª¹Ô´·ÕÁ¡ÒÃà¡Ã秡ŌÒÁà¹×Í (isometric exercise) ÍÒ¨
è Õ é
Ê‹§¼Åµ‹ÍÃдѺ¤ÇÒÁ´Ñ¹ã¹ËÅÍ´àÅ×Í´à¾ÔÁÁÒ¡¡Ç‹Ò¡ÒÃÍÍ¡¡íÒÅѧ¡Òª¹Ô´·ÕÁ¡ÒÃà¤Å×͹äËǢͧ¢ŒÍ
è è Õ è
(isotonic exercise)
¡ÒÃÊÑ觡ÒÃÍÍ¡¡íÒÅѧ¡Ò (Exercise prescription)
ËÅÑ¡¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂÊíÒËÃѺ¼ÙŒãË‹·ÕèÁÕÊØ¢ÀÒ¾á¢ç§áçÊÒÁÒö㪌á¹Ç·Ò§¡ÒÃÃÑ¡ÉҢͧ
American College of Sports Medicine (ACSM) Guidelines 䴌ઋ¹à´ÕÂǡѺ¼Ù໚¹¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§
Œ
ÃÐÂÐ 1 áÅÐ 2 Í‹ҧäáçµÒÁäÁ‹á¹Ð¹íÒ¡ÒÃÍÍ¡¡íÒÅѧ¡Òª¹Ô´ÁÕá経ҹ㹼Ù໚¹¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§
(5)
Œ
ÃÐÂÐ 3 (¤ÇÒÁ´Ñ¹âÅËÔµµÑ§áµ‹ 180/110 ÁÔÅÅÔàÁµÃ»ÃÍ·) à¹×ͧ¨Ò¡ÍÒ¨·íÒãËŒ SVR ÊÙ§¢Ö¹áÅзíÒãËŒ
é (6)
è é
ÁÕ¼ÅàÊÕµ‹ÍÍÇÑÂÇÐÍ×¹æ ä´Œ â´Â·ÑÇ仡ÒÃÍÍ¡¡íÒÅѧ¡Ò¨оԨÒóÒͧ¤»ÃСͺµ‹Ò§æ ´Ñ§µ‹Í仹Õé
è è
1. »ÃÐàÀ·¢Í§¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂ
á¹Ð¹íÒ¡ÒÃÍÍ¡¡íÒÅѧ¡Òª¹Ô´áÍâúԡËÃ×Í¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂà¾×Íà¾ÔÁ¤ÇÒÁ·¹·Ò¹ â´Â
è è
์¹¡ÒÃÍÍ¡¡íÒÅѧ¡Ò¢ͧ¡ÅŒÒÁà¹×Í àª‹¹ à´Ô¹ ÇÔ§ ൌ¹ áÍâúԡ¡Ô¨¡ÃÃÁ¨Ñ§ËÇÐ Ç‹Ò¹éÒ ÃíÒÁǨչ
é è í
໚¹µŒ¹ ʋǹ¡ÒÃÍÍ¡¡íÒÅѧ¡Òª¹Ô´ÁÕá経ҹäÁ‹¤ÍÂÁÕº·ºÒ·ÁÒ¡¹Ñ¡ã¹¡ÒÃÅ´¤ÇÒÁ´Ñ¹(7) ´Ñ§¹Ñ¹¨Ö§
‹ é
äÁ‹á¹Ð¹íÒãˌ໚¹¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂËÅÑ¡ÊíÒËÃѺ¼Ù໚¹¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§(8, 9) Í‹ҧäáçµÒÁ¡ÒÃÍÍ¡¡íÒÅѧ
Œ
¡Òª¹Ô´ÁÕá経ҹÍÒ¨ÁÕ¼ÅÅ´¤ÇÒÁ´Ñ¹âÅËԵ䴌ºÒ§¶ŒÒÍÍ¡¡íÒÅѧ¡ÒÂËÇÁ¡Ñº¡ÒÃÍÍ¡¡íÒÅѧ¡Òª¹Ô´áÍ
Œ
âúԡ ¹Í¡¨Ò¡¹Ñ¹Âѧª‹ÇÂà¾ÔÁ¤ÇÒÁá¢ç§áçáÅÐàÊÃÔÁ¤ÇÒÁÊÒÁÒö㹡ÒûÃСͺ¡Ô¨¡ÃÃÁ»ÃШíÒÇѹ
é è
¨Ö§á¹Ð¹íÒãˌ໚¹¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂàÊÃÔÁµ‹Í¨Ò¡¡ÒÃÍÍ¡¡íÒÅѧ¡Òª¹Ô´áÍâúԡ(10)
2. ¤ÇÒÁ˹ѡàºÒ¢Í§¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂ
ÁÕ¢ŒÍÊÃØ»·ÕèªÑ´à¨¹áÅÐàËç¹¾ŒÍ§µŒÍ§¡Ñ¹Ç‹Ò¼ÙŒ»†Ç¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§¤ÇÃàÃÔèÁÍÍ¡¡íÒÅѧ¡ÒÂ
Í‹ҧÊÁèÒàÊÁÍ´ŒÇ¤ÇÒÁ˹ѡàºÒÃŒÍÂÅÐ 50 ¶Ö§ 70 ¢Í§¡ÒÃ㪌ÍÍ¡«ÔਹÊÙ§ÊØ´ «Ö§à»š¹¤ÇÒÁ˹ѡàºÒ
í è
ÃдѺ¹ŒÍ¶֧»Ò¹¡ÅÒ§ à¹×ͧ¨Ò¡¡ÒÃÍÍ¡¡íÒÅѧ¡Ò´ŒÇ¤ÇÒÁ˹ѡàºÒÃдѺÊÙ§ÍÒ¨äÁ‹ä´ŒÁ»ÃÐ⪹
è Õ
ÁÒ¡¢Ö¹ ÃÇÁ·Ñ§ÂѧÍÒ¨·íÒãËŒà¡Ô´¤ÇÒÁàÊÕ§µ‹Í¡ÒúҴà¨çº¢Í§¡ÅŒÒÁà¹×ÍáÅÐÊ‹§¼ÅàÊÕµ‹ÍÃкºËÑÇã¨áÅÐ
é é è é
ËÅÍ´àÅ×Í´´ŒÇÂ
158 ¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂã¹âä¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§
4. ¤ÇÒÁ¶Õ¢Í§¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂ
è
¢Ö¹¡Ñº¤ÇÒÁ˹ѡàºÒ㹡ÒÃÍÍ¡¡íÒÅѧ¡Ò â´Â¤ÇÒÁ˹ѡÃдѺ»Ò¹¡ÅÒ§ ¤ÇÃÍÍ¡¡íÒÅѧ¡ÒÂ
é
ÊÑ»´ÒËÅÐ 3-5 Çѹ ¶ŒÒÍÍ¡¡íÒÅѧ¡ÒÂÃдѺàºÒÊÒÁÒöÍÍ¡¡íÒÅѧ¡ÒÂä´Œ·¡Çѹ(13)
Ø
ÁÕ¡ÒÃÇԨ·վºÇ‹Ò¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂÊÑ»´ÒËÅÐ 3 Çѹ໚¹Í‹ҧ¹ŒÍ¨Ðä´Œ»ÃÐ⪹㹡ÒÃ
Ñ è
Å´¤ÇÒÁ´Ñ¹âÅËÔµáÅл‡Í§¡Ñ¹¡ÒÃà¡Ô´âäËÑÇã¨áÅÐËÅÍ´àÅ×Í´ä´Œ Í‹ҧäáçµÒÁ¾ºÇ‹Ò¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂ
·Ø¡ÇѹÊÒÁÒöŴ¤ÇÒÁ´Ñ¹âÅËԵ䴌ÁÒ¡¡Ç‹Ò¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂÊÑ»´ÒËÅÐ 3 Çѹ(3)
¨Ò¡¡ÒÃÈÖ¡ÉÒ¤ÇÒÁÊÑÁ¾Ñ¹¸¢Í§µÑÇá»ÃàÃ×ͧ¤ÇÒÁ˹ѡàºÒ ÃÐÂÐàÇÅÒáÅФÇÒÁ¶Õ㹡ÒÃ
è è
ÍÍ¡¡íÒÅѧ¡Òµ‹Í¡ÒÃŴŧ¢Í§¤ÇÒÁ´Ñ¹âÅËÔµ ¾ºÇ‹ÒäÁ‹ÁµÇá»Ãã´·ÕÁ¤ÇÒÁÊÑÁ¾Ñ¹¸Í‹ҧÁÕ¹ÂÊíÒ¤Ñ
Õ Ñ è Õ Ñ
¡Ñº¡ÒÃà»ÅÕ¹á»Å§¢Í§¡ÒÃÅ´¤ÇÒÁ´Ñ¹âÅËÔµ ᵋàÁ×ÍÃÇÁµÑÇá»Ã·Ñ§ 3 µÑÇ ¾ºÇ‹ÒÁÕ¤ÇÒÁÊÑÁ¾Ñ¹¸áÅÐ
è (3)
è é
ÁÕ¹ÂÊíҤѡѺ¡ÒÃà»ÅÕ¹á»Å§¢Í§ÃдѺ¤ÇÒÁ´Ñ¹âÅËÔµ
Ñ è (3)
ʋǹ¡ÒÃÍÍ¡¡íÒÅѧ¡Òª¹Ô´á経ҹãËŒÍÍ¡¡íÒÅѧ¡Ò»ÃÐÁÒ³ 2-3 Çѹµ‹ÍÊÑ»´ÒË(9)
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Hagberg JM, Park JJ, Brown MD. The role of exercise training in the treatment of hypertension. An update.
Sports Med 2000;30:193-206.
2. .agard RH. Exercise characteristics and the blood pressure response to dynamic physical training. Med Sci
Sports Exerc 2001;33:484-92.
3. Keely GA, Kelly KA, Tran ZV. Aerobic exercise and resting blood pressure: a meta-analytic review of randomized,
controlled trials. Prev Cardiol 2001;4:73-80.
4. Swain R, Kaplan B. Treatment hypertension in active patients: which agents work best with exercise?
Physician Sportsmed 1997;25:1-13.
5. American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription. 7th ed.
Baltimore (MD): Lippincott Williams & Wilkins, 2006.
6. Keely GA, Kelly KS. Progressive resistance exercise and resting blood pressure: a meta-analysis of randomized
controlled trials. Hypertension 2000;35:838-43.
7. Pollock ML, .ranklin BA, Gary J, et al. Resistance exercise in individuals with and without cardiovascular
disease: benefits, rationale, safety, and prescription: an advisory from the Committee on Exercise, Rehabilitation,
and Prevention, Council on Clinical Cardiology, American Heart Association. Circulation 2000;101:828-33.
8. American College of Sports Medicine position stand. Physical activity, physical fitness, and hypertension. Med
Sci Sports Exerc 1993;25:1-10.
9. .agard RH, Tipton CM. Physical activity, fitness and hypertension. In: Bouchard C, Shephard RJ, Stephens
T, eds. Physical Activity, .itness and Health. Champaign (IL): Human Kinetics; 1994;633-55.
10. La.ontaine T. Resistance training for patients with hypertension. Strength Condition 1997;19:5-9.
11. Pollock M, .ranklin B, Balady G, Chaitman B, .leg J, .letcher B, et al. AHA science advisory. Resistance
exercise in individuals with and without cardiovascular disease. Circulation 2000;101:828-33.
12. .ranklin B, Whaley M, Holey E. American College of Sports Medicine’s Guidelines for Exercise Testing and
Prescription. 6th ed. Baltimore (MD): Lippincott Williams & Wilkins; 2000.
13. American College of Sports Medicine position stand. The recommended quantity and quality of exercise for
developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med Sci
Sports Exerc 1998;30:975-91.
162 ¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂã¹âäàºÒËÇÒ¹
àÍ¡ÊÒÃ͌ҧÍÔ§
1. American diabetes Association. Standards of medical care for patients with diabetes mellitus. Diabetes Care
2000;23:532-42.
2. Gordon N.. The exercise prescription. In: The Health Professional’s guide to diabetes and exercise. Alexandria,
VA: American Diabetes Association, 1995:70-82.
3. Berger M. Adjustment of insulin therapy. In: The health professional’s guide to diabetes and exercise. Alexandria,
VA: American Diabetes Association, 1995:116-22.
4. Albright AL. Diabetes. In: Durstine JL, ed. ACSM’s Exercise management for persons with chronic diseased
and disabilities. Champaign, IL: Human kinetics, 1997:94-100.
5. Kenny W, Humphrey R, Bryant C. ACSM’s guidelines for exercise testing and prescription. 7th ed. Philadelphia:
Williams & Wilkin: 2005.
168 Whiplash Injury
»Ç´ÃعáçµÑ§áµ‹àÃÔÁµŒ¹ (higher initial pain intensity) ໚¹»˜¨¨Ñ·ժ´à¨¹·Õº§ºÍ¡¶Ö§¡Òÿ„¹µÑÇáÅÐ
é è è Ñ è ‹ œ
ËÒ¨ҡâ䪌ÒáÅзíÒãËŒ»Ç´àÃ×ÍÃѧ ʋǹÍÒÂØ à¾ÈËÔ§ angular deformity of cervical spine, rear-end
é
collision áÅÐ compensation äÁ‹Á¼Åµ‹Í¡Òÿ„¹µÑÇ «Ö§»˜¨¨ÑÂàËÅ‹Ò¹ÕÍҨ໚¹µÑǪ‹ÇÂ㹡ÒÃÇҧἹ¡ÒÃ
Õ œ è é
ÃÑ¡ÉÒáÅл‡Í§¡Ñ¹ÍÒ¡ÒÃàÃ×ÍÃѧ
é (42)
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Spitzer WO, Skovron ML, Salmi LR, Cassidy DJ, Duranceau J, Suissa S, et al. Scientific monograph of the
Quebec Task .orce on whiplash-associated disorders: redefining “whiplash” and its management. Spine 1995;
20(8 Suppl):1S-73S.
2. C?t? P, Cassidy JD, Carroll L, .rank JW, Bombardier C. A systematic review of the prognosis of acute
whiplash and a new conceptual framework to synthesize the literature. Spine 2001; 26(19): E445–58.
3. Barnsley L, Lord SM, Bogduk N. Whiplash injury. Pain 1994;58:283–307.
4. DePalma MJ, Slipman CW. Treatment of common neck problems. In: Braddom RL, editor. Physical Medicine
& Rehabilitation. 3rd ed. China: Saunders Elsevier Inc; 2007. p.797-824.
5. Grauer JN, Panjabi MM, Cholewicki J, Nibu K, Dvorak J. Whiplash produces an S-shaped curvature of the
neck with hyperextension at lower levels. Spine 1997;22(21):2489–94.
6. Nederhand MJ, Hermens HJ, Ijzerman MJ, Turk DC, Zilvold G. Cervical muscle dysfunction in the chronic
whiplash associated disorder grade II (WAD-II). Spine 2000;25:1938-43.
7. Lord SM, Barnsley L, Wallis BJ, McDonald GJ, Bogduk N. Percutaneous radiofrequency neurotomy for chronic
cervical zygapophyseal-joint pain. N Engl J Med 1996;335:1721-6.
8. Binder A. The diagnosis and treatment of nonspecific neck pain and whiplash. Eura Medicophys 2007;43:79-
89.
9. Ide M, Ide J, Yamaga M, Takagi K. Symptoms and signs of irritation of the brachial plexus in whiplash injuries.
J Bone Joint Surg Br 2001;83:226-9.
10. Rodriquez AA, Barr KP, Burns SP. Whiplash: pathophysiology, diagnosis, treatment, and prognosis. Muscle
Nerve 2004;29:768–81.
11. .errari R, Russell AS, Carroll LJ, Cassidy JD. A re-examination of the whiplash-associated disorders (WAD) as
a systemic illness. Ann Rheum Dis 2005;64:1337-42.
12. Buskila D, Neumann L, Vaisberg G, Alkalay D, Wolfe .. Increased rates of fibromyalgia following cervical spine
injury. A controlled study of 161 cases of traumatic injury. Arthritis Rheum 1997;40:446-52.
13. Curatolo M, Petersen-.elix S, Arendt-Nielsen L, Giani C, Zbinden AM, Radanov BP. Central hypersensitivity in
chronic pain after whiplash injury. Clin J Pain 2001;17:306-15.
14. Koelbaek JM, Graven-Nielsen T, Schou OA, Arendt-Nielsen L. Generalised muscular hyperalgesia in chronic
whiplash syndrome. Pain 1999;83:229-34.
15. Sterling M, Jull G, Vicenzino B, Kenardy J. Sensory hypersensitivity occurs soon after whiplash injury and is
associated with poor recovery. Pain 2003;104:509-17.
16. Scott D, Jull G, Sterling M. Widespread sensory hypersensitivity is a feature of chronic whiplash-associated
disorder but not chronic idiopathic neck pain. Clin J Pain 2005;21:175-81.
17. Sal? H, Isberg A. Delayed temporomandibular joint pain and dysfunction induced by whiplash trauma: a
controlled prospective study. J Am Dent Assoc 2007;138(8):1084-91.
196.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 169
18. Gupta V, Posner B. Trauma to the long thoracic nerve and associated scapula winging in a low-velocity rear-
end automobile collision: case report. J Trauma 2004;57(2):402–3.
19. Omar N, Alvi ., Srinivasan MS. An unusual presentation of whiplash injury: long thoracic and spinal accessory
nerve injury. Eur Spine J 2007;16 (Suppl 3):S275–S277.
20. Ronnen HR, de Korte PJ, Brink PR, van der Bijl HJ, Tonino AJ, .ranke CL. Acute whiplash injury: is there a
role for MR imaging?—a prospective study of 100 patients. Radiology 1996;201(1):93–6.
21. Pettersson K, Hildingsson C, Toolanen G, .agerlund M, Bj?rnebrink J. Disc pathology after whiplash injury: a
prospective magnetic resonance imaging and clinical investigation. Spine 1997;22:283–7.
22. Eck JC, Hodges SD, Humphreys SC. Whiplash: a review of a commonly misunderstood injury. Am J Med
2001;110:651–6.
23. Kongsted A, Sorensen JS, Andersen H, Keseler B, Jensen TS, Bendix T. Are early MRI findings correlated
with long-lasting symptoms following whiplash injury? A prospective trial with 1-year follow-up. Eur Spine J
2008;17:996–1005.
24. Juan .J. Use of botulinum toxin-A for musculoskeletal pain in patients with whiplash associated disorders.
BMC Musculoskelet Disord. 2004;5:5(1-10).
25. Borchgrevink GE, Kaasa A, McDonagh D, Stiles TC, Haraldseth O, Lereim I. Acute treatment of whiplash
neck sprain injuries. Spine 1998;23(1):25–31.
26. Rosenfeld M, Seferiadis A, Carlsson J, Gunnarsson R. Active intervention in patient with whiplash-associated
disorder improves long-term prognosis. Spine 2003;28:2491–8.
27. Seferiadis A, Rosenfeld M, Gunnarsson R. A review of treatment interventions in whiplash-associated disorders.
Eur Spine J 2004; 13(5):387-97.
28. Scholten-Peeters G, Bekkering G, Verhagen A, Windt D Van der, Lanser K, Hendricks E, et al. Clinical practice
guideline for the physiotherapy of outpatients with whiplash associated disorders. Spine 2002;27(4):412-22.
29. Conlin A, Bhogal S, Sequeira K, Teasell R. Treatment of whiplash-associated disorders—part I: Non-invasive
interventions. Pain Res Manag 2005;10(1):21-32.
30. .reeman MD, Croft AC, Rossignol AM. Whiplash associated disorders: refining whiplash and it’s management’
by the Quebec Task .orce. Spine 1998,23(9):1043-49.
31. Trinh K, Graham N, Gross A, Goldsmith C, Wang E, Cameron I, et al. Acupuncture for neck disorders. Spine
2007;32(2):236-43.
32. Kong J, .ufa D, Gerber A, Rosman I, Vangel M, Graceley R, et al. Psychophysical outcomes from a
randomised pilot study of manual, electro and sham acupuncture treatment on experimentally induced thermal
pain. Journal of Pain 2005;6(1):55-64.
33. Verhagen AP, Scholten-Peeters G, van Wijngaarden S, de Bie RA, Bierma-Zeinstra SMA. Conservative treatments
for whiplash [Systematic Review]. Cochrane Database Syst Rev2007;4:4.
34. Nijs J, Van Oosterwijck J, De Hertogh W. Rehabilitation of chronic whiplash: treatment of cervical dysfunctions
or chronic pain syndrome? Clin Rheumatol 2009;28(3):243-51.
35. Stewart MJ, Maher CG, Refshauge KM, Herbert RD, Bogduk N, Nicholas M. Randomized controlled trial of
exercise for chronic whiplash-associated disorders. Pain 2007;128:59-68.
36. Jull G, Sterling M, Kenardy J, Beller E. Does the presence of sensory hypersensitivity influence outcomes of
physical rehabilitation for chronic whiplash? - A preliminary RCT. Pain 2007;129(2):28-34.
37. McDonald GJ, Lord SM, Bogduk N. Long-term follow-up of patients treated with cervical radiofrequency
neurotomy for chronic neck pain. Neurosurgery 1999,45:61-8.
197.
170 Whiplash Injury
38. Conlin A, Bhogal S, Sequeira K, Teasell R. Treatment of whiplash-associated disorders—part II: Medical and
surgical interventions. Pain Res Manag 2005;10(1):33-40.
39. Kamper SJ, Rebbeck TJ, Maher CG, McAuley JH, Sterling M. Course and prognostic factors of whiplash: a
systematic review and meta-analysis. Pain 2008;138(3):617-29.
40. Dufton JA, Kopec JA, Wong H, Cassidy JD, Quon J, McIntosh G, et al. Prognostic factors associated with
minimal improvement following acute whiplash-associated disorders. Spine 2006;31(20):E759–65.
41. Atherton K, Wiles NJ, Lecky .E, Hawes SJ, Silman AJ, Macfarlane GJ, et al. Predictors of persistent neck pain
after whiplash injury. Emerg Med J 2006;23:195–201
42. Scholten-Peeters GG, Verhagen AP, Bekkering GE, van der Windt DA, Barnsley L, Oostendorp RA, et al.
Prognostic factors of whiplash-associated disorders: a systematic review of prospective cohort studies. Pain
2003;104:303–22.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 175
ÃÙ»·Õè 3 áÊ´§·‹ÒºÃÔËÒâÂѺ¤Í (active range of motion)(3)
¡ÒèѴ¡Ãд١ (Manipulation) ์¹á¡Œä¢¢ŒÍµ‹Í¤Íʋǹ·Õà¤Å×͹äËÇä´Œ¹Í ¤ÅÒÂà¡Ã秡ŌÒÁ
è è Œ
à¹×Íàª×ÍÇ‹Ò¡ÒèѴàÃÕ§¡Ãд١ãËŒÍÂÙã¹á¹Ç»¡µÔÊÒÁÒöŴáç¡ÃзíÒµ‹Íʋǹ·ÕÁ¾ÂÒ¸ÔÊÀҾ䴌(3) ÁÕ§Ò¹
é è ‹ è Õ
ÇԨ·վºÇ‹Òä´Œ¼ÅÅ´ÍÒ¡ÒûǴ áÅÐà¾ÔÁ¾ÔÊ¢ŒÍä´Œ ᵋ¤³ÀÒ¾¢Í§§Ò¹ÇÔ¨ÂäÁ‹´¹¡(12) Í‹ҧäáçµÒÁ
Ñ è è Ñ Ø Ñ Õ Ñ
µŒÍ§ÃÐÇѧÀÒÇÐá·Ã¡«ŒÍ¹¨Ò¡¡Ãд١à¤Å×͹¡´·ÑºàÊŒ¹»ÃÐÊÒ·ËÃ×Íä¢ÊѹËÅѧ ¢ŒÍËŒÒÁ·ÕÊÒ¤Ñ ä´Œá¡‹
è èí
¡Ãд١ÊѹËÅѧËÑ¡ ¡Ãд١¾Ãع ¡Ãд١ËÃ×ÍËÁ͹Ãͧ¡Ãд١ÍÑ¡àʺ ¢ŒÍµ‹ÍäÁ‹Á¹¤§ ໚¹µŒ¹ Ñè
¡ÒäÅÒ¨ش»Ç´ (Released myofascial trigger points) ·íÒä´ŒËÅÒÂÇÔ¸·§¡ÒúÃÔËÒÃÂ×´ Õ Ñé
¡ÅŒÒÁà¹×Í ¡ÒÃ㪌à¢çÁ (trigger point injection) ¡ÒÃ㪌à¤Ã×ͧÁ×Í·Ò§¡ÒÂÀÒ¾ºíҺѴ ¡ÒùǴ áÁŒäÁ‹¾º
é è
ËÅÑ¡°Ò¹Ç‹Òä´Œ¼Åã¹ whiplash injury ᵋà¹×ͧ¨Ò¡¾º myofascial trigger points ໚¹ÊÒà˵ØÃÇÁ
(11)
è ‹
¢Í§ÍÒ¡ÒûǴ䴌º‹Í ÍÕ¡·Ñ駡ÒäÅÒ¨ش»Ç´·íÒä´ŒäÁ‹ÂÒ¡áÅÐÁÑ¡ä´Œ¼Å´Õ ¨Ö§¤ÇþԨÒóҷíÒ
(6)
¤Çº¤Ù¡º¡ÒÃÃÑ¡ÉÒÍ×¹æ(1) ·Ñ§¹Õ¡ÒÃ㪌à¢çÁ¤ÅÒ¨ش»Ç´ºÃÔàdzµŒ¹¤Í ÁÑ¡µŒÍ§ÍÒÈÑÂᾷ·àªÕÂǪÒ
‹ Ñ è é é Õè è
à¹×ͧ¨Ò¡ã¡ÅŒËÅÍ´àÅ×Í´ áÅÐä¢ÊѹËÅѧ
è
¡ÒûÃѺá¹Ç¤Ô´ áÅоĵԡÃÃÁ (Cognitive and behavioral therapy) ã¹¼Ù·Áá¹Ç⹌Á Œ Õè Õ
¾Ö§¾Ò ÃͤÍ¡ÒÃÃÑ¡ÉÒ¨Ò¡âç¾ÂÒºÒÅ (passive treatment) äÁ‹¡ÅŒÒ·Õ¨Ðà¤Å×͹äËÇ¤Í ËÃ×Í¡ÅѺä»
è è è
·íÒ¡Ô¨ÇѵõÒÁ»¡µÔ (fear and avoidance) ËÇѧ¼ÅãËŒÍÒ¡ÒÃËÒ¢Ҵ¨Ö§¨ÐàÃÔÁ㪌§Ò¹ (expectation to
è
recovery) ¤Ô´ã¹á§‹Åº (negative thinking) ÇÔµ¡¡Ñ§ÇÅ (anxiety) ÁÕá¹Ç⹌Á¨Ð¡ÅÒÂ໚¹»˜ËÒàÃ×ÍÃѧ é
䴌ʧ ¡ÒÃÃÑ¡ÉÒµŒÍ§·íҤǺ¤Ù仡Ѻ¡ÒûÃѺá¹Ç¤Ô´ áÅоĵԡÃÃÁ â´Â¤‹ÍÂæãËŒàÃÔÁ·íÒ¡Ô¨Çѵà ÍÍ¡
Ù ‹ è
¡íÒÅѧ¡Ò·ÕÅйŒÍ·ÕäÁ‹¡ÃеعãËŒà¡Ô´ÍÒ¡ÒûǴ ์¹ãËŒ¼»ÇÂÃÙ¨¡Êѧࡵ áÅШѴ¡ÒáѺ¤ÇÒÁ»Ç´´ŒÇÂ
è Œ ÙŒ † Œ Ñ
µ¹àͧ ¡ÒõԴµÒÁ¼Å์¹·Õ»ÃÔÁÒ³¡Ô¨¡ÃÃÁ·Õ·Òä´ŒÁÒ¡¢Ö¹ ËѹàˤÇÒÁʹ㨠à¾ÔÁ¤ÇÒÁÁѹã¨ãËŒ¼»ÇÂ
è è í é è è ÙŒ †
â´ÂäÁ‹à¹Œ¹µÔ´µÒÁÃдѺ¤ÇÒÁ»Ç´ (11)
àǪÈÒʵ÷¹Âؤ 2553
Ñ 181
9. Smith LE. Anal fissures. Neth J Med 1990;37(Supp1):S33-6.
10. Gibbons CP, Read NW. Anal hypertonia in fissures: cause or effect? Br J Surg 1986;73:443-5.
11. Tejirian T, Abbas MA. Sitz bath: where is the evidence? Scientific basis of a common practice. Dis Colon
Rectum 2005;48:2336-40.
12. Jiang JK, Chiu JH, Lin JK. Local thermal stimulation relaxes hypertonic anal sphincter: evidence of somatoanal
reflex. Dis Colon Rectum 1999;42:1152-59.
13. Loder PB, Kamm MA, Nicholls RJ, Phillips RK. ‘Reversible chemical sphincterotomy’ by local application of
glyceryl trinitrate. Br J Surg 1994;81:1386-9.
14. Lund JN, Scholefield JH. A randomised, prospective,double-blind, placebo-controlled trial of glyceryl trinitrate
ointment in treatment of anal fissure. Lancet 1997;349:11-4.
15. Maria G, Cassetta E, Gui D, Brisinda G, Bentivoglio AR,Albanese A. A comparison of botulinum toxin and
saline for the treatment of chronic anal fissure. N Engl J Med 1998;338:217-20.
16. Nelson R. A systematic review of medical therapy for anal fissure. Dis Colon Rectum 2004;47:422-31.
17. Garc?a-Aguilar J, Belmonte C, Wong DW, Goldberg SM, Madoff RD. Cutting seton versus two-stage seton
fistulotomy in the surgical management of high anal fistula. Br J Surg 1998;85:243-5.
18. Barillari P, Basso L, Larcinese A, Gozzo P, Indinnimeo M.Cyanoacrylate glue in the treatment of ano-rectal
fistulas.Int J Colorectal Dis 2006;21:791-4.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 185
Liver transplantation
à¹×ͧ¨Ò¡ HCC ¾ºä´ŒºÍÂ㹼ٻǷÕ໚¹µÑºÍÑ¡àʺàÃ×ÍÃѧáÅеѺá¢ç§ ¼Ù»Ç¨íҹǹÁÒ¡·ÕÁÒ
è ‹ Œ † è é Œ † è
¾ºá¾·Â ÍÂÙã¹ÃÐÂзÕäÁ‹ÊÒÁÒöÃÑ¡ÉÒ´ŒÇ¡Òü‹ÒµÑ´ä´Œ ÁÕ¼»ÇÂà¾Õ§ 20% - 30% ෋ҹѹ·ÕÊÒÁÒö
‹ è ÙŒ † é è
ÃѺ¡ÒÃÃÑ¡ÉÒ´ŒÇ¡Òü‹ÒµÑ´ä´Œ ¡ÒÃÃÑ¡ÉÒ HCC ´ŒÇ¡Òü‹ÒµÑ´ËÃ×Íà»ÅÕ¹µÑº Áբʹշҧ·ÄÉ®ÕËÅÒÂ è Œ
Í‹ҧ 䴌ᡋ ¡ÒõѴµÑºà´ÔÁ·Ô駷Ñé§ËÁ´·íÒãˌ䴌 margin ·Õè¡ÇŒÒ§¡Ç‹Ò ª‹ÇÂÅ´âÍ¡ÒÊ¡ÅѺÁÒãËÁ‹
(recurrence) ¢Í§âä ¡ÒõѺà¹×͵Ѻ·Õ໚¹âäÍÍ¡ ª‹ÇÂÅ´âÍ¡ÒÊ·Õ¨ÐÁÕÁÐàÃ秾Ѳ¹Ò¢Ö¹ãËÁ‹ã¹à¹×͵Ѻ
é è è é é
ʋǹÍ×¹ áÅСÒõѴµÑº·Õ໚¹µÑºá¢ç§ÍÍ¡·Ñ§ËÁ´áÅŒÇãÊ‹µº·Õ´à¢ŒÒä»à»š¹¡ÒÃÃÑ¡ÉÒ portal hypertension
è è é Ñ è Õ
¨Ò¡ cirrhosis ¢Í§¼Ù»Ç´ŒÇ Œ †
ã¹Í´Õµ¡ÒáÅѺ໚¹«éҢͧâäÊÙ§ÁÒ¡à¹×ͧ¨Ò¡¡ÒÃàÅ×Í¡¼Ù»Ç·ÕäÁ‹àËÁÒÐÊÁÁÒ·íÒ¡Òü‹ÒµÑ´
í è Œ † è
à»ÅÕ¹µÑº ã¹»‚ 1996 ÁÕÃÒ§ҹâ´Â Mazzaferro ¨Ò¡»ÃÐà·ÈÍÔµÒÅÕ ÃÒ§ҹ¼Ù»Ç·Õ䴌ú¡Òü‹ÒµÑ´
è 9
Œ † è Ñ
ÃÑ¡ÉÒÁÐàÃ秵Ѻ ´ŒÇ¡Òà ¼‹ÒµÑ´à»ÅÕ¹µÑº 96 ÃÒ â´Â¼Ù»ÇÂÁÕÁÐàÃ秵ѺÃÐÂÐàÃÔÁµŒ¹ ¤×Í ÁÕà¹×ͧ͡ 1
è Œ † è é
¡ŒÍ¹ ¢¹Ò´äÁ‹à¡Ô¹ 5 «Á. ËÃ×ÍÁÕà¹×ͧ͡äÁ‹à¡Ô¹ 3 ¡ŒÍ¹ ᵋÅСŒÍ¹ÁÕ¢¹Ò´äÁ‹à¡Ô¹ 3 «Á. à¹×ͧ͡·Ñ§
é é é
ËÁ´µŒÍ§äÁ‹ÁÕ vascular invasion áÅÐÂѧäÁ‹Á¡ÒáÃШÒ¢ͧà¹×ͧ͡Í͡仹͡µÑº ¨Ò¡ÃÒ§ҹ´Ñ§
Õ é
¡Å‹ÒǾºÇ‹Ò¼Ù»ÇÂÁÕ͵ÃÒ¡ÒÃÍÂÙÃÍ´·Õè 4 »‚ ÊÙ§¶Ö§ 75% ã¡ÅŒà¤Õ§¡Ñº¼Ù»Ç·Õ䴌ú¡Òü‹ÒµÑ´à»ÅÕ¹
Œ † Ñ ‹ Œ † è Ñ è
µÑº¨Ò¡¢ŒÍº‹§ªÕ͹·ÕäÁ‹Áà¹×ͧ͡ ࡳ±¡ÒÃàÅ×Í¡¼Ù»Ç´ѧ¡Å‹ÒÇ»˜¨¨Øº¹ÃÙ¨¡¡Ñ¹á¾Ã‹ËÅÒª×Í Milan
é ×è è Õ é Œ † Ñ ŒÑ è
criteria «Ö§ãªŒ¡¹Í‹ҧá¾ÃËÅÒ·ÑÇâÅ¡ÃÇÁ·Ñ§»ÃÐà·ÈÊËÃÑ°ÍàÁÃÔ¡Ò
è Ñ è é
¼ÙŒ»†ÇÂÁÐàÃ秵Ѻ·ÕèÍÂÙ‹ã¹ Milan criteria ÁÕÊѴʋǹ¹ŒÍÂàÁ×èÍà·Õº¡Ñº¼ÙŒ»†ÇÂÁÐàÃ秵Ѻ·Ñé§ËÁ´
¼ÙàªÕÂǪÒËÅÒ·‹Ò¹¤Ô´Ç‹Òࡳ±¹¨Ò¡Ñ´à¡Ô¹ä» ·íÒãËŒ¼»Ç¨íҹǹÁÒ¡·ÕÍÂٹ͡ࡳ± àÊÕÂâÍ¡ÒÊ·Õè
Œ è Õé í ÙŒ † è ‹
¨Ð䴌ú¼Å´Õ¨Ò¡¡Òü‹ÒµÑ´ ¤ÇÒÁ¾ÂÒÂÒÁ¼‹ÒµÑ´ã¹¼Ù»Ç·ÕÁÁÐàÃç§ÍÂٹ͡ Milan criteria ¾ºÇ‹Ò¼Ù»ÇÂ
Ñ Œ † è Õ ‹ Œ †
ºÒ§ÃÒ¡çÂѧ䴌¼Å´Õ ¨Ò¡¡ÒÃÈÖ¡ÉÒÇÔà¤ÃÒÐË¢ŒÍÁÙŢͧ¼ÙŒ»†Ç·ÕèÍÂÙ‹¹Í¡à¡³±·Õèä´ŒÃѺ¡Òü‹ÒµÑ´
à»ÅÕ¹µÑºáÅŒÇä´Œ¼Å´Õ ·íÒãËŒÁ¡ÒþѲ¹Òࡳ±ãËÁ‹æ¢Ö¹ÁÒઋ¹ UCS. criteria10 ໚¹µŒ¹ Yao10 ÃÒ§ҹ
è Õ é
Ç‹Ò¶ŒÒ¼Ù»ÇÂÍÂÙ㹡ÅØÁ·ÕÁà¹×ͧ͡à¾Õ§¡ŒÍ¹à´ÕÂÇ¢¹Ò´äÁ‹à¡Ô¹ 6.5 «Á. ËÃ×ÍÁÕà¹×ͧ͡äÁ‹à¡Ô¹ 3 ¡ŒÍ¹
Œ † ‹ ‹ è Õ é é
ᵋÅСŒÍ¹ÁÕ¢¹Ò´äÁ‹à¡Ô¹ 4.5 «Á. áÅТ¹Ò´àÊŒ¹¼‹ÒÈٹ¡ÅÒ§ÃÇÁ¢Í§à¹×ͧ͡äÁ‹à¡Ô¹ 8 «Á. (within é
UCS. criteria) ¼Ù»ÇÂÊÒÁÒöÁÕ͵ÃÒ¡ÒÃÍÂÙÃÍ´·Õè 5 »‚ ÊÙ§¶Ö§ 75.2%
Œ † Ñ ‹
DC bead
à¹×ͧ¨Ò¡¼Ù»Ç HCC ʋǹÁÒ¡äÁ‹ÊÒÁÒöÃÑ¡ÉÒ´ŒÇ¡Òü‹ÒµÑ´ä´Œà¹×ͧ¨Ò¡ÀÒÇеѺá¢ç§ ·íÒãËŒ
è Œ † è
àËÅ×Í liver reserve äÁ‹à¾Õ§¾Í ¡ŒÍ¹ HCC ¢¹Ò´ãË‹¡äÁ‹àËÁÒÐ㹡Ò÷íÒ R.A ¡ÒÃãËŒ systemic
ç
chemotherapy ¡çä´Œ¡Òõͺʹͧ·ÕäÁ‹´Õ áÅÐÁռŢŒÒ§à¤Õ§ÁÒ¡ ¨Ö§ä´ŒÁ¡ÒþѲ¹Ò¡Ò÷íÒ transarterial
è Õ
chemoembolization (TACE) ¡Ò÷íÒ TACE ÍÒÈÑÂËÅÑ¡¡Ò÷ÕÇÒà¹×͵Ѻ»¡µÔ¨Ð䴌úàÅ×Í´ÁÒàÅÕ§
è‹ é Ñ é
·Ñ§¨Ò¡ hepatic artery áÅÐ portal vein ã¹¢³Ð·Õè HCC ¨Ðä´ŒàÅ×Í´ÁÒàÅÕ§ʋǹÁÒ¡¨Ò¡ hepatic artery
é é
¡ÒÃãËŒ chemotherapeutic agent ·Ò§ hepatic artery áÅŒÇÍØ´ hepatic artery ·Õä»àÅÕ§¡ŒÍ¹à¹×ͧ͡
è é é
¨Ð·íÒãËŒ à¹×ͧ͡¢Ò´ blood supply áÅÐ chemotherapeutic agent ÊÑÁ¼ÑʡѺà¹×ͧ͡´ŒÇ dose ·Õʧ
é é èÙ
188 Hepatocellular Carcinoma : Management in the New Era
10. Yao .Y, .errell L, Bass NM, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor
size limits does not adversely impact survival. Hepatology 2001;33:1394-403.
11. Lewis AL, Gonzalez MV, Leppard SW, et al. Doxorubicin eluting beads – 1: Effects of drug loading on bead
characteristics and drug distribution. J Master Sci 2007;18: 1691-9.
12. Lammar J, Malagari K, Vogl T, et al. Prospective randomized study of Doxorubicin-Eluting-Bead embolization
in the treatment of hepatocellular carcinoma: Result of the PRECISION V Study. Cardiovasc Intervent Radiol
2010;33:41-52.
13. Li YY, Sha WH, Zhou YJ, Nie YQ. Short and long term efficacy of high intensity focused ultrasound therapy
for advanced hepatocellular carcinoma. J Gastroentero Hepato 2007;22:2148-2154.
14. Wu ., Wang ZB, Chen WZ, et al. Advanced hepatocellular carcinoma: treatment with high-intensity focused
ultrasound ablation combined with transcatheter arterial embolization. Radiology 2005;235:659-67.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 191
transplantation) äÁ‹ÇÒ¨Ð໚¹¨Ò¡¼ÙãË‹Êà´ç¡ (adult to child) ËÃ×ͼÙãˋʼãË‹ (adult to adult) «Ö§
‹ Œ Ù‹ Œ Ù‹ ÙŒ è
á¹Ç·Ò§¡ÒôíÒà¹Ô¹¡Òõ‹Ò§ æ ¢ŒÒ§µŒ¹¹Õä´ŒàÃÔÁ¹íÒÁÒ»ÃÐÂØ¡µãªŒã¹âç¾ÂÒºÒÅÈÔÃÃÒªáÅŒÇ ¤³Ð¼Ù´áÅ
é è Ô Œ Ù
ÃÑ¡ÉҼٻǻÅÙ¡¶‹ÒµѺÁÕ¤ÇÒÁÁاÁѹ·Õ¨Ð¾Ñ²¹Ò¡Ãкǹ¡ÒôÙáÅÃÑ¡ÉÒ·Ø¡ æ ´ŒÒ¹à¾×ÍÃÑ¡ÉÒªÕǵ¼Ù»ÇÂ
Œ † ‹ è è è Ô Œ †
ãËŒÁ¤³ÀÒ¾áÅлÃÔÁÒ³ÁÒ¡¢Ö¹µÅÍ´ä»
Õ Ø é
àǪÈÒʵ÷¹Âؤ 2553
Ñ 195
¡ÒõÃǨàÍç¡«àûʹáÅФÅ×¹ËÑÇ㨠¼Åã¹¼ÙºÃÔ¨Ò¤ÃÒ¹ÕäÁ‹¾º¤ÇÒÁ¼Ô´»¡µÔ
è Œ é
2. ¡ÒõÃǨ·Ò§¨ÔµàǪâ´Â¨Ôµá¾·Â ¾ºÇ‹Ò¼ÙºÃÔ¨Ò¤äÁ‹ÁÊÀÒÇзҧ¨Ôµ·Õ¼´»¡µÔ áÅÐÊÁѤÃ
Œ Õ è Ô
㨷ըкÃÔ¨Ò¤ãˌᡋº´Ò
è Ô
3. ¡ÒõÃǨ·Ò§ÃѧÊÕÇ·ÂÒà¾×Í»ÃÐàÁÔ¹¡ÒÂÇÔÀÒ¤¢Í§µÑº
Ô è
Computer tomography of liver ËÇÁ¡Ñº computer tomography angiography and
venopraphy with three diameter reconstruction à¾×Í´Ù hepatic artery, portal vein, hepatic vein
è
anatomy and variation áÅÐ computer tomography volumetry à¾×Í»ÃÐàÁÔ¹»ÃÔÁҵâͧ right lobe,
è
left lobe áÅÐ caudate lobe ã¹¼ÙºÃÔ¨Ò¤ ¾ºÁÕ accessory left hepatic artery ¨Ò¡ left gastric artery,
Œ
normal portal vein anatomy, normal hepatic vein anatomy with inferior right hepatic vein 4 mm
in size, CT volumetry ¾ºÇ‹Ò»ÃÔÁҵâͧ right lobe ෋ҡѺ 753.1 ml, left lobe ෋ҡѺ 418.3 ml,
caudate lobe ෋ҡѺ 20.2 ml
¨Ò¡¡ÒõÃǨ¤Œ¹à¾ÔÁàµÔÁ¢Í§¼ÙºÃÔ¨Ò¤ÃÒ¹Õé äÁ‹¾ºÇ‹ÒÁÕ¢ÍËŒÒÁ (contraindication) 㹡ÒÃ
è Œ Œ
ºÃÔ¨Ò¤ÍÇÑÂÇеѺ áÅШҡ¡ÒûÃÐàÁÔ¹»ÃÔÁҵâͧµÑº´ŒÇ ¹íÒÁÒ¤íҹdz future liver remnant (.LR)
«Ö§à·‹Ò¡Ñº future liver remnant volume x 100/total liver volume ෋ҡѺ (left + caudate) x 100/
è
(right + left + caudate) ¤‹Ò .LR ·ÕàËÁÒÐÊÁ ¤ÇèÐäÁ‹¹ÍÂ¡Ç‹Ò 35% à¾×ͤÇÒÁ»ÅÍ´ÀÑÂÊíÒËÃѺ¼ÙºÃÔ
è Œ è Œ
¨Ò¤ ¶ŒÒµÑº·ÕàËÅ×ͧ͢¼ÙºÃÔ¨Ò¤àËÅ×͹ŒÍÂà¡Ô¹ä»¡ç¨ÐÁÕ¤ÇÒÁàÊÕ§㹡ÒÃà¡Ô´µÑºÇÒÂÀÒÂËÅѧ¡Òü‹ÒµÑ´ä´Œ
è Œ è
¹Í¡¨Ò¡¹Ñé¹ÂѧµŒÍ§»ÃÐàÁԹNjҵѺʋǹ·Õèä´ŒÃѺºÃÔ¨Ò¤ÁÒà¾Õ§¾Íµ‹Í¤ÇÒÁµŒÍ§¡Òâͧ
¼ÙúºÃÔ¨Ò¤ËÃ×Í äÁ‹ â´Â㪌¡ÒäíҹdzËÒ graft-recipient weight ratio (GRWR) «Ö§à·‹Ò¡Ñº graft
ŒÑ è
volume(L) / recipient body weight (kg) ¤‹Ò GRWR ·ÕàËÁÒÐÊÁäÁ‹¤ÇùŒÍÂ¡Ç‹Ò 0.8% à¾ÃÒТ¹Ò´
è
¢Í§ graft ·ÕàÅç¡à¡Ô¹ä»¨ÐÊ‹§¼Åµ‹Í¡Ò÷íÒ§Ò¹¢Í§ liver graft à¡Ô´ÀÒÇзÕàÃÕÂ¡Ç‹Ò small-for-size syndrome
è è
䴌
ã¹¼ÙºÃÔ¨Ò¤áÅмٻǹÕé ¤íҹdz䴌¤Ò .LR ෋ҡѺ 36.8% GRWR ෋ҡѺ 1.29 «Ö§
Œ Œ † ‹ è
àËÁÒÐÊÁµ‹Í¡Òü‹ÒµÑ´»ÅÙ¡¶‹ÒµѺ
¡Òü‹ÒµÑ´¼ÙŒºÃÔ¨Ò¤ÍÇÑÂÇеѺ (Donor operation) ໚¹¡Òü‹ÒµÑ´ right hepatectomy
·Õ¨Ò໚¹µŒÍ§ÃÐÁÑ´ÃÐÇѧ structure ÊíÒ¤ÑËÅÒÂÍ‹ҧ ¡ÒÃãËŒÂÒÃЧѺ¤ÇÒÁÃÙÊ¡´ŒÇ¡ÒÃãËŒ epidural
èí ŒÖ
anesthesia ËÇÁ¡Ñº¡ÒôÁÂÒÊź ¡ÒÃཇÒÃÐÇѧÊÑÒ³ªÕ¾·íÒâ´Â¡ÒÃãÊ‹ÊÒ arterial line áÅÐ central
venous pressure (CVP) line áÅÐ㪌෤¹Ô¤ low CVP à¾×ÍÅ´¡ÒÃÊÙàÊÕÂàÅ×Í´ÃÐËÇ‹Ò§¡ÒõѴàÅÒÐ
è
à¹×ÍàÂ×͵Ѻ ¡ÒÃ㪌 intraoperative ultrasonography ÁÕ¤ÇÒÁÊíÒ¤Ñ㹡ÒûÃÐàÁÔ¹à¹×͵ѺáÅÐá¹Ç·Ò§
é è é
à´Ô¹¢Í§àÊŒ¹àÅ×Í´µ‹Ò§ æ 㹵Ѻ ¡Ò÷íÒ intraoperative cholangiography ¼‹Ò¹·Ò§ cystic duct à¾×Í è
»ÃÐàÁÔ¹ anatomy ¢Í§·‹Í¹éÒ´Õ«ÒÂáÅТÇÒ㹵Ѻ ໚¹¡ÒÃÇҧἹµíÒá˹‹§·Õ¨ÐµÑ´·‹Í¹íÒ´ãËŒ¾Í´Õ äÁ‹
í Œ è Œ Õ
໚¹ÍѹµÃÒµ‹Í·‹Í common hepatic duct áÅÐ left intrahepatic duct ¡ÒÃàÅÒÐẋ§à¹×͵Ѻ㪌à¤Ã×ͧ é è
Cavitron Ultrasonic Surgical Aspirator (CUSA) 㹡Òü‹ÒµÑ´¤Ãѧ¹Õä´ŒàÅÒÐàÊŒ¹àÅ×Í´ middle hepatic
é é
vein 仡Ѻ liver graft ´ŒÇ àÁ×ÍÊÒÁÒöµÑ´µÑº¡ÅÕº¢ÇÒÍÍ¡ÁÒä´ŒáÅŒÇ ¨Ð perfuse µÑº´ŒÇ preservative
è
solution (University of Wisconsin solution) ·ÕÁ¤ÇÒÁàÂç¹ã¹¹éÒá¢ç§ ªÑ§ÇÑ´¹íÒ˹ѡ¢Í§ graft ä´Œ
è Õ í è Œ
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 197
30
Robotic Surgery for General Surgeons :
.utute or .antasy
Vitoon Chinswangwatanakul, MD., PhD.
Thawatchai Akaraviputh, MD.
Attaporn Trakarnsanga, MD.
Asada Metasate, MD., PhD.
Thanyadej Nimmanwudipong, MD.
Naraong Lertakyamanee, MD.
Department of Surgery, .aculty of Medicine Siriraj Hospital, Mahidol University
Robotic surgery is one of the innovations by the end of the last century. The word
‘robot’, described for the first time by Karel Capek in 1921, was named after the Czeck word
‘robota’ which means ‘forced labor’. The rapid advances of mechanical engineering in combination
with computer science has led to the fundamental establishment in robotic surgery.
History of robotic surgical machines
In 1993, the first robotic-assisted machine was launched named AESOP® Endoscope
Positioner which provided the stability of endoscope positioning.1
The next machine called HERMES® O.R. Control Center was a computer-driven system
which allowed surgeons to control extra devices by voice. The HERMES voice-activated device
control system could control 28 different devices from tables, cameras, to lighting systems and
electrosurgical units. It offers direct control and eliminates the various interfaces between surgeon
and other personnel in order to adjust the surgical equipments.
In 1998, ZEUS® Surgical System is made up of a surgeon console and three
table-mounted robotic arms, which provide visualization during performing endoscopic surgical
tasks. (.igure 1) The ZEUS system assists surgeons to increase dexterity of the surgical
procedures. Surgeon could control the right and left arms of ZEUS, with a real-time articulation
of the surgical instruments, meanwhile the third camera arm incorporated with the AESOP®
provides magnified, steady visualization of the operative field. In 1999, ZEUS made history in
225.
198 Robotic Surgery for General Surgeons : .uture or .antasy
the world's first robotic-assisted beating-heart bypass surgery, by Douglas Boyd. This milestone
indicated a new era of minimally invasive surgery.2
.igure 1. The ZEUS® Surgical System.3
In 2000, da Vinci Surgical System® was launched by Intuitive Surgical, after merging
with Computer Motion. It consists of an ergonomically designed surgeon’s console, a patient-
side cart with four interactive robotic arms, the high-performance 3-D InSite® Vision System and
EndoWrist® Instruments. (.igure 2) The surgeon’s hand movements are scaled, filtered and
effectively translated into precise movements of the EndoWrist® Instruments. The da Vinci
Surgical System® is now the only commercially available technology that can provide surgeons
with the spontaneous control, wider range of motion, fine tissue manipulation capability and 3-D
visualization, through tiny typical incisions of minimally invasive surgery.4
In 2001, the SOCRATESTM
.igure 2. The da Vinci Surgical System®.5
226.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 199
Telecollaboration system synergized a number of systems including Zeus, AESOP,
and HERMES. It allows remotely located surgeons to receive a live endoscopic video image of
the operative field. The audio and video links the operating room with the remote station. The
SOCRATESTM system controls the operative site's AESOP endoscope camera view of the
operative site while communicating with HERMES OR control to provide securely remote control
of networked surgical devices. The safety features allow surgeon to halt all movements initiated
by the collaborating surgeon via voice-activated commands.6
Table 1. Computer Motion systems that all are now owned by Intuitive Surgical.6
Equipment Costs Company Equipment Descriptions
da Vinci Surgical $1 million Intuitive Robot-assistant, with arms to
System Surgical connect surgical instruments
Zeus Robot Surgical $975,000 Computer Robot-assistant, with arms
System Motion* to connect surgical instruments
Aesop 3000 $80,000 Computer Voice-controlled endoscope-
Motion* positioning robot
Hermes Control Center n/a Computer Centralized system used to
Motion* network an intelligent OR
Socrates Robotic n/a Computer Allows shared control of
Telecollaboration System Motion* Aesop 3000 from different locations
*.ormer Computer Motion systems that are now owned by Intuitive Surgical.
Sources: from Journal of Healthcare Management 46:4 July/August 2003.
What sort of operations we can do...
The U.S. .ood and Drug Administration (US .DA) has cleared the da Vinci® Surgical
System for use in urological surgical procedures, general laparoscopic surgical procedures,
gynecologic laparoscopic surgical procedures, transoral otolaryngology surgical procedures
restricted to benign and malignant tumors classified as T1 and T2, general thoracoscopic surgical
procedures, and thoracoscopically assisted cardiotomy procedures.7-8 The system can also be
employed with adjunctive mediastinotomy to perform coronary anastomosis during cardiac
revascularization. The da Vinci® System has been successfully used in the following procedures,
among others:
227.
200 Robotic Surgery for General Surgeons : .uture or .antasy
Table 2 The procedures have been successfully performed by da Vinci® System.7
Surgical Specialties Procedures
Urology Radical prostatectomy, pyeloplasty,
cystectomy, nephrectomy, ureteral reimplantation
Gynecology Hysterectomy, myomectomy and
sacrocolpopexy
Cardiothoracic Surgery Internal mammary artery mobilization and
cardiac tissue ablation
Mitral valve repair, endoscopic atrial septal
defect closure
Mammary to left anterior descending coronary
artery anastomosis for cardiac revascularization
with adjunctive mediastinotomy
Gastrointestinal Surgery Cholecystectomy, Nissen fundoplication, Heller
myotomy, gastric bypass, donor nephrectomy,
adrenalectomy, splenectomy and bowel resection
Otolaryngology Oropharyngeal, laryngeal and hypopharyngeal
resections; floor of mouth and oral cavity
resections
In September 2000, .DA Approved the da Vinci® robotic surgery for the following operative
procedures :-
! Cholecystectomy
! Antireflux procedures
! Heller’s cardiomyotomy
! Distal pancreatectomy
! Gastrojejunostomy
! Esophagectomy
! Gastric bypass
! Gastric banding
! Pyloroplasty
! Colectomy
! Adrenalectomy
! Splenectomy
228.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 201
Robotic surgery in gastrointestinal surgery : Siriraj experience
We started to perform the first case of robotic-assisted laparoscopic esophagomyotomy
on November, 30th 2007. Since then, 11 different types of laparoscopic gastrointestinal surgery
were carried out with the successful rate over 84%. (Table 2) The principle of case selection
has been based on the most benefits surgeons could gain from robotic-assisted devices. The
need for tissue dissection in depth, differentiation of delicated tissue (such as sympathetic
nerve plexus) or use of intracorporeal suturing and anastomosis were the reason to choose
robotic-assisted laparoscopic approach. The most complex surgical procedure we performed
was pancreaticoduodenectomy. Even though the successful rate on such a complex surgery
was only 50%, all of the last 3 cases was uneventfully successful. The more procedures we
have performed, the more experience we have received. To overcome the learning curve, we
have to establish a good surgical team work, because the complex procedures certainly extend
the operative time which cause the stress and fatigue to a single surgeon. Thus, we switched
the surgical operator every 1-2 hours among 3 surgeons. This work as team approach led to
nonstop operation with the most effective result. We demonstrated the shorter operative time
by this technique.
Table 3 The variety of surgical procedures performed in the Division of General Surgery,
Department of Surgery, .aculty of medicine Siriraj Hospital.
Procedures Attempt .ailure
Esophagomyotomy 18 0
Pancreaticoduodenectomy 6 3
Low Anterior Resection 6 1
Nissen .undoplication 5 1
Partial Gastrectomy 2 0
Hepatectomy 2 1
Cholecystectomy 2 0
Hepaticojejunostomy 1 0
Abdominoperineal Resection 1 0
Sigmoidectomy and Rectopexy 1 0
Partial Duodenectomy 1 1
Total 45 7
229.
202 Robotic Surgery for General Surgeons : .uture or .antasy
Conclusion
Robotic surgery is now accepted as an alternative for selected surgical procedures.
This is just a dawn of the new era for future surgery. We believe this innovation from the end of
the last century would certainly establish a milestone of robotic surgery for the benefit of mankind.
References
1. Sackier JM, Wang Y. Robotically assisted laparoscopic surgery: from concept to development. Surg Endosc
1994;8:63-6.
2. Ballantyne GH. Robotic surgery, telerobotic surgery, telepresence, and telementoring: Review of early clinical
results. Surg Endosc 2002;6:1389-402.
3. http://library.thinkquest.org/03oct/00760/Zeus%20System.htm (Accessed on 17 July 2010)
4. http://www.intuitivesurgical.com/products/davinci_surgicalsystem/index.aspx (Accessed on 17 July 2010)
5. http://www.intuitivesurgical.com/www/site1/products/robotic/4th-Arm_259X319.jpg (Accessed on 17 July 2010)
6. http://www.frost.com/prod/servlet/market-insight-top.pag?docid=4453859 (Accessed on 17 July 2010)
7. Talamini MA, Chapman S, Horgan S, Melvin WS. A prospective analysis of 211 robotic-assisted surgical
procedures. Surg Endosc 2003;17:1521–4.
8. Watanabe G. Are You Ready to Take Off as a Robo-surgeon? Surg Today 2010;40:491–3.
212 Journey to Excellent Burn Unit
ÀÒ¾«ŒÒ¡‹Í¹»ÃѺ»Ãا ÀÒ¾¢ÇÒ Burn Unit ÀÒÂËÅѧ»ÃѺ»Ãا
ˌͧ»ÃЪØÁ»ÃѺ»ÃاãËÁ‹ ÊíÒËÃѺ¡ÒÃàÃÕ¹¡ÒÃÊ͹ ´Ù§Ò¹ à¼Âá¾Ã‹¤ÇÒÁÃÙáÅлÃЪØÁ·Õ·¹ÊÁÑÂ
Œ è Ñ
¹íÒ¤ÇÒÁÃÙŒáÅÐÇÔ·ÂÒ¡Ò÷Õè·Ñ¹ÊÁÑÂÁÒ»ÃѺ»Ãا¡ÒÃàÃÕ¹¡ÒÃÊ͹ Burn Injury ·Ñé§ã¹Ëͼٌ»†ÇÂ
Siriraj Burn Unit áÅÐ ã¹ËŒÍ§¼‹ÒµÑ´µÖ¡ÍغѵÔà˵Ø
Prince Michael of Kent, United Kingdom àÊ´ç¨àÂÕèÂÁªÁ Siriraj Burn Unit
àǪÈÒʵ÷¹Âؤ 2553
Ñ 215
Hydrosurgery
¡ÒùíÒà·¤¹Ô¤áÅÐà¤Ã×ͧÁ×ͼ‹ÒµÑ´áç´Ñ¹¹éÒÊÙ§ÁÒ㪌໚¹áË‹§áá㹻ÃÐà·Èä·Â ¹Ñ¹¤×Í
è í è
Hydrosurgery (Smith & Nephew Ltd.) «Ö§à¤Â໚¹à·¤¹Ô¤¡Òü‹ÒµÑ´·Õ¹ÂÁ㪌㹻ÃÐà·È·Õ¾²¹Ò â´Â
è è Ô è Ñ
àËÁÒСѺºÒ´á¼Åä¿äËÁŒ·ÁÕ eschar ¹ØÁæ áÅÐàÃÔÁËÅØ´ÅÍ¡ÍÍ¡ ¡ÒùíÒà·¤¹Ô¤¹ÕÁÒ㪌ÊÒÁÒöŴ
Õè ‹ è é
¡ÒÃÊÙàÊÕÂà¹×ÍàÂ×Í·Õ´Õ ·íÒãˌŴ¡ÒÃàÊÕÂàÅ×Í´ Å´¡ÒõѴºÒ´á¼ÅÅÖ¡à¡Ô¹ä» â´Â¼Ù»ÇÂÃÒÂáá¢Í§
é è è Œ †
»ÃÐà·Èä·Â¹Ñ¹ä´ŒÃº¡Òü‹ÒµÑ´¢³Ð admit ÍÂÙ‹ º¹ËͼٻÇ Siriraj Burn Unit ã¹à´×͹¸Ñ¹ÇÒ¤Á
é Ñ Œ †
»‚ 2547 »˜¨¨Øº¹à·¤¹Ô¤¹Õä´Œ¹ÒÁÒ㪌Í‹ҧá¾Ã‹ËÅÒÂã¹»ÃÐà·Èä·Â
Ñ é í
Hydrosurgery ¼‹ÒµÑ´ä¿äËÁŒÃعáç·ÕèÁÕ¢ŒÍº‹§ªÕé·ÕèàËÁÒÐÊÁ ÊÒÁÒöŴ¡ÒõѴà¹×éÍ´Õà¡Ô¹¨íÒ
໚¹ Å´¡ÒûÅÙ¡¶‹Ò¼ÔÇ˹ѧáÅÐà¾ÔèÁºÒ´á¼ÅãËÁ‹á¡‹¼ÙŒ»†Ç áÅÐ ºÒ´á¼ÅËÒÂàÃçÇ¢Öé¹
Tissue engineering artificial dermal template
¼Ù»ÇÂä¿äËÁŒÃ¹áç·ÕÁ¼Ç˹ѧäÁ‹¾ÍÁÒ·íÒ skin graft »´á¼Å ËÃ×ͺҴá¼Åä¿äËÁŒÃ¹áç
Œ † Ø è Õ Ô Ø
·ÕËÒÂáÅŒÇáÅÐÁÕÀÒÇÐË´Ãѧ¨Ò¡ scar contracture µŒÍ§ä´ŒÃº¡Òü‹ÒµÑ´ reconstruction ᵋäÁ‹ÁÕ skin
è é Ñ
graft ·Õ´¾Í¨ÐÁÒ»´á¼Å ÁÕ¤ÇÒÁ¨íÒ໚¹µŒÍ§ãªŒ tissue engineering template ÁÒÊÌҧªÑ¹ dermis
è Õ é
¢Ö¹ÁÒãËÁ‹ Siriraj Burn Unit Âѧ໚¹ unit ·ÕÁ»ÃÐʺ¡Òó㹡ÒùíÒ artificial dermis ÁÒ㪌ÁÒ¡·ÕÊ´
é Õ èØ
¶Ù¡µŒÍ§µÒÁ¢ŒÍº‹§ªÕ¢Í§¡ÒÃ㪌áÅмٻÇÂà¡×ͺ·Ñ§ËÁ´ä´Œ¼ÅÅѾ¸¡ÒÃÃÑ¡ÉÒ·Õ´àÂÕÂÁ ·íÒãËŒºÒ´á¼ÅËÒÂ
é Œ † é è Õ è
ä´Œ Å´¡Ò÷ء¢·ÃÁÒ¹¨Ò¡ºÒ´á¼ÅäÁ‹ËÒ ¤ÇÒÁà¨çº»Ç´¢Í§ºÒ´á¼Å áÅÐÅ´¡ÒÃà¡Ô´á¼ÅË´Ãѧ䴌 é
໚¹Í‹ҧ´Õ
Tissue engineering artificial dermis ¹íÒÁÒ¼‹ÒµÑ´»´Å§º¹ºÒ´á¼Åä¿äËÁŒà¡Ô¹ 80%
¢Í§¾×é¹·Õè¼ÔÇ àËÅ×Í skin graft ·Õè´Õ¹ŒÍ ÊÒÁÒöᡌÀÒÇÐË´ÃÑ駴ÕàÂÕèÂÁ
¼ÙŒ»†ÇÂà´ç¡ÃÒ¹Õé¨Ò¡à´Ô¹äÁ‹ä´Œ ¡ÅѺä»à»š¹¹Ñ¡¡ÕÌҿصºÍŢͧâçàÃÕ¹䴌
243.
216 Journey to Excellent Burn Unit
¼‹ÒµÑ´á¡Œä¢ÀÒÇÐË´ÃÑé§ ¢Í§ºÒ´á¼Åä¿äËÁŒÅÖ¡Ãعáç áÅÐᡌ䢴ŒÇÂ
tissue engineering artificial dermis
¡ÒúÃÔ¡ÒôبҵÔÁµÃ Ô
ãËŒ¡ÒúÃÔ¡ÒôبҵÔÁµÃ ´ŒÇ·ÕÁá¾·ÂáÅоÂÒºÒÅ·ÕÁ¤ÇÒÁàªÕÂǪÒã¹´ŒÒ¹¡ÒôÙáÅ
Ô è Õ è
ÃÑ¡ÉÒ¼Ù»ÇÂä¿äËÁŒ¹ÒÌ͹Åǡ໚¹Í‹ҧ´Õ ãËŒ¼»ÇÂáÅÐÒµÔä´ŒáÊ´§¢ŒÍàʹÍá¹Ð ¢ŒÍ¤Ô´àËç¹ä´ŒµÅÍ´
Œ † éí ÙŒ †
à¾×è͹íÒä»»ÃѺ»Ãا㹴ŒÒ¹¡ÒúÃÔ¡ÒÃãËŒ´ÕÂÔ觢Öé¹ä» ÀÒÂËÅѧ¨íÒ˹‹Ò¼ٌ»†ÇÂÍÍ¡¨Ò¡âç¾ÂÒºÒÅÁÕ
.amily planning ãˌᡋ¼»ÇÂáÅÐÒµÔ áÅйѴ¼Ù»ÇÂÁÒÃѺ¡ÒÃÃÑ¡ÉÒÍ‹ҧµ‹Íà¹×ͧ ¤ÃºÇ§¨Ã ´ÙáÅ´ŒÒ¹
ÙŒ † Œ † è
¡ÒÃà¡Ô´ºÒ´á¼ÅË´Ãѧ ´ŒÒ¹¨Ôµã¨ áÅÐ àǪÈÒʵÿ¹¿Ù ÁÕ¡ÒõԴµ‹Í»ÃÐÊÒ¹§Ò¹¡ÑºË¹‹Ç§ҹµ‹Ò§æ
é „œ
·Õà¡ÕÂÇ¢ŒÍ§ ໚¹¡ÒÃÃÑ¡ÉÒ multidisciplinary approach Ẻ¤ÃºÇ§¨Ã
è è
ºÃÔ¡ÒôŒÇÂ㨠´Ø¨ÒµÔÁÔµÃ
2. ¡ÒÃÇÔ¨ÑÂáÅÐà¼Âá¾Ã‹¤ÇÒÁÃÙŒ
·ÕÁá¾·ÂáÅоÂÒºÒÅã¹ Siriraj Burn Unit µÃÐ˹ѡ¶Ö§¤ÇÒÁÊíҤѢŒÍ¹ÕàÊÁÍ ¡Ò÷íÒÇÔ¨Â
é Ñ
áÅÐà¼Âá¾Ã‹Í§¤¤ÇÒÁÃ٨зíÒãˌ˹‹Ç§ҹ¾Ñ²¹ÒáÅÐÊÌҧª×ÍàÊÕ§ãËŒ¡ºÊ¶ÒºÑ¹ ã¹Ãͺ 5 »‚·¼Ò¹ÁÒ
Œ è Ñ Õè ‹
ÁռŧҹµÕ¾Á¾â´Â·ÕÁá¾·ÂáÅоÂÒºÒŨҡ Siriraj Burn Unit ·Ñ§ã¹»ÃÐà·ÈáÅе‹Ò§»ÃÐà·ÈÍ‹ҧ
Ô é
µèÒà¹×ͧ ÃÇÁ·Ñ§ºØ¤ÅÒ¡Ãã¹Ë¹‹Ç§ҹ䴌໚¹ÇÔ·ÂÒ¡Ãà¼Âá¾Ã‹¤ÇÒÁÃÙ·§ã¹áÅе‹Ò§»ÃÐà·ÈÃÇÁ¡Ç‹Ò
í è é Œ Ñé
200 ¤ÃÑ§é ¤Ãѧ˹֧à¤Âä´Œ¹ÒàʹÍ໚¹áººÍ‹ҧã¹â¤Ã§¡Òà R2R ¢Í§¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª
é è í ÔÔ
¾ÂÒºÒÅ ·Ò§Ë¹‹Ç§ҹ䴌úÃÒ§ÇÑÅÁÒ¡ÁÒ·ѧ¨Ò¡¡ÒÃà¼Âá¾Ã‹»ÃСǴ¼Å§Ò¹ÇÔ¨ÂÀÒ¹͡¤³Ð
Ñ é Ñ
áÅÐÀÒÂ㹤³Ðä´ŒÃѺÃÒ§ÇÑŨҡ¹Çѵ¡ÃÃÁãËÁ‹æËÅÒÂÃÒ§ÇÑÅÃÇÁ·Ñé§ä´ŒÃѺÃÒ§ÇÑÅ˹‹Ç§ҹ´Õà´‹¹
µÑÇÍ‹ҧ»ÃÐàÀ· ´ÒǷͧµÔ´µ‹Í¡Ñ¹ 3 »‚«Í¹ (2551-2553) ã¹»˜¨¨Øº¹ÁÕ¹¡ÈÖ¡ÉÒ»ÃÔÒâ·áÅÐàÍ¡
Œ Ñ Ñ
¨Ò¡Ê¶ÒºÑ¹Í×¹ÁÒËÇÁ»¯Ôºµ§Ò¹·Õè Siriraj Burn Unit ໚¹ÃÐÂÐæ ·íÒãËŒÁáÅ¡à»ÅÕ¹¤ÇÒÁÃÙã¹´ŒÒ¹¡ÒÃ
è Ñ Ô Õ è Œ
ÇÔ¨Âã¹Ç§¡ÇŒÒ§¢Ö¹ ÁÕ¡ÒáÃШÒÂͧ¤¤ÇÒÁÃÙáÅ¡à»ÅÕ¹¾Ñ²¹Òã¹ÃдѺ·Õʧ¢Ö¹ ¡ÒþѲ¹Ò¼Å§Ò¹ÇÔ¨Â
Ñ é Œ è èÙ é Ñ
244.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 217
¡ç¨Ð´ÕáÅÐÁÒ¡¢Ö¹µÒÁÅíҴѺ Siriraj Burn unit ÁÕ¹âºÒ¡ÒþѲ¹Òͧ¤¤ÇÒÁÃÙáÅмŧҹ´ŒÒ¹ÇÔ¨Â
é Œ Ñ
á¡‹º¤Åҡ÷ѧ˹‹ÇÂäÁ‹ÇÒ¨Ð໚¹ÍÒ¨ÒÃÂᾷ ᾷ»ÃШíÒºŒÒ¹ ¾ÂÒºÒÅ ·ÕÁ¤ÇÒÁʹã¨áÅзíÒ§Ò¹
Ø é ‹ è Õ
ÍÂÙ‹ ³ ËͼٻÇÂáË‹§¹Õé »˜¨¨Øº¹ÁÕ¾ÂÒºÒÅàªÕÂǪÒÃдѺ 9 1 ¤¹ ¾ÂÒºÒÅàªÕÂǪÒÃдѺ 8 ¶Ö§
Œ † Ñ è è
6 ¤¹ àÃÒ¶×ÍNjҺؤÅÒ¡Ãã¹Ë¹‹Ç§ҹ·Ø¡¤¹¤×Í burn team à´ÕÂǡѹ áÅШзíÒ§Ò¹ã¹áºº team work
à¾×ÍÊÌҧª×ÍàÊÕ§ãËŒ¡ºÊ¶ÒºÑ¹¤×Í ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ
è è Ñ ÔÔ
ºØ¤ÅÒ¡Ãã¹Ë¹‹Ç§ҹ¹íÒàʹͼŧҹÇԨѷÑé§ã¹áÅе‹Ò§»ÃÐà·È
ÃÒ§ÇÑÅáË‹§¤ÇÒÁÊíÒàÃç¨ã¹Ãͺ 5 »‚·Õ輋ҹÁÒ໚¹¼Å§Ò¹¢Í§ºØ¤ÅÒ¡Ã Siriraj Burn Team:
ä´ŒÃѺÃÒ§ÇÑÅ˹‹Ç§ҹ´Õà´‹¹´ÒǷͧ ¹Çѵ¡ÃÃÁ´Õà´‹¹ áÅÐ
ÃÒ§ÇÑŪ¹ÐàÅÔȨҡ¡ÒûÃСǴ¼Å§Ò¹ÇÔ¨ÂÁÒ¡ÁÒÂ
Ñ
¢³Ð¹ÕàÃÒÁÕ Siriraj Burn Unit Âؤ»ÃѺ»ÃاãËÁ‹ àÁ×ÍÁÕºÒ¹ËÅѧãËÁ‹·¾ÃŒÍÁ·Ñ§ã¹´ŒÒ¹ºØ¤ÅÒ¡Ã
é è Œ Õè é
·ÕÁ§Ò¹ à¤Ã×ͧÁ×ÍÍØ»¡Ã³¡ÒÃᾷ··¹ÊÁÑ ¡çà»ÃÕºàÊÁ×͹ÁÕÃÒ¡°Ò¹·Õá¢ç§á¡Ã‹§ ¾ÃŒÍÁ·Õ¨Ð¾Ñ²¹Ò
è Õè Ñ è è
ËÃ×Í¡ŒÒǵ‹Íä»´ŒÇ¤ÇÒÁÁѹ¤§ ¡íÒÅѧÊíҤѢͧºØ¤Åҡ÷ء淋ҹã¹ËͼٻÇ Siriraj burn unit ¤×Í
è Œ †
áç¼ÅÑ¡´Ñ¹·Õ¨Ð·íÒãËŒ»ÃÐʺ¤ÇÒÁÊíÒàÃ稴ѧ·ÕËÇѧäÇŒ ໚¹ËͼٻÇ·ÕãËŒ¡ÒôÙáÅÃÑ¡ÉҼٻǴŒÇ¨Եã¨
è è è Œ † è Œ †
ºÃÔÊ·¸Ôì äÁ‹Á§ËÇѧ¼Å¡íÒäÃËÃ×ͼŵͺ᷹ã´æ àÃÒ ËÃ×Í “Siriraj Burn Team” 㹤ÇÒÁËÁÒ¢ͧ¼Á
Ø Ø‹
¹Ñ¹¤×ͤÇÒÁËÇÁÁ×ͷѧËÁ´¨Ò¡àÅ×Í´ÊÕà´ÕÂǡѹ¹Ñ¹¤×Í¡íÒÅѧ¼ÅÑ¡´Ñ¹¨Ò¡ÊͧÊÒ¢ÒÇÔªÒ¤×Í ÈÑÅÂÈÒʵÃ
é é è
ÍغѵÔà˵ØáÅÐÈÑÅÂÈÒʵõ¡áµ‹§ ÍÕ¡¡ÅØ‹Á§Ò¹Ë¹Ö觷Õè¼ÁÍ´·Õè¨Ð¢Íº¤Ø³áÅЪ×蹪Áà¾ÃÒжŒÒ¢Ò´à¢Ò
àËÅ‹Ò¹Õä» ¡Ò÷íÒ§Ò¹ã¹Ëͼٻǹդ§äÁ‹ÃÒºÃ׹໚¹á¹‹¹¹¤×Í ·ÕÁ¾ÂÒºÒżÙàªÕÂǪҴŒÒ¹¡ÒôÙáÅ
é Œ † é è Ñè Œ è
¼Ù»ÇÂä¿äËÁŒáÅкؤÅÒ¡Ãã¹ËͼٻÇ Siriraj Burn Unit ·Ñ§ËÁ´ ³ ºÑ´¹Õé Siriraj Burn Unit ¨Ð໚¹
Œ † Œ † é
245.
218 Journey to Excellent Burn Unit
˹‹Ç§ҹ˹֧·Õ¾ÃŒÍÁ¨ÐËÇÁ¡Ñ¹ÊÌҧª×ÍàÊÕ§Íѹà¡ÃÕ§ä¡ÃãËŒ¡ºÀÒ¤ÇÔªÒÈÑÅÂÈÒʵÃÈÃÃÒªÍѹ໚¹·Õè
è è è Ñ ÔÔ
ÃÑ¡ÂÔ§¢Í§àÃÒ ¾ÃŒÍÁ·Õ¨Ð¡ŒÒÇä»Í‹ҧäÁ‹ËÂØ´ÂѧÊÁ´Ñ§¤íÒ “Journey to Excellent Siriraj Burn Unit.”
è è é
ÊØ´·ŒÒ¹ռÁ¢ÍãËŒ Siriraj Burn Unit ¨Ð໚¹ËͼٻÇ·ըÐ໚¹·Õ¾§ËÃ×ͤÇÒÁËÇѧ˹֧¢Í§¼Ù»ÇºҴà¨çº
é Œ † è è Öè è Œ †
ä¿äËÁŒã¹»ÃÐà·Èä·ÂÍѹ໚¹·Õá¢Í§àÃÒµÅÍ´¡ÒŹҹ
èÑ
àǪÈÒʵ÷¹Âؤ 2553
Ñ 227
4. Mirels H. Metastatic disease in long bones: A prosposed scoring system for diagnosing impending pathologic
fractures. Clin Orthop 1989;249:256-64.
5. Damron TA and Sim .H. Instructional Course Lectures, The Ameriacan Acadamy of Orthopaedic Surgeons
– Operative Treatment for Metastatic Disease of the Pelvis and the Proximal End of the .emur. J Bone Joint
Surg Am. 2000;82:114-26.
6. Malawer MM and Sugarbaker PH. Treatment of Metastatic Bone Disease in Musculoskeletal Cancer Surgery.
Philadelphia: Kluwer Acadamic Publishers; 2001: 215-30.
7. Lewis VO. Surgical Management of Upper Extremity Metastatic Disease in Schwartz HS editor. Orthopaedic
Knowledge Update: Musculoskeletal Tumors 2. 2nd ed. Rosemont: American Acadamy of Orthopaedic Surgeons
2007: 375-82.
8. Weber KL, Randall RL, Grossman S, Parvizi J. Management of Lower-Extremity Bone Metastasis. J Bone
Joint Surg Am. 2006;88:11-9.
230 Practical Management of Dysfunctional Uterine Bleeding
3. Menstrual phase ໚¹à˵ءÒó·à¡Ô´ËÅѧ¨Ò¡ÊÔ¹ÊØ´ luteal phase ¡Ò÷Õè corpus luteum
Õè é
ËÂØ´¡Ò÷íÒ§Ò¹ ·íÒãËŒäÁ‹ÁÎÍÃâÁ¹à¾È¨Ò¡Ãѧ䢋ä»ËÅ‹ÍàÅÕ§àÂ×ͺØÁ´ÅÙ¡ãËŒ¤§ÊÀÒ¾µ‹Íä»ä´Œ àÂ×ͺØ
Õ é è è
Á´ÅÙ¡¨ÐËÅØ´ÅÍ¡ÍÍ¡à¡Ô´à»š¹ raw surface ·íÒãËŒÁàÅ×Í´Í͡໚¹ÃдÙ
Õ
¹Í¡¨Ò¡¼Å¨Ò¡¡ÒÃà»ÅÕè¹á»Å§¢Í§ÎÍÃâÁ¹áÅŒÇÂѧÁÕ¡Ãкǹ¡ÒÃà»ÅÕè¹á»Å§ã¹ÃдѺ
âÁàÅ¡ØÅ (molecular cascade) ã¹àÂ×ͺØÁ´ÅÙ¡(3) ÁÕ¡ÒÃÊÌҧÊÒà cytokine áÅÐÎÍÃâÁ¹·ÕÍÍ¡Ä·¸Ôì
è è
Ẻ paracrine ÊÒÃàËÅ‹Ò¹Õ·ÒãËŒà¡Ô´ÁÕË´ÃÑ´µÑÇã¹ arteriole áÅÐ coiled artery ¢Í§Á´ÅÙ¡ ·íÒãËŒàÂ×ͺØ
é í è
Á´ÅÙ¡¢Ò´àÅ×Í´áÅÐÍÍ¡«ÔਹÁÒàÅÕ§ ÁÕ¡ÒûŴ»Å‹ÍÂàÍ繫ÑÂÁÍÍ¡ÁÒ‹ÍÂÊÅÒÂà¹×ÍàÂ×Í áÅŒÇàÂ×ͺءç
é é è è
¨ÐÅÍ¡ËÅØ´ÍÍ¡¾ÃŒÍÁ¡Ñ¹·ÑǷѧâ¾Ã§Á´ÅÙ¡ ¾ÃŒÍÁ¡ÑºÁÕàÅ×Í´ÍÍ¡¨Ò¡ raw surface áŌǨ֧µÒÁÁÒ´ŒÇÂ
è é
¡ÒáÃе،¹¡Ãкǹ¡ÒÃá¢ç§µÑǢͧàÅ×Í´ áÅСÃкǹ¡Òë‹ÍÁá«Áà¹×éÍàÂ×èÍ ·íÒãËŒàÅ×Í´ËÂØ´ áÅÐ
ÁÕàÂ×ͺØÁ´ÅÙ¡ãËÁ‹à¨ÃÔÁÒ»¡¤ÅØÁ¼¹Ñ§â¾Ã§Á´ÅÙ¡ ´Ñ§¹Ñ¹ËÒ¡àÂ×ͺØÁ´Å١䴌ú¡ÒáÃеع´ŒÇÂÎÍÃâÁ¹
è é è Ñ Œ
Í‹ҧäÁ‹àËÁÒÐÊÁ ¨Ð·íÒãËŒâ¤Ã§ÊÌҧ¢Í§Áѹà»ÃÒкҧ ÁÕ¡ÒÃÊÅÒÂáÅÐÅÍ¡ËÅØ´Í͡໚¹Ë‹ÍÁæ
äÁ‹¾ÃŒÍÁ¡Ñ¹·ÑǷѧâ¾Ã§Á´ÅÙ¡ ¨Ö§·íÒãËŒÁàÅ×Í´Ãдٷ¼´»¡µÔ
è é Õ Õè Ô
¤ÇÒÁÊÑÁ¾Ñ¹¸ÃÐËÇ‹Ò§ÎÍÃâÁ¹à¾È¡Ñº¡ÒÃÁÕàÅ×Í´ÍÍ¡¨Ò¡â¾Ã§Á´ÅÙ¡(4)
¡ÒÃà»ÅÕ¹á»Å§¢Í§ÎÍÃâÁ¹à¾Èã¹ÃٻẺµ‹Ò§æ Ê‹§¼ÅãËŒÁàÅ×Í´ÍÍ¡¨Ò¡â¾Ã§Á´ÅÙ¡ ´Ñ§¹Õé
è Õ
Estrogen-progesterone withdrawal bleeding ¤×Í ÀÒÇÐàÅ×Í´ÍÍ¡ÀÒÂËÅѧ¨Ò¡ä´ŒÃº¡Òà Ñ
¡Ãеع´ŒÇ estrogen áÅÐ progesterone µÒÁÅíҴѺ àÁ×ÍËÂØ´ãËŒÎÍÃâÁ¹¡ç¨ÐÁÕàÅ×Í´ÍÍ¡¨Ò¡ secretory
Œ è
endometrium àÅ×Í´·ÕÍÍ¡¨Ò¡¡ÒáÃеع´ŒÇÂÎÍÃâÁ¹ã¹ÅѡɳйÕé 䴌ᡋ Ãдٻ¡µÔã¹Ãͺà´×͹·ÕÁÕ
è Œ è
䢋µ¡ ËÃ×ÍàÅ×Í´·ÕÍÍ¡ÀÒÂËÅѧ¡ÒÃ㪌ÎÍÃâÁ¹áºº sequential ¤×Í ãËŒ estrogen áŌǵÒÁ´ŒÇ progestin
è
Progesterone withdrawal bleeding ¤×Í ÀÒÇÐàÅ×Í´ÍÍ¡ËÅѧ¨Ò¡ä´ŒÃº progesterone ËÃ×Í
Ñ
progestin áÅŒÇËÂØ´ãËŒÎÍÃâÁ¹¹ÕµÍ ¨ÐÁÕàÅ×Í´ÍÍ¡¨Ò¡ secretory endometrium ¤ÅŒÒ¡ÒÃÁÕÃдٵÒÁ
é ‹
»¡µÔ ¤×Í ÁÕ estrogen-progesterone withdrawal bleeding ·Ñ§¹Õà¹×ͧ¨Ò¡ progestin ¨ÐÍÍ¡Ä·¸ÔµÍàÂ×Í
é é è ì ‹ è
ºØÁ´ÅÙ¡ä´Œ¡µÍàÁ×ÍàÂ×ͺع¹ä´ŒÃº¡ÒáÃеع´ŒÇ estrogen ÁÒ¡‹Í¹à·‹Ò¹Ñ¹ «Ö§ estrogen 㹡óչÕé
ç ‹ è è Ñé Ñ Œ é è
¤×Í estrogen ·ÕÃÒ§¡Ò¼ÅÔµÁÒ¨Ò¡Ãѧ䢋àͧ àÅ×Í´·ÕÍÍ¡¨Ò¡¡ÒáÃеع´ŒÇÂÎÍÃâÁ¹ã¹ÅѡɳйÕé 䴌ᡋ
è‹ è Œ
àÅ×Í´·ÕÍÍ¡ÀÒÂËÅѧ¡ÒÃÃѺ»Ãзҹ progestin à¾×ÍàÅ×͹Ãд٠ËÃ×Í à¾×Í¡Òêѡ¹íÒãËŒÁÃдÙã¹¼Ù·¢Ò´
è è è è Õ Œ Õè
ÃдÙà¹×ͧ¨Ò¡ÀÒÇÐäÁ‹Á䢋µ¡
è Õ
Estrogen withdrawal bleeding ¤×Í ÀÒÇÐàÅ×Í´ÍÍ¡ËÅѧ¨Ò¡ËÂØ´ãËŒ¡ÒáÃеع´ŒÇ estrogen
Œ
à¾Õ§Í‹ҧà´ÕÂÇ ¨ÐÁÕàÅ×Í´ÍÍ¡¨Ò¡ proliferative endometrium «Ö§¨ÐÅÍ¡ËÅØ´äÁ‹¾ÃŒÍÁ¡Ñ¹·Ñ§â¾Ã§
è é
Á´ÅÙ¡ áÅÐËÅØ´äÁ‹ËÁ´ àÁ×ÍãËŒÎÍÃâÁ¹áºº¹Õ໚¹ÃÐÂÐàÇÅÒ¹Ò¹¡ç¨Ð·íÒãËŒÁ¤ÇÒÁàÊÕ§µ‹Í¡ÒÃ໚¹à¹×Í
è é Õ è é
§Í¡¢Í§àÂ×ͺØÁ´ÅÙ¡ (endometrial neoplasia) àÅ×Í´·ÕÍÍ¡¨Ò¡¡ÒáÃеع´ŒÇÂÎÍÃâÁ¹ã¹ÅѡɳйÕé
è è Œ
䴌ᡋ ¡ÒÃãËŒÎÍÃâÁ¹ã¹ÊµÃÕÇÂËÁ´ÃдÙâ´ÂãˌẺ estrogen-only regimen «Ö§ã¹»˜¨¨Øº¹¨ÐäÁ‹ãËŒ
Ñ è Ñ
ÎÍÃâÁ¹áºº¹Õã¹ÊµÃշ§ÁÕÁ´ÅÙ¡
é Õè Ñ
Estrogen-progesterone breakthrough bleeding ¤×Í ÀÒÇÐàÅ×Í´ÍÍ¡ã¹¢³Ð·Õèä´ŒÃѺ
estrogen áÅÐ progesterone ËÇÁ¡Ñ¹Í‹ҧµ‹Íà¹×ͧ໚¹àÇÅÒ¹Ò¹ ¡Åä¡·Õ·ÒãËŒÁàÅ×Í´ÍÍ¡¼Ô´»¡µÔ
è è í Õ
240 Practical Management of Dysfunctional Uterine Bleeding
14. Vilos GA, Tureanu V, Garcia M, Abu-Rafea B. The levonorgestrel intrauterine system is an effective treatment
in women with abnormal uterine bleeding and anticoagulant therapy. J Minim Invasive Gynecol. 2009;16:
480-4.
15. Hill D, Maher P. Treatment of menorrhagia by endometrial ablation. Med J Aust. 1990;152:564-5.
16. .raser IS, Angsuwathana S, Mahmoud ., Yezerski S. Short and medium term outcomes after rollerball
endometrial ablation for menorrhagia. Med J Aust. 1993;158:454-7.
17. .raser IS. The dysfunctional uterus: dysmenorrrhea and dysfunction uterine bleeding. In: Shearman RP,
editor. Clinical reproductive endocrinology. New york: Churchill Livingstone; 1985. 579-98.
18. Jutras ML, Cowan BD. Abnormal bleeding in the climacteric. Obstet Gynecol Clin North Am 1990;17:409-25.
19. Lacey JV, Jr., Chia VM. Endometrial hyperplasia and the risk of progression to carcinoma. Maturitas. 2009;63:
39-44.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 249
ËÒÂã¨à˹ÕÂÇ¢Œ¹ÁÒ¡¼Ô´»¡µÔ áÅÐú¡Ç¹¡Ò÷íÒ§Ò¹¢Í§ÈÕàÅÕ â´Â·Õâ¤Ã§ÊÌҧ·Ò§¨ØÅÀÒ¤ áÅСÒ÷íÒ è
§Ò¹¢Í§ÈÕàÅÕÂÂѧ»¡µÔ à¡Ô´ colonization ¢Í§áº¤·ÕàÃÕ ·íÒãËŒà¡Ô´¡ÒõԴàª×Í«éÒàµÔÁ áÅÐàÃ×ÍÃѧ áÅÐ é í é
¾ºÇ‹Òâä cystic fibrosis ÁÕ䫹ÑÊÍÑ¡àʺàÃ×ÍÃѧ áÅÐ ÃÔ´Êմǧ¨ÁÙ¡ä´ŒºÍ â´ÂÃŒÍÂÅÐ 40 ¢Í§ cystic
é ‹
fibrosis ÁÕôÊմǧ¨Á١ËÇÁ´ŒÇÂ
Ô (9)
2. âä¨ÁÙ¡ÍÑ¡àʺÀÙÁÔᾌ (Allergic rhinitis) ¨Ò¡¡ÒÃÈÖ¡ÉÒ ¾ºÍغµ¡Òó¢Í§âä¨ÁÙ¡ Ñ Ô
ÍÑ¡àʺÀÙÁᾌ䴌ºÍÂã¹¼Ù»ÇÂ䫹ÑÊÍÑ¡àʺ àÁ×Íà·Õº¡Ñº»ÃЪҡû¡µÔ
Ô ‹ Œ † è (10, 11)
»¯Ô¡ÃÂÒ¡ÒÃÍÑ¡àʺ¨Ò¡
ÔÔ
ÀÙÁᾌã¹âä¨ÁÙ¡ÍÑ¡àʺÀÙÁᾌ ÍÒ¨·íÒãËŒà¡Ô´ä«¹ÑÊÍÑ¡àʺàÃ×ÍÃѧ䴌§Ò¢ֹ à¹×ͧ¨Ò¡àÂ×ͺØâ¾Ã§¨ÁÙ¡ ÁÕ
Ô Ô é ‹ é è è
¡ÒÃÍÑ¡àʺáÅкÇÁ ä»ÍØ´¡Ñ¹ºÃÔàdzÃÙà»´¢Í§ä«¹ÑÊ à¡Ô´ä«¹ÑÊÍÑ¡àʺ䴌 Í‹ҧäáçµÒÁ äÁ‹¾ºÍغµÔ
é Ñ
¡Òó¢Í§ä«¹ÑÊÍÑ¡àʺ㹼ٻÇÂâä¨ÁÙ¡ÍÑ¡àʺÀÙÁᾌ ÁÒ¡¢Ö¹ã¹ª‹Ç§Ä´Ù¡ÒÅ·ÕÁÊÒá‹ÍÀÙÁᾌÁÒ¡
Œ † Ô é è Õ Ô (12)
ÀÒÇÐÀÙÁᾌ໚¹ÊÒà˵Ø˹֧¢Í§ä«¹ÑÊÍÑ¡àʺ áÅÐ໚¹ä´Œ·§ predisposing áÅÐ contributing factor
Ô è Ñé
¢Í§¡ÒÃÍÑ¡àʺã¹âä䫹ÑÊÍÑ¡àʺ ¡ÒÃÃÑ¡ÉÒâäÀÙÁᾌÃÇÁ´ŒÇ ¨Ð·íÒãËŒ¼Å¢Í§¡ÒÃÃÑ¡ÉÒ䫹ÑÊÍÑ¡ Ô ‹
àʺ´Õ¢Ñé¹ ÍÒ¨äÁ‹¨íÒ໚¹µŒÍ§·íÒ¡Òü‹ÒµÑ´ËÃ×ͶŒÒ¨íÒ໚¹µŒÍ§¼‹ÒµÑ´ ¨Ð·íÒãËŒ¼Å¡Òü‹ÒµÑ´¹Ñé¹´ÕÂÔè§
¢Ö¹(13, 14)
é
ºÒ§¡ÒÃÈÖ¡ÉÒ¾ºÍغµ¡Òó¢Í§âä¨ÁÙ¡ÍÑ¡àʺÀÙÁᾌ ä´ŒºÍÂ䴌㹼ٻÇÂÃÔ´Êմǧ¨ÁÙ¡ µÑ§áµ‹
Ñ Ô Ô ‹ Œ † é
ÃŒÍÂÅÐ 10-64 (15, 16)
ᵋºÒ§¡ÒÃÈÖ¡ÉÒ¡çäÁ‹¾ºÍغµ¡Òó¢Í§âä¨ÁÙ¡ÍÑ¡àʺÀÙÁᾌ ·Õʧ¼Ô´»¡µÔã¹¼ÙŒ
Ñ Ô Ô èÙ
»†ÇÂÃÔ´Êմǧ¨ÁÙ¡ (17, 18)
´Ñ§¹Ñé¹âä¨ÁÙ¡ÍÑ¡àʺÀÙÁÔᾌ äÁ‹ãª‹ÊÒà˵آͧ¡ÒÃà¡Ô´ÃÔ´Êմǧ¨ÁÙ¡àÊÁÍä»
ᵋ¶ÒÃÔ´Êմǧ¨ÁÙ¡ à¡Ô´ã¹¼Ù»ÇÂâä¨ÁÙ¡ÍÑ¡àʺÀÙÁᾌ »¯Ô¡ÃÂÒ¡ÒÃÍÑ¡àʺ¨Ò¡ÀÙÁᾌ¨Ð·íÒãˌôÊմǧ
Œ Œ † Ô ÔÔ Ô Ô
¨ÁÙ¡ÁÕ¢¹Ò´âµ¢Ö¹ ËÃ×ÍÁըҹǹÁÒ¡¢Ö¹ä´Œ ËÃ×Í·íÒãËŒ¡ÅѺ໚¹«éÒ䴌͡
é í é í Õ
3. âäË×´ âä䫹ÑÊÍÑ¡àʺ¾ºÃ‹ÇÁ¡ÑºâäË×´ä´ŒºÍ ¾ºÇ‹ÒÃŒÍÂÅÐ 40 ¶Ö§ 75 ¢Í§¼Ù»Ç ‹ Œ †
âäË×´ ÁÕ»ËÒâä䫹ÑÊÍÑ¡àʺàÃ×ÍÃѧ ã¹¢³Ð·ÕÃÍÂÅÐ 35 ¢Í§¼Ù»ÇÂâä䫹ÑÊÍÑ¡àʺàÃ×ÍÃѧ ÁÕ»ËÒ
˜ é (19)
èŒ Œ † é ˜
âäË״ËÇÁ´ŒÇ ÁÕËÅÑ¡°Ò¹áÊ´§ãËŒàËç¹Ç‹Ò ¼Ù»Ç·Õ໚¹âäË×´ ¨ÐÁÕÍÒ¡ÒÃá‹ŧ àÁ×Í໚¹âä䫹ÑÊ
(20)
Œ † è è
ÍÑ¡àʺËÇÁ´ŒÇ (21)
áÅÐàÁ×ÍãËŒ¡ÒÃÃÑ¡ÉÒ䫹ÑÊÍÑ¡àʺáÅŒÇ äÁ‹ÇÒ´ŒÇÂÂÒ ËÃ×Í¡Òü‹ÒµÑ´¨Ð·íÒãËŒÍÒ¡ÒâͧâäË×´
è ‹
´Õ¢¹ áÅмٻÇÂ㪌ÂÒÃÑ¡ÉÒâäË×´¹ŒÍÂŧ
Öé Œ † (22)
¡Åä¡·Õè·íÒãËŒ¡Ò÷íÒ§Ò¹¢Í§·Ò§à´Ô¹ËÒÂã¨Ê‹Ç¹Å‹Ò§¼Ô´»¡µÔã¹¼ÙŒ»†Ç·Õè໚¹âä䫹ÑÊ
ÍÑ¡àʺÁմѧµ‹Í仹Õé
3.1) ¼Ù·à»š¹âä䫹ÑÊÍÑ¡àʺ ÁÕ¡Ò÷íÒ§Ò¹¢Í§¨ÁÙ¡ «Ö§·íÒ˹ŒÒ·Õ໚¹µÑÇ¡ÃͧÍÒ¡ÒÈ áÅÐ
Œ Õè è è
»ÃѺÊÀÒ¾ÍÒ¡ÒÈàÊÕÂä» ¼Ù»ÇµŒÍ§ËÒÂ㨷ҧ»Ò¡ (mouth breathing) ·íÒãËŒ·Ò§à´Ô¹ËÒÂã¨Ê‹Ç¹Å‹Ò§
Œ †
ÁÕâÍ¡ÒÊÊÑÁ¼ÑʡѺÊÒá‹ÍÀÙÁᾌ áÅÐÊÔ§ÃФÒÂà¤×ͧÁÒ¡¢Ö¹ ໚¹¼ÅãËŒà¡Ô´¡Ãкǹ¡ÒÃÍÑ¡àʺ áÅÐ
Ô è é
à¾ÔÁ¤ÇÒÁäǢͧËÅÍ´ÅÁµ‹ÍÊÒáÃеع㹼ٻÇ·ÕÁ¤ÇÒÁàÊÕ§·Õ¨Ðà¡Ô´âäË×´
è Œ Œ † è Õ è è
3.2) Naso-sinobronchial reflex »ÃÐÊÒ·ÃѺ¤ÇÒÁÃÙÊ¡¨Ò¡â¾Ã§¨ÁÙ¡ áÅÐ䫹ÑÊ ÊÒÁÒö ŒÖ
Ê‹§ÊÑÒ³»ÃÐÊҷ仵ÒÁ»ÃÐÊÒ·ÊÁͧ¤Ù‹·Õè 5 áÅÐÃѺÊÑÒ³»ÃÐÊÒ·ÁÒ·Ò§Ãкº»ÃÐÊÒ·
parasympathetic ʋǹ»ÃÐÊÒ·ÃѺ¤ÇÒÁÃÙÊ¡¨Ò¡·Ò§à´Ô¹ËÒÂã¨Ê‹Ç¹Å‹Ò§ÊÒÁÒöʋ§ÊÑÒ³»ÃÐÊÒ·
΅
仵ÒÁ»ÃÐÊÒ·ÊÁͧ¤Ù·Õè 10 áÅÐÃѺÊÑÒ³»ÃÐÊÒ·ÁÒ·Ò§ parasympathetic à¾×ͤǺ¤ØÁ¡Ò÷íÒ
‹ è
àǪÈÒʵ÷¹Âؤ 2553
Ñ 255
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Meltzer EO, Hamilos DL, Hadley JA, Lanza DC, Marple B., Nicklas RA, et al. Rhinosinusitis: Establishing
definitions for clinical research and patient care. Otolaryngol Head Neck Surg 2004;131(6 SUPPL.):S1-62.
2. Lethbridge-Cejku M, Rose D, Vickerie J. Summary health statistics for U.S. adults: National Health Interview
Survey, 2004. National Center for Health Statistics. Vital Health Stat 2006;10(228):19-22.
3. Bhattacharyya N. Clinical and symptom criteria for the accurate diagnosis of chronic rhinosinusitis. Laryngoscope
2006;116:1185-91.
4. Gwaltney JM, Jr. Acute community-acquired sinusitis. Clin Infect Dis 1996;23:1209-23.
5. Bent JP III, Kuhn .A. Allergic fungal rhinosinusitis/polyposis. Allergy Asthma Proc 1996;17:259-68.
6. Chandler JR, Langenbrunner DJ, Stevens ER. The pathogenesis of orbital complications in acute sinusitis.
Laryngoscope 1970;80(9):1414-28.
7. Busuttil A. Dysplastic epithelial changes in nasal polyps. Ann Otol Rhinol Laryngol 1978;87(3 Pt 1):416-20.
8. Hasegawa M, Nasu M, Ohki M, Sugiuchi Y, Watanabe I. Malignant transformation of nasal polyp. Case
report. Arch Otolaryngol Head Neck Surg 1988;114(3):336-7.
9. Hadfield PJ, Rowe-Jones JM, Mackay IS. The prevalence of nasal polyps in adults with cystic fibrosis. Clin
Otolaryngol 2000;25(1):19-22.
10. Emanuel IA, Shah SB. Chronic rhinosinusitis: allergy and sinus computed tomography relationships. Otolaryngol
Head Neck Surg 2000;123(6):687-91.
11. Beninger M. Rhinitis, sinusitis and their relationship to allergies. Am J Rhinol 1992;6:37-43.
12. Karlsson G, Holmberg K. Does allergic rhinitis predispose to sinusitis? Acta Otolaryngol Suppl 1994;515:26-8.
13. Zacharek MA, Krouse JH. The role of allergy in chronic rhinosinusitis. Curr Opin Otolaryngol Head Neck Surg
2003;11:196-200.
14. Krause H.. Allergy and chronic rhinosinusitis. Otolaryngol Head Neck Surg 2003;128:14-6.
15. Blumstein GI, Tuft LI. Allergy treatment in recurrent nasal polyposis: its importance and value. Am J Med Sci
1957;234(3):269-80.
16. English G. Nasal polyposis. In: GM E, editor. Otolaryngology. Philadelphia: Harper and Row; 1985. p. 1-30.
17. Drake-Lee AB. Histamine and its release from nasal polyps: preliminary communication. J R Soc Med
1984;77(2):120-4.
18. Liu CM, Shun CT, Hsu MM. Lymphocyte subsets and antigen-specific IgE antibody in nasal polyps. Ann
Allergy 1994;72(1):19-24.
19. Spector SL, Bernstein IL, Li JT, Berger WE, Kaliner MA, Schuller DE, et al. Parameters for the diagnosis and
management of sinusitis. J Allergy Clin Immunol 1998;102:S107-44.
20. Hoover G, Newman LJ, Platts-Mills TA, Phillips CD, Gross CW, Wheatley LM. Chronic sinusitis: risk factors for
extensive disease. J Allergy Clin Immunol 1997;100:185-91.
21. Druce HM, Slavin RG. Sinusitis: a critical need for further study. J Allergy Clin Immunol 1991;88: 675-77.
22. Oliveira CA, Sole D, Naspitz CK, Rachelefsky GS. Improvement of bronchial hyperresponsiveness in asthmatic
children treated for concomitant sinusitis. Ann Allergy Asthma Immunol 1997;79:70-4.
23. Klossek JM, Neukirch ., Pribil C, Jankowski R, Serrano E, Chanal I, et al. Prevalence of nasal polyposis in
.rance: A cross-sectional, case-control study. Allergy 2005;60(2):233-7.
24. Settipane GA, Chafee .H. Nasal polyps in asthma and rhinitis. A review of 6,037 patients. J Allergy Clin
Immunol 1977;59(1):17-21.
283.
256 䫹ÑÊÍÑ¡àʺ áÅÐÃÔ´Êմǧ¨ÁÙ¡
25. Settipane G. Epidemiology of nasal polyps. In: Settipane G, Lund VJ, Bernstein JM, Tos M., editors. Nasal
polyps: epidemiology, pathogenesis and treatment. Rhode Island: Oceanside Publications; 1997. p. 17-24.
26. Batra PS, Kern RC, Tripathi A, Conley DB, Ditto AM, Haines GK, 3rd, et al. Outcome analysis of endoscopic
sinus surgery in patients with nasal polyps and asthma. Laryngoscope. 2003;113(10):1703-6.
27. Szczeklik A, Stevenson DD. Aspirin-induced asthma: advances in pathogenesis, diagnosis, and management.
J Allergy Clin Immunol. 2003;111(5):913-21.
28. Spector SL, Wangaard CH, .arr RS. Aspirin and concomitant idiosyncrasies in adult asthmatic patients. J
Allergy Clin Immunol. 1979;64(6 Pt 1):500-6.
29. Ogino S, Harada T, Okawachi I, Irifune M, Matsunaga T, Nagano T. Aspirin-induced asthma and nasal polyps.
Acta Otolaryngol Suppl. 1986;430:21-7.
30. Batra PS, Kem RC, Tripathi A, Conley DB, Ditto AM, Haines GK 3rd, et al. Outcome analysis of endoscopic
sinus surgery in patients with nasal polyps and asthma. Laryngoscope 2003;113(10):1703-6.
31. Szczeklik A, Nizankowska E, Duplaga M. Natural history of aspirin-induced asthma. AIANE Investigators.
European Network on Aspirin-Induced Asthma. Eur Respir J 2000;16(3):432-6.
32. DiBaise JK, Olusola B., Huerter JV, Quigley EM. Role of GERD in chronic resistant sinusitis: A prospective,
open label, pilot trial. Am J Gastroenterol 2002;97:843-50.
33. Ulualp SO, Toohill RJ, Hoffmann R, Shaker R. Possible relationship of gastroesophagopharyngeal acid reflux
with pathogenesis of chronic sinusitis. Am J Rhinol 1999;13:197-202.
34. El-Serag HB, Sonnenberg A. Co-morbid occurrence of laryngeal or pulmonary disease with esophagitis in
United States military veterans. Gastroenterology 1997;113:755-60.
35. Bothwell MR, Parsons DS, Talbot A, Barbero GJ, Wilder B. Outcome of reflux therapy on pediatric chronic
sinusitis. Otolaryngol Head Neck Surg 1999;121:255-62.
36. DiBaise JK, Huerter JV, Quigley EM. Sinusitis and gastroesophageal reflux disease. Ann Intern Med
1998;129:1078.
37. Oslen K, Kern E, Westbrook P. Sleep and breathing disturbance secondary to nasal obstruction. Otolaryngol
Head Neck Surg 1981;89:804-10.
38. Klossek JM, Serrano E, Peloquin L, Percodani J, .ontanel JP, Pessey JJ. .unctional endoscopic sinus
surgery and 109 mycetomas of paranasal sinuses. Laryngoscope 1997;107(1):112-7.
39. Brook I. The role of bacteria in chronic rhinosinusitis. Otolaryngol Clin N Am 2005;38(6):1171-92.
40. Thomas M, Yawn B, .okken W. European position paper on the primary care diagnosis and management of
rhinosinusitis and nasal polyp 2007. Prim Care Resp J 2008;17(2):79-89.
41. .okkens WJ, Lund VJ, Mullol J, Bachert C, Cohen N, Cobo R, et al. European position paper on nasal polyp
2007. Rhinology 2007;45(suppl 20):1-139.
42. Dolor RJ, Witsell DL, Hellkamp AS. Comparison of cefuroxime with or without intranasal fluticasone for the
treatment of rhinosinusitis. JAMA 2001;286(24):3097-105.
43. Helmberg K, Juliesson S, Balder B. .luticasone propionate aqueous nasal spray in the treatment of nasal
polyposis. Ann Allergy Asthma Immunol 1997;78(3):270-6.
44. Cervin A, Wallwork B. Anti-inflammatory effects of macrolide antibiotics in the treatment of chronic rhinosinusitis.
Otolaryngol Clin N Am 2005;38(6):1339-50.
45. Meltzer EO, Bachert C, Staudinger H. Treating acute rhinosinusitis: comparing efficacy and safety of mometasone
furoate nasal spray, amoxicillin, and placebo. J Allergy Clin Immunol 2005;116(6):1289-95.
46. KhalilH, Nunez DA. .unctional endoscopic sinus surgery for chronic rhinosinusitis. Cochrane Database of
Systematic Reviews 2006, Issue 3. Art. No.: CD004458. DOI: 0.1002/14651858.CD004458.pub2.
284.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 257
47. Krouse JH, Christmas DA, Jr. Powered instrumentation in functional endoscopic sinus surgery. II: A comparative
study. Ear Nose Throat J 1996;75(1):42.
48. Hackman TG, .erguson BJ. Powered instrumentation and tissue effects in the nose and paranasal sinuses.
Curr Opin Otolaryngol Head Neck Surg 2005;13(1):22-6.
49. Metson R, Cosenza M, Gliklich RE, Montgomery WW. The role of image-guidance systems for head and neck
surgery. Arch Otolaryngol Head Neck Surg 1999;125:1100–4.
50. Tabaee A, Hsu AK, Shrime MG, Rickert S, Close LG. Quality of life and complications following image-guided
endoscopic sinus surgery. Otolaryngol Head Neck Surg 2006;135:76–80.
264 ¡ÒÃ䴌¹º¡¾Ã‹Í§ã¹à´ç¡â´ÂÀÒ¾ÃÇÁáÅСÒäѴ¡Ãͧ¡ÒÃ䴌¹ã¹à´ç¡ááà¡Ô´
Ô Ô
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Joint committee on infant hearing: American Academy of Audiology; American Academy of Pediatrics; American
Speech-Language-Hearing Association; Directors of Speech and Hearing Programs in State Health and Welfare
Agencies. Year 2007 position statement: Principles and Guidelines for Early Hearing Detection and Intervention
Programs. Pediatrics. 2008; 120(4): 898-921.
2. Nelson HD, Bougatsos C, Nygren P, Universal newborn hearing screening: Systematic review to update the
2001 US preventive services task force recommendation. Pediatrics. 2008; 122(1):e266-76.
3. White KR, Vohr BR, Behrens TR. Universal newborn hearing screening using transient evoked otoacoustic
emissions: results of the Rhode Island hearing assessment project. Semin Hear. 1993; 14:18-29.
4. Mehl AL, Thomson V. The Colorado newborn hearing screening project, 1992-1999: on the threshold of
effective population-based universal newborn hearing screening. Pediatrics. 2002; 109(1). Available at: www.
Pediatrics.org/cgi/content/full/109/1/e7
5. American Speech-Language-Hearing Association. www.asha.org
6. Atipas S, Chongkolwatana C. Newborn hearing screening: Overview. Siriraj Med J. 2009: 224-27.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 269
¡ÒÃÃÑ¡ÉÒ´ŒÇ¡Òü‹ÒµÑ´ 䴌ᡋ ¡ÒÃà¨ÒÐá¡ŒÇËÙâ´Â㪌à¢çÁ´Ù´¹éÒã¹ËÙª¹¡ÅÒ§ (tympanocentesis)
í Ñé
à¾×ÍÊ‹§à¾ÒÐàª×Í ¡Òü‹ÒµÑ´à¨ÒÐá¡ŒÇËÙ (myringotomy) ¡ÒÃãÊ‹·Í»ÃѺ¤ÇÒÁ´Ñ¹ (tympanostomy tube)
è é ‹
áÅСÒü‹ÒµÑ´ adenoidectomy Áբͺ‹§ªÕé ´Ñ§¹Õé
Œ
¢ŒÍº‹§ªÕ㹡Ò÷íÒ tympanocentesis(9) 䴌ᡋ ÁÕÍÒ¡ÒûǴËÙùáç 䢌ʧ ÍÒ¡ÒÃäÁ‹´¢¹ ËÃ×Í
é Ø Ù Õ Öé
໚¹ÁÒ¡¢Ö¹ äÁ‹µÍºÊ¹Í§µ‹ÍÂÒµŒÒ¹¨ØŪվÀÒÂã¹ 24-48 ªÑÇâÁ§ ໚¹ AOM ã¹¢³Ð·Õä´ŒÂÒµŒÒ¹¨ØŪվ
é è è
à¾×ÍÃÑ¡ÉÒâäÍ×¹ÍÂÙ‹ ໚¹ AOM ã¹à´ç¡ááà¡Ô´ ËÃ×Í immunocompromised host
è è
¢ŒÍº‹§ªÕ㹡Ò÷íÒ myringotomy(9) 䴌ᡋ ÁÕ suppurative complication ¨Ò¡ AOM »Ç´ËÙÁÒ¡
é
¨Ò¡ AOM à»´á¡ŒÇËÙãËŒ¡ÇŒÒ§¢Ö¹ËÅѧ·íÒ tympanocentesis áÅÐ acute barotitis
é
¢ŒÍº‹§ªÕ㹡ÒÃãÊ‹ tympanostomy tube(9) 䴌ᡋ ÁÕ suppurative complication ໚¹ OME ã¹ËÙ
é
Êͧ¢ŒÒ§¹Ò¹ 3 à´×͹¢Ö¹ä» ËÃ×Í໚¹ OME ã¹ËÙ˹֧¢ŒÒ§ ¹Ò¹ 6 à´×͹¢Ö¹ä» ᵋ¶ÒÁÕÃдѺ¡ÒÃ䴌¹ÊÙ§
é è é Œ Ô
¡Ç‹Ò 25 dB ËÃ×ÍÁÕ»ËҾѲ¹Ò¡ÒôŒÒ¹ÀÒÉÒ ÍÒ¨¾Ô¨ÒóÒãÊ‹·Í»ÃѺ¤ÇÒÁ´Ñ¹àÃçÇ¢Ö¹ recurrent AOM
˜ ‹ é
·Õèä´ŒÃѺ antibiotic prophylaxis áÅŒÇäÁ‹ä´Œ¼Å, recurrent OME â´Â໚¹¹Ò¹ÃÇÁ¡Ñ¹Í‹ҧ¹ŒÍÂ
6-12 à´×͹ ÁÕ Eustachian tube dysfunction ઋ¹ 䴌ú hyperbaric oxygen, ÁÕ atelectasis ËÃ×Í
Ñ
retraction pocket ¢Í§á¡ŒÇËÙ áÅÐ㪌㹡óռҵѴ tympanoplasty ã¹à´ç¡·Õè Eustachian tube Âѧ·íÒ
‹
§Ò¹äÁ‹ä´ŒµÒÁ»¡µÔ
ʋǹ¡Òü‹ÒµÑ´ adenoidectomy ËÇÁ¡Ñº myringotomy áÅÐ tympanostomy tube insertion
Áբͺ‹§ªÕé 䴌ᡋ ¼Ù»Ç otitis media ·ÕÁ»ËҢͧµ‹ÍÁ adenoid ËÇÁ´ŒÇ ઋ¹ ÁÕ obstructive sleep
Œ Œ † è Õ ˜
apnea ËÃ×Í chronic rhinosinusitis, áÅÐ㹼ٻǠrecurrent otitis media ·Õ䴌ú¡ÒÃãÊ‹ tympanostomy
Œ † è Ñ
tube áÅŒÇ tube ËÅØ´ áÅШíÒ໚¹µŒÍ§ãÊ‹ tube «éÒ í
¡ÒþÂҡóâä
¼Ù»Ç·Õ໚¹ AOM ÊÒÁÒöËÒÂä´Œàͧ ÃŒÍÂÅÐ 60 ÀÒÂã¹ 24 ªÑÇâÁ§ áÅÐÃŒÍÂÅÐ 80 ÀÒÂã¹
Œ † è è
2-3 Çѹ â´Â·ÕÃÍÂÅÐ 10 ¢Í§à´ç¡·Õ໚¹ AOM ¨ÐÁÕ middle ear effusion ¹Ò¹ 3 à´×͹¢Ö¹ä» ã¹¢³Ð
(10)
èŒ è é
·Õ¼»Ç·Õ໚¹ OME ¹Ñ¹ ÃŒÍÂÅÐ75-90 ÊÒÁÒöËÒÂä´ŒàͧÀÒÂã¹ 3 à´×͹ ᵋ¾ºÇ‹ÒÃŒÍÂÅÐ 30-40
è ÙŒ † è é (5)
¢Í§à´ç¡ÁÕ¡ÒáÅѺ໚¹«éÒ áÅÐÃŒÍÂÅÐ 5-10 ¢Í§ OME ໚¹¹Ò¹ÁÒ¡¡Ç‹ÒËÃ×Í෋ҡѺ 1 »‚(2, 11)
í
¶Ö§áÁŒÇҼٻǷÕ໚¹ AOM áÅÐ OME ¨ÐÁÕ¡ÒþÂҡóâä·Õ´Õ â´Â·Õ¡ÒÃ䴌¹ÊÒÁÒö¡ÅѺ
‹ Œ † è è è Ô
ÊÙÊÀÒÇл¡µÔä´Œ ᵋ¶ÒËÒ¡äÁ‹ä´ŒÃº¡ÒôÙáÅÃÑ¡ÉÒ ËÃ×ÍÃÑ¡ÉÒäÁ‹¶¡µŒÍ§ ÍÒ¨à¡Ô´¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹
‹ Œ Ñ Ù Ô
ã¹ÃÐÂÐÂÒÇä´Œ ઋ¹ COM «Ö觼ٌ»†Ç¡ÅØ‹Á¹ÕéÁÕá¡ŒÇËÙ·ÐÅØ ÁÕ˹ͧäËŨҡËÙ໚¹æ ËÒÂæ ÍÒ¨ÁÕ
cholesteatoma ËÇÁ´ŒÇ «Ö§ÊÒÁÒö·íÒÅÒ¡Ãд١ÃÙ»¤ŒÍ¹ ·Ñ§ â¡Å¹ä´Œ ÃÇÁ¶Ö§ÍÒ¨¹íÒä»ÊÙÀÒÇÐá·Ã¡
è è ‹
«ŒÍ¹Í×¹æ ·Ñ§ intratemporal áÅÐ intracranial complications
è é
㹼ٻǠOME ËÃ×Í Eustachian tube dysfunction ·Õ໚¹Ãعáç ÍÒ¨ÁÕ retraction pocket
Œ † è
«Ö§¨Ð·íÒãËŒà¡Ô´ cholesteatoma µÒÁÁÒä´Œ ËÃ×ÍÍÒ¨à¡Ô´¡ÒÃῺµÑǢͧᡌÇËٺҧʋǹ (atelectasis)
è
ËÃ×ͷѧËÁ´ (adhesive otitis media) µÔ´¡Ñº¼¹Ñ§´ŒÒ¹ã¹¢Í§ËÙª¹¡ÅÒ§ à¡Ô´¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹áÅÐ
é Ñé Ô
â¤Ã§ÊÌҧÍ‹ҧ¶ÒÇà ¢Í§ËÙª¹¡ÅÒ§ «Ö§ÂÒ¡µ‹Í¡ÒÃá¡Œä¢
Ñé è
297.
270 ¡ÒÃÊÙàÊÕ¡ÒÃä´ŒÂÔ¹¨Ò¡¡ÒùíÒàÊÕ§àÊ×èÍÁã¹¼ÙŒ»†ÇÂà´ç¡
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Teele DW, Klein JO, Rosner B. Epidemiology of otitis media during the first seven years of life in children in
greater Boston: a prospective, cohort study. J Infect Dis. 1989;160(1):83-94.
2. Tos M. Epidemiology and natural history of secretory otitis. Am J Otol. 1984;5(6):459-62.
3. Paradise JL, Rockette HE, Colborn DK, Bernard BS, Smith CG, Kurs-Lasky M, et al. Otitis media in 2253
Pittsburgh-area infants: prevalence and risk factors during the first two years of life. Pediatrics. 1997;99(3):
318-33.
4. Casselbrant ML, Mandel EM. Epidemiology. In: Rosenfeld RM, Bluestone CD, editors. Evidence-based otitis
media. 2nd ed. Hamilton, Ontario: BC Decker Inc; 2003. p. 147-62.
5. Rosenfeld RM, Culpepper L, Doyle KJ, Grundfast KM, Hoberman A, Kenna MA, et al. Clinical practice
guideline: Otitis media with effusion. Otolaryngol Head Neck Surg. 2004;130(5 Suppl):S95-118.
6. Diagnosis and management of acute otitis media. Pediatrics. 2004;113(5):1451-65.
7. Germiller JA. Hearing loss in children. In: Wetmore R., editor. Pediatric Otolaryngology. 1st ed. Philadelphia:
Mosby; 2007. p. 60-76.
8. Rosenfeld RM, Bluestone CD. Clinical pathway for otitis media with effusion. In: Rosenfeld RM, Bluestone
CD, editors. Evidence-based otitis media. 2nd ed. Hamilton(ON): BC Decker;2003. p. 303-24.
9. Bluestone CD. Role in management of otitis media. In: Bluestone CD, editor. Eustachain tube: structure,
function , role in otitis media. 1st ed. Ontario: BC Decker; 2005. p. 145-76.
10. Rosenfeld RM, Kay D. Natural history of untreated otitis media. Laryngoscope. 2003;113(10):1645-57.
11. Williamson IG, Dunleavey J, Bain J, Robinson D. The natural history of otitis media with effusion—a three-year
study of the incidence and prevalence of abnormal tympanograms in four South West Hampshire infant and
first schools. J Laryngol Otol. 1994;108(11):930-4.
272 ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹㹼ٻÇÂà´ç¡¨Ò¡ÊÒà˵طҧ¾Ñ¹¸Ø¡ÃÃÁ
Ô Œ †
¡ÒÃÊÙàÊÕ¡ÒÃä´ŒÂÔ¹ª¹Ô´à»š¹¡ÅØ‹ÁÍÒ¡Òà (Syndromic hearing loss)
¡ÅØ‹ÁÍÒ¡Ò÷ҧ¾Ñ¹¸Ø¡ÃÃÁ»ÃÐÁÒ³ 400 âä¨ÐÁÕ¡ÒÃÊÙàÊÕ¡ÒÃä´ŒÂԹ໚¹ÍÒ¡ÒùíÒËÃ×Í
ÍÒ¡Ò÷վºÃ‹ÇÁ¡Ñº¤ÇÒÁ¼Ô´»¡µÔÍ‹ҧÍ×¹ ´Ñ§¹Ñ¹¼Ù»ÇÂÍÒ¨¨ÐÁÒ¾ºá¾·Â´Ç»˜ËÒ¡ÒÃ䴌¹ ઋ¹
è è é Œ † Œ Ô
¾Ù´ªŒÒËÃ×ÍäÁ‹ËѹµÒÁàÊÕ§ ËÃ×ÍÍÒ¨ÁÒ¾ºá¾·Â´ŒÇ»˜ËÒàÃ×èͧÍ×è¹ áµ‹á¾·ÂµÃǨ¾ºÇ‹Ò¼ÙŒ»†ÇÂ
ÁÕ¤ÇÒÁ¼Ô´»¡µÔ¢Í§¡ÒÃ䴌¹ËÇÁ´ŒÇ ´Ñ§¹Ñ¹¡ÒôÙáżٻÇÂ㹡ÅØÁ¹Õ¨§¨íÒ໚¹·Õ¨ÐµŒÍ§ÍÒÈÑÂá¾·Â
Ô é Œ † ‹ éÖ è
¼ÙŒàªÕèÂǪÒËÅÒÂÊÒ¢Òà¾×è͵ÃǨËÒáÅдÙáŤÇÒÁ¼Ô´»¡µÔ¢Í§ÃкºÍ×è¹ ã¹º·¤ÇÒÁ¹Õé¨Ðẋ§¡ÅØ‹Á
¢Í§ syndromic hearing loss µÒÁ¤ÇÒÁ¼Ô´»¡µÔ·Õ辺ËÇÁáÅСµÑÇÍ‹ҧ¡ÅØ‹ÁÍÒ¡Ò÷Õ辺º‹ÍÂ
㹡ÅØÁ¹Ñ¹æ(6)
‹ é
ÃÙ»·Õè 1 áÊ´§¡ÅØ‹ÁÊÒà˵طҧ¾Ñ¹¸Ø¡ÃÃÁ¢Í§¡ÒÃÊÙàÊÕ¡ÒÃä´ŒÂÔ¹(5)
1. âä¢Í§â¤ÃâÁâ«Á (Chromosome disorders) ·ÕÁ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹ËÇÁ´ŒÇÂ
è Õ Ô
âä¢Í§â¤ÃâÁâ«Á·Õ辺º‹Í·ÕèÊØ´¤×Í ¡ÅØ‹ÁÍÒ¡ÒôÒǹ (Down syndrome) «Ö觨оº
conductive hearing loss ä´Œ¶§ÃŒÍÂÅÐ 60-80 ¨Ò¡¤ÇÒÁ¼Ô´»¡µÔ¢Í§ËÙª¹¡ÅÒ§ »˜¨¨Ñ·շÒãËŒÁ¤ÇÒÁ
Ö Ñé è í Õ
¼Ô´»¡µÔ¢Í§ËÙª¹¡ÅÒ§ã¹à´ç¡¡ÅØÁÍÒ¡ÒôÒǹ¤Í Eustachian tube ᤺ pharyngeal hypotonia áÅÐ
Ñé ‹ ×
¡ÒõԴàª×Í·Ò§à´Ô¹ËÒÂ㨺‹ÍÂæ âä¢Í§â¤ÃâÁâ«ÁÍ×¹æ ઋ¹ ¡ÅØÁÍÒ¡Òà Turner ¨Ð¾ºÁÕ conductive
é è ‹
ËÃ×Í mixed hearing loss 㹪‹Ç§ÇÑÂà´ç¡ ᵋàÁ×ÍÍÒÂØÁÒ¡¢Ö¹¨Ð໚¹ sensorineural hearing loss ¡ÅØÁ
è é ‹
ÍÒ¡Òà velocardiofacial «Ö§à¡Ô´¨Ò¡¢Ò´ËÒÂ仢ͧâ¤ÃâÁâ«Á 22q11.2 ¡ÅØÁÍÒ¡ÒùըÐÁÕྴҹâËÇ‹
è ‹ é
ËÑÇ㨾ԡÒÃᵋ¡Òà¹Ô´ áÅÐÅѡɳÐãºË¹ŒÒ·Õ¨Òà¾ÒÐ ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹㹡ÅØÁÍÒ¡ÒùÕé à¡Ô´ä´Œ·§¨Ò¡
í èí Ô ‹ Ñé
conductive áÅÐ sensorineural hearing loss
300.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 273
2. ¡ÅØÁÍÒ¡Ò÷ÕÁ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ÈÕÃÉÐáÅÐãºË¹ŒÒ (Craniofacial syndromes)
‹ è Õ
·ÕÁ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹ËÇÁ´ŒÇÂ
è Õ Ô
䴌ᡋ¡ÅØÁÍÒ¡Ò÷ÕÁ¡Òû´¢Í§Ã͵‹Í¡ÐâËÅ¡ÈÕÃÉÐàÃçÇ¡Ç‹Ò¡íÒ˹´ (craniosynostosis
‹ è Õ
syndromes) ·Õ¾ºº‹ÍÂ䴌ᡋ¡ÅØÁÍÒ¡Òà Crouzon áÅСÅØÁÍÒ¡Òà Apert «Ö§¡ÅØÁÍÒ¡ÒÃàËÅ‹Ò¹ÕÁ¡ÒÃ
è ‹ ‹ è ‹ é Õ
¶‹Ò·ʹ·Ò§¾Ñ¹¸Ø¡ÃÃÁẺÂչഋ¹ áÅÐà¡Ô´¨Ò¡¡ÒáÅÒ¾ѹ¸Ø¢Í§ÂÕ¹ fibroblast growth factor
receptor 2 (.G.R2) ·Ñ§ 2 ¡ÅØÁÍÒ¡ÒùըÐÁÕ conductive hearing loss ËÇÁ¡Ñº¡Òû´àÃçÇ¡Ç‹Ò¡íÒ˹´
é ‹ é
¢Í§ coronal sutures µÒ⻹ (exorbitism) à¹×ͧ¨Ò¡ª‹Í§¡ÐâËÅ¡ÊíÒËÃѺÅÙ¡µÒµ×¹ ᵋ¡ÅØÁÍÒ¡Òà Apert
è é ‹
¨ÐÁÕ¤ÇÒÁ¼Ô´»¡µÔ¢Í§Á×ÍáÅÐ෌Ҥ×Í ¹ÔÇÁ×Í ¹ÔÇà·ŒÒ äÁ‹á¡¨Ò¡¡Ñ¹ (syndactyly) ¹Í¡¨Ò¡¹Õé ¡ÅØÁÍÒ¡ÒÃ
é é ‹
craniosynostosis ·Õ¾º sensorineural hearing loss ä´Œ¤Í Muenke syndrome «Ö§à¡Ô´¨Ò¡¡ÒáÅÒÂ
è × è
¾Ñ¹¸Ø¢Í§ÂÕ¹ .G.R3
3. ¡ÅØ‹ÁÍÒ¡Ò÷ҧ¾Ñ¹¸Ø¡ÃÃÁ·Õèà¡Ô´¨Ò¡¤ÇÒÁ¼Ô´»¡µÔ¢Í§ branchial arch ·Õè 1
áÅÐ 2
âä·Õ¾ºº‹Í·Õʴ㹡ÅØÁ¹Õ䴌ᡋ oculo-auriculo-vertebral (OAV) spectrum âä¹ÕÁ¡à»š¹
è èØ ‹ é é Ñ
¤¹à´ÕÂÇ㹤Ãͺ¤ÃÑÇ áÅÐÁÕÊÒà˵ط·ÒãËŒà¡Ô´âäËÅÒ¡ËÅÒ·ѧ·Ò§¾Ñ¹¸Ø¡ÃÃÁáÅÐÊÔ§áÇ´ÅŒÍÁ ઋ¹
Õè í é è
ÁÒôÒ໚¹àºÒËÇÒ¹¢³ÐµÑ§¤ÃÃÀ ÅѡɳФÇÒÁ¼Ô´»¡µÔᵋ¡Òà¹Ô´ã¹ OAV spectrum ¨Ðà¡Ô´¨Ò¡¤ÇÒÁ
é í
¼Ô´»¡µÔ¢Í§¡ÒÃÊÌҧÍÇÑÂÇзվ²¹ÒÁÒ¨Ò¡ branchial arch ·Õè 1 áÅÐ 2 䴌ᡋ ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ËÙ
è Ñ
ઋ¹ äÁ‹ÁãºËÙ ËÃ×ÍãºËÙàÅç¡ µÔ§Ë¹ŒÒËÙ ãºË¹ŒÒ 2 «Õ¡äÁ‹à·‹Ò¡Ñ¹ (hemifacial microsomia) ¤ÇÒÁ¼Ô´»¡µÔ
Õ è
¢Í§µÒ ઋ¹ epibulbar dermoid áÅФÇÒÁ¼Ô´»¡µÔ¢Í§¡Ãд١ÊѹËÅѧ ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹·Õ¾ºÃ‹ÇÁÔ è
ʋǹãË‹ ¨Ð໚¹ conductive hearing loss ʋǹ¹ŒÍÂÍÒ¨ÁÕ sensorineural hearing loss ¹Í¡¨Ò¡
¤ÇÒÁ¼Ô´»¡µÔ¢Í§ÈÕÃÉÐáÅÐãºË¹ŒÒáÅŒÇ OAV spectrum ÍÒ¨ÁÕ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ÍÇÑÂÇÐÀÒÂã¹Ã‹ÇÁ´ŒÇÂ
ઋ¹ ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ËÑÇã¨áÅÐäµáµ‹¡Òà¹Ô´ âä·Õ¾ºä´ŒºÍÂÃͧŧÁÒ¤×Í ¡ÅØÁÍÒ¡Òà Treacher-Collins
í è ‹ ‹
«Ö觨ÐÁÕ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ÈÕÃÉÐáÅÐãºË¹ŒÒઋ¹¡Ñ¹áµ‹¨Ðᵡµ‹Ò§µÃ§·Õè ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ãºË¹ŒÒ
áÅÐËÙ·§ 2 ¢ŒÒ§¨ÐàËÁ×͹¡Ñ¹ ¡ÅØÁÍÒ¡Òùըоº¤ÇÒÁ¼Ô´»¡µÔ¢Í§¡ÒÃ䴌¹»ÃÐÁҳÌÍÂÅÐ 40 ¡ÅØÁ
Ñé ‹ é Ô ‹
ÍÒ¡Òà Treacher-Collins à¡Ô´¨Ò¡¡ÒáÅÒ¾ѹ¸Ø¢Í§ÂÕ¹ TCO.1 «Ö§ÁÕ¡Òö‹Ò·ʹẺÂչഋ¹
è
4. ¡ÅØ‹ÁÍÒ¡Ò÷ҧ¾Ñ¹¸Ø¡ÃÃÁ·ÕèÁÕ¤ÇÒÁ¼Ô´»¡µÔ¢Í§¤ÍáÅÐËÙËÇÁ¡Ñ¹ (Cervico-
acoustic defects)
âä·Õ¾ºº‹ÍÂ㹡ÅØÁ¹Õ¤Í ¡ÅØÁÍÒ¡Òà Branchio-Oto-Renal (BOR) «Ö§à»š¹âä·Ò§¾Ñ¹¸Ø¡ÃÃÁ
è ‹ é × ‹ è
·Õ¶Ò·ʹẺÂչഋ¹ áÅÐà¡Ô´¨Ò¡¡ÒáÅÒ¾ѹ¸Ø¢Í§ÂÕ¹ EYA1 ¤ÇÒÁ¼Ô´»¡µÔ·¾º¤×Í ãºËÙ¼´»¡µÔ
è ‹ Õè Ô
ÁÕµ§ËÃ×ÍÃÙàÅç¡æ˹ŒÒËÙ branchial cleft cyst ËÃ×Í fistula áÅФÇÒÁ¼Ô´»¡µÔ¢Í§äµ ¤ÇÒÁ¼Ô´»¡µÔ¢Í§
Ôè
¡ÒÃ䴌¹¨ÐÁÕä´Œ·§ conductive hearing loss áÅÐ sensorineural hearing loss
Ô Ñé
301.
274 ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹㹼ٻÇÂà´ç¡¨Ò¡ÊÒà˵طҧ¾Ñ¹¸Ø¡ÃÃÁ
Ô Œ †
5. âä¡Ãд١¾Ñ¹¸Ø¡ÃÃÁ (Skeletal dysplasias)·ÕÁ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹ËÇÁ´ŒÇÂ
è Õ Ô
âä¡Ãд١¾Ñ¹¸Ø¡ÃÃÁ·ÕÍÒ¨ÁÒ¾ºá¾·Â´ÇÂàÃ×ͧ»˜ËÒ¡ÒÃ䴌¹ 䴌ᡋ ¡ÅØÁÍÒ¡ÒÃ
è Œ è Ô ‹
Stickler «Ö觡ÒÃÊÙàÊÕ¡ÒÃä´ŒÂÔ¹¨Ð໚¹ª¹Ô´ sensorineural hearing loss ¤ÇÒÁ¼Ô´»¡µÔ
¢Í§ÃкºÍ׹䴌ᡋ ÊÒµÒÊѹ ¨Í»ÃÐÊÒ·µÒËÅØ´ÅÍ¡ (retinal detachment) ྴҹâËÇ‹ (cleft
è é
palate) áÅФÇÒÁ¼Ô´»¡µÔ¢Í§ÀÒ¾ÃѧÊÕ·Õè epiphysis áÅСÃд١ÊѹËÅѧ ¡ÅØÁÍÒ¡Òà Stickler
‹
à¡Ô´¨Ò¡¡ÒáÅÒ¾ѹ¸Ø¢Í§ÂÕ¹·ÕÊÌҧ¤ÍÅÅÒਹª¹Ô´·Õè 2 áÅÐ 11
è
6. ¡ÅØÁÍÒ¡Ò÷ÕÁ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹ËÇÁ¡Ñº¤ÇÒÁ¼Ô´»¡µÔ¢Í§äµ
‹ è Õ Ô
¡ÅØÁÍÒ¡Ò÷ÕÁ»ËҢͧ¡ÒÃ䴌¹ËÇÁ¡Ñº¤ÇÒÁ¼Ô´»¡µÔäµ ä´Œá¡‹ ¡ÅØÁÍÒ¡Òà Alport «Ö§
‹ è Õ ˜ Ô ‹ è
ÁÕ¤ÇÒÁ¼Ô´»¡µÔ¢Í§äµà»š¹ chronic nephritis ·íÒãËŒÁÕ microscopic hematuria ËÇÁ¡Ñº¡Ò÷íÒ§Ò¹¢Í§
䵤‹ÍÂæá‹ŧ ʋǹ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹¨ÐàÃÔÁÍÒ¡ÒÃàÁ×ͼٻÇÂࢌÒÊÙÇÂÃع â´Â¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹
Ô è è Œ † ŒÑ ‹ Ô
¨Ð໚¹áºº sensorineural hearing loss ¹Í¡¨Ò¡¹ÕéÍÒ¨¾º¤ÇÒÁ¼Ô´»¡µÔ·Ò§µÒ໚¹µŒÍ¡ÃШ¡
(cataract) ËÃ×Í anterior lenticonus ä´Œ ¡Òö‹Ò·ʹ·Ò§¾Ñ¹¸Ø¡ÃÃÁ¢Í§¡ÅØÁÍÒ¡Òà Alport ÁÕä´ŒËÅÒÂ
‹
Ẻᵋ·¾ºº‹Í·ÕÊ´¤×ÍẺ X-linked â´Âà¡Ô´¨Ò¡¡ÒáÅÒ¾ѹ¸Ø¢Í§ÂÕ¹¤ÍÅÅÒਹª¹Ô´·Õè 4 «Ö§à»š¹
Õè èØ è
â»ÃµÕ¹·ÕÊÒ¤Ñã¹ glomerular basement membrane
èí
7. ¡ÅØ‹ Á ÍÒ¡Ò÷Õè ÁÕ ¡ ÒÃÊÙ àÊÕ Â ¡ÒÃä´Œ ÂÔ ¹ Ë Ç Á¡Ñ º ¤ÇÒÁ¼Ô ´ »¡µÔ ¢ ͧàÁç ´ ÊÕ
(Pigmentary abnormalities)
µÑÇÍ‹ҧ¢Í§âä㹡ÅØÁ¹Õé 䴌ᡋ ¡ÅØÁÍÒ¡Òà Waardenburg «Ö§à»š¹ syndromic hearing
‹ ‹ è
loss ·Õ¶Ò·ʹẺÂչഋ¹·Õ¾ºº‹Í·ÕÊ´ ¼Ù»Ç¨ÐÁÕ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹Ẻ sensorineural hearing
è ‹ è èØ Œ † Ô
loss ËÇÁ¡Ñº¤ÇÒÁ¼Ô´»¡µÔ¢Í§àÁç´ÊÕ·¼Ç˹ѧ ËÃ×ÍàÊŒ¹¼Á ઋ¹ ÁÕšɳлͼÁ¢ŒÒ§Ë¹ŒÒÊÕ¢ÒÇ (white
Õè Ô Ñ
forelock) ËÃ×ÍÊբͧÁ‹Ò¹µÒ͋͹¼Ô´»¡µÔ (heterochromia irides) ¹Í¡¨Ò¡¹Õ¼»ÇÂÍÒ¨ÁÕ¤ÇÒÁ¾Ô¡ÒÃ
é ÙŒ †
ᵋ¡Òà¹Ô´¢Í§á¢¹ ËÃ×Í Hirschsprung disease ËÇÁ´ŒÇ¡ÅØÁÍÒ¡Òà Waardenburg à¡Ô´¨Ò¡¡ÒáÅÒÂ
í ‹
¾Ñ¹¸Ø¢Í§ÂÕ¹ PAX3, MIT., SNA12, EDNRB, EDN3 ËÃ×Í SOX10
8. ¡ÅØÁÍÒ¡Ò÷ÕÁ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹ËÇÁ¡Ñº¤ÇÒÁ¼Ô´»¡µÔ¢Í§µÒ
‹ è Õ Ô
㹡ÅØÁ¹Õâä·ÕÁ¤ÇÒÁÊíҤѷÕÊ´¤×Í ¡ÅØÁÍÒ¡Òà Usher «Ö§ÁÕ¡Òö‹Ò·ʹ·Ò§¾Ñ¹¸Ø¡ÃÃÁ
‹ é è Õ èØ ‹ è
ẺÂÕ¹´ŒÍ ¼Ù»Ç¨ÐÁÕ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹Ẻ sensorineural hearing loss µÑ§áµ‹ááà¡Ô´ áÅÐ
Œ † Ô é
ËÅѧ¨Ò¡¹Ñ¹¨ÐàÃÔÁÁÕ¤ÇÒÁ¼Ô´»¡µÔ¢Í§¨Í»ÃÐÊÒ·µÒ ·ÕàÃÕÂ¡Ç‹Ò retinitis pigmentosa «Ö§à»š¹¡ÒÃàÊ×ÍÁ
é è è è è
¢Í§¨Í»ÃÐÊÒ·µÒáÅйíÒä»ÊÙÍÒ¡ÒÃÁͧäÁ‹àËç¹ã¹àÇÅÒ¡ÅÒ§¤×¹ ÅÒ¹ÊÒÂµÒ (visual field) ᤺ŧ
‹
¨¹¡ÃзѧµÒºÍ´àÁ×ÍࢌÒÊÙÇÂÃع ´Ñ§¹Ñ¹¡ÅØÁÍÒ¡Òà Usher ¨Ö§à»š¹ÊÒà˵ØÊҤѢͧ¤ÇÒÁ¾Ô¡ÒëéÒ«ŒÍ¹
è è ‹Ñ ‹ é ‹ í í
·Ñ§¡ÒÃ䴌¹áÅСÒÃÁͧàËç¹ ·ÕÊҤѤ×Í retinitis pigmentosa ¨ÐÂѧäÁ‹»ÃÒ¡®ã¹ª‹Ç§ 10 »‚áá ᵋ
é Ô èí
¨ÐÊÒÁÒöµÃǨ¾º¤ÇÒÁ¼Ô´»¡µÔªÇ§áá¢Í§¨Í»ÃÐÊÒ·µÒä´Œ â´ÂÇÔ¸Õ electroretinography (ERG)
‹
302.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 275
¹Í¡¨Ò¡¹Õ¼»Ç¡ÅØÁÍÒ¡Òà Usher ª¹Ô´·Õè 1 ÍÒ¨ÁÕ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ vestibule ·íÒãËŒ¾²¹Ò¡ÒÃ
é ÙŒ † ‹ Ñ
à¡ÕÂǡѺ¡Ò֍µÑÇઋ¹ ¡ÒùѧËÃ×Íà´Ô¹ªŒÒ¡Ç‹Ò»¡µÔ
è è
9. ¡ÅØÁÍÒ¡Ò÷ÕÁ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹ËÇÁ¡Ñº¤ÇÒÁ¼Ô´»¡µÔ¢Í§µ‹ÍÁäÃŒ·Í
‹ è Õ Ô ‹
㹡ÅØÁ¹Õâä·ÕÊҤѷÕÊ´¤×Í ¡ÅØÁÍÒ¡Òà Pendred «Ö§à»š¹ syndromic hearing loss ·Õ¾º
‹ é èí èØ ‹ è è
º‹Í·ÕÊ´ ÅѡɳзÕÊҤѢͧâä¹Õ¤Í ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹ᵋ¡Òà¹Ô´áºº sensorineural hearing
èØ èí é × Ô í
loss Í‹ҧÃعáç ËÇÁ¡Ñº¤ÇÒÁ¼Ô´»¡µÔ¢Í§â¤Ã§ÊÌҧ¢Í§¡Ãд١ temporal áÅÐËÙª¹ã¹ áÅФ;͡
Ñé
ª¹Ô´äÁ‹à»š¹¾ÔÉ áµ‹¤Í¾Í¡¨ÐàÃÔÁáÊ´§ÍÒ¡ÒÃËÅѧࢌÒÊÙÇÂÃع ¤ÇÒÁ¼Ô´»¡µÔ¢Í§µ‹ÍÁä·ÃÍ´ à¡Ô´¨Ò¡
è ‹Ñ ‹
¤ÇÒÁº¡¾Ã‹Í§¢Í§ organification ¢Í§ iodine «Ö§ÊÒÁÒöµÃǨà¨Íä´Œ´Ç perchlorate discharge test
è Œ
ʋǹ¤ÇÒÁ¼Ô´»¡µÔ¢Í§â¤Ã§ÊÌҧ¢Í§ËÙª¹ã¹ (bony labyrinth) ¨ÐÁÕšɳТͧ vestibular aqueduct
Ñé Ñ
¢ÂÒÂãË‹¢Öé¹·ÕèàÃÕÂ¡Ç‹Ò Mondini dysplasia «Ö觵ÃǨà¨Íä´Œâ´ÂÀÒ¾ÃѧÊÕ¤ÍÁ¾ÔÇàµÍà (computed
tomography, CT) ¢Í§¡Ãд١ temporal âä¹Õ໚¹âä¾Ñ¹¸Ø¡ÃÃÁ ·Õ¶Ò·ʹẺÂÕ¹´ŒÍ áÅÐà¡Ô´¨Ò¡
é è ‹
¡ÒáÅÒ¾ѹ¸Ø¢Í§ÂÕ¹ SLC26A4 (PDS)
10. ¡ÅØÁÍÒ¡Ò÷ÕÁ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ËÑÇã¨Ã‹ÇÁ¡Ñº¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹
‹ è Õ Ô
âä·ÕÊÒ¤Ñ㹡ÅØÁ¹Õ¤Í ¡ÅØÁÍÒ¡Òà Jervell áÅÐ Lange-Nielson «Ö§¶‹Ò·ʹ·Ò§¾Ñ¹¸Ø¡ÃÃÁ
èí ‹ é × ‹ è
ẺÂÕ¹´ŒÍ ¼Ù»Ç¨ÐÁÕ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹Ẻ sensorineural hearing loss ËÇÁ¡Ñº¤ÇÒÁ¼Ô´»¡µÔ
Œ † Ô
¢Í§¤Å׹俿‡ÒËÑÇ㨠¤×ÍÁÕÃÐÂÐ QT interval ÂÒÇ¡Ç‹Ò»¡µÔ (ÁÒ¡¡Ç‹Ò 440 milliseconds) «Ö§ÍҨ໚¹
è è
ÊÒà˵طÒãËŒ¼»ÇÂàÊÕªÕǵ¡Ð·Ñ¹Ëѹ䴌 ´Ñ§¹Ñ¹¼Ù»Ç·ÕÁ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹ËÇÁ¡Ñº»ÃÐÇѵ·Á¤¹ã¹
í ÙŒ † Ô é Œ † è Õ Ô Ô Õè Õ
¤Ãͺ¤ÃÑÇàÊÕªÕǵ¡Ð·Ñ¹Ëѹ ໚¹âä¹Í¹ËÅѺµÒÂã¹·Òá (sudden infant death syndrome) ໚¹
Ô
ÅÁËÁ´ÊµÔºÍÂæ ËÃ×Í ¡ÅØÁÍÒ¡Òà long QT ¤ÇÃ䴌ú¡ÒõÃǨËÑÇã¨Í‹ҧÅÐàÍÕ´ ¡ÅØÁÍÒ¡ÒùÕà¡Ô´
‹ ‹ Ñ ‹ é
¨Ò¡¡ÒáÅÒ¾ѹ¸Ø¢Í§ÂÕ¹ KCNQ1 áÅÐ KCNE1
¡ÒÃÊÙàÊÕ¡ÒÃä´ŒÂÔ¹ª¹Ô´äÁ‹à»š¹¡ÅØ‹ÁÍÒ¡Òà (Nonsyndromic hearing loss)
໚¹âä·Ò§¾Ñ¹¸Ø¡ÃÃÁ·ÕèÁÕ¡ÒÃÊÙàÊÕ¡ÒÃä´ŒÂÔ¹ áÅÐäÁ‹ÁÕ¤ÇÒÁ¼Ô´»¡µÔÍ‹ҧÍ×è¹Ã‹ÇÁ´ŒÇÂ
â´ÂÁÕ¹·Õà¡ÕÂÇ¢ŒÍ§ 48 ÂÕ¹ âä¡ÅØÁ¹ÕÊÒÁÒöẋ§µÒÁÅѡɳСÒö‹Ò·ʹ·Ò§¾Ñ¹¸Ø¡ÃÃÁä´Œ´§¹Õé
Õ è è ‹ é Ñ
1. ¡ÒÃÊÙàÊÕ¡ÒÃ䴌¹ẺÂÕ¹´ŒÍ (autosomal recessive nonsyndromic hearing loss)
Ô
¾ºä´Œ
2. »ÃÐÁҳÌÍÂÅÐ 70 ¢Í§ nonsyndromic hearing loss ·Ñé§ËÁ´ áÅФÃÖè§Ë¹Ö觢ͧ
nonsyndromic hearing loss ·Õ趋Ò·ʹẺÂÕ¹´ŒÍ à¡Ô´¨Ò¡¡ÒáÅÒ¾ѹ¸Ø ¢Í§ÂÕ¹ GJB2
(connexin 26)(7) ¡ÒáÅÒ¾ѹ¸Ø·¾ºº‹Í·Õʴ㹪ÒǵÐÇѹµ¡¢Í§ÂÕ¹ GJB2 ¤×Í ¡ÒâҴËÒÂä»
Õè è Ø
¢Í§ guanine ·ÕµÒá˹‹§ 35 (35delG) ʋǹ㹻ÃÐà·ÈᶺàÍàªÕ ¡ÒáÅÒ¾ѹ¸Ø·¾ºº‹Í·ÕÊ´¤×Í
è í (8)
Õè èØ
¡ÒâҴËÒÂ仢ͧ cytosine ·ÕµÒá˹‹§ 235 (235delC) ʋǹÂÕ¹Í×¹¾ºà»š¹Ê‹Ç¹¹ŒÍÂ
è í (9)
è
àǪÈÒʵ÷¹Âؤ 2553
Ñ 279
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Jariengprasert C, Lertsukprasert K, Kasemsuwan L ,et al. Newborn hearing screening using otoacoustic
emission (OAEs): a 1-year study at Ramathibodi Hospital. Thai J Otolaryngol Head Neck Surg 2003;4:27–41.
2. Davis A, Parving A. Toward appropriate epidemiology data on childhood hearing disability: comparative
European study of birth cohorts 1982–88. J Audiol Med. 1994;3:35–47.
3. Marazita ML, Ploughman LM, Rawlings B, Remington E, Arnos KS, Nance WE. Genetic epidemiological
studies of early-onset deafness in the U.S. school-age population. Am J Med Genet. 1993;46:486–91.
4. Toriello HV, Reardon W, Gorlin R., editors. Hereditary hearing loss and its syndrome, 2nd ed. New York:
Oxford University Press, 2004.
5. Kochhar A, Hildebrand MS, Smith RJ. Clinical aspects of hereditary hearing loss. Genet Med. 2007;9:393-408.
6. .alk RE, Honrubia D, .ischel-Ghodsian N. Hereditary hearing loss and deafness. In: Rimoin DL, Connor JM,
Pyeritz RE, Korf BR, editors. Emery and Rimoin’s principles and practice of medical genetics, 5th ed. Philadelphia:
Churchill Livingstone; 2007. p.3265-303.
7. Estivill X, .ortina P, Surrey S, Rabionet R, Melchionda S, D’Agruma L, et al. Connexin-26 mutations in
sporadic and inherited sensorineural deafness. Lancet. 1998;351:394–8.
8. Snoeckx RL, Huygen PL, .eldmann D, Marlin S, Denoyelle ., Waligora J, et al. GJB2 mutations and degree
of hearing loss: a multicenter study. Am J Hum Genet. 2005;77:945-57.
9. Ohtsuka A, Yuge I, Kimura S, Namba A, Abe S, Van Laer L,et al. GJB2 deafness gene shows a specific
spectrum of mutations in Japan, including afrequent founder mutation. Hum Genet. 2003; 112:329–33.
10. .ischel-Ghodsian N. Mitochondrial mutations and hearing loss: paradigm for mitochondrial genetics. Am J Hum
Genet. 1998;62:15-9.
11. Wattanasirichaigoon D, Limwongse C, Jariengprasert C, Yenchitsomanus PT, Tocharoenthanaphol C,
Thongnoppakhun W, et al. High prevalence of V37I genetic variant in the connexin-26 (GJB2) gene among
non-syndromic hearing-impaired and control Thai individuals. Clin Genet. 2004;66:452-60.
296 ¡Òû‡Í§¡Ñ¹âäËÅÍ´àÅ×Í´ÊÁͧ·Ñ§¡‹Í¹áÅÐËÅѧ¡Òü‹ÒµÑ´
é
ÀÒ¤¼¹Ç¡
µÒÃÒ§áÊ´§ÃдѺ¤ÇÒÁ¹‹Òàª×èͶ×ͧ͢¢ŒÍÁÙÅ
Benefit (B) / I : B >>> R IIa : B >> R IIb : B ? R III : R > B
Risk (R)
Level A Multiple RCT* Some conflict Greater conflict Multiple RCT*
(3-5 trials)
Level B Single RCT* or Some conflict Greater comflict Single RCT* or
(2-3 trials) none RCT* none RCT*
Level C Expert opinion Expert opinion Expert opinion Expert opinion
(1-2 trials)
Summary Indicated Reasonable May be or unclear Not indicated
ËÁÒÂà赯 *RCT: randomized controlled trial
324.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 297
43
Scrub Typhus in Thailand
Yupin Suputtamongkol
Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University,
Human rickettsioses, known to occur in Thailand, include mainly scrub typhus and
murine typhus. Scrub typhus is caused by Orientia tsutsugamushi, an obligate intracellular
Gram-negative bacterium that has a different cell wall structure and genetic makeup from those
of rickettsiae.(1) It is transmitted to humans by the bite of the larval stage of trombiculid mites
(chiggers). Endemic areas of scrub typhus include rural areas of South-East Asia throughout the
Asia Pacific rim and Northern Australia. More than a billion people are at risk of infection and
about one million cases occur annually.(2) In Thailand the report incidence of scrub typhus has
increased during the previous decade.(2, 3) Clinical manifestations of this infection varies widely
from a mild and self-limited febrile illness to a more severe course which may be fatal.2 Scrub
typhus is recently recognized as a common cause of acute undifferentiated fever both in
indigenous population and ill travelers returning from the tropics. (2, 3)
Despite the availability of low cost and effective antibiotic treatment, scrub typhus
continues to cause significant morbidity and mortality in otherwise healthy adults and children.
The greatest challenge to clinician is early diagnosis of this infection, when antibiotic therapy is
most effective. The purpose of this presentation is to summarize the epidemiologic data using
new molecular tools, clinical manifestations and management of scrub typhus.
Epidemiology of scrub typhus in Thailand
Scrub typhus was first reported in human from central region of Thailand in 1952(4) and
O. tsutsugamushi was first isolated from rodent trapped from the same area in
1955.(5)Leptotrombidium deliensis is the primary vector of O. tsutsugamushi. However several
other species have been implicated as vectors such as L. Chiangraiensis, L. imphalum and
Blankaartia acuscutellaris.(6)
Nationwide seroepidemiological studies indicate that O. tsutsugamushi infection is
widespread in Thailand. The seropositivity rates of O. tsutsugamushi among soldiers and patients
325.
298 Scrub Typhus in Thailand
with acute febrile illness varied from 5.4% to 21%. These surveys have found high point
prevalence, varied from 13-31% of inhabitants in suburban Bangkok, to 59 -77% of inhabitants of
3 villages in the northern and northern region respectively.(7) According to the unpublished
records of the Public Health Ministry of Thailand, fewer than 100 cases of scrub typhus were
reported annually before 1983, 750–900 cases/year were reported between 1988 and 1991, and
3,000- 5,000 cases/year has been reported since 2001.
We conducted an epidemiological and clinical study of 1,663 patients with acute
undifferentiated fever, between October 2000 and March 2003 in 6 hospitals in rural Thailand;
four hospitals in the northeastern region, one hospital in the central region and one hospital in
the southern region. There were 268 (16.1%) patients with laboratory confirmed scrub typhus.(8)
The diagnosis of scrub typhus was made by PCR (101 out of 141 patients tested) or by indirect
immunofluorescent antibody (IFA) for combined Karp, Kato, and Gilliam strain of O.
tsutsugamushi (74 patients by a fourfold rising in titer to 1:400, 76 patients by a single titer to
1:400, 17 patients by a fourfold rising in titer or stable titers of at least 1:200). Blood culture
for aerobic bacteria and serological tests for leptospirosis, dengue infection were negative in all
of these patients. Scrub typhus, murine typhus, and SFG rickettsioses were diagnosed in
7.8%, 2.4%, and 5% respectively in the subgroup analysis of these patients who presented
with severe manifestations in our recent publication.(9)
Clinical features
The clinical presentations of scrub typhus are nonspecific. In our clinical study the
median duration of fever was 7 days in patients with scrub typhus. Headache, generalized
myalgia, and calf pain were very common. The classic manifestation of scrub typhus, includes
generalized lymphadenopathy, maculopapular rash and splenomegaly were not common in this
case series. Eschar was detected in 56 (20.9%) patients. Complications such as hepatic
dysfunction (defined as jaundice or total bilirubin 2.5 mg/dl, or high AST and/ or ALT level to
more than 120 IU, or high alkaline phosphatase level to more than 350 IU, or mixed abnormalities),
renal dysfunction (defined as oliguria or abnormal urea and/ or creatinine level), hypotension
(defined as systolic BP <90 mmHg on admission), congestive heart failure, or pulmonary
involvement (defined as abnormal chest radiography) were common in scrub typhus. Only 32%
of patients with scrub typhus did not have any complication on admission.
Hepatic dysfunction was the most common complication. Pulmonary involvement was
found in approximately half of study group. The chest radiographic abnormalities were similar to
those previously reported, except that hilar lymphadenopathy was not as common as previously
326.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 299
reported. Cardiac involvement defined by cardiomegaly or cardiac to thoracic ratio > 0.5 on PA
chest radiography or > 0.6 on AP chest radiography (36/119, 30.3%) or congestive heart failure
(23/119, 19.3%) were common abnormal radiographic findings in this study group. However this
finding was not associated with hypotension on admission. Approximately 12% of the patients
presented with multi-organ dysfunction mimic community-acquired septicemia in this case series.
Overall seven patients with scrub typhus died in this case series. The causes of dead
in all except one patient were multi-organ failure including respiratory failure. ARDS was not a
prominent cause of death in this study. The cause of death (bleeding hepatoma) was unrelated
to scrub typhus in one patient. Scrub typhus was not included in the differential diagnosis
therefore no effective treatment was given in four out of six patients who died. In addition scrub
typhus was diagnosed in 18 out of 51 (35.3%) of patients who presented with septic shock in
one of the study hospital between November 2001 and January 2002. The mortality was 16.7%
in this subgroup of scrub typhus with septic shock.(10)
Conclusion
Scrub typhus is presented with nonspecific symptoms and signs. Eschar is the only
clinical sign that differentiated scrub typhus from other infectious disease. Severe scrub typhus
can manifest as multi-organ dysfunction mimic septicemia from other causes and leptospirosis.
Unaware of the diagnosis of severe scrub typhus in these patients could lead to delay diagnosis
and high mortality.
Awareness that scrub typhus is a prominent cause of acute undifferentiated fever in
adults in Thailand improves the probability of an accurate clinical diagnosis. Early recognition
and appropriate treatment reduce morbidity and mortality. Results from recent clinical studies
from Thailand indicate that rational antimicrobial therapy would be doxycycline in mild cases
and a combination of either cefotaxime or ceftriaxone and doxycycline in severe cases.
Azithromycin could be considered as an alternative treatment when ever doxycycline allergy is
suspected. This would be either curative, or have no ill-effect, in the majority of instances.
Failure to improve or defervesce within the next 48 hours would indicate the need to a thorough
reevaluation of clinical findings and initial laboratory investigation results and a need to change
antibiotic.
327.
300 Scrub Typhus in Thailand
References
1. Tamura A, Ohashi N, Urakami H, Miyamura S. Classification of Rickettsia tsutsugamushi in a new genus,
Orientia gen. nov., as Orientia tsutsugamushi comb nov. Int J Syst Bacteriol 1995;45:589-91.
2. Watt G, Parola P. Scrub typhus and tropical rickettsioses. Curr Opin Infect Dis 2003;16:429-36.
3. Suttinont C, Losuwanaluk K, Niwatayakul K, Hoontrakul S, Intaranongpai W, Silpasakorn S, et al. Causes of
acute, undifferentiated, febrile illness in rural Thailand: results of a prospective observational study. Ann Trop
Med Parasitol 2006;100: 363-70.
4. Trishnanda M, Vasuvat C, Harinasuta C. Investigation of scrub typhus in Thailand. J Trop Med Hyg 1964;67:215-9.
5. Traub R, Johnson P, Mirsse M, Elbel R. Isolation of Rickettsia tsutsugamushi from rodents from Thailand. Am
J Trop Med Hyg 1954;3:356-9.
6. Lerdthusnee K, Khuntirat B, leepitakrat W, Tanskul P, Monkanna T, Khlaimanee N, et al. 2003. Vector
competence of Leptotrombidium Chiangraiensis chiggers and transmission efficacy and isolation of Orientia
tsutsugamushi. Ann N Y Acad Sci 2003;990:25-35.
7. Strickman D, Tanskul P, Eamsila C, Kelly DJ. Prevalence of antibodies to rickettsiae in the human population
of suburban Bangkok. Am J Trop Med Hyg 1994;5:149- 53.
8. Suputtamongkol Y, Suttinont C, Niwatayakul K, Hoontrakul S, Limpaiboon R, Chierakul W, et al. Epidemiology
and clinical aspects of rickettsioses in Thailand. Ann N Y Acad Sci 2009;1166:172- 9.
9. Suputtamongkol Y, Niwattayakul K, Suttinont C, Losuwanaluk K, Limpaiboon R, Chierakul W, et al. An open,
randomized, controlled trial of penicillin, doxycycline, and cefotaxime for patients with severe leptospirosis. Clin
Infect Dis 2004;39:1417-24.
10. Thap LC, Suparanond W, Treeprasertsook S, et al. Septic shock secondary to scrub typhus: characteristics
and complications. Southeast Asian Trop Med Public Health 2002;33:780- 6.
328.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 301
44
Molecular Epidemiology of Scrub Typhus in Thailand
Patimaporn Wongprompitak
Department of Immunology, .aculty of Medicine Siriraj Hospital, Mahidol University,
Scrub typhus is widely distributed in Asia Pacific region. This disease is caused by
Orientia tsutsugamushi infection. O. tsutsugamushi is an obligatory intracellular Gram-negative
bacteria. The pathogenesis of scrub typhus in humans is various, depending on the geographic
area because of an infection with the different strain of O. tsutsugamushi. The geographic
distribution study of the existing strains of O. tsutsugamushi will be beneficial for the epidemiology
and control of this disease. Several strains of O. tsutsugamushi have been reported in different
countries. The Gilliam, Karp, Kato, TA678, TA686, TA716, and TA763 strains have been
identified in South-East Asia and Australia by indirect immunofluorescence (I.) using polyclonal
and monoclonal antibodies. The Karp and Gilliam strains were the most prevalent in China,
Korea and Thailand. (1)
Molecular identification of scrub typhus in Thailand
Genetic analysis of the antigenic protein encoding gene of O. tsutsugamushi, the 56-
kDa protein, 22?kDa protein and the 47?kDa protein, were used for genotypic identification.(1)
The molecular methods including PCR, restriction fragment-length polymorphism (R.LP), and
nucleotide sequencing of specific PCR products were used for direct comparison of products
from the same genes of O. tsutsugamushi. The previous study, a nested PCR based on the
56?kDa protein encoding gene and DNA sequencing of a 487 base pair PCR product were
performed to identify O. tsutsugamushi isolated from scrub typhus patients.(2) DNA from 62
seropositive patients with scrub typhus were extracted. Karp was reported to be the most
prevalent in Thailand with 97% (60/62) of positive samples, followed by Kato (3%; 2/62). Recently,
the entire OR. of the 56-kDa protein encoding gene of each isolates were characterized by
nucleotide sequencing, followed by phylogenetic analysis. (3) The majority isolates in Thailand
was Karp strain (65.2%), then Gilliam (26.1%), TA763 (4.3%) and others (4.3%).
329.
302 Molecular Epidemiology of Scrub Typhus in Thailand
Identification of O. tsutsugamushi in scrub typhus patients
O. tsutsugamushi infection can be identified by serological tests but patient sera often
cross-react with the antigens from different strains. Recently, nested polymerase chain reaction
(PCR) was used for the identification of scrub typhus strains using gene encoding the specific
56-kDa protein of O. tsutsugamushi. In this study, genotypic identification of O. tsutsugamushi
in Thailand was investigated by genetic analysis using nucleotide sequencing and phylogenetic
analysis. The samples from patient with febrile illness were collected and selected for O.
tsutsugamushi infection using PCR amplification of specific 16S rRNA gene. The 56-kDa protein
encoding gene of these samples was amplified and analyzed for nucleotide sequences. The
nucleotide sequences of hypervariable region (VDI-IV) in this gene were compared with the
reference strains in Genbank database and phylogenetic tree was constructed (figure 1). There
were 4 major groups which related to O. tsutsugamushi strains (Karp, Gilliam, TA763 and
Kato). The most prevalent strain of O. tsutsugamushi in Thailand was Karp (43.8%; 28/64),
followed by Gilliam (34.4%; 22/64), TA763 (12.5%; 8/64) and Kato (4.7%; 3/64).
Application in the future
The result of this study might be useful for developing the method for strain identification.
The nucleotide sequences alignment of hypervarible region in 56 KDa encoding gene will be
performed and strain specific primers will be selected for strain identification using nested PCR
amplification. The information of molecular epidemiology of scrub typhus could be also useful
for prevention and controlling of the disease in Thailand.
References
1. Kelly DJ, .uerst PA, Ching WM, Richards AL. Scrub typhus: the geographic distribution of phenotypic and
genotypic variants of Orientia tsutsugamushi. Clin Infect Dis 2009;48:S203-30.
2. Blacksell SD, Luksameetanasan R, Kalambaheti T, Aukkanit N, Paris DH, McGready R, et al. Genetic typing
of the 56-kDa type-specific antigen gene of contemporary Orientia tsutsugamushi isolates causing human scrub
typhus at two sites in north-eastern and western Thailand. .EMS Immunol Med Microbiol 2008;52:335-42.
3. Manosroi J, Chutipongvivate S, Auwanit W, Manosroi A. Determination and geographic distribution of Orientia
tsutsugamushi serotypes in Thailand by nested polymerase chain reaction. Diagn Microbiol Infect Dis 2006;55:185-
90.
330.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 303
.igure 1 Dendrogram representing the genetic relationships of samples from scrub
typhus patients (represented in G alphabet followed by number (Gxx)) and
reference O. tsutsugamushi strains based on the nucleotide sequence of the
56-kDa protein encoding gene demonstrating the relationships between O.
tsutsugamushi strains.
332.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 305
45
Recent Advances in the Diagnosis of Scrub Typhus
Wei-Mei Ching
Viral and Rickettsial Diseases Naval Medical Research Center
Diagnosis of scrub typhus is generally based on the clinical presentation and the history
of a patient. However, differentiating scrub typhus from other acute tropical febrile illnesses
such as leptospirosis, murine typhus, malaria, dengue fever, and viral hemorrhagic fevers can
be difficult because of the similarities in these signs and symptoms. Besides the isolation of
the causative agent Orientia from patient blood as the confirmatory test, many modern
technologies have been applied in the development of diagnostic assays. Recent advances in
the diagnosis of scrub typhus are briefly described below, with emphasis on the activities
carried out in my laboratory.
Immuno-detection
The early serological assays include Weil-Felix test (1916), indirect immunofluorescent
antibody test (IFA, 1963), indirect immunoperoxidase (IIP, 1982), passive hemagglutination
assay (1993), dipstick dot –blot assay (1995) and ELISA (1997). Almost all of the assays use
whole cell grown in egg yolk sac or tissue culture as the antigen. Due to the intracellular nature
of Orientia and the hazardous procedures which require biosafety level 3 (BSL3) facilities and
practices for large scale production, not many diagnostic laboratories have the ability to culture
and purify O. tsutsugamushi. It was not until 1993, Kim et. el.1 developed the first recombinant
antigen of the outer membrane protein, the 56 kDa antigen, which comprises 10-15% of the total
bacterial protein. This protein is an ideal antigen to be used in sero-diagnosis because sera from
95–99% of patients with scrub typhus recognize this variable 56 kDa antigen of O. tsutsugamushi.
The availability of recombinant Orientia protein antigens that can be produced and
purified in large amounts and have similar antigenic properties as Orientia-derived antigens has
opened up a new avenue to develop low cost rapid assays. However, O. tsutsugamushi exhibits
considerable antigenic strain variation and the antigenic differences depend largely on the outer
membrane protein, that varies in size from 53 to 63 kDa. In order to develop a more broadly
333.
306 Recent Advances in the Diagnosis of Scrub Typhus
reactive diagnostic reagent, we produced t truncated recombinant protein of the 56 kDa antigen
(r56) from three prototype strains (Karp, Gilliam, and Kato). The combination of these three r56
(Tri-r56) in ELISA performed as well as the combination of whole cell antigens from the same
strains in IFA. Table 1 shows Tri- r56 in ELISA has the same sensitivity as IFA for IgM detection.
The results for IgG are also in very good agreement (data not shown).
Table 1 Combination of r56 from three strains in ELISA can detect IgM as early as IFA
The collaborative efforts of AccessBio and the DoD Laboratory at the Naval Medical
Research Center culminated in the development of a CareStartTM Scrub Typhus Combo Test
Device.This device was evaluated at the DoD Laboratorywith sera collected in Taiwan (Table 2)
and sera collected in the tropical environment of the Lao People’s Democratic Republic (Laos)
and Thailand (Table 3). Both evaluations have suggested that this test kit is sensitive (>90%)
and specific (>90%) for early diagnosis (IgM detection) as compared to IFA. On the basis of
data from stored patient samples, the AccessBio scrub typhus IgM rapid assay appears to
provide accurate results for the diagnosis of acute scrub typhus in a tropical setting where
scrub typhus is endemic.2 The ease of use and low cost of test kit have enhanced its
commercial applicability in the mostly underdeveloped endemic countries
Table 2 The performance of CareStartTM Scrub Typhus Combo Test Device (using the
mixture of recombinant antigen r56 from three proto type strains) as compared to current gold
standard IFA using whole cell lyaste (mixture of three proto type strains).
334.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 307
Table 2A DoD laboratory evaluation of CareStartTM Scrub Typhus Combo for IgM detection.
Comparison between the results of IgM of CareStartTM Scrub Typhus Combo and IFA IgM
Specificity Specificity % Sensitivity Sensitivity % Agreement %
Site 1: Access Bio 93/94 98.9% 18/19 94.7% 98.2%
Site 2: NMRC 91/112 81.3% 93/98 94.9% 87.6%
Total 184/206 89.3% 111/117 94.9% 91.3%
Table 2B DoD laboratory evaluation of CareStartTM Scrub Typhus Combo for IgG
detection
Comparison between the results of total antibody of CareStartTM Scrub Typhus Combo and IFA total antibody
Specificity Specificity % Sensitivity Sensitivity % Agreement %
Site 1: Access Bio 92/94 97.9% 19/19 100% 98.2%
Site 2: NMRC 38/40 95% 117/120 97.5% 96.9%
Total 130/134 97% 136/139 97.7% 97.8%
Table 3 Overall diagnostic accuracy and sensitivity of the AccessBio scrub typhus
Combo for detection of IgM and total antibodies compared to the results of the
gold standard assay, IFA
Antibody Sensitivity Specificity PPV NPV
IgM 96.8 (92.0–99.1) 93.3 (86.7–97.3) 94.5 (89.1–97.8) 96.1 (90.3–98.9)
Total antibody 97.6 (93.1–99.5) 71.4 (61.8–79.8) 80.3 (73.0–86.3) 96.2 (89.2–99.2)
To encompass a broader spectrum of antigenic variations, we have produced the r56
from strain TA763, chigger isolate Lc-1, and four chimeric r56s based on the sequences of Karp
and TA763 in the variable regions. Three of these chimeric r56s (C1, C2, and C3) were as
reactive as either Karpr56 or TA763r56 against 14 strain specific sera from infected mice3,
suggesting that the chimeric r56 exibited broader reactivity as compared to their parent r56,
either from Karp or TA763.
Nucleic acid detection
The value of serological assays for diagnosis of acute infection inclinical settings has
its limitations. This is because the earliest detection of antibodies is at least 4-5 days after the
onset of illness. In addition, there are high background titers in endemic populations. Therefore
335.
308 Recent Advances in the Diagnosis of Scrub Typhus
antigen detection is important for early diagnosis. However, the amount of Orientia in scrub
typhus patients during bacteremia is very low (5-10 organisms/ul). The immuno-capture assay is
not sensitive enough without an additional step for sample concentration. With the advent of
polymerase chain reaction (PCR), Furuya et al. first demonstrated that amplification of the 56-
kDa protein gene was a reliable method for early diagnosis (1991). Later on, PCR, nested PCR,
and quantitative PCR against different target genes such as 16S RNA, 60 kDa GroEL heat
shock protein and 47 kDa HtrA1 gene were developed. The use of nucleic acid amplification
has provided sufficient sensitivity. However, this approach requires sample processing (DNA
extraction), sophisticated instrumentation, expensive temperature sensitive reagents, and
extensive training of the end user. Its application is suitable for hospital centers with high
complexity laboratories, but not for rudimentary point-of-care centers such as doctors offices in
endemic rural areas. Another potential disadvantage is that false positives due to DNA
contamination are often observed.
Recently, Paris et al. described a new nucleic acid based assay using LAMP (loop-
mediated isothermal amplification) for the detection of Orientia (2008)(4). LAMP assay is quick,
easy to perform without the need of a thermal cycler for amplification. The Bst DNA polymerase
used in LAMP provides an additional advantage due to its insensitivity to blood borne components
including myoglobin, heme-blood protein complexes and immunoglobin, which inhibit the Taq
polymerase used in PCR. Thus much simpler sample preparation and reaction conditions are
required for LAMP compared to conventional PCR or real-time, quantitative PCR. Primers against
the Orientia specific region of groEL gene were designed using the Primer Explorer software of
Eiken (http://primerexplorer.jp/e/). The LAMP assay was carried out in a single tube 65C for 90
min for DNAs extracted from cultured Orientia, or Orientia infected buffy coat and whole blood
of confirmed scrub typhus patient. The detection limits were about 5 to 10 fold less than that of
qPCR. The results were in 100% agreement with those of the gold standard IFA. Therefore
LAMP assay has a very high potential to be used in rural areas.
We have sequenced the 47 kDa antigen gene from 25 disparate strains previously
selected to cover the wide range of strain variation. The 25 strains included six proto type
strains, all but one of human origin and were isolated from different locations throughout the
Asia-Pacific-Australia endemic region. LAMP primers against the conserved region of 47kDa
gene were designed. The assay has been performed isothermally at 60?C for 60 or 90 minutes.
The detection limit is consistently around 200 copies/ 25uL reaction with occasional detection
of as few as 10 copies/25uL reaction. The sensitivity of this LAMP assay was similar to that of
real-time PCR experiments using the same primers and to that of the LAMP assay using GroEL
336.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 309
gene as the target. So far this LAMP assay has been shown to detect at least 6 immunologically
and biologically disparate strains (Karp, Kato, Gilliam, TA763, TH11811, and TH1812) which
cover the major clades of prevalent strains of Orientia with similar sensitivity.(5)
Host response gene profile: the next generation diagnosis tool
It has been hypothesized that (1) a unique set of early response genes for a specific
rickettsial pathogen can be defined in vitro by using the high-throughput cDNA microarray
technology. (2) The expression profile of these unique sets of genes can be detected in patient
blood cells. (3) The characterization of these unique genes can be used to differentiate rickettsial
infections as well as infections caused by other agents. The proof of this hypothesis will
undoubtedly lead to the development of diagnostic kits using cDNA microarrays containing
genes that change significantly in their expression level in response to infection. Furthermore,
the cDNA microarray technology could be used as a true multiplex diagnostic platform to
differentiate various infections. The application of this approach for early diagnosis is remarkable.
It can detect the infection of a particular pathogen long before the onset of symptoms, and
much earlier than the current method of nucleic acid based real-time PCR and antigen based
serology tests. Unlike the host responses monitored by microarray technology, antigen detection
assays require adequate amounts of bacterial DNA or antigen; achieved only through infection
for a few days or more, for optimal detection. Moreover, antibody detection assays usually
requires 5-10 days for the host to develop a significant enough immune response to detect
specific IgM and IgG antibodies. Gene profile signatures related to the time course of impending
illness can be especially helpful for physicians to treat patients properly.
337.
310 Recent Advances in the Diagnosis of Scrub Typhus
As Orientia is an obligate intracellular pathogen, organisms disseminate from the skin
to target organs strongly suggest that they may enter the peripheral circulation. Walsh et al.
presented the evidence that Orientia was present in circulating white blood cells (mostly
mononuclear cells) of humans with acute scrub typhus (2001)(5). For determination of host
response genes that play a role in infection, we performed the in vitro study described below.
Freshly isolated peripheral blood mononuclear cells (PBMC) from healthy donors were
infected with Orientia and samples were collected at 1 h, 4 h, 8 h or 18 h post infection. The
gene expression profiles were monitored by cDNA microarray. Among the 7489 genes 658
genes were up or down regulated upon infection. Semi-quantitative PCR using specific primers
that flank the mRNA splicing sites of these 658 genes were carried out to verify microarray
results using glyceraldehyde 3-phosphate dehydrogenase (GAPDH) as the reference gene. Among
these 658 genes, 22 genes were confirmed to beup or down regulated (Table 4). Quantitative
PCR using 18S rRNA as the reference further confirmed two genes (NM_001547 and NM_006187)
exhibited significant increase of expression Analysis of these 22 genes and the specific increase
of both NM_001547 and NM_006187 suggest the list of 22 genes appears to be unique for O.
tsutsugamushi infection and has the potential for use in differentiating infections caused by
viruses, bacteria, parasites and other pathogens.(6)
Table 4. List of genes confirmed by semi-quantitative PCR
Accessionnumber Name of Genes Biological processes
NM_000530 myelin protein zero (Charcot-Marie-Tooth neuropathy 1B) (MPZ), Signal transduction
NM_000595 lymphotoxin alpha (TNF superfamily, member 1) (LTA), Signal transduction
NM_000801 FK506 binding protein 1A, 12kDa (FKBP1A), transcript variant 12B Signal transduction
NM_001547 interferon-induced protein with tetratricopeptide repeats 2 (IFIT2), Cell growth and/or maintenance
NM_001838 chemokine (C-C motif) receptor 7 (CCR7), Signal transduction
NM_002498 NIMA (never in mitosis gene a)-related kinase 3 (NEK3), transcript variant 1, Signal transduction
NM_002922 regulator of G-protein signalling 1 (RGS1), Signal transduction
NM_002946 replication protein A2, 32kDa (RPA2), Nucleotide and nucleic acid
metabolism
NM_002983 chemokine (C-C motif) ligand 3 (CCL3), Immune response
NM_003205 transcription factor 12 (HTF4, helix-loop-helix transcription Nucleotide and nucleic acid
factors 4) (TCF12), transcript variant 3 metabolism
NM_003404 tyrosine 3-monooxygenase/tryptophan 5-monooxygenase Signal transduction
activation protein, beta polypeptide (YWHAB), transcript variant 1
NM_003906 MCM3 minichromosome maintenance deficient 3 (S. cerevisiae) Signal transduction
associated protein (MCM3AP),
338.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 311
Accessionnumber Name of Genes Biological processes
NM_004551 NADH dehydrogenase (ubiquinone) Fe-S protein 3, 30kDa Metabolism, Energy pathways
(NADH-coenzyme Q reductase) (NDUFS3),
NM_005082 tripartite motif-containing 25 (TRIM25), Nucleotide and nucleic acid
metabolism
NM_005623 chemokine (C-C motif) ligand 8 (CCL8), Signal transduction
NM_006187 2'-5'-oligoadenylate synthetase 3, 100kDa (OAS3), Immune response
NM_007215 polymerase (DNA directed), gamma 2, accessory subunit Nucleotide and nucleic acid
(POLG2), metabolism
NM_015369 TP53TG3 protein (TP53TG3), transcript variant 1 Regulation of cell cycle
NM_021991 junction plakoglobin (JUP), transcript variant 2 Cell adhesion
NM_033340 caspase 7, apoptosis-related cysteine peptidase (CASP7), Apoptosis
transcript variant beta
NM_080657 radical S-adenosyl methionine domain containing 2 (RSAD2), Immune response
NM_152998 enhancer of zeste homolog 2 (Drosophila) (EZH2), transcript Nucleotide and nucleic acid
variant 2 metabolism
Bolded genes are down-regulated
In summary, recent advances in the diagnosis of scrub typhus are exciting. Significant
progress has has already been made in rapid serological test and nucleic acid based molecular
detection. The establishment of host responsive gene profile specific to Orientia infection may
provide the opportunity for early diagnosis at the onset of illness.
References
1. Kim IS, Seong SY, Woo SG, Choi MS, and Chang WH. High-level expression of a 56-kilodalton protein gene
(bor56) of Rickettsia tsutsugamushi Boryong and its application to enzyme-linked immunosorbent assays. J.
Clin Microbiol 1993;1:598-605.
2. Blacksell SD, Jenjaroen K, Phetsouvanh R, Wuthiekanun V, Day NP, Newton PN, Ching WM. Accuracy of
AccessBio Immunoglobulin M and Total Antibody Rapid Immunochromatographic Assays for the Diagnosis of
Acute Scrub Typhus Infection. Clin Vaccine Immunol 2010;17:263-6.
3. Chao CC, Zhang Z, Huber E, and Ching WM. Cross reactivity of various 56 kDa recombinant protein
antigens with sera from Orientia tsutsugamushi infected mice. 5th International Conference on Rickettsiae and
Rickettsial Diseases, May 18-20, 2008, Marseille, France.
4. Paris DH, Blacksell SD, Newton PN, and Day NPJ. Simple, rapid and sensitive detection of Orientia tsutsugamushi
by loop-isothermal DNA amplification. Trans R Soc Trop Med Hyg 2008;102:1239-46.
339.
312 Recent Advances in the Diagnosis of Scrub Typhus
5. Chao CC, Huber E, Chen HW, and Ching WM. Detection of Orientia tsutsugamushi DNA using loop-mediated
isothermal amplification: a rapid and sensitive alternative to real-time PCR, 24th Meeting of the American
Society for Rickettsiology, July 31 – Aug 3, 2010, Skamania Lodge, Stevenson, Washington, USA.
6. Chao CC, Li X, Hammamieh R, O’Leary B, Jett M and Ching WM. Identification of human peripheral
leukocyte early response genes following infection with Orientia tsutsugamushi by DNA microarray and real-
time PCR. Accepted by Chao CC The Open Infectious Diseases Journal, 2010.
340.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 313
46
Iron Chelation : New Hope
´Í¡àµÍê®Ò ¾ÔÈÒž§È
ʶҺѹÇÔ¨ÂáÅоѲ¹Ò ͧ¤¡ÒÃàÀÊѪ¡ÃÃÁ
Ñ
ͧ¤¡ÒÃàÀÊѪ¡ÃÃÁ䴌ǨÂÂҢѺàËÅ硪¹Ô´ÃѺ»Ãзҹ·ÕÁªÍÊÒÁÑÇ‹Ò deferiprone ËÃ×Í L1
ÔÑ è Õ ×è
áÅÐÁժ͡ÒäŒÒÇ‹Ò GPO-L-ONE Í‹ҧ¤ÃºÇ§¨ÃµÑ§áµ‹¡ÒÃÊѧà¤ÃÒÐËǵ¶Ø´º¨¹¶Ö§à»š¹ÂÒàÁç´à¤Å×ͺ
×è é Ñ Ô
ÃÇÁ¶Ö§ÁÕ¡ÒÃÇԨ´ŒÒ¹»ÃÐÊÔ·¸ÔÀÒ¾áÅФÇÒÁ»ÅÍ´ÀÑ¢ͧÂÒ à¾×Íãˌ䴌ÂÒ·ÕÁ¤³ÀÒ¾áÅÐÃÒ¤Ò¶Ù¡
Ñ è è Õ Ø
ãËŒ¼»Ç¸ÒÅÑÊ«ÕàÁÕ«֧à´ÔÁäÁ‹ÊÒÁÒöࢌҶ֧ÂÒ ä´ŒãªŒÂÒÍ‹ҧ·ÑǶ֧ ÂÒ GPO-L-ONE ÁÕ¤³ÀÒ¾
ÙŒ † è è Ø
»ÃÐÊÔ·¸ÔÀÒ¾ áÅФÇÒÁ»ÅÍ´ÀÑÂà·‹Òà·ÕÂÁ¡ÑºÂÒµŒ¹áºº ᵋÃÒ¤ÒÂÒ¶Ù¡¡Ç‹ÒÂÒµŒ¹áººÁÒ¡
¢Ñ¹µÍ¹¡ÒÃÇÔ¨ÂáÅмÅÔµÂÒ GPO-L-ONE
é Ñ
¡ÒÃÇԨѡÒÃÊѧà¤ÃÒÐËÇѵ¶Ø´Ôº ¾Ñ²¹ÒÇÔ¸¡ÒÃÊѧà¤ÃÒÐË¢¹ãËŒàËÁÒÐÊÁµ‹Í¡ÒüÅÔµã¹
Õ Öé
ÃдѺÍصÊÒË¡ÃÃÁ â´Â䴌ǵ¶Ø´º L1 ·ÕÁ¤ÇÒÁºÃÔÊ·¸Ôì
Ñ Ô è Õ Ø
¡ÒþѲ¹ÒÊÙµÃÂÒàÁç´ ¹íÒÇѵ¶Ø´º L1 ·Õʧà¤ÃÒÐËä´ŒÁÒ㪌àµÃÕÂÁ໚¹ÂÒàÁç´à¤Å×ͺ
Ô èÑ
¡Ò÷´Êͺ¤ÇÒÁ¤§µÑÇ ¹íÒÇѵ¶Ø´ºáÅÐÂÒàÁç´·ÕàµÃÕÂÁ䴌价´Êͺ¤ÇÒÁ¤§µÑǷѧÊÀÒ¾
Ô è é
»¡µÔ áÅзÕÊÀÒ¾à˧ à¾×Í¡íÒ˹´ÍÒÂآͧÇѵ¶Ø´ºáÅÐÂÒÊíÒàÃç¨ÃÙ»
è è Ô
àǪÈÒʵ÷¹Âؤ 2553
Ñ 321
5. Nisbet-Brown E, Olivieri N., Giardina PJ, et al. Effectiveness and safety of ICL670 in iron-loaded patients with
thalassaemia: a randomised, double-blind, placebo-controlled, dose-escalation trial. Lancet. 2003;361:1597-602.
6. Galanello R, Piga A, Cappellini MD, et al. Effect of food, type of food, and time of food intake on deferasirox
bioavailability: recommendations for an optimal deferasirox administration regimen. J Clin Pharmacol. 2008;48:
428-35.
7. Waldmeier ., Bruin GJ, Glaenzel U, et al. Pharmacokinetics, metabolism, and disposition of deferasirox in beta-
thalassemic patients with transfusion-dependent iron overload who are at pharmacokinetic steady state. Drug
Metab Dispos. 2010;38:808-16.
8. Cappellini MD, Cohen A, Piga A, et al. A phase 3 study of deferasirox (ICL670), a once-daily oral iron chelator,
in patients with beta-thalassemia. Blood. 2006;107:3455-62.
9. Vichinsky E, Onyekwere O, Porter J, et al. A randomised comparison of deferasirox versus deferoxamine for
the treatment of transfusional iron overload in sickle cell disease. Br J Haematol. 2007;136:501-8.
10. Porter J, Galanello R, Saglio G, et al. Relative response of patients with myelodysplastic syndromes and other
transfusion-dependent anaemias to deferasirox (ICL670): a 1-yr prospective study. Eur J Haematol. 2008;80:
168-76.
11. Taher A, El-Beshlawy A, Elalfy MS, et al. Efficacy and safety of deferasirox, an oral iron chelator, in heavily iron-
overloaded patients with beta-thalassaemia: the ESCALATOR study. Eur J Haematol. 2009;82:458-65.
12. Taher A, Cappellini MD, Vichinsky E, et al. Efficacy and safety of deferasirox doses of >30 mg/kg per d in
patients with transfusion-dependent anaemia and iron overload. Br J Haematol. 2009;147:752-9.
13. Cappellini MD, Porter J, El-Beshlawy A, et al. Tailoring iron chelation by iron intake and serum ferritin: the
prospective EPIC study of deferasirox in 1744 patients with transfusion-dependent anemias. Haematologica.
2010;95:557-66.
14. Esposito BP, Breuer W, Sirankapracha P, Pootrakul P, Hershko C, Cabantchik ZI. Labile plasma iron in iron
overload: redox activity and susceptibility to chelation. Blood. 2003;102:2670–7.
15. Porter JB. Pathophysiology of iron overload. Hematol Oncol Clin North Am. 2005;19 (suppl 1):7-12.
16. Daar S, Pathare A, Nick H, et al. Reduction in labile plasma iron during treatment with deferasirox, a once-daily
oral iron chelator, in heavily iron-overloaded patients with beta-thalassaemia. Eur J Haematol. 2009;82:454-7.
17. Porter JB, Cappellini MD, El-Beshlawy A, et al. Effect of deferasirox on labile plasma iron levels in heavily iron-
overloaded patients with transfusion-dependent anemias enrolled in the large-scale, prospective 1-year EPIC
trial (abstract). Blood112. 2008;112:5411.
18. Masera N, Rescaldani C, Azzolini M, et al. Development of lens opacities with peculiar characteristics in
patients affected by thalassemia major on chelating treatment with deferasirox (ICL670) at the Pediatric Clinic
in Monza, Italy. Haematologica. 2008;93:e9-10.
19. Delea TE, Sofrygin O, Thomas SK, Baladi J., Phatak PD, Coates TD. Cost effectiveness of once-daily oral
chelation therapy with deferasirox versus infusional deferoxamine in transfusion-dependent thalassaemia patients:
US healthcare system perspective. Pharmacoeconomics. 2007;25:329-42.
20. Karnon J, Tolley K, Oyee J, Jewitt K, Ossa D, Akehurst R. Cost-utility analysis of deferasirox compared to
standard therapy with desferrioxamine for patients requiring iron chelation therapy in the United Kingdom. Curr
Med Res Opin. 2008;24:1609-21.
350.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 323
48
ÂÒ¨Ò¡ÊÁعä¾Ã¡ÑºàǪÈÒʵÃàªÔ§»ÃШѡÉ
Herbal Medicinal Products and Evidence-based Medicine
ÍÒ¨ÒààÀÊѪ¡ÃËÔ§³Ñª¡Ã ÅéíÒàÅÔÈ¡Ô¨
ÃͧÈÒʵÃÒ¨Òà¹ÒÂᾷ»ÃÐÇÔ·Â ÍѤÃàÊÃÕ¹¹·
ÍÒ¨Òà»ÃÐʾ¾Ã ¾Ñ¹¸à¾ç§
ÃͧÈÒʵÃÒ¨Òà¹ÒÂᾷ·ÇÕ àÅÒ˾ѹ¸
ʶҹ¡ÒÃá¾·Âá¼¹ä·Â»ÃÐÂØ¡µ ¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
㹪‹Ç§ 20 »‚·¼Ò¹ÁÒ á¹Ç¤Ô´àÃ×ͧàǪÈÒʵÃàªÔ§»ÃШѡÉä´Œ·ÒãËŒº¤Åҡ÷ҧ¡ÒÃá¾·Â
Õè ‹ è í Ø
ÁÕ¤ÇÒÁµ×¹µÑÇ㹡ÒÃËÒ¢ŒÍÁÙÅËÅÑ¡°Ò¹àªÔ§»ÃШѡɷ´·Ê´ÁÒ»ÃÐÂØ¡µãªŒã¹àǪ»¯ÔºµÔ à¾×ÍãËŒ¡ÒôÙáÅ
è Õè Õ Õè Ø Ñ è
ÃÑ¡ÉÒ¼Ù»ÇÂÁÕ»ÃÐÊÔ·¸Ô¼ÅáÅлÅÍ´ÀÑÂÁÒ¡·ÕÊ´ ¡ÒôÙáÅÃÑ¡ÉÒ´ŒÇÂÈÒʵáÒÃá¾·Âá¼¹ä·Â«Ö§à»š¹
Œ † èØ è
ͧ¤¤ÇÒÁÃÙŒ·ÕèÊ׺·Í´¡Ñ¹ÁÒÂÒǹҹ¡çä´ŒÃѺÍÔ·¸Ô¾Å¨Ò¡á¹Ç¤Ô´¹Õéઋ¹¡Ñ¹ ¨Ö§à¡Ô´¤ÇÒÁµ×è¹µÑÇàÃ×èͧ
¡ÒÃ㪌ÂÒ¨Ò¡ÊÁعä¾Ãº¹ËÅÑ¡°Ò¹ÇÔªÒ¡Òà ¢³Ðà´ÕÂǡѹ¡ÃÐáÊ¡ÒÃ㪌¼ÅÔµÀѳ±¨Ò¡ÊÁعä¾Ã·ÑÇâÅ¡ è
¡çà¾ÔÁÁÒ¡¢Ö¹Í‹ҧµ‹Íà¹×ͧ ÁÕÁŤ‹Ò»‚ÅÐËÅÒ¾ѹŌҹ´ÍÅÅÒÃÊËÃÑ°(1) äÁ‹ÇÒ¨Ð㪌໚¹ÂÒÃÑ¡ÉÒâä
è é è Ù ‹
ÍÒËÒÃàÊÃÔÁÊØ¢ÀÒ¾ à¤Ã×ͧÊíÒÍÒ§ ËÃ×ÍÍÒËÒÃ
è
ÊÒà˵ط·Òãˌʧ¤ÁËѹÁÒºÃÔâÀ¤¼ÅÔµÀѳ±¨Ò¡ÊÁعä¾Ã¡Ñ¹ÁÒ¡¢Ö¹ ʋǹ˹֧à¾ÃÒÐࢌÒã¨Ç‹Ò
Õè í Ñ é è
¼ÅÔµÀѳ±·ÕèÁÒ¨Ò¡¸ÃÃÁªÒµÔäÁ‹ÁÕÍѹµÃÒ áÅÐÍաʋǹ˹Öè§à¾ÃÒÐÍÔ·¸Ô¾Å¢Í§Ê×èÍ»ÃÐàÀ·µ‹Ò§æ
·Õè¹íÒàʹ͢ŒÍÁÙÅà¡ÕèÂǡѺ»ÃÐÊÔ·¸Ô¼Å¢Í§¼ÅÔµÀѳ±¨Ò¡ÊÁعä¾Ã ·Ñ駷ҧâ·Ã·Ñȹ ˹ѧÊ×;ÔÁ¾
ÍÔ¹àµÍÃà¹ç· ËÃ×ÍẺ»Ò¡µ‹Í»Ò¡ ᵋÊÍàËÅ‹Ò¹ÕºÒ§¤Ãѧ¡çäÁ‹ÊÒÁÒöãËŒ¢ÍÁÙŷդú¶ŒÇ¹ä´Œ à¹×ͧ¨Ò¡
×è é é Œ è è
ÊÁعä¾ÃʋǹÁÒ¡ÂѧäÁ‹ÁËÅÑ¡°Ò¹·Ò§ÇÔªÒ¡Ò÷ÕÁÒʹѺʹع»ÃÐÊÔ·¸ÔÀÒ¾áÅФÇÒÁ»ÅÍ´ÀÑ ¶Ö§áÁŒ
Õ è
ÊÁعä¾ÃºÒ§ª¹Ô´¨ÐÁÕ¡ÒÃÈÖ¡ÉÒÇԨ¡çµÒÁ ᵋËÅÑ¡°Ò¹·ÕÁ¤ÇÒÁ¹‹Òàª×Ͷ×Íã¹ÃдѺÊÙ§Áըҹǹ¹ŒÍÂ
Ñ è Õ è í
ÊÁعä¾Ãä·Â·Õ¾ºº‹ÍµÒÁàÇçºä«µµÒ§æ 䴌ᡋ ¢ÁÔ¹ªÑ¹ ¿‡Ò·ÐÅÒÂâ¨Ã ÁÐÃØÁ ¡ÃЪÒ´íÒ
è ‹ é
Ç‹Ò¹ªÑ¡Á´ÅÙ¡ ¾ÃÔ¡ä·Â´íÒ ºÍÃÐà¾ç´ ྪÃÊѧ¦Òµ ËŒÒ˹ǴáÁÇ ªØÁàËç´à·È ÃÒ§¨×´ ´Í¡¤íÒ½ÍÂ
µíÒÃѺÂÒµ‹Ò§æ ઋ¹ ÂÒËÍÁ ÂÒºÃÃà·ÒÃÔ´Êմǧ·ÇÒà ÂÒá¡ŒäÍ à»š¹µŒ¹ ʋǹÁÒ¡¨íÒ˹‹ÒÂã¹ÃٻẺ
ÂÒàÁç´ ÂÒ᤻«ÙÅ ÂÒÅÙ¡¡Å͹ ËÃ×ÍÂÒª§ ¹Í¡¨Ò¡¹ÕéÂѧÁÕ·Õè໚¹ÂÒ㪌ÀÒ¹͡ ÍÒËÒÃàÊÃÔÁ áÅÐ
à¤Ã×ͧÊíÒÍÒ§
è
àǪÈÒʵ÷¹Âؤ 2553
Ñ 325
µÒÃÒ§·Õè 2 ÃдѺ¢Í§¤íÒá¹Ð¹íÒ (Grades of recommendation)(3)
ÃдѺ ࡳ±¡ÒûÃÐàÁÔ¹
A ËÅÑ¡°Ò¹ÃдѺ 1 ·ÕÊÍ´¤ÅŒÍ§¡Ñ¹
è
B ËÅÑ¡°Ò¹ÃдѺ 2 ËÃ×Í 3 ·ÕÊÍ´¤ÅŒÍ§¡Ñ¹ ËÃ×Í ÃÒ§ҹà¾ÔÁàµÔÁ¨Ò¡ËÅÑ¡°Ò¹ÃдѺ 1
è è
C ËÅÑ¡°Ò¹ÃдѺ 4 ËÃ×Í ÃÒ§ҹà¾ÔÁàµÔÁ¨Ò¡ËÅÑ¡°Ò¹ÃдѺ 2 ËÃ×Í 3
è
D ËÅÑ¡°Ò¹ÃдѺ 5 ËÃ×Í ËÅÑ¡°Ò¹ÃдѺÍ×¹·ÕÁ¤ÇÒÁ¤ÅØÁà¤Ã×ÍËÃ×͢ѴáÂŒ§¡Ñ¹
è è Õ
¶ŒÒ¡ÒõѴÊÔ¹ã¨ãËŒ¡ÒÃÃÑ¡ÉÒ¼ÙŒ»†Ç µÑé§ÍÂÙ‹º¹ËÅÑ¡¡ÒâͧàǪÈÒʵÃàªÔ§»ÃШѡɫÖè§àª×èͶ×Í
ã¹ËÅÑ¡°Ò¹·Õè໚¹ RCT ¤íÒ¶ÒÁ¤×ÍÂÒÊÁعä¾Ã¨ÐÊÒÁÒö¹íÒÁÒ㪌㹡ÒÃÃÑ¡ÉÒä´ŒËÃ×ÍäÁ‹ à¾ÃÒÐ
ËÅÑ¡°Ò¹·Õà¡ÕÂÇ¢ŒÍ§¡ÑºÂÒ¨Ò¡ÊÁعä¾ÃáÅÐÊÁعä¾Ãä·ÂʋǹÁҡ໚¹ÃдѺ 5 ¤×Í à»š¹¢ŒÍÁÙŨҡ¡ÒÃ
è è
·´Åͧã¹ËÅÍ´·´Åͧ ÊѵǷ´Åͧ ºÑ¹·Ö¡¨Ò¡µíÒÃÒËÃ×ͤÑÁÀÕõ‹Ò§æ·Õè໚¹ÀÙÁÔ»˜Ò ໚¹µŒ¹
ʋǹ¢ŒÍÁÙÅ¡ÒÃÇԨѷҧ¤ÅÔ¹Ô¡·Õ蹋Òàª×èͶ×Í¡çÁÑ¡¨Ð໚¹ÊÁعä¾Ãà´ÕèÂÇ·ÕèÁÕ¡ÒÃ㪌¡Ñ¹ÁÒ¡ËÃ×ÍÁÕ¡ÒÃ㪌
ã¹·ÇÕ » ÍàÁÃÔ ¡ ÒËÃ× Í ÂØ â û ઋ ¹ ¿‡ Ò ·ÐÅÒÂâ¨ÃáÅТÁÔé ¹ ªÑ ¹ «Öè § ໚ ¹ ÊÁØ ¹ ä¾Ã¨í Ò ¹Ç¹¹Œ Í ÂÁÒ¡
àÁ×èÍà·Õº¡Ñº¨íҹǹÊÁعä¾Ã·ÕèÁÕ¡ÒÃ㪌ÍÂÙ‹¨ÃÔ§ã¹àǪ»¯ÔºÑµÔ«Öè§ÁÕÁÒ¡¡Ç‹Ò 500 ª¹Ô´ µÒÁ¢ŒÍÁÙŨҡ
ʶҹ¡ÒÃá¾·Âá¼¹ä·Â»ÃÐÂØ¡µ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ÔÔ
Í‹ҧäáç´ã¹ÃÐÂÐËÅѧ ºØ¤Åҡ÷շҧҹ´ŒÒ¹ÊÁعä¾Ãä´Œ¾ÂÒÂÒÁ·íÒ¡ÒÃÇԨ¶֧»ÃÐÊÔ·¸Ô¼Å
Õ è í Ñ
áÅФÇÒÁ»ÅÍ´ÀÑ à¾×ÍãËŒ¡ÒÃ㪌ÂÒ¨Ò¡ÊÁعä¾Ã໚¹ä»Í‹ҧÊÁà˵ØÊÁ¼Å ઋ¹ ¡ÒÃËÒÊÒÃÊíÒ¤Ñ
è
¡Ò÷´Êͺķ¸Ô·Ò§àÀÊѪÇÔ·ÂҤǺ¤Ù仡Ѻ¡Ò÷´Åͧ·Ò§¤ÅÔ¹¡ ໚¹µŒ¹
ì ‹ Ô
µÑÇÍ‹ҧ¡ÒÃÇÔà¤ÃÒÐËËÅÑ¡°Ò¹àªÔ§»ÃШѡɢͧÂÒ¨Ò¡ÊÁعä¾Ã
1. ¢ÁÔ鹪ѹ
ÁÕªÍÇÔ·ÂÒÈÒʵÃÇÒ Curcuma longa L. Ç§È Zingiberaceae ¤ÑÁÀÕÃÊÃþ¤Ø³ÂÒ(4) «Ö§ãªŒ
×è ‹ è
͌ҧÍԧ㹷ҧ¡ÒÃá¾·Âá¼¹ä·ÂÃкØÇÒ¢ÁÔ¹ªÑ¹ÁÕÊÃþ¤Ø³ “ᡌ䢌͹ºÑ§à¡Ô´áµ‹´Õ ªíÒÃÐâäÍѹºÑ§à¡Ô´
‹ é Ñ
µÒÁ¼ÔÇ˹ѧ ÃЧѺàµâª¸ÒµØãËŒ´º á¡ŒàÊÁËзíÒãËŒ¿¡ºÇÁ áÅá¡ŒºÒ´á¼Å” áÅеÑÇÍ‹ҧµíÒÃѺÂÒ·ÕÁÕ
Ñ è
¢ÁÔ¹ªÑ¹à»š¹Ê‹Ç¹»ÃСͺ áÅÐÃкØÊÃþ¤Ø³äÇŒ ઋ¹ “¨Ñ¹·¹à·È ¢Ñ³±Ê¡Ã ËÑÇáËŒÇËÁÙ â¡°¡Ãд١ Ç‹Ò¹
é
¹éÒ ¢ÁÔ¹ªÑ¹ ਵÁÙÅà¾ÅÔ§ µíÒáÂà¤Ã×Í ¢Ô§Ê´ ÍѹNjÒÂÒËÁÙ¹¡ÃзíÒãËŒ¿¡ºÇÁÂغŧ” ËÃ×Í “¤Ø³¢ÁÔ¹ªÑ¹
í é ‹ Õé é
¢ÁԹ͌Í ÁÕÃÊà¼ç´ÃŒÍ¹ á¡Œ¾ÉâÅËÔµ áÅÅÁ á¡ŒºÇÁ á¡ŒàÊÁËРᡌ䢌·§»Ç§ á¡ŒµÇ¾ÂÒ¸Ô¡ÃзíÒãËŒ¤¹
é Ô Ñé Ñ Ñ
·ÑÇÊÃþҧ¤ á¡Œ½”
è ‚
»˜¨¨Øº¹¢ÁÔ¹ªÑ¹¨Ñ´à»š¹ÂÒ¨Ò¡ÊÁعä¾Ã㹺ѪÕÂÒ¨Ò¡ÊÁعä¾ÃáË‹§ªÒµÔ ¾.È. 2549 Áբͺ‹§ãªŒ
Ñ é Œ
㹡ÒúÃÃà·ÒÍÒ¡ÒÃṋ¹¨Ø¡àÊÕ´ ¹Í¡¨Ò¡¹Õ§¾ºÇ‹ÒÁÕ¡ÒÃ͌ҧÊÃþ¤Ø³µŒÒ¹¡ÒÃÍÑ¡àʺ µŒÒ¹ÁÐàÃç§
(5)
é Ñ
áÅеŒÒ¹Í¹ØÁÙÅ ÍÔÊÃдŒÇ ÃдѺ¢Í§ËÅÑ¡°Ò¹àªÔ§»ÃШѡÉáÅÐÃдѺ¢Í§¤íÒá¹Ð¹íÒÊíÒËÃѺ¢ÁÔ鹪ѹ
áÊ´§änj㹵ÒÃÒ§·Õè 3
353.
326 ÂÒ¨Ò¡ÊÁعä¾Ã¡ÑºàǪÈÒʵÃàªÔ§»ÃШѡÉ
µÒÃÒ§·Õè 3 ËÅÑ¡°Ò¹àªÔ§»ÃШѡɢͧ¢ÁÔ鹪ѹ
¢ŒÍº‹§ãªŒ ÃдѺ¢Í§ ÃдѺ¢Í§
ËÅÑ¡°Ò¹ ¤íÒá¹Ð¹íÒ
ÃÑ¡ÉÒÍÒ¡ÒÃṋ¹¨Ø¡àÊÕ´(5) 2 B
Å´¡ÒÃÍÑ¡àʺ(5-8)
- ¡Ãд١¢ŒÍÍÑ¡àʺàÃ×ÍÃѧ ¡ÒÃÍÑ¡àʺ¢Í§á¼ÅËÅѧ¼‹ÒµÑ´
é
àÂ×ͺصÒÍÑ¡àʺàÃ×ÍÃѧ
è é 2, 4, 5 B
»‡Í§¡Ñ¹áÅÐÃÑ¡ÉÒá¼Åã¹·Ò§à´Ô¹ÍÒËÒÃ(5, 6, 8) 2, 5 D*
µŒÒ¹àª×ÍẤ·ÕàÃÕÂ(5)
é 5 D*
µŒÒ¹ÍÑÅä«àÁÍÃ(8) 5 D
¢Ñº¹éÒ´Õ Å´¡ÒúպµÑǢͧÅíÒäÊŒ(5)
í 5 D
µŒÒ¹ÁÐàÃç§(6, 8) µŒÒ¹Í¹ØÁÅÍÔÊÃÐ(6, 9)
Ù 5 D
µŒÒ¹¡ÒÃà¡ÒСÅØÁ¢Í§à¡Åç´àÅ×Í´(6)
‹ 5 D
ËÁÒÂà赯 * ËÅÑ¡°Ò¹ÁÕ¤ÇÒÁ¢Ñ´áÂŒ§¡Ñ¹
áÁŒ¨ÐÁÕ§Ò¹ÇÔ¨ÂÁÒ¡ÁÒ·ÕʹѺʹع»ÃÐ⪹¢Í§¢ÁÔ¹ªÑ¹ã¹´ŒÒ¹µ‹Ò§æ ᵋ¡¾ºÇ‹ÒÁբ͢ѴáÂŒ§
Ñ è é ç Œ
¡Ñ¹ÍÂÙºÒ§ ઋ¹ Ä·¸Ô㹡ÒÃÂѺÂѧàª×Í Helicobacter pyroli «Ö§à»š¹µŒ¹à˵آͧ¡ÒÃà¡Ô´á¼Å㹡ÃÐà¾ÒÐ
‹ Œ ì é é è
ÍÒËÒÃ(5) Ä·¸Ô㹡ÒÃÃÑ¡ÉÒá¼Å㹡ÃÐà¾ÒÐÍÒËÒ÷ÕÁ§Ò¹ÇԨ·ҧ¤ÅÔ¹¡ËÅÒªԹ ઋ¹ ÍѪÅÕáÅФ³Ð
ì è Õ Ñ Ô é
(2529) Prucksunand áÅФ³Ð (1986 áÅÐ 2001) ¾ºÇ‹Ò¢ÁÔ鹪ѹÁÕ»ÃÐÊÔ·¸Ô¼Å㹡ÒÃÃÑ¡ÉÒá¼Å
㹡ÃÐà¾ÒÐÍÒËÒÃ(8) ᵋ Van Dau áÅФ³Ð (1998) ÃÒ§ҹNjҢÁÔ¹ªÑ¹äÁ‹Á»ÃÐÊÔ·¸Ô¼ÅàÁ×Íà·Õº¡Ñº
é Õ è
ÂÒËÅÍ¡ ´Ñ§¹Ñ¹¨Ò¡ËÅÑ¡°Ò¹àªÔ§»ÃШѡɷÁÍÂÙ·ÒãËŒàª×ÍÁѹ䴌ÇÒ¢ÁÔ¹ªÑ¹ÊÒÁÒö㪌áÉÒÍÒ¡ÒÃṋ¹
(6)
é Õè Õ ‹ í è è ‹ é Ñ
¨Ø¡àÊÕ´䴌 ʋǹķ¸ÔµÒ¹¡ÒÃÍÑ¡àʺ áÁŒ¨ÐÁÕËÅÑ¡°Ò¹ÁÒʹѺʹع ᵋÃдѺ¢Í§¤íÒá¹Ð¹íÒÍÂÙã¹ÃдѺ
ì Œ ‹
B à¹×ͧ¨Ò¡¾ºÇ‹Ò§Ò¹ÇÔ¨ÂÁÕ¢¹Ò´¢Í§µÑÇÍ‹ҧ¹ŒÍ ¨Ö§ÂѧµŒÍ§¡ÒÃÈÖ¡ÉÒà¾ÔÁàµÔÁµ‹Íä»
è Ñ è
2. ¿‡Ò·ÐÅÒÂâ¨Ã
ÁÕª×èÍÇÔ·ÂÒÈÒʵÃÇ‹Ò Andrographis paniculata (Burm.f.) Wall. Ex. Nees ÍÂÙ‹ã¹Ç§È
Acanthaceae ÊÁعä¾Ãª¹Ô´¹ÕÁ¡ÒÃ㪌Áҹҹ㹻ÃÐÇѵÈÒʵáÒÃá¾·Âá¼¹¨Õ¹ ¡ÒÃá¾·ÂÍÒÂØÃàÇ·
é Õ Ô
ÍÔ¹à´Õ ÃÇÁ·Ñ§¡ÒÃá¾·Âá¼¹ä·Â â´Â㪌ÃÊ¢Á¢Í§ÂÒ㹡ÒÃÃÑ¡ÉÒ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ÃкºÂ‹ÍÂÍÒËÒÃ
é
áÅÐŴ䢌 »˜¨¨ØºÑ¹¿‡Ò·ÐÅÒÂâ¨Ã໚¹ÊÁعä¾Ã·ÕèÁÕ¡ÒÃ㪌Í‹ҧÁÒ¡ã¹»ÃÐà·ÈᶺÊ᡹´Ôà¹àÇÕÂ
㹡ÒÃÃÑ¡ÉÒ¡ÒõԴàª×Í·Ò§à´Ô¹ËÒÂã¨Ê‹Ç¹º¹áÅÐ䢌ËÇÑ´(10) ã¹»ÃÐà·Èä·Â¿‡Ò·ÐÅÒÂâ¨Ã໚¹ÊÁعä¾Ã
é
㹺ѪÕÂÒ¨Ò¡ÊÁعä¾ÃáË‹§ªÒµÔ ¾.È. 2549 Áբͺ‹§ãªŒã¹¡ÒúÃÃà·ÒÍÒ¡Ò÷ŒÍ§àÊÕÂäÁ‹µ´àª×Í ºÃÃà·Ò
Œ Ô é
ÍÒ¡ÒÃà¨çº¤Í ºÃÃà·ÒÍÒ¡ÒâͧâäËÇÑ´ ઋ¹ à¨çº¤Í ͋͹à¾ÅÕ »Ç´àÁ×Í¡ŌÒÁà¹×Í ¹éÒÁÙ¡äËÅ
è é í
໚¹µŒ¹(5) ã¹»‚ ¾.È. 2552 ª‹Ç§·ÕÁ¡ÒÃá¾Ã‹ÃкҴ¢Í§âä䢌ËÇÑ´ãË‹ 2009 ÁÕ¤Òá¹Ð¹íÒãˌú»Ãзҹ
è Õ í Ñ
354.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 327
ÊÁعä¾ÃµÑǹÕ(11) ÃдѺ¢Í§ËÅÑ¡°Ò¹àªÔ§»ÃШѡÉáÅÐÃдѺ¢Í§¤íÒá¹Ð¹íÒÊíÒËÃѺ¿‡Ò·ÐÅÒÂâ¨ÃáÊ´§äÇŒ
é
ã¹µÒÃÒ§·Õè 4
µÒÃÒ§·Õè 4 ËÅÑ¡°Ò¹àªÔ§»ÃШѡɢͧ¿‡Ò·ÐÅÒÂâ¨Ã
¢ŒÍº‹§ãªŒ ÃдѺ¢Í§ ÃдѺ¢Í§
ËÅÑ¡°Ò¹ ¤íÒá¹Ð¹íÒ
ºÃÃà·ÒÍÒ¡ÒâͧâäËÇÑ´ ઋ¹ à¨çº¤Í ͋͹à¾ÅÕÂ
»Ç´àÁ×Í¡ŌÒÁà¹×Í ¹éÒÁÙ¡äËÅ(8, 12)
è é í 1, 2 A
ºÃÃà·ÒÍÒ¡Ò÷ŒÍ§àÊÕÂäÁ‹µ´àª×Í(5, 8)
Ô é 2, 5 B
ºÃÃà·ÒÍÒ¡ÒÃà¨çº¤Í (5)
2 B
»‡Í§¡Ñ¹ËÇÑ´(8) 2 B
ºÃÃà·ÒÍÒ¡Ò÷ŒÍ§àÊÕµԴàª×Í(5, 8) é 2, 5 D*
Ä·¸ÔºÂѧàª×ÍẤ·ÕàÃÕÂ
ì Ñ é é (5, 8)
2, 5 D*
Ä·¸Ô͹æ·ÕÁ¡ÒÃÈÖ¡ÉÒ ä´Œá¡‹ Ä·¸ÔµÒ¹àª×ÍäÇÃÑÊ(8)
ì ×è è Õ ì Œ é
Å´¡ÒÃÍÑ¡àʺ Ŵ䢌 ¡ÃеعÃкºÀÙÁ¤Á¡Ñ¹(5, 8)
(5, 8) (5, 8)
Œ Ô ØŒ 5 D
ËÁÒÂà赯 * ËÅÑ¡°Ò¹ÁÕ¤ÇÒÁ¢Ñ´áÂŒ§¡Ñ¹
¨Ò¡ËÅÑ¡°Ò¹·Õʺ¤Œ¹ä´Œ ÃдѺ¢Í§¤íÒá¹Ð¹íÒãˌ㪌¿Ò·ÐÅÒÂâ¨ÃºÃÃà·ÒÍÒ¡ÒâͧâäËÇÑ´
è × ‡
à¨çº¤Í áÅзŒÍ§àÊÕÂäÁ‹µ´àª×ÍÁÕ¤ÒÊÙ§¤×Í A ʋǹ¡ÒÃÃÑ¡ÉÒÍÒ¡Ò÷ŒÍ§àÊÕµԴàª×Í ¶Ö§áÁŒ¨ÐÁÕ§Ò¹ÇÔ¨Â
Ô é ‹ é Ñ
·Ò§¤ÅÔ¹Ô¡ÃÒ§ҹ»ÃÐÊÔ·¸Ô¼Å´ŒÒ¹¹Õé ᵋ§Ò¹ÇÔ¨ÑÂËÅÒªÔé¹ÃкØÇ‹Ò¿‡Ò·ÐÅÒÂâ¨ÃäÁ‹ÁÕ¼Å㹡ÒõŒÒ¹
àª×ÍẤ·ÕàÃÕ ÃдѺ¢Í§¤íÒá¹Ð¹íÒÊíÒËÃѺ¢ŒÍº‹§ãªŒ¹¨§à·‹Ò¡Ñº D ¹Í¡¨Ò¡¹ÕÁÃÒ§ҹNjҿ‡Ò·ÐÅÒÂâ¨Ã
é Õé Ö é Õ
ÍÒ¨·íÒãËŒà¡Ô´ anaphylactic shock ä´Œ¶ŒÒÃѺ»Ãзҹ㹢¹Ò´ÊÙ§(5, 12) ÍÒ¨·íÒãˌᢹ¢ÒªÒËÃ×Í
͋͹áçàÁ×èÍ㪌µÔ´µ‹Í¡Ñ¹¹Ò¹(5) ¨Ö§¤ÇÃÃÐÁÑ´ÃÐÇѧ㹡ÒÃ㪌 áÅÐäÁ‹¤ÇÃ㪌ã¹ÊµÃÕÁÕ¤ÃÃÀà¹×èͧ¨Ò¡
ÁÕÃÒÂ§Ò¹Ç‹Ò ·íÒãËŒà¡Ô´¡ÒÃá·Œ§(5)
3. ÁÐÃØÁ
ÁÕªÍÇÔ·ÂÒÈÒʵÃÇÒ Moringa oleifera Lamarack ÍÂÙã¹Ç§È Moringaceae µÒÁÀÙÁ»Ò
×è ‹ ‹ Ô ˜
´Ñ§à´ÔÁ¢Í§ä·Â ¹Í¡¨Ò¡ãªŒÁÐÃØÁ໚¹ÍÒËÒÃáÅŒÇ ÂѧÊÒÁÒö㪌à¡×ͺ·Ø¡Ê‹Ç¹¢Í§µŒ¹ÁÐÃØÁ໚¹ÂÒä´Œ
é
à»Å×Í¡µŒ¹ÁÕÃÊÌ͹ ÃѺ»Ãзҹ໚¹ÂҢѺÅÁã¹ÊíÒäÊŒ ·íÒãËŒ¼ÒÂËÃ×ÍàÃÍ ¤ØÁ¸ÒµØ͋͹æ(13) ¤ÑÁÀÕÃ
ÊÃþ¤Ø³ÂÒ(4) ÃкØÇ‹ÒãºÁÐÃØÁÁÕÊÃþ¤Ø³ãªŒà»š¹¹éíÒ¡ÃÐÊÒÂÂÒ áÅеÑÇÍ‹ҧµíÒÃѺÂÒ·ÕèÁÕÁÐÃØÁ໚¹
ʋǹ»ÃСͺÃкØÊÃþ¤Ø³´Ñ§¹Õé “¤Ø³ãºá¤·Ñé§ ò ãºÊÁÕ ãºªØÁàËç´ ãºÁÐÃØÁ 㺾ÃÔ¡ä·Â ãºÁÐÃÐ
ãºÁÐä¿ ãºäÁŒ·§ ø ÊÔ§¹Õé á¡Œ¹Í¹ÁÔËÅѺãËŒÃÐÊèÒÃÐÊÒ ãËŒàÍÒãºäÁŒ¹Õé ᡧ¡Ô¹¡Ñº¢ŒÒÇ à¨ÃÔâÅËÔµ
Ñé è í
¹Í¹ËÅѺáÅ ãºäÁŒÍ¹¡Å‹ÒÇÁÒᵋ¡Í¹¹Ñ¹ ãºÍ‹Í¹¡Ô¹à¡Ô´â·É”
Ñ ‹ é
355.
328 ÂÒ¨Ò¡ÊÁعä¾Ã¡ÑºàǪÈÒʵÃàªÔ§»ÃШѡÉ
»˜¨¨Øº¹ÁÐÃØÁ໚¹ÊÁعä¾Ã·ÕÁ¡ÒÃ͌ҧÊÃþ¤Ø³ÁÒ¡ÁÒ ઋ¹ ÃÑ¡ÉÒâä¢Ò´ÊÒÃÍÒËÒà âä
Ñ è Õ
µÒà¡×ͺ·Ø¡ª¹Ô´ âäàºÒËÇÒ¹ âä¤ÇÒÁ´Ñ¹âÅËÔµÊÙ§ âä¡Ãд١ âäÁÐàÃç§ âäàÍ´Ê àÊÃÔÁÊÌҧÀÙÁÔ
¤ØÁ¡Ñ¹ âäÅíÒäʌ͡àʺ âäÀÙÁᾌáÅÐÃÑ¡ÉÒá¼ÅàÃ×ÍÃѧ(14) ÃÇÁ件֧¡ÒÃ͌ҧNjÒÊÒÁÒö¹íÒÁÒ㪌¡º
Œ Ñ Ô é Ñ
âäËÇÑ´ 2009
ËÅÑ¡°Ò¹·ÕÃкØà¡ÕÂǡѺ»ÃÐ⪹¢Í§ÁÐÃØÁÁÕÁÒ¡ÁÒ·ѧËÅÑ¡°Ò¹àªÔ§ÇÔ·ÂÒÈÒʵÃáÅзÕ໚¹
è è é è
ºÑ¹·Ö¡µ‹Ò§æ Jed W .ahey (2005) ä´ŒÃǺÃÇÁ¢ŒÍÁÙÅËÅÑ¡°Ò¹µ‹Ò§æà¡ÕÂǡѺÁÐÃØÁäÇŒ ´Ñ§¹Õé ´ŒÒ¹ÊÒÃ
è
ÍÒËÒà ãºÁÐÃØÁÁÕÇÔµÒÁÔ¹àÍ á¤Åà«ÕÂÁ ¸ÒµØàËÅç¡ ÇÔµÒÁÔ¹«Õ áÅÐâ¾á·Êà«ÕÂÁÊÙ§ ¡ÒÃÈÖ¡ÉÒ´ŒÒ¹
¾Ä¡Éà¤ÁÕ (Phytochemical) ¾ºÇ‹Ò¾×ªã¹µÃСÙÅ Moringa ÁÕÊÒþǡ¹éÒµÒÅàªÔ§à´ÕÂÇáÅÐÊÒûÃСͺ
í è
glucosinolates áÅÐ isothiocyanates ã¹»ÃÔÁÒ³ÁÒ¡ áÅÐÊÒÃà¤ÁÕËÅÒµÑÇ·Õ¾ºÁÕÃÒ§ҹNjÒÁÕÄ·¸Ôì
è
Å´¤ÇÒÁ´Ñ¹âÅËÔµ µŒÒ¹ÁÐàÃç§ µŒÒ¹àª×ÍẤ·ÕàÃÕ ÃдѺ¢Í§ËÅÑ¡°Ò¹àªÔ§»ÃШѡÉáÅÐÃдѺ¢Í§¤íÒá¹Ð
é
¹íÒÊíÒËÃѺÁÐÃØÁáÊ´§änj㹵ÒÃÒ§·Õè 5
µÒÃÒ§·Õè 5 ËÅÑ¡°Ò¹àªÔ§»ÃШѡɢͧÁÐÃØÁ
¢ŒÍº‹§ãªŒ ÃдѺ¢Í§ ÃдѺ¢Í§
ËÅÑ¡°Ò¹ ¤íÒá¹Ð¹íÒ
Ä·¸ÔÅ´ÃдѺ¹éÒµÒÅã¹àÅ×Í´(15, 16)
ì í 4, 5 D
âäÀÙÁÔᾌáÅÐÃÑ¡ÉÒá¼ÅàÃ×éÍÃѧ(14) 5 D
Ä·¸ÔµÒ¹àª×ÍẤ·ÕàÃÕ àª×ÍÃÒ àª×ÍäÇÃÑÊ ¾ÂÒ¸Ô
ì Œ é é é
ÂѺÂѧà«ÅÅÁÐàÃç§
é (17)
5 D
»‡Í§¡Ñ¹¡ÒÃŴŧ¢Í§ÃдѺ¡ÅÙµÒä¸â͹(18) 5 D
Å´ÃдѺä¢ÁѹáÅÐà¾ÔÁÃдѺ HDLã¹àÅ×Í´(19)
è 5 D
ÂѺÂѧ¡ÒÃà¡Ô´ÍÍ¡«ÔപѹáÅÐÊÒÁÒö¨ÑºÍ¹ØÁÅÍÔÊÃÐä´Œ(20)
é Ù 5 D
¨ÐàËç¹ä´ŒÇÒáÁŒ¨ÐÁÕ¡ÒÃÈÖ¡ÉÒÇÔ¨ÂÄ·¸Ô¢Í§ÁÐÃØÁã¹´ŒÒ¹µ‹Ò§æÁÒ¡ÁÒ ᵋÊǹÁҡ໚¹¡ÒÃ
‹ Ñ ì ‹
·´ÅͧẺ in vitro áÅÐ in vivo ʋǹ¡ÒÃÈÖ¡ÉÒ·Ò§¤ÅÔ¹Ô¡·Õè·íÒ¡çäÁ‹ãª‹ÃٻẺ Randomized,
double-blind, placebo-controlled trials ¨Ö§·íÒãËŒÃдѺ¢Í§¤íÒá¹Ð¹íÒÍÂÙã¹ÃдѺµèÒ ÁÕà¾Õ§¡ÒÃÈÖ¡ÉÒ
‹ í
¹íÒËͧâ´Â Anthanont P áÅФ³Ð (2553) ·Õ·Ò¡ÒÃÈÖ¡ÉҼŢͧãºÁÐÃØÁµ‹ÍÃдѺ¹éÒµÒÅã¹àÅ×Í´áÅÐ
è í í
¡ÒÃËÅÑè§ÍÔ¹«ÙÅÔ¹ã¹ÍÒÊÒÊÁѤÃÊØ¢ÀÒ¾´Õ 10 ÃÒ «Ö觾ºÇ‹Ò¡ÒÃÃѺ»ÃзҹãºÁÐÃØÁã¹¢¹Ò´ÊÙ§ÁÕ¼Å
µ‹Í¡ÒÃà¾ÔèÁ¡ÒÃËÅÑè§ÍÔ¹«ÙÅԹ䴌 Í‹ҧäáç´Õ ¤ÇÃÁÕ¡ÒÃÈÖ¡ÉÒà¾ÔèÁàµÔÁ¶Ö§»ÃÐÊÔ·¸Ô¼Å¢Í§ãºÁÐÃØÁ
µ‹Í¡ÒùíÒÁÒ㪌㹼ٻÇÂàºÒËÇÒ¹ª¹Ô´·Õè 2 µ‹Íä»
Œ †
336 ËÅÑ¡¡ÒÃÊíҤѢͧ¡ÒÃá¾·Âá¼¹ä·Â
á¹Ç¤Ô´àÃ×èͧ¸ÒµØ : ¤ÇÒÁÊÑÁ¾Ñ¹¸¢Í§Á¹ØÉ¡ѺÊÔè§áÇ´ÅŒÍÁ âÅ¡ áÅÐ
¨Ñ¡ÃÇÒÅ
¡ÒÃá¾·Âá¼¹ä·ÂÁÕÁÁÁͧµ‹ÍÊÃþÊԧNjÒÁÕ¤ÇÒÁàª×ÍÁâ§ÊÑÁ¾Ñ¹¸¡¹ Í‹ҧ໚¹à˵Ø໚¹¼Å
Ø è è Ñ
áÅÐ໚¹Í§¤ÃÇÁ á¹Ç¤Ô´àÃ×ͧ¸ÒµØ໚¹¾×¹°Ò¹ÊíÒ¤Ñ㹡ÒÃÈÖ¡ÉÒ¡ÒÃá¾·Âá¼¹ä·Â Á¹ØɨÐÁÕ¤ÇÒÁ
è é
ÊآʺÒÂä´Œ¶ÒÁÕ¤ÇÒÁÃÙ¤ÇÒÁࢌÒã¨àÃ×ͧ¸ÒµØáÅÐÁÕ¤ÇÒÁÊÑÁ¾Ñ¹¸·¶¡µŒÍ§¡ÑºÊÔ§µ‹Ò§æ·ÕÍÂÙÃͺµÑÇ
Œ Œ è Õè Ù è è ‹
¡ÒÃá¾·Âá¼¹ä·Âàª×ÍÇ‹ÒËҧ¡ÒÂÁ¹ØÉ»ÃСͺ¢Ö¹¨Ò¡¸ÒµØ·Ñé§ 4 ËÃ×Í ÁËÒÀÙµÃÙ» 4 ¤×Í
è é
¸ÒµØ´Ô¹ ¸ÒµØ¹éíÒ ¸ÒµØÅÁ áÅÐ ¸ÒµØä¿ ¤ÑÁÀÕÃÇÊ·¸ÔÁÃä¡Å‹ÒÇÇ‹Ò (5) ÔØ
“ÍѹÊÃÕáÒÂáË‹§àÃÒ·‹Ò¹·Ñ§ËÅÒ ¨Ð»ÃÒ¡¯Ç‹Ò¹ŒÍÂÇ‹ÒãË‹ Ç‹ÒµèÒÇ‹Ò¡ÃдŒÒ§ Ç‹ÒÁѹNjҷ¹¹Ñ¹
é í è é
ÍÒÈÑÂá¡‹»°ÇÕ¸ÒµØ ·Õ¨Ð໚¹¹éÒ໚¹àÂ×Í»Åѧà¤Ã‹§¤ÃÑ´ªØÁÁѹ¹Ñ¹ÍÒÈÑÂá¡‹ÍÒâ»¸ÒµØ ÍÒ⻸ҵع¹µÑ§ÍÂÙã¹
è í è è ‹ é Ñé é ‹
»°ÇÕ¸ÒµØ ä´Œ»°ÇÕ¸ÒµØ໚¹·Õµ§ ä´Œàµâª¸ÒµØ໚¹¼ÙÍÀÔºÒÅÃÑ¡ÉÒ ä´ŒÇÒâ¸ҵØ໚¹¼ÙÍ»¶ÑÁÀ ¨Ö§µÑ§ÍÂÙä´Œ
è Ñé Œ ŒØ é ‹
໚¹Íѹ´Õ ÁÔä´ŒÃÇÁÔä´ŒäËÅÍÍ¡ ¡ÃзíÒÊÃÕáÒ»ÃÐà·È¹Ñ¹ ãËŒÍÁÍÂÙàµçÁ໚¹Íѹ´ÕÁä´Œº¡ÁÔä´Œ¾Ã‹Í§”
Ñè é Ôè ‹ Ô
¸ÒµØ´Ô¹ ËÃ×Í »°ÇÕ¸ÒµØ ä´Œá¡‹ ÍÇÑÂÇТͧËҧ¡Ò »ÃСͺ´ŒÇ ¼Á ¢¹ àÅçº ¿˜¹ ¼ÔÇ˹ѧ
ÊÁͧ ¡ÅŒÒÁà¹×Í àÍç¹ ¡Ãд١ 䢡Ãд١ ËÑÇ㨠ÁŒÒÁ µÑº ¾Ñ§¼×´ äµ »Í´ ÅíÒäÊŒ ÍÒËÒ÷Õà¾Ô§
é è è
‹ÍÂãËÁ‹æ ÍÒËÒ÷մ´«ÖÁáÅŒÇ ÃÇÁ·Ñ§¢Í§àÊÕ è Ù é
¸ÒµØ¹éíÒ ËÃ×Í ÍÒâ»¸ÒµØ ä´Œá¡‹ ¢Í§àËÅǵ‹Ò§æ áÅÐÊÒá֧¢Í§á¢ç§ã¹Ã‹Ò§¡Ò »ÃСͺ è
´ŒÇÂàÅ×Í´ ´Õ àÊÁËР˹ͧ à˧×Í Áѹ ä¢Áѹ ¹éÒµÒ ¹éÒÅÒ ¹éÒ㹨ÁÙ¡ »˜ÊÊÒÇÐáÅйéÒ䢢ŒÍ
è í í í í
¸ÒµØÅÁ ËÃ×Í ÇÒâÂ¸ÒµØ ä´Œá¡‹ ¾Åѧ§Ò¹·Õ¤Çº¤ØÁ¡ÒÃà¤Å×͹äËǢͧËҧ¡Ò »ÃСͺ´ŒÇ è è
ÅÁ¾Ñ´àº×ͧº¹ ÅÁ¾Ñ´àº×ͧŋҧ ÅÁã¹·ŒÍ§ ÅÁã¹ÅíÒäÊŒ ÅÁ¾Ñ´·ÑÇËҧ¡Ò áÅÐÅÁËÒÂã¨
é é è
¸ÒµØä¿ ËÃ×Í àµâª¸ÒµØ 䴌ᡋ ¾Åѧ¤ÇÒÁÌ͹áË‹§ªÕǵ·Õ·ÒãËŒÃÒ§¡ÒÂͺÍع ¤ÇÒÁÌ͹ Ô è í ‹ ‹
áÅСÒÃà¼ÒäËÁŒ »ÃСͺ´ŒÇÂä¿ÍعËҧ¡Ò 俷շÒãËŒà¡Ô´¤ÇÒÁÇÔµ¡ ä¿·Õ·Òãˌᡋ áÅÐ
‹ è í è í
ä¿Â‹ÍÂÍÒËÒÃ
Á¹ØÉÂᵋÅФ¹¨ÐÁÕʋǹ»ÃСͺ¢Í§¸ÒµØ·Ñé§ 4 àËÁ×͹¡Ñ¹ ᵋÁÕÊѴʋǹ¢Í§¸ÒµØäÁ‹à·‹Ò¡Ñ¹
ÁÕ¸ÒµØã´¸ÒµØ˹֧໚¹ãË‹ àÃÕ¡NjҸҵØ਌ÒàÃ×͹ ᵋ¸ÒµØ਌ÒàÃ×͹«Ö§ÁÕÁҵѧᵋà¡Ô´ÁÕ¡ÒÃà»ÅÕ¹á»Å§
è è é è
ä´ŒµÒÁÍÔ·¸Ô¾Å¢Í§»˜¨¨Ñµ‹Ò§æ ઋ¹ ÍÒÂØ Ä´Ù¡ÒÅ ¡ÒÅàÇÅÒ ¶Ô¹·ÕÍÂÙ‹ áÅоĵԡÃÃÁ¢Í§¤¹æ ¹Ñ¹ è è é
â´Â»¡µÔÃÒ§¡Ò¨оÂÒÂÒÁ»ÃѺãËŒ¸ÒµØµÒ§æÍÂÙã¹ÀÒÇÐÊÁ´ØÅ ¶ŒÒ»ÃѺãËŒà¡Ô´ÀÒÇÐÊÁ´ØÅäÁ‹ä´ŒàÁ×Íã´
‹ ‹ ‹ è
¡ç¨Ðà¡Ô´âäËÃ×ͤÇÒÁà¨çº»†Ç¢ֹ é
ÊÔ§·ÕÍÂÙÃͺµÑÇÁ¹ØÉ¡»ÃСͺ¢Ö¹¨Ò¡¸ÒµØ·§ 4 ઋ¹¡Ñ¹ àÁ×ÍÁͧÊÔ§·ÕÍÂÙáÇ´ÅŒÍÁÃͺµÑÇ¡ç¨Ð
è è ‹ ç é Ñé è è è ‹
àË繸ҵصҧæ ઋ¹ 俨ҡ¡Í§¿„¹ ÅÁ·Õ¾´¼‹Ò¹ ¹éÒ·ÕÍÂÙ㹤Åͧ ºÖ§ áÅдԹ·ÕÍÂÙ㹼׹Ἃ¹´Ô¹ ÀÙà¢Ò
‹ è Ñ í è ‹ è ‹
ÅѡɳÐÀÙÁ»ÃÐà·È«Ö§à»š¹¶Ô¹·ÕÍÂ٢ͧÁ¹ØÉ¡Á¤ÇÒÁµ‹Ò§¡Ñ¹ à¹×ͧ¨Ò¡àª×ÍÇ‹Ò»ÃСͺ¢Ö¹¨Ò¡ÊѴʋǹ
Ô è è è ‹ ç Õ è è é
¢Í§¸ÒµØᵡµ‹Ò§¡Ñ¹ ໚¹·Õµ§áË‹§ÊÁد°Ò¹¢Í§â䵋ҧ¡Ñ¹ ઋ¹ ÀÙÁ»ÃÐà·È·Õ໚¹ÀÙà¢ÒÊÙ§ ¨Ñ´à»š¹
è Ñé Ô è
»ÃÐà·ÈÌ͹ ໚¹·Õµ§áË‹§ÊÁد°Ò¹¸ÒµØä¿ ÀÙÁ»ÃÐà·È·ÕáËŒ§áÅŒ§à»š¹¡ÃÇ´·ÃÒ ¨Ñ´à»š¹»ÃÐà·ÈͺÍع
è Ñé Ô è ‹
໚¹·ÕèµÑé§áË‹§ÊÁد°Ò¹¸ÒµØ¹éíÒ ÀÙÁÔ»ÃÐà·È·Õè໚¹ÅØ‹Á¹éíÒ ¨Ñ´à»š¹»ÃÐà·ÈàÂç¹ à»š¹·ÕèµÑé§áË‹§ÊÁد°Ò¹
¸ÒµØÅÁ ÀÙÁ»ÃÐà·È·Õµ´·ÐàÅ ¨Ñ´à»š¹»ÃÐà·È˹ÒÇ à»š¹·Õµ§áË‹§ÊÁد°Ò¹¸ÒµØ´¹(6)
Ô è Ô è Ñé Ô
344 ¡ÒÃÊ‹§àÊÃÔÁÊØ¢ÀÒ¾´ŒÇ¸ÃÃÁÒ¹ÒÁÑÂ
ÃÙ»·Õè 2 ¡ÒºÃÔËÒÃÃٻẺµ‹Ò§æ
¨ÔµµÒ¹ÒÁÑÂ
¤×Í ¡ÒôÙáÅãËŒà¡Ô´Í¹ÒÁÑ¢ͧ¨Ôµ Á¹ØÉ·¡¤¹ÁÕ¨µà»š¹¹ÒÂÁÕ¡ÒÂ໚¹º‹ÒÇ à¾ÃÒШԵ໚¹µÑÇ
Ø Ô
¡íÒ˹´ ¡íҡѺ ËÃ×ͤǺ¤ØÁ¾ÄµÔ¡ÃÃÁ¢Í§¡Ò ·Ñ§¡ÒþٴáÅСÒáÃзíÒ ´Ñ§¹Ñ¹ÊÔ§ÊíҤѷÕäÁ‹Â§Ë‹͹
é é è è Ôè
ËÃ×ÍÊíÒ¤ÑÂÔ§¡Ç‹Ò¡ÒþѲ¹Ò¡Ò ¡ç¤Í¡ÒÃÊ‹§àÊÃÔÁÊØ¢ÀÒ¾¨Ôµ ËÃ×Í¡ÒþѲ¹Ò͹ÒÁÑ¢ͧ¨ÔµãËŒÁ¨µ·Õè
è × ÕÔ
ÊÁºÙó ¾ÃоÃËÁ¤Ø³ÒÀó (».Í.»Âصâµ) ¡Å‹ÒÇÇ‹Ò ¨Ôµ·ÕÊÁºÙó»ÃСͺ´ŒÇÂÀÒÇÐ 3 »ÃСÒà ¤×Í
Ú è (5)
(1) ¤Ø³ÀÒ¾ 䴌ᡋ ¤Ø³¸ÃÃÁ ¤ÇÒÁàÁµµÒ¡ÃØ³Ò ¤ÇÒÁàÍ×Íà¿„Íà¼×ÍἋ ¤ÇÒÁ«×ÍÊѵ ໚¹µŒ¹
é œ è è
(2) ÊÁÃöÀÒ¾ 䴌ᡋ ¤ÇÒÁࢌÁá¢ç§Áѹ¤§ ¤ÇÒÁà¾ÕÂþÂÒÂÒÁ ¤ÇÒÁÁاÁѹ ʵÔáÅÐÊÁÒ¸Ô
è ‹ è
໚¹µŒ¹
(3) ÊØ¢ÀÒ¾ 䴌ᡋ ¤ÇÒÁÊØ¢ ¤ÇÒÁ»µÍÁ㨠¤ÇÒÁËÒàÃÔ§àºÔ¡ºÒ¹ã¨ ¤ÇÒÁ¼‹Í§ãÊ à»š¹µŒ¹
Ô Ôè
´Ñ§¹Ñ¹¨Ôµ¨ÐÊÁºÙó䴌µÍ§ä´ŒÃº¡ÒþѲ¹Ò·Ñ§ 3 ´ŒÒ¹ ¡ÒþѲ¹Ò¨ÔµãËŒÁ¤³ÀÒ¾ ËÁÒ¶֧
é Œ Ñ é Õ Ø
¡ÒÃàÃÕ¹ÃÙãˌࢌÒã¨áÅл¯Ôºµä´Œ¶¡µŒÍ§µÒÁËÅÑ¡¤Ø³¸ÃÃÁ ¡ÒþѲ¹ÒãËŒ¨µÁÕÊÁÃöÀÒ¾ ¨Ð·íÒãËŒ¨µ
Œ Ñ Ô Ù Ô Ô
ÁÕ¾×é¹°Ò¹·ÕèࢌÁá¢ç§ÁÑ蹤§ ¨ÐÍÂÙ‹¹Ôè§áÅеÑé§ÁÑè¹ä´Œ àÃÕ¡NjÒÁÕÊÁÒ¸Ô àÁ×èÍÁÕÊÁÒ¸Ô ¨Ôµ¡ç¨ÐÊÒÁÒö
¾Ô¨ÒÃ³Ò ÃѺÃÙŒ àÃÕ¹ÃÙŒ ÊÔ§µ‹Ò§æ ä´ŒµÒÁ¤ÇÒÁ໚¹¨ÃÔ§ ࢌÒ㨪ÕǵáÅÐÊÃþÊÔ§·Ñ§ËÅÒµÒÁ¨ÃÔ§«Ö§¡ç¤Í
è Ô è é è ×
»˜Ò áÅÐÂѧÃÙ෋ҷѹNjҤÇû¯ÔºµµÍÊÔ§µ‹Ò§æ Í‹ҧäè֧¨Ð¶Ù¡µŒÍ§àËÁÒÐÊÁ ¼Ù·¾²¹Ò¨Ôµ¨¹ÁÕ
Œ Ñ Ô ‹ è Œ Õè Ñ
¤Ø³ÊÁºÑµàª‹¹¹Õé ‹ÍÁ໚¹»ÃÐ⪹͋ҧÂÔ§µ‹Íµ¹àͧáÅÐÊѧ¤Á ·Ñ§¡Òû¯ÔºµË¹ŒÒ·Õ¡Òçҹ㹤ÇÒÁ
Ô è é Ñ Ô è
ÃѺ¼Ô´ªÍº ¡ÒôíÒà¹Ô¹ªÕǵ áÅСÒê‹ÇÂá¡Œ»ËÒáÅÐÊÌҧÊÃäʧ¤Á
Ô ˜ Ñ
372.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 345
ÃÙ»·Õè 3 ¾Ñ²¹Ò¨ÔµãËŒÁդسÀÒ¾
ÃÙ»·Õè 4 ¾Ñ²¹Ò¨ÔµãËŒÁÕÊÁÃöÀÒ¾
¾ÃоÃËÁ¤Ø³ÒÀó (».Í.»Âصâµ) ͸ԺÒÂÇ‹Ò ¨Ôµ·Õ䴌ú¡ÒþѲ¹Ò¨Ð໚¹¨Ôµ·ÕÁ¤³¸ÃÃÁ
Ú è Ñ è Õ Ø
«Ö§¨Ð¡íҡѺ¾ÄµÔ¡ÃÃÁãˌ໚¹ä»ã¹·Ò§·Õ´Õ ¶Ù¡µŒÍ§ àËÁÒÐÊÁ ᵋ¾ÄµÔ¡ÃÃÁ·Õ´ÍÒ¨äÁ‹Á¹¤§ ËÒ¡¢Ò´
è è è Õ Ñè
¹éíÒËÅ‹ÍàÅÕ駤س¸ÃÃÁ㹨Ե㨠«Ö觡ç¤×ͤÇÒÁÊØ¢ ´Ñ§¹Ñ鹨֧µŒÍ§¾Ñ²¹Ò¨ÔµãËŒÁÕÊØ¢ÀÒ¾´ŒÇ ËÁÒ¶֧
¡ÒÃàÃÕ¹ÃÙŒáÅÐࢌÒã¨àÃ×èͧ¤ÇÒÁÊØ¢«Öè§ËÁÒ¶֧¤ÇÒÁµŒÍ§¡Ò÷Õèä´ŒÃѺ¡Òõͺʹͧ áÅФÇÒÁÊØ¢
ÁÕËÅÒ¢ѹ (5)䴌ᡋ
é
¤ÇÒÁÊØ¢¢Ñé¹·Õè 1 ໚¹¤ÇÒÁÊØ¢·Õèà¡Ô´¨Ò¡¡ÒÃàʾÇѵ¶Ø ໚¹¤ÇÒÁÊØ¢·ÕµÍ§ËÒ µŒÍ§àÍÒ µŒÍ§
è Œ
䴌ǵ¶ØÁÒàʾ¨Ö§¨ÐÁÕ¤ÇÒÁÊØ¢ µŒÍ§¢Ç¹¢ÇÒÂËÒÁÒãˌ䴌¨§¨ÐÁÕ¤ÇÒÁÊØ¢ µŒÍ§ä´ŒµÍ§àʾ¨Ö§¨ÐÍÂÙä´Œ ¤×Í
Ñ Ö Œ ‹
äÁ‹ÁÕäÁ‹ä´Œ Á¹ØÉ·ÕèÁÕ¤ÇÒÁÊآẺ¹ÕéáÊ´§Ç‹Ò¢Ò´á¤Å¹¤ÇÒÁÊØ¢ à»ÃÕºàÊÁ×͹ÊÙàÊÕÂÍÔÊÃÀÒ¾
ËÒ¡Êѧ¤ÁÁÕᵋ¼¤¹·ÕËÒ¤ÇÒÁÊآẺ¹Õé ¡ç¨ÐµŒÍ§á‹§ªÔ§àºÕ´àºÕ¹¡Ñ¹ ÁÕ½ÒÂ˹֧䴌 ½†ÒÂ˹֧ʹËÃ×Í
ÙŒ è † è è
àÊÕ ¨Ö§à»š¹¤ÇÒÁÊØ¢·Õèà¡Ô´º¹¤ÇÒÁ·Ø¡¢¢Í§¼ÙŒÍ×è¹ ´Ñ§¹Ñé¹Á¹Øɨ֧µŒÍ§½ƒ¡µ¹àͧÍ‹ÒãËŒ¤ÇÒÁÊØ¢
µŒÍ§¢Ö¹¡ÑºÇѵ¶ØÁÒ¡ ½ƒ¡ãËŒ ÁÕ¡ç´Õ äÁ‹ÁÕ¡çä´Œ ¨¹¶Ö§¢Ñ¹ ÁÕ¡çä´Œ äÁ‹ÁÕ¡ç´Õ
é é
¤ÇÒÁÊØ¢¢Ñ¹·Õè 2 ໚¹¤ÇÒÁÊØ¢·Õà¡Ô´¨Ò¡¡ÒÃãËŒ´Ç¤ÇÒÁàÁµµÒ¡ÃØ³Ò àª‹¹ ¾‹ÍáÁ‹Á¤ÇÒÁ
é è Œ Õ
ÊØ¢àÁ×Íãˌᡋš àËç¹ÅÙ¡ÁÕ¤ÇÒÁÊØ¢µÑÇàͧ¡çÁ¤ÇÒÁÊØ¢ ËÒ¡ÊÒÁÒö¾Ñ²¹Òµ‹Íä»ãËŒ¤ÇÒÁàÁµµÒ¡ÃسÒ
è Ù Õ
Ἃ¢ÂÒÂÍ͡件֧¼Ù͹ ¡ÒÃãËŒ¼Í¹ ãËŒÊǹÃÇÁ ãˌʧ¤Á ¡ç¨Ð·íÒãËŒµÇàͧÁÕ¤ÇÒÁÊØ¢ ¤ÇÒÁÊآ㹢ѹ¹Õé
Œ ×è ÙŒ ×è ‹ Ñ Ñ é
໚¹¤ÇÒÁÊآËÇÁ¡Ñ¹
¤ÇÒÁÊØ¢¢Ñ¹·Õè 3 ໚¹¤ÇÒÁÊØ¢·Õà¡Ô´¨Ò¡¡ÒôíÒà¹Ô¹ªÕǵ¶Ù¡µŒÍ§ÊÍ´¤ÅŒÍ§¡Ñº¤ÇÒÁ໚¹
é è Ô
¨ÃÔ§¢Í§¸ÃÃÁªÒµÔ â´Â¸ÃÃÁªÒµÔ¢Í§ÇÔ¶ªÇµÁ¹ØÉ Á¹ØÉ´Òà¹Ô¹ªÕǵÍÂÙ·ÒÁ¡ÅÒ§¸ÃÃÁªÒµÔáÇ´ÅŒÍÁ
Õ ÕÔ í Ô ‹ ‹
373.
346 ¡ÒÃÊ‹§àÊÃÔÁÊØ¢ÀÒ¾´ŒÇ¸ÃÃÁÒ¹ÒÁÑÂ
áÅÐÊѧ¤Áà¾×͹Á¹ØÉ ´Ñ§¹Ñ¹â´Â¸ÃÃÁªÒµÔ¢Í§¡ÒôíÒà¹Ô¹ªÕǵÁ¹Øɨ§ÁÕ¤ÇÒÁÊØ¢¨Ò¡¡ÒÃä´ŒÍÒÈÑÂÍÂÙ‹
è é Ô Ö
ã¹ËÁÙà¾×͹Á¹ØÉ·Á¤ÇÒÁÊÑÁ¾Ñ¹¸Í¹´ÕµÍ¡Ñ¹ ª‹ÇÂàËÅ×ÍàÍ×ÍÍҷáѹ ä´ŒÍÒÈÑÂÍÂÙ㹸ÃÃÁªÒµÔáÇ´ÅŒÍÁ
‹ è Õè Õ Ñ ‹ é ‹
·ÕùÃÁ à¡×Í¡Ùŵ‹ÍªÕǵ ä´Œ¼Å§Ò¹Íѹà¡Ô´¨Ò¡¡ÒûÃСͺÍÒªÕ¾¡ÒçҹµÃ§µÒÁ¸ÃÃÁªÒµÔ¢Í§§Ò¹
è ×è é Ô
¤ÇÒÁÊØ¢·Õèà¡Ô´¨Ò¡¡ÒÃàʾºÃÔâÀ¤äÁ‹¨ÕÃѧÂÑè§Â×¹ Á¹ØɤÇþѲ¹ÒãËŒÊÒÁÒöËÒ¤ÇÒÁÊØ¢¨Ò¡¡ÒÃ
´íÒà¹Ô¹ªÕǵ·Õ¶¡µŒÍ§µÒÁ¤ÇÒÁ໚¹¨ÃÔ§¢Í§¸ÃÃÁªÒµÔ
Ô è Ù
¤ÇÒÁÊØ¢¢Ñé¹·Õè 4 ໚¹¤ÇÒÁÊØ¢·Õèà¡Ô´¨Ò¡¡ÒûÃاᵋ§¤ÇÒÁ¤Ô´ Á¹ØÉÂÁšɳоÔàÈÉ ¤×Í ÕÑ
»Ãاᵋ§¤ÇÒÁ¤Ô´ä´Œ »Ãاᵋ§ãËŒ·Ø¡¢¡çä´Œ ¤×Íà¡çºàÍÒÍÒÃÁ³·ÕèäÁ‹´Õ ·Õè¢Ñ´ËÙ ¢Ñ´µÒ ¢Ñ´ã¨ àÍÒÁÒ
¤Ãع¤Ô´ãËŒäÁ‹ÊºÒÂ㨠¢Ø¹ÁÑÇ àÈÃŒÒËÁͧ ËÃ×Í»Ãاᵋ§ãËŒÊØ¢¡çä´Œ ¤×Íà¡çºàÍÒᵋÍÒÃÁ³·´ÁÒ»Ãاᵋ§
‹ ‹ Õè Õ
ã¨ãˌʺÒ Á¹ØÉÂÊÒÁÒö½ƒ¡¡ÒûÃاᵋ§Êآ䴌 ઋ¹ ¢³ÐËÒÂ㨾ٴã¹ã¨¾ÃŒÍÁ¡Ñº·íÒã¨ãËŒÊÍ´¤ÅŒÍ§
¡Ñº¤íÒ¾Ù´Ç‹Ò ¨Ôµã¨àºÔ¡ºÒ¹ËÒÂã¨à¢ŒÒ ¨Ôµã¨âÅ‹§àºÒËÒÂã¨ÍÍ¡ ËÃ×ÍËÒÂã¨à¢ŒÒÊÙ´àÍÒ¤ÇÒÁÊ´ª×¹ ËÒÂ㨠è
ÍÍ¡¿Í¡ã¨ãˌʴãÊ
¤ÇÒÁÊØ¢¢Ñ¹·Õè 5 ໚¹¤ÇÒÁÊØ¢·Õà¡Ô´ä´Œâ´ÂäÁ‹µÍ§»Ãاᵋ§ à¡Ô´¨Ò¡¡ÒþѲ¹ÒãËŒÁ»Ò
é è Œ Õ ˜
ãËŒÃ෋ҷѹ¤ÇÒÁ¨ÃÔ§¢Í§âÅ¡áÅЪÕǵ ·íÒãËŒÇÒ§ã¨Å§µÑÇʹԷ ʺÒ¡Ѻ·Ø¡ÊÔ§·Ø¡Í‹ҧ àÁ×ÍÃÙࢌÒ㨤ÇÒÁ
ÙŒ Ô è è Œ
¨Ãԧਹ¨º´Õ ¤ÇÒÁÃ٨лÃѺ¤ÇÒÁÃÙÊ¡ãˌŧµÑÇ à»š¹ÊÀÒ¾¨Ôµ·ÕàÃÕº ʧº ´Ñ§¹Ñ¹Á¹ØɤÇõѧ໇ÒËÁÒÂ
Œ ŒÖ è é é
¡ÒþѲ¹Ò¨ÔµãËŒ¶Ö§ÃдѺÁÕ»˜Òãˌ䴌 à¾ÃÒл˜Ò¨Ð¹íÒÁÒ«Ö觤ÇÒÁÊØ¢¢Ñé¹·Õè 5 Íѹ໚¹¤ÇÒÁÊØ¢
·ÕÊÁºÙó ʺÒ·ÕÊ´ Á¹ØÉ·¾²¹Ò¤ÇÒÁÊØ¢¶Ö§¢Ñ¹·Õè 5 ¹Õé ¨Ð໚¹¼Ù¾ÃŒÍÁàÊǤÇÒÁÊØ¢·Ø¡Í‹ҧ㹠4
è èØ Õè Ñ é Œ
¢Ñ¹áá ᵋ¨Ð໚¹ÊØ¢·ÕäÁ‹Á¤ÇÒÁ·Ø¡¢à¨×Í»¹ äÁ‹Á¤ÇÒÁ¢Ø¹ÁÑÇ àª‹¹ ¤ÇÒÁ¡Ñ§ÇÅ ¤ÇÒÁàÊÕ´Ò ὧÍÂÙ‹
é è Õ Õ ‹
ªÕÇÔµÒ¹ÒÁÑÂ
¡ÒôÙáÅàÃ×ͧ¡ÒÃ㪌ªÇµËÃ×Í¡ÒôíÒà¹Ô¹ªÕǵµÒÁËÅѡ͹ÒÁÑ 䴌ᡋ ¡ÒÃÃÑ¡ÉÒ¤ÇÒÁÊÐÍÒ´
è ÕÔ Ô
¡ÒúÃÔâÀ¤ÍÒËÒäú¶ŒÇ¹ ¶Ù¡µŒÍ§ ¡ÒÃÅÐàÇŒ¹ÊÔ§·ÕäÁ‹¤ÇÃàʾ áÅСÒÃ㪌ªÇµã¡ÅŒª´¡Ñº¸ÃÃÁªÒµÔ è è ÕÔ Ô
¡ÒÃÃÑ¡ÉÒ¤ÇÒÁÊÐÍҴ໚¹àÃ×ͧ·Õá¹ÍÂÙ໚¹Ê‹Ç¹ÁÒ¡ ઋ¹ ¤ÇÒÁÊÐÍҴʋǹµÑÇ à¤Ã×ͧ
è è ÙŒ Ñ ‹ è
¹Ø§Ë‹Á ·ÕÍÂÙÍÒÈÑ ¡ÒÃ䴌úÍÒ¡ÒȺÃÔÊ·¸Ôì
‹ è ‹ Ñ Ø
¡ÒúÃÔâÀ¤ÍÒËÒë֧໚¹Ë¹Ö§ã¹»˜¨¨ÑÂÊբͧÁ¹Øɹ¹ ã¹áµ‹ÅÐÇѹÁ¹ØɨеŒÍ§ä´ŒÃºÍÒËÒÃ
è è è Ñé Ñ
ã¹»ÃÔÁÒ³·Õà¾Õ§¾Íà¾×ÍãËŒ´ÒçªÕǵÍÂÙä´Œ´ÇÂ´Õ ¡ÒÃÃѺ»Ãзҹ·Õ¶¡µŒÍ§¨ÐµŒÍ§ãˌ䴌úÊÒÃÍÒËÒÃ
è è í Ô ‹ Œ è Ù Ñ
¤Ãº¶ŒÇ¹µÒÁËÅÑ¡âÀª¹Ò¡Òà µŒÍ§ÁÕ¤ÇÒÁËÅÒ¡ËÅÒÂà¾×èͤÇÒÁÊÁ´ØŢͧÊÒÃÍÒËÒÃáÅÐá˸ҵØ
·ÕÃÒ§¡ÒµŒÍ§¡Òà ÍÒËÒÃÁÕ¤ÇÒÁÊÐÍÒ´ ÁÕ¤³ÀÒ¾ áÅлÅÍ´ÊÔ§·Õ໚¹¾ÔÉ áÅÐËҡ໚¹ÍÒËÒèҡ
è‹ Ø è è
¸ÃÃÁªÒµÔ ·ÕÁ¡ÒûÃاᵋ§¹ŒÍ·ÕÊ´¡ç¨ÐãËŒ»ÃÐ⪹ʧÊØ´ ËÒ¡ãËŒ¤ÇÒÁʹ㨤ÇÒÁÃÙàÃ×ͧÍÒËÒë֧
è Õ èØ Ù Œ è è
໚¹ÀÙÁÔ»˜Ò·ÕèªÒÇä·ÂÊÑè§ÊÁ¶‹Ò·ʹÊ׺µ‹Í¡Ñ¹ÁÒ ¨ÐàËç¹ä´ŒÇ‹ÒÍÒËÒÃä·ÂÍØ´Áä»´ŒÇ¼ѡ ¼ÅäÁŒ
áÅоתÊÁعä¾Ã «Ö§¨Ðª‹ÇÂ㹡ÒôÙáÅÊØ¢ÀҾ䴌 ¹Í¡¨Ò¡ÍÒËÒÃáÅŒÇÂѧÁÕà¤Ã×ͧ´×ÁáÅйéÒÊÁعä¾Ã´ŒÇÂ
è è è í
¡ÒÃÍÂÙ‹ã¡ÅŒªÔ´¸ÃÃÁªÒµÔ ËÃ×ÍÍÂÙ‹¡Ñº¸ÃÃÁªÒµÔ ¨Ð·íÒãËŒÃÒ§¡ÒÂÁÕÊ¢ÀÒ¾´Õ à¹×ͧ¨Ò¡¡Òà ‹ Ø è
ä´ŒÊÁ¼ÑʡѺ¸ÃÃÁªÒµÔ ¹Í¡¨Ò¡¨Ðä´ŒàËç¹·ÑȹÕÂÀÒ¾ÍѹÊǧÒÁ ä´Œ¿§àÊÕ§¨Ò¡¸ÃÃÁªÒµÔáÅŒÇ ¨Ð·íÒ
Ñ ˜
ãˌ䴌ÍÒ¡ÒȺÃÔÊ·¸Ôì äÁ‹ÁÁžÔÉ ÍÒ¡ÒÈ·ÕºÃÔÊ·¸Ô¨ÐࢌÒ仿͡»Í´·íÒãËŒÃÊ¡Ê´ª×¹á¨‹ÁãÊ ÃÇÁ·Ñ§¡ÒÃ
Ø Õ è Ø ì ÙŒ Ö è é
ä´Œ¾¡¼‹Í¹ ÁÕÍÃÂÒº¶µÒÁʺÒ ¨Ðª‹ÇÂÅ´¤ÇÒÁà¤ÃÕ´
Ñ ÔÔ
374.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 347
¨Ò¡»ÃÐʺ¡Òó¢Í§ÈÒʵÃÒ¨ÒùÒÂá¾·ÂÍÇ ࡵØÊ§Ë Ãкº»¯Ôºµ¹¨ÐãËŒ»ÃÐ⪹
Ô Ñ Ô Õé
Í‹ҧ¨ÃÔ§¨Ñ§ àË繼ŴÕä´Œª´à¨¹ÁÒ¡ã¹¼Ù»¯Ôºµ·ÁÍÒÂØà¡Ô¹ 35 »‚¢¹ä» ¼Ù·ÁÍÒÂعÍ¡çÍÒ¨»¯Ôºµä´Œ
Ñ Œ Ñ Ô Õè Õ Öé Œ Õè Õ Œ Ñ Ô
ä´Œ¼ÅàËÁ×͹¡Ñ¹áµ‹ÍҨഋ¹ªÑ´¹ŒÍ¡NjÒà¾ÃÒÐÊÀҾËҧ¡Ò´ÕÍÂÙ‹ ᵋ¡ÒÃàÃÔÁµŒ¹µÑ§áµ‹ÍÒÂا¹ŒÍ‹ÍÁ
è é Ñ
¨ÐãËŒ¼ÅÁÒ¡¡Ç‹ÒàÃÔÁàÁ×ÍÍÒÂØÁÒ¡áÅŒÇ
è è (4)
ÃÙ»·Õè 5 ÍÒËÒÃä·ÂÍØ´Á´ŒÇ¾ת¼Ñ¡ÊÁعä¾Ã
ÃÙ»·Õè 6 ÍÂÙ‹ã¡ÅŒªÔ´¸ÃÃÁªÒµÔ
ÊÃØ»
ËÅÑ¡ “¸ÃÃÁÒ¹ÒÁÑ” ¢Í§ÈÒʵÃÒ¨ÒùÒÂá¾·ÂÍÇ ࡵØÊ§Ë à»š¹Ãкº»¯Ôºµ·ÊÁºÙó
Ô Ñ Ô Õè
Ẻ㹡ÒÃÊÌҧàÊÃÔÁÊØ¢ÀÒ¾â´ÂÇÔ¸Õ¸ÃÃÁªÒµÔ 㹡ÒôÙáÅ»˜¨¨Ñ·ÕèÁռšÃзºµ‹ÍÊØ¢ÀҾ͋ҧ໚¹
ͧ¤ÃÇÁ ·Ñ§·Ò§´ŒÒ¹¡Ò ¨Ôµ áÅоĵԡÃÃÁ ËÅÑ¡¡Òôѧ¡Å‹ÒÇÂѧ¤§·Ñ¹ÊÁÑ ÊÍ´¤ÅŒÍ§¡ÑºËÅÑ¡¡ÒÃ
é
·Õ¡Ò˹´änj㹸ÃÃÁ¹ÙÊØ¢ÀÒ¾áË‹§ªÒµÔ ¾.È. 2552 áÅзÕÊҤѤ×Íä´Œ¼ÊÁ¼ÊÒ¹ÀÙÁ»Ò¢Í§ªÒµÔ
è í èí Ô ˜
äÇŒ´ŒÇ ¨Ö§àËÁÒÐÊÁ·Õè¨Ðà¼Âá¾Ã‹ãˌ㪌໚¹á¹Ç·Ò§ã¹¡ÒÃÊ‹§àÊÃÔÁÊØ¢ÀÒ¾µ‹Íä» ËÒ¡Êѧ¤Áä·Â
ÁÕ»ÃЪҡ÷ÕÁÊ¢ÀÒ¾¡ÒÂáÅШԵ´Õ ÁվĵԡÃÃÁ·Õ¶¡µŒÍ§ ‹ÍÁÊÒÁÒöª‹ÇÂàËÅ×͵¹àͧáÅÐÊѧ¤Áä·Â
è ÕØ è Ù
áÅÐÊѧ¤Áâš䴌໚¹àÇÅÒÂÒǹҹ ÊÁ´Ñ§à¨µ¹ÒÃÁ³¢Í§ÈÒʵÃÒ¨ÒùÒÂá¾·ÂÍÇ ࡵØÊ§Ë Ô
àǪÈÒʵ÷¹Âؤ 2553
Ñ 357
¡Òü‹ÒµÑ´¤Ç÷ըеÃǨ¤Ñ´¡ÃͧʵÃÕàËÅ‹Ò¹Õ´Ç¡ÒõÃǨàÅ×Í´ËÒ CA125 ËÇÁ¡Ñº¡ÒõÃǨÍÑŵÃÒ
è é Œ
«Òǹ·Ò§ª‹Í§¤Åʹ໚¹ÃÐÂÐæ (7)
ÂѧäÁ‹ÁÕ¢ŒÍ¾ÔÊÙ¨¹Ç‹Ò¡ÒõÃǨ¤Ñ´¡ÃͧâäÁÐàÃç§Ãѧ䢋¹Õé ¨Ðà¾ÔèÁÍѵÃÒ¡ÒÃÍÂÙ‹ÃÍ´â´ÂÃÇÁä´Œ
à¾ÃÒÐáÁŒÇÒÃѧ䢋·§ 2 ¢ŒÒ§¨Ð䴌ú¡Òü‹ÒµÑ´ÍÍ¡ä»áÅŒÇ ¡ç§ÁÕ¤ÇÒÁàÊÕ§µ‹Í¡ÒÃà¡Ô´ÁÐàÃ秷ÕàÂ×ͺتͧ
‹ Ñé Ñ Ñ è è è ‹
·ŒÍ§ä´Œ
¡ÒõÃǨ¤Ñ´¡ÃͧÁÐàÃç§Ãѧ䢋
ÇÔ¸Õ¡Ò÷Õè¨Ð¹íÒÁÒ㪌㹡ÒõÃǨ¤Ñ´¡ÃͧâäÁÐàÃç§Ãѧ䢋¹Õé¤ÇõŒÍ§ÁÕ¤ÇÒÁäÇÊÙ§ (high
sensitivity) ÁÒ¡¡Ç‹ÒÃŒÍÂÅÐ 75 ÊíÒËÃѺâäã¹ÃÐÂзÕè 1 áÅÐÁÕ¤ÇÒÁ¨íÒà¾ÒÐÊÙ§ (high specificity)
ÁÒ¡¡Ç‹ÒÃŒÍÂÅÐ 99.6 à¾×ͷըзíÒãˌ䴌 positive predictive value Í‹ҧ¹ŒÍÂÃŒÍÂÅÐ 10 ¤×Í ã¹ÊµÃÕ
è è
·Ñ§ËÁ´ 10 ÃÒ·ÕÁ¼Å¡ÒõÃǨ¤Ñ´¡Ãͧ໚¹ºÇ¡ µŒÍ§ÁռźǡÅǧäÁ‹à¡Ô¹ 9 ÃÒÂ(7) à¹×ͧ¨Ò¡àÁ×Í
é è Õ è è
ÁռŵÃǨ¤Ñ´¡Ãͧ໚¹ºÇ¡áŌǨеŒÍ§ä´ŒÃѺ¡ÒõÃǨà¾ÔèÁàµÔÁ䴌ᡋ ¡Òü‹ÒµÑ´ laparoscopy ËÃ×Í
laparotomy µ‹Íä»(8)
áÁŒÇÒâäÁÐàÃç§Ãѧ䢋¹¨ÐÁÕͺµ¡Òó¹ÍÂàÁ×Íà»ÃÕºà·Õº¡ÑºÁÐàÃç§Ê‹Ç¹Í×¹æ ᵋà¹×ͧ¨Ò¡à»š¹
‹ Õé Ø Ñ Ô Œ è è è
âä·ÕÁ͹µÃÒÂÁÒ¡¨Ö§ÁÕ¡Ò÷íÒÇÔ¨Âà¡ÕÂǡѺ¡ÒõÃǨ¤Ñ´¡Ãͧâä¡Ñ¹Í‹ҧ¡ÇŒÒ§¢ÇÒ§ ·ÕÁ¡ÒáŋÒǶ֧
è ÕÑ Ñ è è Õ
¡Ñ¹ÁÒ¡·Õʴ䴌ᡋ¡ÒÃÇԨ¢ͧ The UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS) (9)
èØ Ñ
«Ö§ÃÒ§ҹ¼Å prevalence screen àÁ×Íà´×͹àÁÉÒ¹ ¾.È. 2552 㹡ÒõÃǨ¤Ñ´¡ÃͧâäÁÐàÃç§
è è
Ãѧ䢋ã¹ÊµÃÕÇÂËÁ´ÃдÙÍÒÂØ 50 - 74 »‚ ÃÇÁ·Ñ§ÊÔ¹ 202,638 ÃÒ «Ö§à»š¹¡ÒÃÇԨ·ÕÁ¢¹Ò´ãË‹·Ê´
Ñ é é è Ñ è Õ Õè Ø
ã¹»˜¨¨Øº¹ â´Âà¡çº¢ŒÍÁÙÅÃÐËÇ‹Ò§»‚¾.È. 2544 ¶Ö§¾.È. 2548 ´ŒÇÂÇÔ¸¡ÒõÃǨẺÊØÁÍ‹ҧÁÕÃкº
Ñ Õ ‹
(Randomized controlled trial) (¤Ø³ÀÒ¾ËÅÑ¡°Ò¹ÃдѺ 1) â´Â¨Ò¡¼Å¡ÒÃÈÖ¡ÉÒàº×ͧµŒ¹¾ºÇ‹Ò¡Òà é
µÃǨ¤Ñ´¡ÃͧâäÁÐàÃç§Ãѧ䢋´Ç¡ÒõÃǨÇÑ´ÃдѺà«ÃÑÁ CA125 »‚ÅÐ 1 ¤Ãѧ áÅеÃǨÍÑŵÃÒ«Òǹ
Œ è é
Ãѧ䢋àÁ×ÍÁռšÒõÃǨàÅ×Í´·Õ¼´»¡µÔÁ¤ÇÒÁäÇÃŒÍÂÅÐ 89.4 ¤ÇÒÁ¨íÒà¾ÒÐÃŒÍÂÅÐ 99.8 ¤‹Ò positive
è è Ô Õ
predictive value ÃŒÍÂÅÐ 43.3 㹡ÒõÃǨâäÁÐàÃç§Ãѧ䢋áÅÐÁÐàÃ秷‹Í¹íÒ䢋ÀÒÂã¹ÃÐÂÐàÇÅÒ 1 »‚
·ÕµÃǨ¤Ñ´¡Ãͧâä «Ö§¼Å´Ñ§¡Å‹ÒǹշÒãËŒÊÒÁÒöŴÍѵÃÒ¡Òü‹ÒµÑ´ã¹¡ÅØÁ·ÕÁ¼Å¡ÒõÃǨ¤Ñ´¡Ãͧ
è è é í ‹ è Õ
໚¹ºÇ¡ ŧàËÅ×Í 2.3 ÊíÒËÃѺ¼Å¢Í§¡ÒõÃǨ¤Ñ´¡Ãͧâ䵋ÍÍѵÃÒ¡ÒõÒ¨ҡâä¹Ñ¹¨ÐÊÃØ»¼Åä´Œ é
ã¹»‚¾.È. 2557
à¹×ͧ¨Ò¡ÁÒ¡¡Ç‹ÒÃŒÍÂÅÐ 90 ¢Í§¼Ù»ÇÂÁÐàÃç§Ãѧ䢋äÁ‹Á¤ÇÒÁà¡ÕÂÇ¢ŒÍ§¡Ñº¡Òö‹Ò·ʹ·Ò§
è Œ † Õ è
¾Ñ¹¸Ø¡ÃÃÁ ¨Ö§Ê¹ÑºÊ¹Ø¹ãËŒµÃǨ¤Ñ´¡Ãͧâäã¹ÊµÃÕ·ÕèÍÂÙ‹ã¹ÇÑÂËÁ´ÃдÙáÅŒÇËÃ×ÍÁÕÍÒÂØ 50 »‚¢Öé¹ä»
ᵋ㹤Ãͺ¤ÃÑÇ·ÕèÁÕ»ÃÐÇѵԡÒö‹Ò·ʹ·Ò§¾Ñ¹¸Ø¡ÃÃÁËÃ×ÍʧÊÑÂÇ‹ÒÁÕÊÒþѹ¸Ø¡ÃÃÁ·Õè¼Ô´»¡µÔ
ઋ¹ BRCA1, BRCA2 ËÃ×Í HNPCC ¤ÇÃàÃÔÁ¡ÒõÃǨ¤Ñ´¡ÃͧâäãËŒàÃçÇ¢Ö¹ â´ÂÁÕ¡ÒÃÈÖ¡ÉÒÇÔ¨Â
è é Ñ
ẺµÃǨµÔ´µÒÁ仢ŒÒ§Ë¹ŒÒ (Prospective cohort study) (¤Ø³ÀÒ¾ËÅÑ¡°Ò¹ÃдѺ 2) 㹡ÅØÁʵÃÕ·Õè ‹
ÁÕ¤ÇÒÁàÊÕ§ÊÙ§â´ÂàÃÔÁµÃǨµÑ§áµ‹ÍÒÂØ 35 »‚¢¹ä»â´Â¡ÒÃÇÑ´ÃдѺ CA125 ã¹àÅ×ʹËÇÁ¡Ñº¡ÒõÃǨ
è è é Öé
ÍÑŵÃÒ«Òǹç䢋·¡ 6 à´×͹ ´Ñ§á¼¹ÀÙÁÔ
Ñ Ø (3)
366 ¡Òû‡Í§¡Ñ¹ÀÒÇÐÊÁͧàÊ×èÍÁÃдѺ»°ÁÀÙÁÔ
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Muangpaisan W, Praditsuwan R, Assanasen J, Srinonprasert V, Assantachai P, Intalapaporn S, et al. Caregiver
burden and needs of dementia caregivers in Thailand: a cross-sectional study. J Med Assoc Thai 2010;93(5):601-
7.
2. Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi HM. .orecasting the global burden of Alzheimer’s
disease. Alzheimers Dement 2007;3(3):186-91.
3. Muangpaisan W, Assantachai P, Intalapaporn S, Richardson K, Brayne C. Health expectancies in the older
Thai population. Arch Gerontol Geriatr 2010;(Article in Press).
4. Jitapunkul S, Chansirikanjana S, Thamarpirat J. Undiagnosed dementia and value of serial cognitive impairment
screening in developing countries: a population-based study. Geriatr Gerontol Int 2009;9(1):47-53.
5. ÇÕÃÈÑ¡´Ôì àÁ×ͧä¾ÈÒÅ. ÀÒÇÐÊÁͧàÊ×ÍÁã¹¼ÙʧÍÒÂØáÅСÒû‡Í§¡Ñ¹. ã¹: »ÃÐàÊÃÔ° ÍÑÊÊѹµªÑÂ, ºÃóҸԡÒÃ. »˜ËÒÊØ¢ÀÒ¾
è ŒÙ
·Õ¾ºº‹ÍÂã¹¼ÙʧÍÒÂØ. ¡Ãا෾ÁËÒ¹¤Ã: ºÃÔÉ·ÂÙà¹Õ¹ ¤ÃÕàͪѹ ¨íÒ¡Ñ´; 2552. ˹ŒÒ 125-57.
è ŒÙ Ñ è è
6. Mitchell AJ, Shiri-.eshki M. Temporal trends in the long term risk of progression of mild cognitive impairment:
a pooled analysis. J Neurol Neurosurg Psychiatry 2008;79(12):1386-91.
7. Gatz M, Prescott CA, Pedersen NL. Lifestyle risk and delaying factors. Alzheimer Dis Assoc Disord 2006;20(3
Suppl 2):S84-8.
8. Borenstein AR, Copenhaver CI, Mortimer JA. Early-life risk factors for Alzheimer disease. Alzheimer Dis Assoc
Disord 2006;20(1):63-72.
9. Bendlin BB, Carlsson CM, Gleason CE, Johnson SC, Sodhi A, Gallagher CL, et al. Midlife predictors of
Alzheimer’s disease. Maturitas 2010;65(2):131-7.
10. .licker L. Life style interventions to reduce the risk of dementia. Maturitas 2009;63(4):319-22.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 371
§. ¼Ù»ÇÂáÅФÃͺ¤ÃÑÇÂÍÁÃѺ¡ÒÃÃÑ¡ÉÒÇÔ¸¹ä´ŒËÃ×ÍäÁ‹?
Œ † Õ Õé
ÊíÒËÃѺ¡ÒÃÃÑ¡ÉÒ´ŒÇÂÂÒã¹¼ÙŒ»†ÇÂÊÙ§ÍÒÂØ à»š¹»ÃÐà´ç¹·Õèᾷ¤ÇÃãËŒ¤ÇÒÁʹã¨à»š¹¾ÔàÈÉ
à¹×èͧ¨Ò¡¼ÙŒÊÙ§ÍÒÂØ໚¹¼ÙŒ»†Ç·ÕèÁÕá¹Ç⹌Á·Õè¨Ðà¡Ô´¼Å¢ŒÒ§à¤Õ§¨Ò¡ÂÒ (adverse drug reactions)
ä´Œ §‹ Ò Â¡Ç‹ Ò ¼ÙŒ »† Ç ÂÇÑ Â Í×è ¹ ¨Ò¡¡ÒÃà»ÅÕè  ¹á»Å§·Ò§ÊÃÕ Ã ÇÔ · ÂÒ·Ñé § pharmacokinetics áÅÐ
pharmacodynamics µÒÁÇÑ ¨íҹǹÂÒ·Õ¼»ÇÂ䴌ú áÅШíҹǹâäËÇÁ¢Í§¼Ù»ÇÂ(1)
è ÙŒ † Ñ Œ †
ÊÒà˵Ø˹֧·Õ·ÒãËŒà¡Ô´»˜ËҼŢŒÒ§à¤Õ§¨Ò¡ÂÒ¤×Í ¡ÒÃ㪌ÂÒËÇÁËÅÒ¢¹Ò¹ÁÒ¡à¡Ô¹¤ÇÃ
è è í
ËÃ×Í·ÕàÃÕÂ¡Ç‹Ò polypharmacy «Ö§ÁÕ¼ãËŒ¤Ò¨íÒ¡Ñ´¤ÇÒÁÇ‹Ò à»š¹¡ÒÃ㪌ÂÒËÅÒ¢¹Ò¹ã¹àÇÅÒà´ÕÂǡѹ
è è ÙŒ í
«Ö§à¡Ô¹¤ÇÒÁ¨íÒ໚¹ áÅÐà¡Ô¹¡Ç‹Ò¢ŒÍº‹§ªÕ·Ò§¤ÅÔ¹¡ â´Â·ÑÇ件×ÍÇ‹Ò¨íҹǹÂҵѧᵋ 5 ª¹Ô´¢Ö¹ä»µ‹Í
è é Ô è é é
¼Ù»Ç 1 ¤¹
Œ † (1)
Beers áÅФ³Ð䴌ËÇÁ¡Ñ¹Ãкت×èÍÂÒ«Ö觶×ÍÇ‹Ò໚¹ÂÒ·ÕèÁÕ¤ÇÒÁàÊÕè§ÊÙ§ÊíÒËÃѺ¼ÙŒ»†ÇÂÊÙ§ÍÒÂØ
(Beers list of potentially inappropriate medications for older adults) µÑ§áµ‹ ¤.È.1997 à¹×ͧ¨Ò¡
é è
໚¹ÂÒ·ÕÁ¼Å¢ŒÒ§à¤Õ§ÁÒ¡ ä´Œ»ÃÐ⪹¹ÍÂàÁ×Íà·Õº¡Ñº¤ÇÒÁàÊÕ§·Õ¼»ÇÂ䴌ú¨Ò¡ÂÒ áÅÐÁÕÂÒÍ×¹
è Õ Œ è è è ÙŒ † Ñ è
໚¹·Ò§àÅ×Í¡á·¹ «Ö§ .ick áÅФ³Ðä´Œ»ÃѺ»ÃاÃÒ¡ÒÃÂҴѧ¡Å‹ÒÇãËŒ·¹ÊÁÑ¢ֹ㹠¤.È.2003
è Ñ é (16)
´Ñ§áÊ´§ã¹µÒÃÒ§
´Ñ§¹Ñ¹ ᾷ·´áżٻÇÂÊÙ§ÍÒÂؾ§ÃÐÁÑ´ÃÐÇѧ㹡ÒÃÊѧÂÒÊíÒËÃѺ¼Ù»ÇÂ໚¹¾ÔàÈÉ ¾Ö§ËÅÕ¡àÅÕ§
é Õè Ù Œ † Ö è Œ † è
ÂÒ·ÕÁ¤ÇÒÁàÊÕ§ÊÙ§µÒÁÃÒ¡ÒâŒÒ§µŒ¹ à¹×ͧ¨Ò¡ÁÕµÇàÅ×Í¡Í×¹·Õ»ÅÍ´ÀÑÂ¡Ç‹Ò áÅзÕÊҤѷÕÊ´
è Õ è è Ñ è è (16)
è í è Ø
ãˌ´ËÅÑ¡ “start low, go slow” ËÃ×Í¡ÒÃàÃÔÁÊѧÂÒã¹¢¹Ò´µèÒ áŌǤ‹ÍÂæ »ÃѺ¢¹Ò´ÂÒà¾ÔÁ¢Ö¹ªŒÒæ
Ö è è í è é
㹡óշÕ赌ͧÊÑè§ÂÒÊíÒËÃѺâäàÃ×éÍÃѧ áÅо֧ËÅÕ¡àÅÕ觡ÒÃÊÑè§ÂÒÁÒ¡à¡Ô¹¤ÇÒÁ¨íÒ໚¹ÊíÒËÃѺ¼ÙŒ»†ÇÂ
(polypharmacy) â´Â¶×Í໚¹Ë¹ŒÒ·Õ㹡Ò÷º·Ç¹ÃÒ¡ÒÃÂҢͧ¼Ù»Ç (review of treatment) µÑ§áµ‹
è Œ † é
ááÃѺ¼ÙŒ»†Ç áÅзíÒ໚¹»ÃШíÒÍ‹ҧ¹ŒÍÂÊÑ»´ÒËÅФÃÑ駨¹¨íÒ˹‹Ò¼ٌ»†Ç ÊíÒËÃѺ¡Ò÷º·Ç¹ (1)
ÃÒ¡ÒÃÂÒ¹Ñé¹ ÁÔ㪋à¾×èÍÅÍ¡ÃÒ¡ÒÃÂÒà´ÔÁãËŒ¤Ãº¶ŒÇ¹ ËҡᵋãËŒ¶ÒÁµ¹àͧ·Ø¡¤ÃÑ駷Õè·º·Ç¹Ç‹Ò
ÂÒ¹ÕéÂѧÁÕ¤ÇÒÁ¨íÒ໚¹ÊíÒËÃѺ¼ÙŒ»†ÇÂã¹¢³Ð¹ÕéËÃ×ÍäÁ‹ ËÒ¡µÍºÇ‹ÒäÁ‹¨íÒ໚¹ËÃ×ÍäÁ‹á¹‹ã¨ ãËŒËÂØ´ÂÒ
¹Ñ¹àÊÕÂ
é
µÒÃÒ§ áÊ´§µÑÇÍ‹ҧÂÒ·ÕèäÁ‹àËÁÒÐÊÁ·Õè¨Ð㪌㹼ٌ»†ÇÂÊÙ§ÍÒÂØ ¨íÒṡµÒÁ¤ÇÒÁàÊÕè§
ÂÒ·ÕèÁÕ¤ÇÒÁàÊÕè§ÊÙ§µ‹Í¼ÙŒÊÙ§ÍÒÂØ ÂÒ·ÕèÁÕ¤ÇÒÁàÊÕ觵‹Í¼ÙŒÊÙ§ÍÒÂØ áµ‹¹ŒÍ¡NjÒ
Antidepressants: Antihypertensives:
- Amitriptyline, Doxepin - Doxazosin
- Daily fluoxetine - Reserpine at doses >0.25 mg
- Clonidine
Long-acting benzodiazepines: Cardiac drug: Digoxin
- .lurazepam, Chlordiazepoxide, Diazepam (should not exceed >0.125 mg/d except
and Chlorazepate treating atrial arrhythmias)
399.
372 Harmonized Care for Older Patients : .ocus on Hospitalized Patients
ÂÒ·ÕèÁÕ¤ÇÒÁàÊÕè§ÊÙ§µ‹Í¼ÙŒÊÙ§ÍÒÂØ ÂÒ·ÕèÁÕ¤ÇÒÁàÊÕ觵‹Í¼ÙŒÊÙ§ÍÒÂØ áµ‹¹ŒÍ¡NjÒ
Doses of short-acting benzodiazepines: Antiplatelet aggregation: Short-acting
daily doses greater than dipyridamole
- Lorazepam 3 mg, Alprazolam 2 mg, Antimigraine: Ergot mesyloids
Temazepam 15 mg, Triazolam 0.25 mg H2 receptor blockers: Cimetidine
Barbiturates (except phenobarbital) Antianemics: .errous sulfate >325 mg/d
Antipsychotics: Thioridazine
Opioids: Pentazocine, Meperidine
Antihypertensives:
Methyldopa, Short acting nifedipine
Antiarrhythmics: Disopyramide
Hypoglycemics: Chlorpropamide
Antiplatelet aggregating agents:
Ticlopidine
Muscle relaxants and antispasmodics:
Methocarbamol, Carisoprodol,
Chlorzoxazone, Cyclobenzaprine,
Orphenadrine and Oxybutynin
Gastrointestinal antispasmodic drugs:
Dicyclomine,Hyoscyamine, Propantheline,
Belladonna alkaloids, and Clidinium-
chlordiazepoxide (Librax)
Anticholinergics and antihistamines:
Chlorpheniramine, Diphenhydramine,
Hydroxyzine, Cyproheptadine, Promethazine
and Diphenhydramine
NSAIDs: Indomethacin
Long-term use of full-dosage, longer half
-life, non–COX-selective NSAIDs:
Naproxen and Piroxicam
Laxatives: Mineral oil
Long-term use of stimulant laxatives:
Bisacodyl, Cascara sagrada except
in the presence of opiate analgesic use
ËÁÒÂà赯 ´Ñ´á»Å§¨Ò¡ .ick DM, Cooper JW, Wade WE, et al(16)
384 Harmonized Care for Older Patients : .ocus on Cognition
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Michaud L, Bula C, Berney A, Camus V, Voellinger R, Stiefel ., et al. Delirium: guidelines for general
hospitals. J Psychosom Res. 2007;62(3):371-83.
2. .laherty JH. Insomnia among hospitalized older persons. Clin Geriatr Med. 2008;24(1):51-67, vi.
3. Kakuma R, du .ort GG, Arsenault L, Perrault A, Platt RW, Monette J, et al. Delirium in older emergency
department patients discharged home: effect on survival. J Am Geriatr Soc. 2003;51(4):443-50.
4. Sieber .E. Postoperative delirium in the elderly surgical patient. Anesthesiol Clin. 2009;27(3):451-64.
5. Brouquet A, Cudennec T, Benoist S, Moulias S, Beauchet A, Penna C, et al. Impaired mobility, ASA status
and administration of tramadol are risk factors for postoperative delirium in patients aged 75 years or more
after major abdominal surgery. Ann Surg. 2010;251(4):759-65.
6. Bruce AJ, Ritchie CW, Blizard R, Lai R, Raven P. The incidence of delirium associated with orthopedic
surgery: a meta-analytic review. Int Psychogeriatr. 2007;19(02):197-214.
7. Siddiqi N, House AO, Holmes JD. Occurrence and outcome of delirium in medical in-patients: a systematic
literature review. Age & Ageing. 2006;35(4):350-64.
8. van der Mast RC, Roest .H. Delirium after cardiac surgery: a critical review. J Psychosom Res. 1996;41(1):13-
30.
9. Breitbart W, Strout D. Delirium in the terminally ill. Clin Geriatr Med. 2000;16(2):357-72.
10. Lee HB, DeLoatch CJ, Cho S, Rosenberg P, Mears SC, Sieber .E. Detection and management of pre-
existing cognitive impairment and associated behavioral symptoms in the Intensive Care Unit. Crit Care Clin.
2008;24(4):723-36, viii.
11. .ong TG, Tulebaev SR, Inouye SK. Delirium in elderly adults: diagnosis, prevention and treatment. Nat Rev
Neurol. 2009;5(4):210-20.
12. Inouye SK. Delirium in older persons. N Engl J Med. 2006;354(11):1157-65.
13. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion
assessment method. A new method for detection of delirium.Ann Intern Med. 1990;113(12):941-8.
14. Wei LA, .earing MA, Sternberg EJ, Inouye SK. The Confusion Assessment Method: a systematic review of
current usage. J Am Geriatr Soc. 2008;56(5):823-30.
15. Maldonado JR. Delirium in the acute care setting: characteristics, diagnosis and treatment. Crit Care Clin.
2008;24(4):657-722, vii.
16. Moore AR, O’Keeffe ST. Drug-induced cognitive impairment in the elderly. Drugs Aging. 1999 Jul;15(1):15-28.
17. Chutka DS, Takahashi PY, Hoel RW. Inappropriate medications for elderly patients. Mayo Clin Proc. 2004
Jan;79(1):122-39.
18. Inouye SK, Bogardus ST, Jr., Charpentier PA, Leo-Summers L, Acampora D, Holford TR, et al. A multicomponent
intervention to prevent delirium in hospitalized older patients. N Engl J Med. 1999;340(9):669-76.
19. Marcantonio ER, .lacker JM, Wright RJ, Resnick NM. Reducing delirium after hip fracture: a randomized trial.
J Am Geriatr Soc. 2001;49(5):516-22.
20. Lundstrom M, Olofsson B, Stenvall M, Karlsson S, Nyberg L, Englund U, et al. Postoperative delirium in old
patients with femoral neck fracture: a randomized intervention study. Aging Clin Exp Res. 2007;19(3):178-86.
21. Kalisvaart KJ, de Jonghe J., Bogaards MJ, Vreeswijk R, Egberts TC, Burger BJ, et al. Haloperidol prophylaxis
for elderly hip-surgery patients at risk for delirium: a randomized placebo-controlled study. J Am Geriatr Soc.
2005;53(10):1658-66.
412.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 385
22. Maldonado JR, Wysong A, van der Starre PJ, Block T, Miller C, Reitz BA. Dexmedetomidine and the
reduction of postoperative delirium after cardiac surgery. Psychosomatics. 2009;50(3):206-17.
23. Prakanrattana U, Prapaitrakool S. Efficacy of risperidone for prevention of postoperative delirium in cardiac
surgery. Anaesth Intensive Care. 2007;35(5):714-9.
24. Inouye SK. Delirium in Older Persons. N Engl J Med. 2006;354(11):1157-65.
25. Markowitz JD, Narasimhan M. Delirium and antipsychotics: a systematic review of epidemiology and somatic
treatment options. Psychiatry (Edgmont). 2008;5(10):29-36.
26. Meagher DJ. Regular review: Delirium: optimising management. BMJ. 2001;322(7279):144-9.
27. Attard A, Ranjith G, Taylor D. Delirium and its treatment. CNS Drugs. 2008;22(8):631-44.
28. Bourne RS, Tahir TA, Borthwick M, Sampson EL. Drug treatment of delirium: Past, present and future. J
Psychosom Res. 2008;65(3):273-82.
29. Lonergan E, Britton AM, Luxenberg J, Wyller T. Antipsychotics for delirium. Cochrane Database Syst Rev.
2007(2):CD005594.
30. Seitz DP, Gill SS, van Zyl LT. Antipsychotics in the treatment of delirium: a systematic review. J Clin Psychiatry.
2007;68(1):11-21.
388 Harmonized Care for Older Patients : .ocus on Mobility
âÅ¡ (antigravity muscles) Í‹ҧäáçµÒÁÍѵÃÒ¡ÒÃÅÕº¢Í§¡ÅŒÒÁà¹×ÍäÁ‹à·‹Ò¡Ñ¹ â´Â¾ºÇ‹Ò¡ÅŒÒÁà¹×Í
é é
Quadriceps ¡ÅŒÒÁà¹×éÍÃͺÊÐ⾡áÅСŌÒÁà¹×éÍËÅѧ¨ÐÅÕºàÃçÇ¡Ç‹Ò¡ÅØ‹ÁÍ×è¹æ ¡Ò÷ÕèÁÕ¡ÅŒÒÁà¹×éÍÅÕº
·ÑÇæ 仹ѹ ¨ÐÊ‹§¼Åµ‹Í¤ÇÒÁÊÒÁÒö㹡ÒÃÂ×¹ à´Ô¹ ¡ÒÃà¤Å×͹·Õè áÅÐ໚¹¼Åźµ‹Í¡ÒûÃÐÊÒ¹
è é è
¡Ò÷íÒ§Ò¹¢Í§¡ÅŒÒÁà¹×Í¡ÅØÁµ‹Ò§æ (coordination) ¹Í¡¨Ò¡¹Õ§¾º¡ÒÃŴŧ¢Í§ myofilaments áÅÐ
é ‹ é Ñ
sarcomeres áÅÐÀÒÇСŌÒÁà¹×ÍŌҧ‹Ò¨ҡ¡ÒÃŴŧ¢Í§ oxidative enzyme áÅÐ mitochondria
é
ã¹Ê‹Ç¹¢Í§àÍ繡ŌÒÁà¹×Í ¾º¡ÒÃË´Ãѧ¢Í§àÍç¹·Õà¡ÒТŒÒÁÊͧ¢ŒÍ (two-joint muscles) 䴌ᡋ
é é è
¡ÅŒÒÁà¹×Í hamstring ¡ÅŒÒÁà¹×Í hip flexor áÅСŌÒÁà¹×Í gastrocnemius áÅÐÂѧ¾º¡ÒÃà»ÅÕ¹á»Å§
é é é è
¢Í§à¹×ÍàÂ×Íà¡ÕÂǾѹ·Õ˹ҵÑÇ¢Ö¹ ·íÒãËŒ¤ÇÒÁÂ×´ËÂع¢Í§¢ŒÍµ‹Íµ‹Ò§ æ Ŵŧ
é è è è é ‹
ʋǹ¡Ãд١¹Ñé¹¾º¡Ò÷íÒÅÒ¡Ãд١·Õèà¾ÔèÁÁÒ¡¢Ö鹡NjҡÒÃÊÌҧà¹×éÍ¡Ãд١ à¹×èͧ¨Ò¡¢Ò´
áç¡Ãеع¨Ò¡¡ÒÃË´µÑǢͧ¡ÅŒÒÁà¹×Í·ÕÁµÍàÂ×ÍËØÁ¡Ãд١ (periostium) ·íÒãËŒà¡Ô´ÀÒÇСÃд١¾Ãع
Œ é è Õ ‹ è Œ
ä´ŒËÒ¡ÁÕ¡Òù͹¹Ò¹
2. ¡ÒÃà»ÅÕ¹á»Å§¢Í§ÃкºËÑÇã¨áÅÐËÅÍ´àÅ×Í´
è
¡ÒÃà»ÅÕ¹á»Å§¢Í§Ãкº¹Õ¤Í ¡ÒÃൌ¹¢Í§ËÑÇã¨ã¹¢³Ð¾Ñ¡ÁÕ¤Òà¾ÔÁ¢Ö¹ 1/2 beat µ‹ÍÇѹ
è é × ‹ è é
ʋǹ»ÃÔÁÒ³àÅ×Í´·ÕËÇ㨺պµÑÇã¹áµ‹ÅФÃѧ (stroke volume) »ÃÔÁÒ³àÅ×Í´·ÕËÇ㨺պµ‹Í˹֧¹Ò·Õ
è Ñ é è Ñ è
(cardiac output) áÅФÇÒÁÊÒÁÒö㹡ÒÃ㪌ÍÍ¡«ÔਹÊÙ§ÊØ´ (VO2max) ¨ÐŴŧ
ã¹´ŒÒ¹¤ÇÒÁ´Ñ¹âÅËÔµ ¾ºÇ‹Ò¡Òù͹¹Ò¹¨Ð·íÒãËŒà¡Ô´ÀÒÇФÇÒÁ´Ñ¹âÅËԵŴŧ㹢³Ð
à»ÅÕ¹·‹Ò à¹×ͧ¨Ò¡¡Åä¡¡ÒûÃѺµÑǢͧËÅÍ´àÅ×Í´àÊÕÂä» ¹Í¡¨Ò¡¹Õ§ÍÒ¨¾º¡ÒÃà¡Ô´ÅÔÁàÅ×Í´ÍØ´µÑ¹
è è éÑ è
ËÅÍ´àÅ×Í´ä´Œ§Ò¢ֹ «Ö§ÍҨ໚¹ÍѹµÃÒ¶֧ᡋªÇµä´Œ
‹ é è ÕÔ
ʋǹÃкºËÒÂ㨠¾ºÇ‹Òà¡Ô´¡Òõպ¢Í§ËÅÍ´ÅÁ (atelectasis) ä´Œ§‹Ò ÃÇÁ¶Ö§àÊÁËÐ
ÍØ´µÑ¹ã¹ËÅÍ´ÅÁ (secretion obstruction)
3. ¡ÒÃà»ÅÕ¹á»Å§¢Í§Ãкº·Ò§à´Ô¹»˜ÊÊÒÇÐ
è
»˜ËÒÃкº·Ò§à´Ô¹»˜ÊÊÒÇзվº¨Ò¡¡Òù͹¹Ò¹ ¤×Í »˜ËÒ¡Òö‹Ò»˜ÊÊÒÇÐÂÒ¡ ·íÒãËŒ
è
àËÅ×Í»ÃÔÁÒ³»˜ÊÊÒÇФŒÒ§ã¹¡ÃÐà¾Òл˜ÊÊÒÇÐÁÒ¡ áÅÐÊ‹§¼ÅãËŒà¡Ô´¡ÒõԴàª×Í·Ò§à´Ô¹»˜ÊÊÒÇÐà¾ÔÁ¢Ö¹
é è é
4. ¡ÒÃà»ÅÕ¹á»Å§¢Í§ÃкºÍ×¹æ ã¹Ã‹Ò§¡Ò 䴌ᡋ
è è
¡Ò÷íÒ§Ò¹¢Í§ÅíÒäÊŒÃÇÁ·Ñ駡ÒÃà¨ÃÔÍÒËÒÃŴŧ, ÍÒÃÁ³à»ÅÕè¹á»Å§§‹ÒÂ, ºÒ§ÃÒÂ
ÁռšÃзºµ‹Í¡Òù͹ËÅѺ, ¤ÇÒÁ·¹¹éÒµÒÅŴŧ (decreased glucose tolerance), ¤ÇÒÁÊÁ´ØÅ
í
¢Í§ä¹âµÃਹ໚¹Åº (negative nitrogen balance), ºÒ§¤ÃÑé§ÍÒ¨¾º¡ÒᴷѺ¢Í§àÊŒ¹»ÃÐÊÒ·
(entrapment neuropathy) ËÒ¡¹Í¹äÁ‹¶¡·‹Ò
Ù
àǪÈÒʵ÷¹Âؤ 2553
Ñ 395
»Ò¡ ¡ÒÃÍÒº¹éÒ ÅŒÒ§Ë¹ŒÒ á»Ã§¿˜¹ áÅÐᵋ§µÑÇ ÃÇÁ¶Ö§·íÒ¤ÇÒÁÊÐÍÒ´µ¹àͧÀÒÂËÅѧ¡ÒâѺ¶‹ÒÂ
í
¹Ñ¹àͧ
è
ÃÙ»·Õè 6 ¡ÒúÃÔËÒôŒÇ peg board
ÃÙ»·Õè 7 ¡ÒúÃÔËÒôŒÇ shoulder bar
! ¡ÒôÙáÅÊÀÒ¾¨Ôµã¨
¤ÇÃÁÕ¡ÒûÃÐàÁÔ¹ÊÀÒ¾¨Ôµã¨àº×ͧµŒ¹ ઋ¹ ¡ÒÃÊͺ¶ÒÁà¡ÕÂǡѺÊÀÒ¾¨Ôµã¨ ¤ÇÒÁÃÙŒ
é è
ÊÖ¡ ÍÒÃÁ³ ¡ÒÃÃѺ»ÃзҹÍÒËÒà ¡Òù͹ËÅѺ ÃÇÁ·Ñ§¤ÇÒÁࢌÒã¨áÅзÑȹ¤µÔµÍ¤ÇÒÁà¨çº»†Ç ໚¹
é ‹
µŒ¹ ºÒ§ÃÒÂÍÒ¨µŒÍ§»ÃÐàÁÔ¹à¾×ͤѴ¡ÃͧÀÒÇЫÖÁàÈÃŒÒâ´Â㪌Ẻ·´Êͺ à¹×ͧ¨Ò¡ÀÒÇЫÖÁàÈÃŒÒ໚¹
è è
ÀÒÇзվºä´ŒºÍÂã¹¼ÙʧÍÒÂØ(8) áÅÐ໚¹à˵عÒä»ÊÙ¡Òæ‹ÒµÑǵÒÂã¹ÇÑÂÊÙ§ÍÒÂØ ÍÕ¡·Ñ§à»š¹ÍØ»ÊÃä·Õè
è ‹ ŒÙ í ‹ é
ÊíҤѢͧ¡Òÿ„¹¿ÙÊÀÒ¾ ¨Ö§¤ÇÃ䴌ú¡ÒûÃÐàÁÔ¹¤Ñ´¡ÃͧµÑ§áµ‹ÃÐÂÐàÃÔÁáá à¾×Í¡ÒÃá¡Œä¢Í‹ҧ¶Ù¡
œ Ñ é è è
µŒÍ§ â´Â¹Ñ¡¨ÔµÇÔ·ÂÒãËŒ¤Ò»ÃÖ¡ÉÒ ¨Ðª‹Ç»ÃÐàÁÔ¹ÊÀÒÇзҧ´ŒÒ¹¨Ôµã¨ áÅЪÕá¹Ð¡ÒûÃѺÊÀÒ¾¨Ôµ
í é
㨷ըÐÂÍÁÃѺáÅдíÒçªÕǵÍÂÙ¡º¤ÇÒÁà¨çº»†Ç·ҧ¡ÒÂÍ‹ҧäÁ‹·¡¢ÁÒ¡¨¹à¡Ô¹ä»
è Ô ‹ Ñ Ø
423.
396 Harmonized Care for Older Patients : .ocus on Mobility
ÊÃØ»
¡ÒôÙáżٌÊÙ§ÍÒÂØ·ÕèࢌÒÃѺ¡ÒÃÃÑ¡ÉÒµÑÇ໚¹¼ÙŒ»†ÇÂã¹âç¾ÂÒºÒŹÑé¹ µŒÍ§¡ÒáÒôÙáÅ
·Ñ§·Ò§´ŒÒ¹Ã‹Ò§¡Ò áÅÐÊÀÒ¾¨Ôµã¨ â´ÂÍÒÈѤÇÒÁËÇÁÁ×ÍáÅФÇÒÁࢌÒ㨢ͧҵÔáÅФÃͺ¤ÃÑÇ
é
㹡ÒÃÁÕʋǹËÇÁ·ÕèÊíÒ¤Ñ ¡ÒôÙáŷҧËҧ¡Ò¹Ñé¹ ã¹¼ÙŒ·ÕèÂѧäÁ‹¾ÃŒÍÁÃѺâ»Ãá¡ÃÁ¿„œ¹¿Ù ¤ÇÃãËŒ
¡Òû‡Í§¡Ñ¹ÀÒÇÐá·Ã¡«ŒÍ¹Íѹà¡Ô´¨Ò¡¡Òù͹¹Ò¹ ʋǹ¼Ù·ÊÀҾËҧ¡Ò¾ÌÍÁ½ƒ¡ ãËŒ¾ÂÒÂÒÁÅØ¡
Π͏
¹Ñ§ Â×¹ ËÃ×Íà´Ô¹à·‹Ò·Õ·Òä´Œ â´ÂÁÕ¤¹´ÙáÅãËŒ¡Òê‹ÇÂàËÅ×ͺŒÒ§ËÃ×ÍÍҨ㪌ͻ¡Ã³ªÇÂËÇÁ´ŒÇ ·Ñ§¹Õé
è è í Ø ‹ é
¡ÒôÙáÅÁا์¹¤Ø³ÀÒ¾ªÕǵ·Õ´¢Í§¼ÙʧÍÒÂØ໚¹ÊíÒ¤Ñ
‹ Ô è Õ ŒÙ
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Halar EM, Bell KR. Immobility and inactivity: Physiological and functional changes, prevention, and treatment.
In: DeLisa JA, Gans BM, Walsh NE, eds. Physical Medicine & Rehabilitation; Principles and Practice, 4th ed.
Philadelphia: Lippincott Williams & Wilkins, 2005:1447-67.
2. Sharpless JW. Maintenance of joint mobility. In: Sharpless JW, ed. Mossman’s A problem-oriented approach to
stroke rehabilitation, 2nd ed. Springfield: Charles C Thomas, 1982:83-143.
3. Allman RM. Epidemiology of pressure sores in different populations. Decubitus 1989;2:30-3.
4. O’Connor KC. Pressure ulcers. In: DeLisa JA, Gans BM, Walsh NE, eds. Physical Medicine & Rehabilitation;
Principles and Practice, 4th ed. Philadelphia: Lippincott Williams&Wilkins, 2005:1605-18.
5. Tongpiputh S, Kunavusant N, Senjunfichui C. Lower extremity deep vein thrombosis among the Thai patients
with stroke. Neurol J Southeast Asia 1994;4:13-8.
6. Chang NT, Yang NP, Chou P. Incidence, risk factors and consequences of falling injuries among the
community-dwelling elderly in Shihpai, Taiwan. Aging Clin Exp Res 2010;22:70-7.
7. d’Escrivan T, Guery B. Prevention and treatment of aspiration pneumonia in intensive care units. Treat Respir
Med 2005;4:317-24.
8. Covinsky KE, .ortinsky RH, Palmer RM, Kresevic DM, Landefeld CS. Relation between symptoms of
depression and health status outcomes in acutely ill hospitalized older persons. Ann Intern Med 1997;126:417-
25.
400 Health Impacts of Environmental Threats in Thailand : Epidemiological Aspects
8. »˜ ËÒà·¤â¹âÅÂÕ á ÅÐÊØ ¢ ÀÒ¾ ã¹¢³Ð·Õè ÇÔ · ÂÒÈÒʵà á ÅÐà·¤â¹âÅÂÕ ÁÕ ¡ ÒÃ¾Ñ ² ¹Ò
ä»Í‹ҧÁÒ¡áÅÐÃÇ´àÃçÇä´Œ¡‹ÍãËŒà¡Ô´¼Å»ÃÐ⪹µ‹ÍÁ¹ØɪҵÔÁÒ¡ÁÒ ᵋ෤â¹âÅÂÕàËÅ‹Ò¹Ñé¹
¡çÍÒ¨¨Ð¡‹ÍãËŒà¡Ô´¼Åźµ‹ÍÁ¹ØÉÂáÅÐÊÔè§áÇ´ÅŒÍÁ䴌ઋ¹¡Ñ¹ »˜¨¨ØºÑ¹ÁÕà·¤â¹âÅÂÕãËÁ‹æ ·Õèà¡Ô´¢Öé¹
·ÕÍÒ¨¨Ð¡‹ÍãËŒà¡Ô´¼Å¡Ãзºµ‹ÍÊØ¢ÀÒÇзդÇèÐÁÕ¡ÒÃÈÖ¡ÉÒáÅеԴµÒÁཇÒÃÐÇѧ·ÕÊÒ¤Ñ ¤×Í ¹Òâ¹
è è è í
à·¤â¹âÅÂÕ ÊÒõѴµ‹Í·Ò§¾Ñ¹¸Ø¡ÃÃÁ ÃÇÁ·Ñ§ÊÔ§·ÕÁ¡ÒÃ㪌㹪Õǵ»ÃШíÒÇѹ·Õ¤ÇõԴµÒÁ ¤×Í ¡ÒÃ㪌
é è è Õ Ô è
â·ÃÈѾ·ÁͶ×Í à»š¹µŒ¹
×
9. »˜ËÒÊÔ§áÇ´ÅŒÍÁÍ×¹æ ઋ¹ »˜ËÒÍغµÀµ‹Ò§æ ·Ñ§ÀÑ·Õà¡Ô´µÒÁ¸ÃÃÁªÒµÔáÅзÕà¡Ô´¨Ò¡
è è Ñ Ô Ñ é è è
¡ÒáÃзíҢͧÁ¹ØÉ »˜ËÒʧ¤ÃÒÁáÅФÇÒÁÃعáçµ‹Ò§æ »˜ËÒ¨Ò¡¡Òá‹Í¡ÒÃÌҠ»˜ËÒâä
µÔ´µ‹ÍÃعáç·Ñ§·ÕͺµãËÁ‹áÅÐÍغµ«Ò ໚¹µŒ¹
é èØ Ñ Ô Ñ Ô éí
ÊÃØ»
¨Ò¡·Õ¡Å‹ÒÇÁÒ¢ŒÒ§µŒ¹¤§¨Ð·íÒãËŒàËç¹ÀÒ¾¢Í§Ê¶Ò¹¡Òó»ËÒ·Ò§´ŒÒ¹ÊÔ§áÇ´ÅŒÍÁ ·ÕÁ¼Å
è ˜ è è Õ
¡Ãзºµ‹ÍÊØ¢ÀÒ¾¢Í§»ÃÐà·Èä´ŒÇÒ á¹Ç⹌Á¢Í§Ê¶Ò¹¡ÒóÁ¤ÇÒÁÃعáçÁÒ¡¢Ö¹ áÅÐÁÕ¤ÇÒÁ«Ñº
‹ Õ é
«ŒÍ¹¢Í§¡ÒÃà¡Ô´ËÃ×Í¡‹Í»˜ËÒÁÒ¡¢Ö¹ ÊÁ¤ÇÃ໚¹Í‹ҧÂÔ§·Õ˹‹Ç§ҹ·Õà¡ÕÂÇ¢ŒÍ§·Ñ§ÀÒ¤ÃÑ°áÅÐàÍ¡ª¹
é è è è è é
ÃÇÁ·Ñ§ÀÒ¤»ÃЪҪ¹ ¤ÇõÃÐ˹ѡã¹Ê¶Ò¹¡Òó»ËÒ·Õà¡Ô´¢Ö¹áÅÐËÇÁÁ×Í㹡ÒÃËÒÁҵáÒõ‹Ò§æ
é ˜ è é
à¾×Í¡Òû‡Í§¡Ñ¹áÅФǺ¤ØÁ»˜ËҼšÃзº·Õà¡Ô´¨Ò¡ÁžÔÉÊÔ§áÇ´ÅŒÍÁ´Ñ§¡Å‹ÒÇÍ‹ҧà˧´‹Ç¹
è è è
àÍ¡ÊÒÃ͌ҧÍÔ§
1. .rumkin H. Environmental Health: .rom Global to Local., USA; Jossey-Bass Published, 2005.
2. ÊÁà¡ÕÂÃµÔ ÈÔÃõ¹¾Ä¡É áÅФ³Ð. ÃÒ§ҹ¡ÒÃÈÖ¡ÉÒ àÃ×ͧ ʶҹ¡ÒóÍÒªÕÇ͹ÒÁÑÂáÅÐÊÔ§áÇ´ÅŒÍÁã¹»ÃÐà·Èä·Â
ÔÑ è è
Êíҹѡâä¨Ò¡¡ÒûÃСͺÍÒªÕ¾áÅÐÊÔ§áÇ´ÅŒÍÁ ¾.È. 2548, 2548.
è
3. ÊíҹѡÃкҴÇÔ·ÂÒ. ÊÃØ»ÃÒ§ҹ¡ÒÃཇÒÃÐÇѧâä 2551. ¡Ãا෾ÁËÒ¹¤Ã: âç¾ÔÁ¾Í§¤¡ÒÃÃѺʋ§ÊÔ¹¤ŒÒáÅоÑÊ´ØÀ³±,
Ñ
2551.
4. Êíҹѡâä¨Ò¡¡ÒûÃСͺÍÒªÕ¾áÅÐÊÔ§áÇ´ÅŒÍÁ. ʶҹ¡Òó»ËÒᤴàÁÕÂÁ ÍíÒàÀÍáÁ‹ÊÍ´ ¨Ñ§ËÇÑ´µÒ¡. ¨ØÅÊÒáÃÁ
è ˜ è
¤Çº¤ØÁâä, 2547;15:7-9.
5. Êíҹѡâä¨Ò¡¡ÒûÃСͺÍÒªÕ¾áÅÐÊÔ§áÇ´ÅŒÍÁ. ¡ÒÃÈÖ¡ÉÒʶҹ¡ÒóâÅËÐ˹ѡ㹹éÒºÃÔâÀ¤ã¹¾×¹·ÕàÊÕ§µ‹ÍÊÒÃ˹٢ͧ
è í é è è
»ÃÐà·Èä·Â. ¹¹·ºØÃ:Õ àÍ¡ÊÒÃÍÑ´ÊíÒà¹Ò, 2547.
402 ¡ÒÃÈÖ¡ÉҼšÃзºµ‹ÍÊØ¢ÀÒ¾»ÃЪҪ¹·ÕèÍÒÈÑÂÍÂÙ‹Ãͺ¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´
ÁÕÍÂÙ‹Í‹ҧ¨íÒ¡Ñ´ ·íÒãËŒ¢Ò´¤ÇÒÁࢌÒ㨻˜ËÒ·Õèà¡Ô´¢Öé¹ã¹¾×é¹·Õè¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´ ´Ñ§¹Ñé¹
¡ÒÃÈÖ¡ÉҼšÃзºµ‹ÍÊØ¢ÀÒ¾¨Ò¡ÁžÔÉã¹ÍÒ¡ÒÈ·ÕèÁÒ¨Ò¡ÍصÊÒË¡ÃÃÁ¤ÃÑ駹Õé ¨Ð·íÒãËŒÁÕ¢ŒÍÁÙÅ
·Ò§ÇÔªÒ¡ÒôŒÒ¹ÃкҴÇÔ·ÂÒÊÔè§áÇ´ÅŒÍÁáÅÐà¾ÔèÁ¤ÇÒÁࢌÒã¨Ê¶Ò¹¡Ò󻘨¨ØºÑ¹¢Í§¾×é¹·Õè áÅÐ
¤ÇÒÁàÊÕ觢ͧ»ÃЪҡÃã¹¾×é¹·ÕèÁÒºµÒ¾Ø´ Íѹ¨Ð໚¹»ÃÐ⪹µ‹Í¡ÒèѴ¡ÒäǺ¤ØÁáÅл‡Í§¡Ñ¹
¼Å¡Ãзºµ‹ÍÊØ¢ÀÒ¾¢Í§»ÃЪҪ¹µ‹Íä»
Çѵ¶Ø»ÃÐʧ¤
Çѵ¶Ø»ÃÐʧ¤ËÅÑ¡¤×Í ÈÖ¡ÉÒ¤ÇÒÁÊÑÁ¾Ñ¹¸ÃÐËÇ‹Ò§¡ÒÃÍÒÈÑÂÍÂÙ‹Ãͺ¹Ô¤ÁÍصÊÒË¡ÃÃÁ
ÁÒºµÒ¾Ø´ ¡Ñº¡ÒÃãËŒ¡Òà¹Ô´·Òᡋ͹¡íÒ˹´ ËÃ×Í·ÒáÁÕ¹Ò˹ѡááà¡Ô´µèÒ¡Ç‹Ò»¡µÔ áÅе‹Í¡ÒÃà¡Ô´
í éí í
ÍÒ¡Ò÷ҧÃкº»ÃÐÊÒ·
ÇÔ¸Õ¡ÒÃÈÖ¡ÉÒ
»ÃЪҡ÷ÕèÈÖ¡ÉÒ¤×ͼٌ·ÕèÍÒÈѺÃÔàdzâ´ÂÃͺ¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´ ÀÒÂã¹ÃÑÈÁÕ
»ÃÐÁÒ³ 10 ¡ÔâÅàÁµÃ¨Ò¡¹Ô¤ÁÏ áÅСÒÃÈÖ¡ÉÒ¤Ãѧ¹Õ»ÃСͺ´ŒÇ 3 ¡ÒÃÈÖ¡ÉÒ‹Í 䴌ᡋ
é é
1. ¡ÒÃÈÖ¡ÉÒẺ population-based case-control study à¾×ÍÈÖ¡ÉÒ¤ÇÒÁàÊÕ§µ‹Í¡ÒäÅÍ´
è è
¡‹Í¹¡íÒ˹´ ËÃ×Í ¡ÒäÅÍ´·Òá¹éÒ˹ѡááà¡Ô´µèÒ¡Ç‹Ò»¡µÔ â´Âà»ÃÕºà·ÕºËÔ§·ÕãËŒ¡Òà¹Ô´ºØµÃ
í í è í
»¡µÔ ¨íҹǹ 487 ¤¹ ¡ÑºËÔ§·Õè¤ÅÍ´¡‹Í¹¡íÒ˹´ ËÃ×Í ÁÕ¹éíÒ˹ѡáá·Òáà¡Ô´µèíÒ¡Ç‹Ò»¡µÔ
¨íҹǹ 229 ¤¹ â´Â¢³ÐµÑ§¤ÃÃÀä´ŒÍÒÈÑÂÍÂÙã¹¾×¹·ÕºÃÔàdz¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´
é ‹ é è
2. ¡ÒÃÈÖ¡ÉÒẺ population-based survey à¾×ÍÈÖ¡ÉÒ¤ÇÒÁÊÑÁ¾Ñ¹¸¢Í§¡ÒÃà¡Ô´ÍÒ¡ÒÃ
è
·Ò§Ãкº»ÃÐÊÒ· (subjective symptoms) ¡Ñº¡ÒÃÍÒÈÑÂÍÂÙ‹ºÃÔàdz¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´
«Ö§·íÒ¡ÒÃà¡çºÃǺÃÇÁ¢ŒÍÁÙÅâ´Â¡ÒÃÊÑÁÀÒɳ ¡ÅØÁµÑÇÍ‹ҧ·ÕÁÍÒÂص§áµ‹ 13 »‚ ¢Ö¹ä»·ÕÍÒÈÑÂã¹¾×¹·Õè
è ‹ è Õ Ñé é è é
ÈÖ¡ÉÒ «Ö§ÁըҹǹµÑÇÍ‹ҧ·Ñ§ËÁ´ 17,515 ¤¹
è í é
3. ¡ÒÃÈÖ¡ÉÒẺ population-based survey à¾×ÍÈÖ¡ÉÒ¤ÇÒÁÊÑÁ¾Ñ¹¸¢Í§¡ÒÃà¡Ô´ÍÒ¡ÒÃ
è
·Ò§·Ò§¨Ôµ»ÃÐÊÒ·¡Ñº¡ÒÃÍÒÈÑÂÍÂÙºÃÔàdz¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´ â´Â㪌Ẻ·´ÊͺÁҵðҹ
‹
à¾×Í·´Êͺ·Ò§»ÃÐÊÒ·¨ÔµÇÔ·ÂÒ (neuropsychological testing) ËÅÒªش 㹡ÅØÁµÑÇÍ‹ҧ¼Ù·ÁÍÒÂØ
è ‹ Œ Õè Õ
µÑ§áµ‹ 6 »‚ ¢Ö¹ä» ·Õ·Ò¡ÒÃÊØÁẺÍÔÊÃШҡ»ÃЪҡÃã¹¾×¹·ÕÈ¡ÉÒ à¾×Í·´ÊͺÍÒ¡Ò÷ҧ¨Ôµ»ÃÐÊÒ·
é é è í ‹ é è Ö è
â´ÂÁըҹǹµÑÇÍ‹ҧ·Ñ§ËÁ´ 6,514 ¤¹
í é
à¹×ͧ¨Ò¡¢³Ð·íÒ¡ÒÃÈÖ¡ÉÒ äÁ‹Á¢ÍÁÙÅ¡ÒõÃǨÇÑ´ VOCs ã¹¾×¹·Õ·È¡ÉÒÊíÒËÃѺ¡ÒûÃÐàÁÔ¹
è Õ Œ é è Õè Ö
¡ÒÃÊÑÁ¼ÑÊÊÒà VOCs ¢Í§¡ÅØÁµÑÇÍ‹ҧâ´ÂµÃ§ ´Ñ§¹Ñ¹ ¡ÒÃÈÖ¡ÉÒ¤Ãѧ¹Õ¨§ãªŒÃÐÂÐÃÐËÇ‹Ò§·ÕÍÂÙÍÒÈÑÂ
‹ é é éÖ è ‹
¡ÑºÈٹ¡ÅÒ§¹Ô¤ÁÏ à»š¹µÑÇ᷹㹡ÒûÃÐàÁÔ¹¡ÒÃÊÑÁ¼ÑÊÁžÔÉÍÒ¡ÒȢͧ¡ÅØÁµÑÇÍ‹ҧ·ÕÍÂÙÍÒÈÑ ‹ è ‹
ÃÍºæ ¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´ â´ÂÁÕÊÁÁص°Ò¹Ç‹Ò¼Ù·ÍÂÙã¡ÅŒ¹¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´ ÁÕ¤ÇÒÁ
Ô Œ Õè ‹ Ô
àÊÕ§µ‹Í¡ÒÃ䴌ú¼Å¡Ãзº·Ò§ÊØ¢ÀÒ¾ÁÒ¡¡Ç‹Ò¼Ù·ÍÒÈÑÂÍÂÙä¡Å¹Ô¤ÁÏ ¡ÒÃÇÑ´ÃÐÂзҧ㪌â»Ãá¡ÃÁ
è Ñ Œ Õè ‹
ÊÒÃʹà·ÈàªÔ§ÀÙÁÈÒʵà (Geographic Information System) ¡ÒÃÇÑ´ÃÐÂзҧ¨Ð¶Ù¡Ãкؾ¡´´ŒÇÂà¤Ã×ͧ
Ô Ô Ñ è
ºÍ¡¾Ô¡´´ŒÇ´ÒÇà·ÕÂÁ (Geopositioning System)
Ñ
404 ¡ÒÃÈÖ¡ÉҼšÃзºµ‹ÍÊØ¢ÀÒ¾»ÃЪҪ¹·ÕèÍÒÈÑÂÍÂÙ‹Ãͺ¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´
àÍ¡ÊÒÃ͌ҧÍÔ§
1. ¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´ (2552). ·íÒà¹Õºâç§Ò¹ÍصÊÒË¡ÃÃÁ. àÍ¡ÊÒÃäÁ‹µ¾Á¾à¼Âá¾Ã‹.Õ Ô
2. Agency for Toxic Substances and Disease Registry. (2007a). Toxicological Profile for Benzene. U.S. Department
of Health and Human services, Public Health Services, Atlanta. GA.
3. Agency for Toxic Substances and Disease Registry (ATSDR). (2004). Toxicological Profile for vinyl cholride.
U.S. Department of Health and Human services, Public Health Services, Atlanta. GA.
4. Agency for Toxic Substances and Disease Registry (ATSDR). (1993). Toxicological Profile for 1,3 butadiene.
U.S. Department of Health and Human services, Public Health Services, Atlanta. GA.
5. Agency for Toxic Substances and Disease Registry (ATSDR). (1996). Toxicological Profile for 1,2-dichloroethene.
U.S. Department of Health and Human services, Public Health Services, Atlanta. GA.
6. Agency for Toxic Substances and Disease Registry. (2000). Toxicological Profile for toluene. U.S. Department
of Health and Human services, Public Health Services, Atlanta. GA.
7. Agency for Toxic Substances and Disease Registry. (2007b). Toxicological Profile for styrenes. U.S. Department
of Health and Human services, Public Health Services, Atlanta. GA.
8. Agency for Toxic Substances and Disease Registry. (2007c). Toxicological Profile for xylene. U.S. Department
of Health and Human services, Public Health Services, Atlanta. GA.
9. Lin et. al, Increased risk of preterm delivery in areas with air pollution from a petroleum refinery plant in Taiwan.
J Toxicol Environ Health A. 2001;64(8):637-44.
10. Lin et. al, Association between maternal exposure to elevated ambient sulfur dioxide during pregnancy and
term low birth weight. Environ Res. 2004;96(1):41-50.
11. Tsai et. al, Increased incidence of preterm delivery in mothers residing in an industrialized area in Taiwan. J
Toxicol Environ Health A. 2003;66(11):987-94.
12. Yang et. al, Increased risk of preterm delivery in areas with cancer mortality problems from petrochemical
complexes. Environ Res. 2002;89(3):195-200.
432.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 405
60
Climate Change and Allergic Disease
ÍÒ¨Òà¹ÒÂá¾·ÂÇÃÇÔª àËÅ×ͧàǪ¡ÒÃ
ÀÒ¤ÇÔªÒÇÔ·ÂÒÀÙÁ¤Á¡Ñ¹ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ØŒ ÔÔ
¼ÙŒª‹ÇÂÈÒʵÃÒ¨Òà¹ÒÂá¾·Â »ÒÃÂÐ ÍÒȹÐàʹ
ÀÒ¤ÇÔªÒâʵ ¹ÒÊÔ¡ ÅÒÃÔ§« ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ÔÔ
ÃͧÈÒʵÃÒ¨Òà¹ÒÂá¾·Â µ‹Í¾§É ·Í§§ÒÁ
ÀÒ¤ÇÔªÒÍÒÂØÃÈÒʵà ¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ã¹»˜¨¨Øº¹ä´ŒÁ¡Òõѧ¢ŒÍÊѧࡵNjÒÁÕ¡ÒÃà¡Ô´ÍغµÀº‹Í¢ֹáÅÐÃعáç¢Ö¹·ÑÇâÅ¡ÍÒ·Ôઋ¹¡ÒÃ
Ñ Õ é Ñ Ô Ñ é é è
à¡Ô´¤Å×¹ÂÑ¡ÉʹÒÁÔã¹àÍàªÕ àÁ×Íà´×͹¸Ñ¹ÇÒ¤Á ¤.È. 2004 ¾ÒÂØàÎÍÃÔह·ÕÁÅÃÑ° New Orleans »ÃÐ
è Ö è è
à·ÈÊËÃÑ°ÍàÁÃÔ¡Ò àÁ×Íà´×͹ÊÔ§ËÒ¤Á ¤.È. 2005 ¾ÒÂØ㵌½¹¹ÒáÊã¹»ÃÐà·ÈàÁÕ¹ÁÒà àÁ×Íà´×͹
è ؆ Ô è
¾ÄÉÀÒ¤Á ¤.È. 2008 áÅÐÅ‹ÒÊشἋ¹´Ô¹äËǤÃѧãË‹ã¹»ÃÐà·ÈàÎµÔ àÁ×Íà´×͹Á¡ÃÒ¤Á ¤.È. 2010
é è
ÍغµÀµ‹Ò§æ ·Õà¡Ô´¢Ö¹ÍÒ¨ÁÕÊÒà˵ØÁÒ¨Ò¡ÀÒÇÐ global warming «Ö§¹Í¡¨Ò¡¨ÐÁռŵ‹Í¡ÒÃà¡Ô´ÀÑÂ
Ñ Ô Ñ è é è
¸ÃÃÁªÒµÔáÅŒÇ ÀÒÇÐ global warming ÂѧÁÕ¼Åâ´ÂµÃ§µ‹ÍÊØ¢ÀÒ¾¢Í§Á¹ØÉ´§¹Õ(1) Ñ é
! ÍѵÃÒ¡ÒÃà¨çº»†ÇÂáÅСÒÃàÊÕªÕǵ¨Ò¡¤Å×¹¤ÇÒÁÌ͹ (heat wave) à¾ÔÁÊÙ§¢Ö¹
Ô è è é
! ¤ÇÒÁªØ¡¢Í§âäÀÙÁᾌáÅÐâä·Ò§à´Ô¹ËÒÂã¨à¾ÔÁ¢Ö¹
Ô è é
! ÁÕ»ÃÔÁÒ³áÅСÒáÃШÒµÑǢͧÊÒá‹ÍÀÙÁᾌÁÒ¡¢Ö¹ Ô é
¡ÒÃà»ÅÕè  ¹á»Å§¢Í§ºÃÃÂÒ¡ÒÈà¡Ô ´ ¨Ò¡¡ÒÃà¾Ôè Á ¢Öé ¹ ¢Í§¡ Ò «àÃ× Í ¹¡ÃШ¡·Õè Êí Ò ¤Ñ ¤× Í
¡Ò«¤Òú͹ä´ÍÍ¡ä«´ (CO2) ÁռŷíÒãˌͳËÀÙÁâ´ÂÃÇÁà¾ÔÁÊÙ§¢Ö¹Í‹ҧµ‹Íà¹×ͧ (global warming)
Ø Ô è é è
áÅÐÁÕÊÀÒ¾ÀÙÁÍÒ¡ÒÈ·Õá»Ã»ÃǹÁÒ¡¢Ö¹ ¡Ò« CO2 à¡Ô´¢Ö¹ÁÒ¨Ò¡¡ÒûÃСͺ¡Ô¨ÇѵûÃШíÒÇѹµ‹Ò§æ
Ô è é é
¢Í§Á¹ØÉÂáÅСÃкǹ¡ÒüÅÔµã¹ÀÒ¤ÍصÊÒË¡ÃÃÁ ÁÕ¡ÒäҴ¡ÒóNjҶ֧áÁŒ¨ÐÁÕÁҵáÒÃ
Å´¡ÒÃà¡Ô´¡Ò« CO2 Í‹ҧ¨ÃÔ§¨Ñ§ ÍسËÀÙÁâ´ÂÃÇÁ¢Í§âÅ¡¨Ðà¾ÔÁ»ÃÐÁÒ³ 1.8 oC 㹤.È. 2099
Ô è
ᵋËÒ¡»Å‹ÍÂãËŒÁ¡ÒÃà¾ÔÁ¢Ö¹¢Í§¡Ò« CO2 Í‹ҧµ‹Íà¹×ͧઋ¹ã¹»˜¨¨Øº¹ ÍسËÀÙÁâ´ÂÃÇÁ¢Í§âÅ¡
Õ è é è Ñ Ô
¨Ðà¾ÔèÁ¶Ö§»ÃÐÁÒ³ 4 C 㹤.È. 2099 ¹Í¡¨Ò¡¡Ò« CO2 áÅŒÇ ¡Ò«Í×è¹æ ·Õè¡‹ÍãËŒà¡Ô´ÁÅÀÒÇÐ
o (2)
㹺ÃÃÂÒ¡ÒÈ»ÃСͺ´ŒÇ¡ҫä¹âµÃਹä´ÍÍ¡ä«´ (NO2) ¡Ò« methane âÍ⫹ (O3) particulate
matter (PM) ¤ÅÍâÿÅÙÍÍâäÒú͹ (C.C) áÅÐ diesel exhaust particle (DEP) ÁÅÀÒÇе‹Ò§æ
àËÅ‹Ò¹ÕéÁÕʋǹÊÑÁ¾Ñ¹¸¡Ñº¡ÒÃà¡Ô´âäÀÙÁÔᾌáÅÐâäË×´«Ö觾ºÇ‹ÒÁÕÍغѵԡÒóà¾ÔèÁ¢Öé¹·ÑèÇâÅ¡ ÊíÒËÃѺ
ã¹»ÃÐà·Èä·Â ÍغѵԡÒó¢Í§âä¨ÁÙ¡ÍÑ¡àʺÀÙÁÔᾌáÅÐâäË×´ÀÙÁÔᾌÊÙ§¢Öé¹à»š¹ÅíҴѺ «Öè§ÊÒà˵Ø
ʋǹ˹֧¹‹Ò¨ÐÁÕ¤ÇÒÁàª×ÍÁ⧡ѺÊÒá‹ÍÀÙÁᾌã¹ÍÒ¡ÒÈáÅÐÁÅÀÒÇзÕà¾ÔÁÊÙ§¢Ö¹
è è Ô è è é
412 Climate Change and Allergic Disease
¡Ò««ÑÅà¿ÍÃÍÍ¡ä«´ (SO2) 㹺ÃÃÂÒ¡ÒÈʋǹãË‹à¡Ô´¨Ò¡¡ÒÃà¼Ò¶‹Ò¹ËԹ໚¹àª×éÍà¾ÅÔ§
¡ÒÃËÒÂã¨àÍÒ¡Ò« SO2 ࢌÒ仨зíÒãËŒà¡Ô´¡ÒÃË´µÑǢͧËÅÍ´ÅÁÍ‹ҧÃÇ´àÃçÇ »ÃÔÁÒ³¡Ò« SO2 0.5
ppm ¨Ð·íÒãËŒà¡Ô´¡ÒõպµÑǢͧËÅÍ´ÅÁã¹¼Ù»ÇÂâäË×´ä´Œ(41) ¢ŒÍÁÙŨҡ¡ÒûÃÐÁÒ³¡Ò󺧪ÕÇÒ
Œ † ‹ é‹
ËÒ¡ÁÕ͵ÃÒ¡ÒÃ㪌¶Ò¹ËԹ໚¹àª×Íà¾Åԧઋ¹ã¹»˜¨¨Øº¹ »ÃÔÁÒ³¢Í§¡Ò« SO2 ¨Ðà¾ÔÁ¢Ö¹ÍÕ¡ÃŒÍÂÅÐ 74
Ñ ‹ é Ñ è é
¢Í§ÃдѺ·ÕǴ䴌㹻˜¨¨Øº¹ã¹»‚ ¤.È. 2030
èÑ Ñ (42)
ÁҵáÒê‹ÇÂÅ´âšÌ͹
! 㪌ËÅÍ´ä¿¿ÅÙÍÍàÃÊૹµËÃ×ÍËÅÍ´µÐà¡Õº᷹ËÅÍ´ä¿áºº¸ÃÃÁ´Ò¨Ðª‹ÇÂÅ´¡Ò«
CO2 ä´Œ 150 »Í¹´/»‚
! 㪌ö¹µãËŒ¹ÍÂŧ ¨Ðª‹ÇÂÅ´¡Ò« CO2 ä´Œ 1 »Í¹´/¡ÒâѺö 1 äÁÅ
Œ
! ª‹Ç¡ѹ»ÃÐËÂÑ´¹éÒÁѹ·Õ㪌ÊÒËÃѺÂÒ¹¾Ò˹Р¨Ðª‹ÇÂÅ´¡Ò« CO2 20 »Í¹´/¡ÒÃ㪌¹Ò
í è í éí
Áѹ 1 á¡ÅÅ͹
! ¾ÂÒÂÒÁ¤Ñ´á¡¢ÂÐ áÅÐࢌҡÃкǹ¡ÒùíÒ¡ÅѺÁÒ㪌ãËÁ‹ (recycle)
! 㪌¹ÒÌ͹෋ҷըÒ໚¹ à¾×ÍÅ´¡ÒÃ㪌àª×Íà¾Åԧ㹡ÒÃËاµŒÁ
éí èí è é
! ËÅÕ¡àÅÕ§¡ÒÃ㪌ʹ¤ŒÒ·ÕÁ¡ÒúÃèØ˺ˋÍÁÒ¡à¡Ô¹¤ÇÒÁ¨íÒ໚¹ à¾×ÍÅ´»ÃÔÁÒ³¢ÂÐ ¨ÐÊÒ
è Ô è Õ Õ è
ÁÒöŴ¡Ò« CO2 ä´Œ 1,200 »Í¹´/¡ÒÃÅ´»ÃÔÁÒ³¢ÂÐÃŒÍÂÅÐ 10
! »ÃѺÍسËÀÙÁ¢Í§à¤Ã×ͧ»ÃѺÍÒ¡ÒÈãËŒàËÁÒÐÊÁ
Ô è
! »´áÅжʹ»ÅÑ¡à¤Ã×ͧ㪌俿‡Ò·Ø¡¤ÃѧàÁ×ÍàÅԡ㪌
ê è é è
! ª‹Ç¡ѹ»ÅÙ¡µŒ¹äÁŒ ¾ºÇ‹ÒµÅÍ´ªÕǵ¢Í§µŒ¹äÁŒ 1 µŒ¹ ÊÒÁÒö´Ù´«Ñº¡Ò« CO2 ä´Œ»ÃÐÁÒ³
Ô
1 µÑ¹
º·ÊÃØ»
¡ÒÃà»ÅÕè¹á»Å§¢Í§ÍÒ¡ÒÈ áÅÐÁÅÀÒÇзÕèà¡Ô´¨Ò¡¡Ô¨¡ÃÃÁ¡ÒôíÒà¹Ô¹ªÕÇÔµ»ÃШíÒÇѹ
¢Í§Á¹ØÉÂã¹»˜¨¨ØºÑ¹ÁÕʋǹʋ§àÊÃÔÁãËŒà¡Ô´âäÀÙÁÔᾌÁÒ¡¢Öé¹ áÅзíÒãËŒÍÒ¡Òâͧ¼ÙŒ»†ÇÂÃعáç¢Öé¹
ÁÅÀÒÇйÕ§Áռŵ‹Í¡ÒÃà¨ÃÔàµÔºâµ¢Í§¾×ª·Õ໚¹µŒ¹µÍ¢Í§ÊÒá‹ÍÀÙÁᾌã¹ÍÒ¡ÒÈ·íÒãËŒÁ¡ÒüÅÔµ
é Ñ è Ô Õ
ÊÒá‹ÍÀÙÁÔᾌà¾ÔèÁ¢Öé¹ áÅÐà¾ÔèÁ¤ÇÒÁÊÒÁÒö㹡Òá‹Íà¡Ô´ÀÙÁÔᾌ ¨Ö§ÁÕ¤ÇÒÁÊíÒ¤ÑáÅШíÒ໚¹·ÕèàÃÒ
¨ÐµŒÍ§¾ÂÒÂÒÁ»‡Í§¡Ñ¹ ËÃ×Í·íÒãËŒà¡Ô´¡ÒÃà»ÅÕ¹á»Å§¢Í§ÍÒ¡ÒÈã¹âÅ¡àÃÒ ¹ŒÍ·ÕÊ´à·‹Ò·Õ¨Ð໚¹ä»ä´Œ
è èØ è
ઋ¹ ¡ÒÃóç¤Å´ÀÒÇÐâšÌ͹áÅÐÁžÔÉã¹ÍÒ¡ÒÈ
440.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 413
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Ayres JG, .orsberg B, Annesi-Maesano I, et al. Climate change and respiratory disease: European Respiratory
Society position statement. Eur Respir J 2009;34(2):295-302.
2. IPCC 2007: summary for policy makers. In: Solomon S, Qin D, Manning M, Chen Z, Marquis M, Averyt KB,
et al, ed. Climate change 2007: the physical science basis Contribution of the Working Group I to the .ourth
Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge, United Kingdom, and
New York: Cambridge University Press.
3. Beggs PJ. Impacts of climate change on aeroallergens: past and future. Clin Exp Allergy 2004;34(10):1507-13.
4. Cortegano I, Civantos E, Aceituno E, et al. Cloning and expression of a major allergen from Cupressus
arizonica pollen, Cup a 3, a PR-5 protein expressed under polluted environment. Allergy 2004;59(5):485-90.
5. Armentia A, Lombardero M, Callejo A, et al. Is Lolium pollen from an urban environment more allergenic than
rural pollen? Allergol Immunopathol (Madr) 2002;30(4):218-24.
6. .ranze T, Weller MG, Niessner R, Poschl U. Enzyme immunoassays for the investigation of protein nitration
by air pollutants. Analyst 2003;128(7):824-31.
7. .ranze T, Weller MG, Niessner R, Poschl U. Protein nitration by polluted air. Environ Sci Technol 2005;39(6):
1673-8.
8. Gruijthuijsen YK, Grieshuber I, Stocklinger A, et al. Nitration enhances the allergenic potential of proteins. Int
Arch Allergy Immunol 2006;141(3):265-75.
9. Behrendt H, Becker WM. Localization, release and bioavailability of pollen allergens: the influence of environmental
factors. Curr Opin Immunol 2001;13(6):709-15.
10. Motta AC, Marliere M, Peltre G, Sterenberg PA, Lacroix G. Traffic-related air pollutants induce the release of
allergen-containing cytoplasmic granules from grass pollen. Int Arch Allergy Immunol 2006;139(4):294-8.
11. Bartra J, Mullol J, del Cuvillo A, et al. Air pollution and allergens. J Investig Allergol Clin Immunol 2007;17
Suppl 2:3-8.
12. Sydbom A, Blomberg A, Parnia S, Stenfors N, Sandstrom T, Dahlen SE. Health effects of diesel exhaust
emissions. Eur Respir J 2001;17(4):733-46.
13. Ormstad H, Johansen BV, Gaarder PI. Airborne house dust particles and diesel exhaust particles as allergen
carriers. Clin Exp Allergy 1998;28(6):702-8.
14. Schober W, Belloni B, Lubitz S, et al. Organic extracts of urban aerosol (< or =PM2.5) enhance rBet v 1-
induced upregulation of CD63 in basophils from birch pollen-allergic individuals. Toxicol Sci 2006;90(2):377-84.
15. Shea KM, Truckner RT, Weber RW, Peden DB. Climate change and allergic disease. J Allergy Clin Immunol
2008;122(3):443-53; quiz 54-5.
16. Ziska LH, Epstein PR, Schlesinger WH. Rising CO(2), climate change, and public health: exploring the links to
plant biology. Environ Health Perspect 2009;117(2):155-8.
17. Peteet D. Sensitivity and rapidity of vegetational response to abrupt climate change. Proc Natl Acad Sci U S
A 2000;97(4):1359-61.
18. .itter AH, .itter RS. Rapid changes in flowering time in British plants. Science 2002;296(5573):1689-91.
19. Ziska LH, Gebhard DE, .renz DA, .aulkner S, Singer BD, Straka JG. Cities as harbingers of climate change:
common ragweed, urbanization, and public health. J Allergy Clin Immunol 2003;111(2):290-5.
20. Rogers CA, Wayne PM, Macklin EA, et al. Interaction of the onset of spring and elevated atmospheric CO2
on ragweed (Ambrosia artemisiifolia L.) pollen production. Environ Health Perspect 2006;114(6):865-9.
21. Breton MC, Garneau M, .ortier I, Guay ., Louis J. Relationship between climate, pollen concentrations of
Ambrosia and medical consultations for allergic rhinitis in Montreal, 1994-2002. Sci Total Environ 2006;370(1):
39-50.
441.
414 Climate Change and Allergic Disease
22. Rasmussen A. The effects of climate change on the birch pollen season in Denmark. Aerobiologia 2002;18:
253-65.
23. .renguelli G, Tedeschini E, Veronesi ., Bricchi E. Airborne pine (Pinus spp.) pollen in the atmosphere of
Perugia (Central Italy): Behavior of pollination in the two last decades. Aerobiologia 2002;18:223-8.
24. Teranishi H, Kenda Y, Katoh T, Kasuya M, Oura E, Taira H. Possible role of climate change in the pollen
scatter of Japanese cedar Cryptomeria japonica in Japan. Climate Res 2000;14:65-70.
25. Saxon A, Diaz-Sanchez D. Air pollution and allergy: you are what you breathe. Nature immunology 2005;6(3):
223-6.
26. Trevino RJ. Air pollution and its effect on the upper respiratory tract and on allergic rhinosinusitis. Otolaryngol
Head Neck Surg 1996;114(2):239-41.
27. Bjorksten ., Suoniemi I. Time and intensity of first pollen contacts and risk of subsequent pollen allergies. Acta
Medica Scandinavica 1981;209(4):299-303.
28. Braat JP, Mulder PG, Duivenvoorden HJ, Gerth Van Wijk R, Rijntjes E, .okkens WJ. Pollutional and meteorological
factors are closely related to complaints of non-allergic, non-infectious perennial rhinitis patients: a time series
model. Clin Exp Allergy 2002;32(5):690-7.
29. Assanasen P, Naclerio RM. Cold, dry air and hyperosmolar challenge in rhinitis. In: Pawankar R, Holgate ST,
Rosenwasser LJ, ed. Allergy frontiers: Clinical manifestations. Tokyo: Springer; 2009:157-71.
30. Gauderman WJ, Vora H, McConnell R, et al. Effect of exposure to traffic on lung development from 10 to 18
years of age: a cohort study. Lancet 2007;369(9561):571-7.
31. McCreanor J, Cullinan P, Nieuwenhuijsen MJ, et al. Respiratory effects of exposure to diesel traffic in persons
with asthma. N Engl J Med 2007;357(23):2348-58.
32. Edwards J, Walters S, Griffiths RK. Hospital admissions for asthma in preschool children: relationship to major
roads in Birmingham, United Kingdom. Arch Environ Health 1994;49(4):223-7.
33. Lin S, Munsie JP, Hwang SA, .itzgerald E, Cayo MR. Childhood asthma hospitalization and residential
exposure to state route traffic. Environ Res 2002;88(2):73-81.
34. Nicolai T, Carr D, Weiland SK, et al. Urban traffic and pollutant exposure related to respiratory outcomes and
atopy in a large sample of children. Eur Respir J 2003;21(6):956-63.
35. McConnell R, Berhane K, Gilliland ., et al. Asthma in exercising children exposed to ozone: a cohort study.
Lancet 2002;359(9304):386-91.
36. McDonnell W., Abbey DE, Nishino N, Lebowitz MD. Long-term ambient ozone concentration and the incidence
of asthma in nonsmoking adults: the AHSMOG Study. Environ Res 1999;80(2 Pt 1):110-21.
37. Holz O, Mucke M, Paasch K, et al. Repeated ozone exposures enhance bronchial allergen responses in
subjects with rhinitis or asthma. Clin Exp Allergy 2002;32(5):681-9.
38. Brunekreef B, .orsberg B. Epidemiological evidence of effects of coarse airborne particles on health. Eur
Respir J 2005;26(2):309-18.
39. Pope CA, 3rd, Burnett RT, Thun MJ, et al. Lung cancer, cardiopulmonary mortality, and long-term exposure to
fine particulate air pollution. JAMA 2002;287(9):1132-41.
40. Barck C, Lundahl J, Hallden G, Bylin G. Brief exposures to NO2 augment the allergic inflammation in asthmatics.
Environ Res 2005;97(1):58-66.
41. Peden DB. Mechanisms of pollution-induced airway disease: in vivo studies. Allergy 1997;52(38 Suppl):37-44;
discussion 57-8.
42. Energy Information Administration. International Energy Outlook 2008. Available at http://www.eia.doe.gov/
oiaf/ieo/coal.html. Accessed March 30, 2008.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 439
Hemiballism
ÀÒÇÐ hemiballism ໚¹ÀÒÇÐ hyperkinetic movement ÃٻẺ·ÕÁ¤ÇÒÁÃعáçÁÒ¡·ÕÊ´
è Õ è Ø
áÅÐÊÒÁÒö·íÒãËŒ¤¹ä¢ŒÁÕ exhaustion 䴌͋ҧÁÒ¡ ᵋÊǹãË‹ hemiballism ÁÑ¡¨ÐËÒÂä»àͧ ã¹
‹
¡Ã³Õ·Õè hemiballism äÁ‹ËÒÂä»àͧËÅѧ¡ÒõԴµÒÁ໚¹àÇÅÒ¹Ò¹¾ÍÊÁ¤Çà ÊÁ¤ÇþԨÒóҶ֧¡Òü‹Ò
µÑ´ «Öè§ÁÕÃÒ§ҹ¡ÒüšÒü‹ÒµÑ´·Õè´Õ·Ñ駨ҡ thalamotomy ààÅÐ pallidotomy ¼Å¡Òü‹ÒµÑ´¼ÙŒ»†ÇÂ
persistent hemiballism 1 ÃÒ´ŒÇÂÇÔ¸Õ pallidotomy ¾ºÇ‹Ò hemiballism ËÒÂä»ã¹¡ÒõԴµÒÁ 5 »‚
Tourette syndrome
»˜¨¨Øº¹ÁÕÃÒ§ҹ¼Å·Õ´¨Ò¡¡Òü‹ÒµÑ´ deep brain stimulation àോµÒàà˹‹§ target ¢Í§¡ÒÃ
Ñ è Õ í
¼‹ÒµÑ´ÂѧÁÕ¤ÇÒÁËÅÒÂËÅÒ¡ ÁÕÃÒ§ҹ¼Å¡Òü‹ÒµÑ´·Õè´Õ·Ñ駨ҡ anteromedial globus pallidus,
posterolateral globus pallidus, anterior limb of internal capsule, neuclear accumben ààÅÐ medial
thalamus «Ö§ÁÕÃÒ§ҹ¨íҹǹ¼Ù»ÇÂÁÒ¡·ÕÊ´ â´Â¨Ð target ·Õè centromedian parafasicular complex
è Œ † èØ
(CM-Pfc) ËÇÁ¡Ñº Ventral oraoanterior nucleus (VOa) ¢Í§ thalamus26 ¼Å¡Òü‹ÒµÑ´¼Ù»Ç 2 ÃÒÂ
Œ †
´ŒÇÂÇÔ¸Õ bilateral CM-Pfc-VOa deep brain stimulation ààÅÐÍÕ¡ 1 ÃÒ´ŒÇÂÇÔ¸Õ bilateral pallidal deep
brain stimulation ¾ºÇ‹Òª‹ÇÂãËŒ motor tics ààÅÐ vocal tics ´Õ¢¹Öé
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Kelly PJ, Gillingham .J. The long-term results of stereotaxic surgery and L-dopa therapy in patients with
Parkinson’s disease. A 10-year follow-up study. J Neurosurg 1980;53(3):332-7.
2. .ine J,Duff J, Chen R, Chir B, Hutchison W, Lozano AM, Lang AE. Long-term follow-up of unilateral pallidotomy
in advance Parkinson’s disease. N Engl J Med 2000;342(23):1708-14.
3. Krack P, Batir A, Van Blercom N, Charbardes S, .raix V, Ardouin C, Koudsie A, Limousine PD, Benazzouz A,
LeBus J., Benabid AL, Pollak P. .ive-year follow-up of bilateral stimulation of the subthalamic nucleus in
advance Parkinson’s disease. N Engl J Med 2003;349(20):1925-34.
4. Nunta-aree S, Sithinamsuwan B, Boonyapisit K, Pisarnpong A. 2 year outcomes of subthalamic deep brain
stimulation for idiopathic Parkinson’s disease. J Med Assoc Thai 2010;93(5):529-40.
5. Deep brain stimulation for Parkinson’s disease study group. Deep brain stimulation of the subthalamic nucleus
or the par interna of the globus pallidus in Parkinson’s disease. N Engl J Med 2001;345(13):956-63.
6. Volkmann J, Albert N, Vogas J, Sturm V, Schnitzler A, .reund HJ. Long-term results of bilateral pallidal
stimulation in Parkinson’s disease. Ann Neurol 2004;55(6):871-5.
7. Stefani A, Lozano AM, Peppe A, Stanzione P, Galati S, Tropepi D, Pierantozzi M, Brusa L, Scarnati E,
Mazzone P. Bilateral deep brain stimulation of the pedunculopontine and subthalamic nuclei in severe Parkinson’s
disease. Brain 2007;130:1596-1607.
8. .rench Stimulation du Pallidum Interne dans la Dystonie (SPIDY) Study Group. Bilateral deep brain stimulation
of the globus pallidus in primary general dystonia. N Engl J Med 2005;352:459-67.
9. Coubes P, Rouberrtie A, Vayssiere N, Hemm S, Echenne B. Treatment of DYT1-generalised dystonia by
stimulation of the internalglobus pallidus. Lancet 2000;355(9222):2220-1.
10. Alkhani A, Bohlega S: Unilateral pallidotomy for hemidystonia. Mov Disord 2006;21(6):852-5.
467.
440 Movement Disorder Surgery
11. Biolsi B, Cif L, El .ertit H: Long-term follow-up of Huntington disease treated by bilateral deep brain stimulation
of the internal globus pallidus. J Neurosurg 2008;109:130–2.
12. Chuang C, .ahn S, .rucht SJ: The natural history and treatment of acquired hemidystonia: report of 33 cases
and review of the literature. J Neurol Neurosurg Psychiatry 2002;72:59–67.
13. Coubes P, Echenne B, Cif L, et al: Electrical stimulation of the internal globus pallidus in generalized dystonia.
Mov Disord 2002;17 (Suppl 5):S6.
14. Gruber D, Trottenberg T, Kivi A, et al: Long-term effects of pallidal deep brain stimulation in tardive dystonia.
Neurology 2009;73:53-8.
15. Holloway K, Baron M, Brown R, et al: Deep brain stimulation for dystonia: a meta-analysis. Neuromodulation
2006;9:253–61.
16. Justeson CR, Penn RD, Kroin JS, et al: Stereotactic pallidotomy in a child with Hallervorden-Spatz disease.
Case report. J Neurosurg 1999;90:551-4.
17. Loher TJ, Hasdemir MG, Burgunder JM, et al: Long-term follow-up study of chronic globus pallidus internus
stimulation for posttraumatic hemidystonia. J Neurosurg 2000;92:457–60.
18. Starr PA, Turner RS, Rau G, et al: Microelectrode – guided implantation of deep brain stimulators into the
globus pallidus internus for dystonia: techniques, electrode locations, and outcomes. Neurosurg .ocus 2004;
17(1):E4:20-31.
19. Umemura A, Jaggi JL, Dolinskas CA, et al: Pallidal deep brain stimulation for longstanding severe generalized
dystonia in Hallervorden-Spatz syndrome. Case report. J Neurosurg 2004;100:706–9.
20. Volkmann J, Benecke R: Deep brain stimulation for dystonia: patient selection and evaluation. Mov Disord
2002;17(Suppl. 3):S112-5.
21. Yianni J, Bain P, Giladi N, et al: Globus pallidus internus deep brain stimulation for dystonic conditions: a
prospective audit. Mov Disord 2003;18:436–2.
22. Bertrand CM. Selective peripheral denervation for spasmodic torticollis:surgical technique, results, and observations
in 260 cases. Surg Neurol 1993;40(2):96-103.
23. Alusi S H; Aziz T Z; Glickman S; Jahanshahi M; Stein J .; Bain P G. Stereotactic lesional surgery for the
treatment of tremor in multiple sclerosis: a prospective case-controlled study. Brain 2001;124:1576-89.
24. Nandi D; Chir M; Liu X; Bain P; Parkin S; Joint C; Winter J; Stein J; Scott R; Gregory R; Aziz T. Electrophysiological
confirmation of the zona incerta as a target for surgical treatment of disabling involuntary arm movements in
multiple sclerosis: use of local field potentials. Journal of clinical neuroscience 2002;9(1):64-8.
25. Plaha P, Patel NK, Gill SS. Stimulation of the subthalamic region for essential tremor. J Neurosurg 2004;101:305-
11.
26. Servello D, Porta M, Sassi M, Brambilla A, Robertson MM. Deep brain stimulation in 18 patients with severe
Gilles de la Tourette syndrome refractory to treatment: the surgery and stimulation. J Neurol Neurosurg
Psychiatry 2008;79:136-42.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 451
6. Definition of mild traumatic brain injury developed by the Mild Traumatic Brain Injury Committee of the Head
Injury Interdisciplinary Special Interest Group of the American Congress of Rehabilitation Medicine. J Head
Trauma Rehabil 1993:8(3):86-7.
7. Alexander MP. Mild traumatic brain injury: Pathophysiology, natural history, and clinical management. Neurology
1995;45(7):1253-60.
8. Madikians A, Giza CC. A clinician’s guide to the pathophysiology of traumatic brain injury. Indian J Neurotrauma
2006;3(1):9-17.
9. Haydel MJ, Preston CA, Mills TJ, Luber S, Blaudeau E, DeBlieux PM. Indications for computed tomography
in patients with minor head injury. N Engl J Med 2000;343(2):100–5.
10. Ruff RM, Iverson GL, Barth JT, Bush SS, Broshek DK, the NAN Policy and Planning Committee.
Recommendations for diagnosing a mild traumatic brain injury: a national academy of neuropsychology
education paper. Arch Clin Neuropsychol 2009;24 (1):3-10.
11. Vos PE, Battistin L, Birbamer G, Gerstenbrand F, Potapov A, Prevec T, Stepan ChA, Traubner P, Twijinstra A,
Vecsei L, von Wild K; European Federation of Neurological Societies. EFNS guideline on mild traumatic brain
injury: report of an EFNS task force. Eur J Neurol 2002 9(3):207-19.
12. Chambers J, Cohen SS, Hemminger L, Prall JA, Nichols JS. Mild traumatic brain injuries in low-risk trauma
patients. J Trauma 1996;41(6):976-80.
13. Bohnen N, Jolles J, Twijnstra A. Neuropsychological deficits in patients with persistent symptoms six months
after mild head injury. Neurosurgery 1992;30(5):695-6.
14. Arciniegas DB, Anderson CA, Topkoff J, McAllister TW. Mild traumatic brain injury: a neuropsychiatric approach
to diagnosis, evaluation, and treatment. Neuropsychitr Dis Treat 2005;1(4):311-27.
15. Smith DH. Postconcussional symptoms not a syndrome. Psychosomatics 2006;47(3):271.
16. Riggio S, Wong M. Neurobehavioral sequelae of traumatic brain injury. Mount Sinai J Med 2009;76:163-72.
17. Greenberg MS. Handbook of Neurosurgery 6th ed. Ontario: Thieme;2006.
18. Thurman DJ, Branche CM, Sniezek JE. The epidemiology of sports related traumatic brain injuries in the
United States: recent developments. J Head Trauma Rehabil 1998;13(2):1–8.
19. Sturmi JE, Smith C, Lombardo JA. Mild brain trauma in sports diagnosis and treatment guidelines. Sports Med
1998;25(6):351-8.
20. Majerske CW, Mihalik JP, Ren D, Collins MW, Reddy CC, Lovell MR, Wagner AK. Concussion in sports:
postconcussive activity, levels, symptoms, and neurocognitive performance. J Athl Train 2008;43(3):265-74.
21. Heck J, Rosa R. Evaluating mild head injuries incorporating the standardized assessment of concussion. Sport
Med Updates 2001;15(2):46-52.
480.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 453
64
Neuropsychiatric Disorders after Mild Traumatic Brain Injury
ÍÒ¨ÒàᾷÂËÔ§¾Ã¨ÔÃÒ »ÃÔÇѪÃÒ¡ØÅ
ÀÒ¤ÇÔªÒ¨ÔµàǪÈÒʵà ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ÔÔ
¡ÒúҴà¨çº·ÕÈÃÉÐáÅÐÊÁͧ ໚¹»˜ËÒÊÒ¸ÒóÊØ¢·ÕÊҤѢͧ»ÃÐà·Èä·Â â´ÂÃŒÍÂÅÐ 77
è Õ èí
¢Í§¼Ù»ÃÐʺÍغµà˵بҡ¡ÒèÃҨèÐÁÕÍÒ¡ÒúҴà¨çº·ÕÈÃÉÐËÇÁ´ŒÇ «Ö§áÁŒÇÒʋǹãˋ໚¹¡ÒÃ
Œ Ñ Ô è Õ è ‹
ºÒ´à¨çº·ÕÈÃÉÐáÅÐÊÁͧàÅ硹ŒÍ¶֧»Ò¹¡ÅÒ§ ᵋ¡Ê§¼ÅãËŒà¡Ô´¤‹Ò㪌¨Ò·ѧ·Ò§µÃ§áÅзҧ͌ÍÁÊÙ§
è Õ ç‹ ‹ é
¶Ö§»‚ÅÐ 40 ŌҹºÒ· (1) »˜ËÒ¡ÒûÃÐʺÍغµà˵غҴà¨çº·Ò§ÊÁͧàÅ硹ŒÍ (mild traumatic brain
Ñ Ô
injury) ¾ºä´ŒºÍÂã¹à´ç¡ ÇÑÂÃع ¼ÙãË‹µÍ¹µŒ¹ áÅмÙʧÍÒÂØ(2-3) áÅоºã¹à¾ÈªÒÂÁÒ¡¡Ç‹Òà¾ÈËÔ§
‹ ‹ Œ ŒÙ
¡ÒúҴà¨çº´Ñ§¡Å‹ÒÇÊ‹§¼ÅãËŒ¤ÇÒÁÊÒÁÒö¢Í§¼Ù»ÇÂŴŧ áÅÐÁÕ¤ÇÒÁàÊÕ§·Õ¨Ðà¡Ô´âä·Ò§¨ÔµàǪ
Œ † è è
ÁÒ¡¡Ç‹Ò¼ÙŒ·ÕèäÁ‹»ÃÐʺÍغѵÔà˵ض֧ 2.8 à·‹Ò ·íÒãËŒà¡Ô´¼ÅàªÔ§Åºµ‹Í¡Ò÷íÒ§Ò¹ Êѧ¤Á ÊÑÁ¾Ñ¹¸
(4)
ÀÒ¾ÃÐËÇ‹Ò§ºØ¤¤Å ÃÇÁ件֧¤Ø³ÀÒ¾ªÕǵ¢Í§·Ñ§¼Ù»Ç áÅÐÒµÔ¼´áÅÍÕ¡´ŒÇÂ(5-6)
Ô é Œ † ÙŒ Ù
¹ÔÂÒÁ
Mild traumatic brain injury (MTBI) µÒÁ¹ÔÂÒÁ¢Í§ American Congress of Rehabilitation
Medicine (ACRM) Brain Injury Special Interest Group (7) ËÁÒ¶֧ ¡ÒúҴà¨çº·ÕÈÃÉзÕà¡Ô´¤ÇÒÁ
è Õ è
¼Ô´»¡µÔ·Ò§ÊÃÕÃÇÔ·ÂҢͧ˹ŒÒ·ÕèÊÁͧ (physiological disruption) «Öè§áÊ´§à»š¹ÍÒ¡ÒÃÍ‹ҧ¹ŒÍÂ
1 ã¹ 4 ¢ŒÍ´Ñ§µ‹Í仹Õé
1. ÃÐÂÐàÇÅÒ·Õ¼»ÇÂËÁ´ÊµÔ (duration of loss of consciousness; LOC) ¹ŒÍÂ¡Ç‹Ò 30 ¹Ò·Õ
è ÙŒ †
áÅÐ Glasgow Coma Score (GCS) ËÅѧ¼Ù»Ç¿„¹¨Ò¡¡ÒÃËÁ´ÊµÔ ÁÕ¤Ò 13 -15 ¤Ðá¹¹
Œ † œ ‹
2. ÁÕ¡ÒÃÊÙàÊÕ¤ÇÒÁ¨íÒà¡ÕÂǡѺà˵ءÒó¡Í¹Íغµà˵ØËÃ×ÍËÅѧÍغµà赯 â´Â post-traumatic
è ‹ Ñ Ô Ñ Ô
amnesia (PTA) ¹ŒÍÂ¡Ç‹Ò 24 ªÑÇâÁ§
è
3. ÁÕ¡ÒÃà»ÅÕ¹á»Å§¢Í§ÊÀÒ¾¨Ôµ (mental state)ã¹¢³Ð·Õà¡Ô´ÍغµàËµØ àª‹¹ ÃÙÊ¡ÁÖ¹§§ ÊѺʹ
è è Ñ Ô ŒÖ
disorientate
4. Focal neurological deficit (s) «Ö§ÍÒ¨ÁժǤÃÒÇËÃ×ÍäÁ‹¡ä´Œ
è Ñè ç
¾ÂÒ¸ÔÊÃÕÃÇÔ·ÂÒ
456 Neuropsychiatric Disorders after Mild Traumatic Brain Injury
»˜¨¨Ñ¢ŒÒ§µŒ¹·Ñé§ 3 ¡ÅØ‹Á ÊÒÁÒöÁռŵ‹Í¡Ñ¹áÅСѹ áÅÐÁÕÍÔ·¸Ô¾Åµ‹Í neuropsychiatric
symptoms ·Ñ§ã¹á§‹¢Í§ÅѡɳÐÍÒ¡Òà ¡Òä§ÍÂÙ‹ áÅСÒÃËÒ¨ҡÍÒ¡ÒÃ
é
¡ÒÃÃÑ¡ÉÒ
¡ÒÃÃÑ¡ÉҼٻǠMTBI ·ÕÁÀÒÇзҧ¨ÔµàǪ ¤ÇÃ㪌¡ÒÃÃÑ¡ÉÒẺͧ¤ÃÇÁ ¤ÇÃÃÑ¡ÉÒÍÒ¡ÒÃ
Œ † è Õ
µ‹Ò§æ ãËŒ¤Ãͺ¤ÅØÁ´ŒÇ¡ÒÃ㪌ÂÒãËŒ¹Í·ÕÊ´à·‹Ò·Õ¨Ð໚¹ä»ä´Œ ¼Ù»Ç·ÕÁÕ MTBI ÁÑ¡¨Ðäǵ‹Í¡ÒÃà¡Ô´
Œ èØ è Œ † è
¼Å¢ŒÒ§à¤Õ§¨Ò¡ÂÒä´Œ§Ò ´Ñ§¹Ñ¹ãËŒàÃÔÁÂÒ·Õ¢¹Ò´µèÒ áÅлÃѺ¢Ö¹ªŒÒæ â´Â¾ÂÒÂÒÁËÅÕ¡àÅÕ§ÂÒ·ÕÅ´
‹ é è è í é è è
seizure threshold áÅÐÂÒ·Õè·íÒãËŒ¡Òÿ„œ¹¿Ù cognition ªŒÒŧ ઋ¹ phenytoin, phenobarbital,
benzodiazepine, clonidine, haloperidol (¢¹Ò´ > 10 mg/d) ໚¹µŒ¹(11) ¼Ù»ÇÂÁÑ¡ÁÕ¡Òõͺʹͧµ‹Í Œ †
ÂÒªŒÒ áÅÐàÁ×Í»ÃѺÂÒ¶Ö§¢¹Ò´ÊÙ§ÊØ´áÅŒÇ ÍÒ¨µŒÍ§ãªŒàÇÅÒ´ÙÍÒ¡ÒùҹËÅÒÂà´×͹ ¹Í¡¨Ò¡¹Õé ¤ÇÃãËŒ
è
¡ÒÃÃÑ¡ÉÒÍÒ¡ÒÃÍ×¹æ ·ÕÍҨú¡Ç¹¼Ù»Ç ઋ¹ ÍÒ¡ÒûǴ ÍÒ¡Òäѹ ໚¹µŒ¹
è è Œ †
ã¹·Õ¹¨Ð¢Í¡Å‹ÒǶ֧¡ÒÃ㪌ÂÒ໚¹ËÅÑ¡ Í‹ҧäáçµÒÁ¡ÒÃãËŒ¤ÇÒÁÃÙ¡º¼Ù»ÇÂáÅÐÒµÔ ÃÇÁ·Ñ§
è Õé Œ Ñ Œ † é
ãËŒ¡ÒÅѧã¨áÅЪ‹ÇÂàËÅ×Íà¡ÕÂǡѺ¡ÒûÃѺµÑǵ‹Í¡ÒÃà¨çº»†ÇÂ໚¹ÊÔ§ÊíÒ¤Ñ ÁÕ¡ÒÃÈÖ¡ÉÒ¾ºÇ‹Ò·Ñ§»ÃЪҪ¹
í è è é
·ÑÇä»áÅкؤÅҡ÷ҧ¡ÒÃá¾·Â ÁÑ¡äÁ‹à¢ŒÒ㨼Ţͧ MTBI ·ÕÁµÍ neuropsychiatric function ¢Í§
è è Õ ‹
¼Ù»Ç ·íÒãËŒà¡Ô´¤ÇÒÁÃÙÊ¡àªÔ§Åºµ‹Í¼Ù»Ç áÅкҧÃÒ¶١¡Å‹ÒÇËÒÇ‹Òá¡ÅŒ§»†Ç ¨¹ä´ŒÃº¡ÒôÙáÅÍ‹ҧ
Œ † ŒÖ Œ † Ñ
äÁ‹àËÁÒÐÊÁ (12-13)
¡ÒûÃѺ¾ÄµÔ¡ÃÃÁ ¡Òü‹Í¹¤ÅÒ¤ÇÒÁà¤ÃÕ´ áÅд֧¤Ãͺ¤ÃÑÇࢌÒÁÒÁÕÊǹËÇÁ ‹
໚¹ÊÔ§ÊíҤѵ‹Í¡ÒÃÃÑ¡ÉÒ ÃÇÁ·Ñ§à»š¹¡ÒÃà»´âÍ¡ÒÊãˌҵÔä´ŒÃкÒ ÃѺ·ÃÒº¢ŒÍÁÙÅáÅÐÁÕ¤ÇÒÁ¤Ò´
è é
ËÇѧ·ÕÊÍ´¤ÅŒÍ§¡Ñº¤ÇÒÁ໚¹¨ÃÔ§ ÃÇÁ·Ñ§àÃÕ¹ÃÙǸ¡ÒèѴ¡ÒþĵԡÃÃÁ¢Í§¼Ù»ÇÂáÅÐÍÒÃÁ³¢Í§µÑÇ
è é ŒÔÕ Œ †
ÒµÔàͧàÁ×Í༪ԡѺÍÒ¡ÒÃà¨çº»†Ç¢ͧ¼Ù»Ç´ŒÇ «Ö§¨Ð·íÒãËŒ¼Å¡ÒÃÃÑ¡ÉÒâ´ÂÃÇÁ´Õ¢¹ÁÒ¡
è Œ † è Öé
ã¹»˜¨¨Øº¹ ÂÒ·ÕÁËÅÑ¡°Ò¹àªÔ§»ÃШѡÉÊÒËÃѺÃÑ¡ÉÒÍÒ¡Ò÷ҧ¨ÔµàǪ¢Í§¼Ù»Ç MTBI Âѧ¤‹Í¹
Ñ è Õ í Œ †
¢ŒÒ§ÁÕ¨Ò¡Ñ´ (µÒÃÒ§·Õè 2) ᾷ¨§¤ÇÃ㪌ÂÒâ´Â¤íÒ¹Ö§¶Ö§¤ÇÒÁàËÁÒÐÊÁµ‹Í¼Ù»ÇÂᵋÅÐÃÒ ãËŒ¢ÍÁÙÅ
í Ö Œ † Œ
áÅТͤÇÒÁÂÔ¹ÂÍÁ¨Ò¡¼Ù»ÇÂáÅÐ/ËÃ×ÍÒµÔ à½‡ÒÃÐÇѧµÔ´µÒÁ¼ÅÍѹäÁ‹¾§»ÃÐʧ¤¨Ò¡ÂÒ »ÃÐàÁÔ¹
Œ † Ö
»ÃÐÊÔ·¸ÔÀÒ¾¡ÒÃÃÑ¡ÉÒ áÅзº·Ç¹¤ÇÒÁ¨íÒ໚¹¢Í§¡ÒÃ㪌ÂÒÍÂÙàÊÁÍ ‹
¹Í¡¨Ò¡¹Õé¼ÙŒà¢Õ¹ÁÕ¤ÇÒÁàËç¹Ç‹Ò 㹺ÃÔº·¢Í§Êѧ¤Áä·Â »˜¨¨Ñ·ÕèÊíÒ¤ÑÍÕ¡¢ŒÍ·Õè¤ÇùíÒÁÒ
¾Ô¨ÒÃ³Ò ¤×Í àÈÃÉ°°Ò¹Ð¢Í§¼Ù»Ç ¡µÑÇÍ‹ҧઋ¹ ÂÒ fluoxetine áÁŒ¨ÐÁÕËÅÑ¡°Ò¹Ê¹ÑºÊ¹Ø¹ã¹¡ÒÃ
Œ †
ÃÑ¡ÉÒÍÒ¡ÒëÖÁàÈÃŒÒã¹ MTBI ¹ŒÍÂ¡Ç‹Ò sertraline ᵋ¼Å¢ŒÒ§à¤Õ§¹ŒÍÂà·‹Òæ¡Ñ¹ áÅÐÃÒ¤Ò¶Ù¡¡Ç‹Òà¡Ô¹
10 à·‹Ò á¾·Â¤ÇõŒÍ§àʹͷҧàÅ×Í¡Í×¹æ áÅÐãËŒ¢ÍÁÙÅ»ÃСͺ¡ÒõѴÊÔ¹ã¨á¡‹¼»ÇÂËÃ×ÍÒµÔ´ÇÂ
è Œ ÙŒ † Œ
áÁŒ·Ò§àÅ×Í¡Í×¹æ ¹Ñ¹ÍÒ¨ÁÕËÅÑ¡°Ò¹·Ò§ÇÔ·ÂÒÈÒʵÃÁÒʹѺʹع¹ŒÍ¡NjҡçµÒÁ á¹Ç¤ÇÒÁ¤Ô´¹ÕÊÍ´
è é é
¤ÅŒÍ§¡Ñº¹ÔÂÒÁ¡ÒÃ㪌ÂÒÍ‹ҧÊÁà˵ØÊÁ¼Å (rational drug use) ¢Í§Í§¤¡ÒÃ͹ÒÁÑÂâÅ¡·ÕÇÒ “Rational è‹
use of drugs requires that patients receive medications appropriate to their clinical needs, in
doses that meet their own individual requirements for an adequate period of time, and the
lowest cost to them and their community.” (14)
484.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 457
µÒÃÒ§·Õè 2 ¡ÒÃ㪌ÂÒÃÑ¡ÉÒ neuropsychiatric symptoms ã¹¼ÙŒ»†Ç MTBI (11, 15-17)
Neuropsychiatric Symptoms ÂÒ ¢¹Ò´àÃÔÁµŒ¹ (mg/day) ¢¹Ò´ÂÒ໇ÒËÁÒ (mg/day)
è
Depression Sertraline 25 25 - 200
Citalopram 10 20 - 50
Fluoxetine 10 20 - 40
Amitriptyline a 10 - 25 75 - 250
Cognitive disturbance Methylphenidate 5 - 10 10 - 30 (0.25 - 0.3 mg/kg)
Donepezil 5 5 - 10
Rivastigmine 3 3 - 12
Bromocriptine 2.5 < 100
Aggressiveness b Propanolol 20 - 30 60 - 400
Pindolol 40 40 - 100
Buspirone 10 45 - 60
Sodium valproate 200 - 500 750 - 1,000
Carbamazepine 200 - 400 400 - 1200
Psychosis Olanzapine c 5 5 - 20
Haloperidol c 2-5 < 10
Mania Sodium valproate 200 - 500 750 - 1,000
Insomnia Trazodone 25 - 50 50 - 150
a
㪌Í‹ҧÃÐÁÑ´ÃÐÇѧ à¹×ͧ¨Ò¡ÂÒÅ´ seizure threshold
è
b
ÍÒ¨ÃÑ¡ÉÒâ´Â㪌ÂÒÃÑ¡ÉÒÍÒ¡Òà depression ã¹µÒÃҧ䴌ઋ¹¡Ñ¹
c
㪌¢¹Ò´µèÒáÅÐÃÐÂÐÊѹ෋ҷըÒ໚¹ à¹×ͧ¨Ò¡ÂҢѴ¢ÇÒ§¡Òÿ„¹¿Ù´Ò¹ cognition
í é èí è œ Œ
ÊÃØ»
Neuropsychiatric disorders ÊÒÁÒö¾ºä´ŒºÍ¶֧˹֧ã¹ÊÒÁ¢Í§¼Ù»Ç·ÕÁÕ mild traumatic
‹ è Œ † è
brain injury Ê‹§¼Å¡Ãзºµ‹ÍÊØ¢ÀÒ¾áÅФسÀÒ¾ªÕǵ¢Í§¼Ù»ÇÂáÅФÃͺ¤ÃÑÇä´ŒÁÒ¡ áÅÐ໚¹»˜ËÒ
Ô Œ †
·Ò§ÊÒ¸ÒóÊØ¢·ÕÊÒ¤Ñ ºØ¤Åҡ÷ҧ¡ÒÃᾷ¨§¤ÇÃཇÒÃÐÇѧ áÅлÃÐàÁÔ¹ÍÒ¡Òà à¾×ÍãËŒ¡ÒÃÃÑ¡ÉÒ
èí Ö è
á¡‹¼»ÇÂÍ‹ҧàËÁÒÐÊÁ
ÙŒ †
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Suriyawongpaisal P, Kanchanasut S. Road traffic injuries in Thailand: Trends, selected underlying determinants
and status of intervention. Injury Control and Safety Promotion. 2003;10(1-2):95-104.
2. Massagli TL, Fann JR, Burington BE, Jaffe KM, Katon WJ, Thompson RS. Psychiatric illness after mild
traumatic brain injury in children. Arch Phys Med Rehabil. 2004;85(9):1428-34.
3. Schwarzbold M, Diaz A, Martins ET, Rufino A, Amante LN, Thais ME, et al. Psychiatric disorders and
traumatic brain injury. Neuropsychiatr Dis Treat. 2008;4(4):797-816.
485.
458 Neuropsychiatric Disorders after Mild Traumatic Brain Injury
4. Fann JR, Burington B, Leonetti A, Jaffe K, Katon WJ, Thompson RS. Psychiatric illness following traumatic
brain injury in an adult health maintenance organization population. Arch Gen Psychiatry. 2004;61(1):53-61.
5. Rogers JM, Read CA. Psychiatric comorbidity following traumatic brain injury. Brain Inj. 2007;21(13-14):1321-
33.
6. Petchprapai N, Winkelman C. Mild traumatic brain Injury: determinants and subsequent quality of life. a review
of the literature. Journal of Neuroscience Nursing. 2007;39(5):13.
7. Mild Traumatic Brain Injury Committee ACoRM, Head Injury Interdisciplinary Special Interest Group. Definition
of mild traumatic brain injury. Journal of Head Trauma Rehabilitation. 1993;8(3):86-7.
8. Silver JM, McAllister TW, Arciniegas DB. Depression and cognitive complaints following mild traumatic brain
injury. Am J Psychiatry. 2009;166(6):653-61.
9. Koponen S, Taiminen T, Kurki T, Portin R, Isoniemi H, Himanen L, et al. MRI findings and Axis I and II
psychiatric disorders after traumatic brain injury: a 30-year retrospective follow-up study. Psychiatry Res.
2006;146(3):263-70.
10. Bryant RA, O’Donnell ML, Creamer M, McFarlane AC, Clark CR, Silove D. The Psychiatric Sequelae of
Traumatic Injury. Am J Psychiatry. 2010;167(3):312-20.
11. Lombardi F. Pharmacological treatment of neurobehavioural sequelae of traumatic brain injury. European
Journal of Anaesthesiology. 2008;25(Suppl 42):131-6.
12. Guilmette TJ, Paglia MF. The public’s misconceptions about traumatic brain injury: a follow up survey. Archives
of Clinical Neuropsychology. 2004;19(2):183-9.
13. Swift TL, Wilson SL. Misconceptions about brain injury among the general public and non-expert health
professionals: an exploratory study. Brain Injury. 2001;15:149-65.
14. WHO. The Rational Use of Drugs: Report of the Conference of Experts. Geneva: WHO,1985.
15. Fann JR, Hart T, Schomer KG. Treatment for Depression after Traumatic Brain Injury: A Systematic Review.
Journal of Neurotrauma. 2009;26(12):2383-402.
16. Warden DL, Gordon B, McAllister TW, Silver JM, Barth JT, Bruns J, et al. Guidelines for the Pharmacologic
Treatment of Neurobehavioral Sequelae of Traumatic Brain Injury. Journal of Neurotrauma. 2006;23(10):1468-
501.
17. Silver JM, Yudofsky SC, Hales RE. Neuropsychiatric aspects of traumatic brain injury. In: Yudofsky SC, Hales
RE, editors. The American Psychiatric Publishing textbook of neuropsychiatry and behavioral neurosciences:
American Psychiatric Publishing; 2008. p. 595-648.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 477
7. Yaquinto JJ, Harms SE, Siemers PT, .lamig DP, Griffey RH, .oreman ML. Arterial injury from penetrating
trauma: evaluation with single-acquisition fat-suppressed MR imaging. Am J Roentgenol. 1992;158(3):631-3.
8. Catalano C, .raioli ., Laghi A, Napoli A, Bezzi M, Pediconi ., et al. Infrarenal aortic and lower-extremity arterial
disease: diagnostic performance of multi-detector row CT angiography. Radiology. 2004;231(2):555-63.
9. Katz DS, Hon M. CT angiography of the lower extremities and aortoiliac system with a multi-detector row
helical CT scanner: promise of new opportunities fulfilled. Radiology. 2001;221(1):7-10.
10. Martin ML, Tay KH, .lak B, .ry PD, Doyle DL, Taylor DC, et al. Multidetector CT angiography of the aortoiliac
system and lower extremities: a prospective comparison with digital subtraction angiography. Am J Roentgenol.
2003;180(4):1085-91.
11. Ota H, Takase K, Igarashi K, Chiba Y, Haga K, Saito H, et al. MDCT compared with digital subtraction
angiography for assessment of lower extremity arterial occlusive disease: importance of reviewing cross-
sectional images. Am J Roentgenol. 2004;182(1):201-9.
12. Rubin GD, Schmidt AJ, Logan LJ, Sofilos MC. Multi-detector row CT angiography of lower extremity arterial
inflow and runoff: initial experience. Radiology. 2001;221(1):146-58.
13. .ishman EK, Horton KM, Johnson PT. Multidetector CT and three-dimensional CT angiography for suspected
vascular trauma of the extremities. Radiographics. 2008 ;28(3):653-65; discussion 65-6.
14. Rieger M, Mallouhi A, Tauscher T, Lutz M, Jaschke WR. Traumatic arterial injuries of the extremities: initial
evaluation with MDCT angiography. Am J Roentgenol. 2006;186(3):656-64.
15. Pieroni S, .oster BR, Anderson SW, Kertesz JL, Rhea JT, Soto JA. Use of 64-row multidetector CT angiography
in blunt and penetrating trauma of the upper and lower extremities. Radiographics. 2009;29(3):863-76.
488 Imaging of Trauma : Abdominal Trauma
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Rhea JT. CT of Abdominal Trauma in Mann .A. Emergency radiology categorical course in diagnostic
radiology RSNA 2004 Syllabus, 2004:91-112
2. .eliciano DV, Mattox KL, Moore EE. Trauma, 6th ed. New York: McGraw-Hill companies, 2008:261-328
3. Korner M, Krotz MM, Degenhart C, et al. Current role of emergency US in patients with major trauma.
Radiographic 2008;28:225-44
4. Shanmuganathan K, Killeen KL. Imaging of abdominal trauma in Mirvis SE, Shanmuganathan K. Imaging of
trauma and critical care, 2nd ed. Philadelphia: WB Saunders, 2003:369-517
5. Yoon W, Jeong YY, Kim JK, et al. CT in blunt liver trauma. Radiographic 2005;25:87-104
6. Yaghmai V. Splenic trauma and surgery in Gore RM, Levine MS. Textbook of gastrointestinal radiology, 3rd ed.
Philadelphia: WB Saunders, 2008:2051-64
7. Alonso RC, Nacenta SB, Martinez PD, et al. Kidney in danger: CT findings of blunt and penetrating renal
trauma. Radiographics 2009; 2033-53
8. Dunnick NR, Sandler CM, Newhouse JH, et al. Urinary tract trauma in Textbook of uroradiology, 3rd ed.
Philadelphia: Lippincott Williams & Wilkins, 2001:451-83
9. Ramchandani P, Buckler PM. Imaging of genitourinary trauma. AJR 2009;192:1514-23
10. Vaccaro JP, Brody JM. CT cystography in the evaluation of major bladder trauma. Radiographic 2000;20:1373-
81
11. Brody JM, Leighton DB, Murphy BL, et al. CT of blunt trauma bowel and mesenteric injury: typical findings and
pitfalls in diagnosis. Radiographics 2000;20:1525-36
516.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 489
68
Traumatic Cerebrovascular Injury : Neurosurgical Perspective
ÍÒ¨Òà¹ÒÂá¾·ÂàÍ¡ÇØ²Ô ¨Ñ¹á¡ŒÇ1,2
ÍÒ¨Òà¹ÒÂᾷ·ÇÕÈÑ¡´Ôì àÍ×éͺØÒÇѲ¹1,2
ÃͧÈÒʵÃÒ¨ÒàᾷÂËÔ§ÍѪÅÕ ªÙâè¹2
1
ÀÒ¤ÇÔªÒÈÑÅÂÈÒʵà ¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
2
ÀÒ¤ÇÔªÒÃѧÊÕÇ·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ÔÔ
ÀÒÇÐ traumatic cerebrovascular injury ໚¹ÀÒÇзվºäÁ‹ºÍÂᵋÁ¤ÇÒÁÊíÒ¤Ñ «Ö§ÍÒ¨
è ‹ Õ è
·íÒãËŒ¼ÙŒ»†Ç¶֧ᡋªÕÇÔµ ¶ŒÒãËŒ¡ÒÃÃÑ¡ÉÒäÁ‹àËÁÒÐÊÁÍ‹ҧ·Ñ¹·‹Ç§·Õ ¢³Ð¹ÕéÂѧäÁ‹ÁÕ¡ÒÃÃÒ§ҹã¹
»ÃÐà·Èä·Â ᵋÍغѵԡÒó¨Ò¡ÃÒ§ҹ¢Í§µ‹Ò§»ÃÐà·ÈÍÂÙ‹ÃÐËÇ‹Ò§ 0.18-1.55 % ¢Í§¼ÙŒ»†ÇÂ
·ÕúÍغµà赯 ¡ÒÃÃÑ¡ÉÒ¼Ù»ÇÂ㹡ÅØÁ¹Õ§ÁÕ¤ÇÒÁ«Ñº«ŒÍ¹ÁÒ¡¢Ö¹à¹×ͧ¨Ò¡¼Ù»ÇÂÁÑ¡ÁÕ¡ÒúҴà¨çºÃкº
èÑ Ñ Ô Œ † ‹ é Ôè é è Œ †
Í׹ËÇÁ´ŒÇÂ
è
㹺·¤ÇÒÁ¹Õ¨Ð¤Ãͺ¤ÅØÁà¹×ÍËҴѧ¹Õé
é é
1. Classification of traumatic cerebrovascular injury
1.1 Anatomical consideration
1.2 Pathological consideration
2. ¡ÒôÙáżٻÇ·ÕÁÀÒÇÐ traumatic cerebrovascular injury (Evaluation and treatment
Œ † è Õ
option for traumatic cerebrovascular injury)
Classification of traumatic cerebrovascular injury
ã¹»˜¨¨Øº¹ÂѧäÁ‹Á¡ÒèíÒṡ traumatic cerebrovascular injury ·Õ໚¹·ÕÂÍÁÃѺ«Ö§ÍÒ¨à¹×ͧ
Ñ Õ è è è è
ÁÒ¨Ò¡¡ÒúҴà¨çºÁÕËÅÒ¡Åä¡áÅоÂÒ¸ÔÊÀÒ¾ÁÕä´ŒËÅÒ¡ËÅÒ 㹷Õè¹Õé¨Ð¢Í¨íÒṡ traumatic
cerebrovascular injury µÒÁËÑÇ¢ŒÍµ‹Ò§æ´Ñ§¹Õé
By mechanisms of injury
Penetrating cerebrovascular injury
Nonpenetrating cerebrovascular injury
Iatrogenic injury
Cranial injury with secondary cerebrovascular injury
517.
490 Traumatic Cerebrovascular Injury : Neurosurgical Perspective
By location of injury
Cervical portion injury
Skull base portion injury
Intracranial portion injury
By vascular type injury
Arterial system injury
Venous system and dural sinus injury
By arterial distribution
Carotid artery injury
Common carotid artery injury
Internal carotid artery injury
External carotid artery injury
Vertebral artery injury
By pathological finding
Arterial side
Occlusion
Dissection
.alse aneurysm
Arteriovenous fistula
Venous side
Dural tears
Compression of the pial vein and venous thrombosis
ã¹·Õè¹Õé¨Ð¢ÍÊÃػ໚¹ 2 ¨íҾǡà¾×èͧ‹Òµ‹Í¤ÇÒÁࢌÒ㨤×Í â´ÂµíÒá˹‹§¡ÒúҴà¨çº·Ò§
¡ÒÂÇÔÀÒ¤ (by anatomical consideration ) áÅÐ â´Â¾ÂÒ¸ÔÊÀÒ¾·Õà¡Ô´¢Ö¹ (by pathological finding)
è é
¡ÒÃẋ§â´ÂµíÒá˹‹§¡ÒúҴà¨çº·Ò§¡ÒÂÇÔÀÒ¤
ICA Relevant Regional Anatomy Remark
Cervical carotid artery Cervical spine Carotid dissection, Carotid
occlusion : Cerebral emboli
Petrous carotid artery Temporal bone, Ear ossicles, Carotid occlusion : Cerebral
Lower Cranial Nerve emboli
Cavernous carotid artery Cavernous sinus, Sphenoid sinus, .alse carotid aneurysm : massive
Cranial Nerve III, IV, V1, V2 epistaxis, Subarachnoid hemorrhage
(intradural extension)
àǪÈÒʵ÷¹Âؤ 2553
Ñ 493
¡ÒûÃÐàÁÔ¹¼ÙŒ»†Ç·ÕèʧÊÑÂÀÒÇÐ traumatic cerebrovascular injury
1. Basic and advanced trauma life support Âѧ໚¹¡ÒÃÃÑ¡ÉÒàº×ͧµŒ¹·ÕÁ¤ÇÒÁ¨íÒ໚¹
é è Õ
2. »ÃÐàÁÔ¹ neurological deficit
3. ¡ÒÃÊ׺¤Œ¹à¾ÔÁàµÔÁ
è
3.1 CT áÅÐ CTA
໚¹¡ÒÃÊ׺¤Œ¹·ÕÊÒÁÒöµÃǨËÒ¾ÂÒ¸ÔÊÀÒ¾¢Í§ÊÁͧáÅÐ ¡ÒúҴà¨çº¢Í§ËÅÍ´
è
àÅ×Í´ä´Œ¾ÃŒÍÁ¡Ñ¹ã¹ÃÐÂÐàÇÅÒÍѹÊÑé¹ ¹Í¡¨Ò¡¹ÕéµíÒá˹‹§¢Í§àÅ×Í´·ÕèÍÍ¡ËÃ×Í¡ÐâËÅ¡ÈÕÃÉзÕèᵡ
ÊÒÁÒöª‹ÇÂÇҧἹ¡ÒÃÃÑ¡ÉÒËÃ×Í»‡Í§¡Ñ¹ÀÒÇÐá·Ã¡«ŒÍ¹¨Ò¡¡Ò÷íÒ¼‹ÒµÑ´ CT áÅÐ/ËÃ×Í CTA Âѧ
ÁÕÊǹª‹ÇÂÊíÒËÃѺ¡ÒõԴµÒÁ¡ÒÃà»ÅÕ¹á»Å§ÀÒÂËÅѧ¡ÒÃÃÑ¡ÉÒ
‹ è
3.2 Cerebral angiogram
໚¹¡ÒÃÊ׺¤Œ¹·ÕÊÒÁÒöµÃǨËÒ ¡ÒúҴà¨çº¢Í§ËÅÍ´àÅ×Í´ä´Œ¾ÃŒÍÁ¡Ñ¹¡Ñº¡ÒÃ㪌
è
ÃѧÊÕÃÇÁÃÑ¡ÉÒä´Œã¹àÇÅÒà´ÕÂǡѹ ¹Í¡¨Ò¡¹Õ§ÊÒÁÒö»ÃÐàÁÔ¹ cerebral hemodynamic (cerebral blood
‹ éÑ
flow, collateral circulation and occlusion test)
3.3 MRI áÅÐ MRA
໚¹¡ÒÃÊ׺¤Œ¹·ÕèÊÒÁÒöµÃǨËÒ¾ÂÒ¸ÔÊÀÒ¾¢Í§ÊÁͧáÅСÒúҴà¨çº¢Í§ËÅÍ´
àÅ×Í´ä´Œ¾ÃŒÍÁ¡Ñ¹áµ‹¨Ò໚¹µŒÍ§ãªŒàÇÅÒ㹡ÒõÃǨ·Õ¹Ò¹áÅÐÍÒ¨äÁ‹àËÁÒÐÊÁ㹼ٻǷÕ䴌úÍغµÔà˵Ø
í è Œ † è Ñ
·ÕÍÒ¡ÒÃäÁ‹¤§·Õè
è
3.4 Transcranial Doppler ultrasound (TCD)
໚¹¡ÒÃÊ׺¤Œ¹·ÕÊÒÁÒöµÃǨËÒÍغµ¡Òó¢Í§ÅÔÁàÅ×Í´ËÅØ´ÅÍÂã¹ÊÁͧ (cerebral
è Ñ Ô è
emboli) ¹Í¡¨Ò¡¹Õ§ÊÒÁÒö»ÃÐàÁÔ¹ cerebral hemodynamic (cerebral blood flow, collateral
é Ñ
circulation)
3.5 Brain SPECT without and with stress test
໚¹¡ÒÃÊ׺¤Œ¹·ÕÊÒÁÒö»ÃÐàÁÔ¹ cerebral hemodynamic (cerebral blood flow,
è
collateral circulation) ·Ñ§¹ÕÍҨ㪌ÃÇÁ¡Ñº¡ÒõÃǨÇԸ͹ઋ¹ balloon occlusion test
é é ‹ Õ ×è
¡ÒôÙáÅÃÑ¡ÉÒ¼ÙŒ»†ÇÂÁÕÀÒÇÐ traumatic cerebrovascular injury
Multidisciplinary team approach ÁÕ¤ÇÒÁÊíÒ¤ÑÍ‹ҧÂÔ§ »ÃСͺ´ŒÇ neurovascular team
è
(neurointerventionist neurosurgeon) trauma surgeon ¨Ñ¡ÉØá¾·Â á¾·ÂËÙ ¤Í ¨ÁÙ¡ ¡ÒÃÃÑ¡ÉÒÁÕ
ËÅÒÂÇÔ¸¢¹ÍÂÙ¡º¾ÂÒ¸ÔÊÀÒ¾áÅТŒÍÁÙŨҡ¡ÒÃÊ׺¤Œ¹µ‹Ò§æ´Ñ§·Õä´Œ¡Å‹ÒÇÁÒáŌǢŒÒ§µŒ¹ â´Â·ÑÇä»ÁÑ¡
Õ Öé ‹ Ñ è è
µŒÍ§ãªŒ¡ÒÃÃÑ¡ÉÒËÅÒÂÇÔ¸ÃÇÁ¡Ñ¹
Õ‹
Goal of treatment for arterial injury
1. »‡Í§¡Ñ¹ÀÒÇÐàÅ×Í´ÍÍ¡ (acute hemorrhage or hemorrhagic infarction)
2. »‡Í§¡Ñ¹ÀÒÇÐÊÁͧ¢Ò´àÅ×Í´ (acute or late cerebral infarction)
521.
494 Traumatic Cerebrovascular Injury : Neurosurgical Perspective
2.1 »‡Í§¡Ñ¹ÀÒÇÐÅÔÁàÅ×Í´ (emboli)
è
2.2 »‡Í§¡Ñ¹ÀÒÇÐàÅ×Í´ä»àÅÕ§ÊÁͧäÁ‹à¾Õ§¾Í (inadequate cerebral blood flow)
é
·Ò§àÅ×͡㹡ÒÃÃÑ¡ÉÒ
1. Conservative treatment and/or medical treatment
2. Endovascular treatment
3. Surgical treatment
¡ÒÃàÅ×Í¡ÇÔ¸¡ÒÃÃÑ¡ÉÒÇ‹Ò¨Ð㪌Ǹ㴹ѹ¢Ö¹ÍÂÙ¡ºËÅÒ»˜¨¨Ñ ઋ¹
Õ Ô Õ é é ‹ Ñ
1. µíÒá˹‹§¢Í§ÃÍÂâä (Location of pathology)
2. ÅѡɳТͧ¾ÂÒ¸ÔÊÀÒ¾ áÅСÒôíÒà¹Ô¹âä (Pathology and natural history)
3. Hemodynamic cerebral circulation áÅÐ cerebral reserve
4. ¤ÇÒÁàÊÕ§áÅмÅá·Ã¡«ŒÍ¹·ÕÍÒ¨à¡Ô´¢Ö¹¨Ò¡¡ÒÃÃÑ¡ÉÒᵋÅÐÇÔ¸Õ (Risk and benefit of
è è é
treatment option)
5. »ÃÐʺ¡Òó¢Í§á¾·Â¼·Ò¡ÒÃÃÑ¡ÉÒ
ÙŒ í
¡ÒÃÃÑ¡ÉÒ´ŒÇÂÇÔ¸¡ÒÃ㪌ÊÒÂÊǹ·Ò§ËÅÍ´àÅ×Í´ (Endovascular Treatment)
Õ
1. .low preservation procedure ઋ¹ ¡ÒÃãÊ‹ stent ËÃ×Í balloon à¾×ÍÍØ´µíÒá˹‹§¢Í§ÃÍÂÃÑÇ
è è
¢Í§àÊŒ¹àÅ×Í´á´§
2. .low disruption procedure ઋ¹ ¡ÒÃãÊ‹ coil, detachable balloon ËÃ×Í¡ÒÃÍØ´´ŒÇ¡ÒÇ
(glue embolization)
¡ÒÃÃÑ¡ÉÒ´ŒÇÂÇÔ¸¼ÒµÑ´ (Surgical treatment)
Õ ‹
â´Â¨Ðẋ§ÇÔ¸¡ÒÃÃÑ¡ÉÒ໚¹ 2 ÇÔ¸¤Í
Õ Õ ×
1. .low preservation procedure
2. .low disruption procedure without or with flow augmentation procedure
500 Interventional Radiology Management in Traumatic Patient
¼Å¡ÒÃÃÑ¡ÉÒ´ŒÇÂÇԸʹËÅÍ´àÅ×ʹ㹼ٻǷÕÁ¡ÒúҴà¨çº¢Í§äµ¹Ñ¹ä´Œ¼Å´ÕÁÒ¡ã¹»˜¨¨Øº¹
ÕØ Œ † è Õ é Ñ
ÃÒ§ҹ¤ÇÒÁÊíÒàÃ稻ÃÐÁÒ³ 84-100% ÀÒÇÐá·Ã¡«ŒÍ¹·ÕÍÒ¨à¡Ô´¢Ö¹¾ºä´Œ¹Í 䴌ᡋ ÍÒ¡ÒûǴ
(3)
è é Œ
post embolization syndrome ËÃ×ÍÀÒÇСÒâҴàÅ×Í´¢Í§äµ«Ö§â´Â·ÑÇ仼ٻǨÐäÁ‹ÁÍÒ¡ÒÃ
è è Œ † Õ
ÀÂѹµÃÒµ‹ÍÁŒÒÁ (Traumatic splenic injury)
ÁŒÒÁ໚¹ÍÇÑÂÇзվº¡ÒúҴà¨çºä´ŒºÍ¨ҡ¡ÒÃà¡Ô´Íغµà赯 áÅÐà¹×ͧ¨Ò¡à»š¹ÍÇÑÂÇзÕÁàÅ×Í´
è ‹ Ñ Ô è è Õ
ä»àÅÕ§»ÃÔÁÒ³ÁÒ¡ ¡ÒúҴà¨çº·Õà¡Ô´¡ÑºÁŒÒÁ¨Ö§ÁÕ͹µÃÒ¤‹Í¹¢ŒÒ§ÁÒ¡ »˜¨¨Øº¹¡ÒÃÃÑ¡ÉÒà»ÅÕ¹¨Ò¡
é è Ñ Ñ è
¡Òü‹ÒµÑ´ÁÒ໚¹¡ÒÃÃÑ¡ÉÒẺ»ÃФѺ»ÃФͧËÃ×Í¡ÒÃÃÑ¡ÉÒâ´Â¡ÒÃÍØ´ËÅÍ´àÅ×Í´ÁÒ¡¢Ö¹ à¹×ͧ¨Ò¡
é è
¡Òü‹ÒµÑ´ÁŒÒÁÍÍ¡¹Ñ¹·íÒãËŒà¡Ô´ÀÒÇÐá·Ã¡«ŒÍ¹ã¹ÀÒÂËÅѧ¤×ÍÁÕâÍ¡ÒʵԴàª×Í encapsulated Ấ·ÕàÃÕÂ
é é
à¾ÔÁ¢Ö¹
è é
¡ÒõÃǨàÍ¡«àäÍÁ¾ÔÇàµÍÃ㹼ٻǷÕÁÊÒ³ªÕ¾¤§·ÕÊÒÁÒöª‹Çº͡¤ÇÒÁÃعáç,
Œ † è Õ Ñ è
ª¹Ô´áÅеíÒá˹‹§¢Í§¡ÒÃà¡Ô´¾ÂÒ¸ÔÊÀÒ¾ ÃÇÁ·Ñ§ª‹ÇÂÇҧἹ¡ÒÃÃÑ¡ÉÒ ËÒ¡¾º¾ÂÒ¸ÔÊÀҾઋ¹¨Ø´
é
àÅ×Í´ÍÍ¡ ËÃ×ÍËÅÍ´àÅ×ʹ⻆§¾Í§ ¡ç¤ÇÃ䴌ú¡ÒÃÃÑ¡ÉÒâ´Â¡ÒÃÍØ´ËÅÍ´àÅ×Í´ ã¹·Ò§¡ÅѺ¡Ñ¹ã¹¼Ù»ÇÂ
Ñ Œ †
·ÕʧÊÑ¡ÒúҴà¨çº¢Í§ÁŒÒÁáÅÐÁÕÊÒ³ªÕ¾äÁ‹¤§·Õè ઋ¹ÁÕÀÒÇФÇÒÁ´Ñ¹âÅËÔµµèÒ ¤ÇÃ䴌ú¡ÒÃÃÑ¡ÉÒ
è Ñ í Ñ
´ŒÇ¡Òü‹ÒµÑ´·Ñ¹·Õ
ã¹»˜¨¨Øº¹ proximal splenic coil embolization ¶×Í໚¹Áҵðҹ㹡ÒÃÃÑ¡ÉҼٻǷÕÁ¡ÒÃ
Ñ Œ † è Õ
ºÒ´à¨çº¢Í§ÁŒÒÁÍ‹ҧÃعáç·Ñ§ã¹º·ºÒ·¢Í§ preoperative surgical splenectomy áÅСÒÃÃÑ¡ÉÒ
é
ẺäÁ‹µÍ§¼‹ÒµÑ´ ËÅÑ¡¡Òâͧ¡ÒÃÍØ´ËÅÍ´àÅ×ʹẺ¹Õ¹¹ à¹×ͧÁÒ¨Ò¡ ÁŒÒÁ໚¹ÍÇÑÂÇзÕÁÕ collateral
Œ é Ñé è è
504 Interventional Radiology Management in Traumatic Patient
¼Å¡ÒÃÃÑ¡ÉÒ´ŒÇÂÇÔ¸¡ÒÃÍØ´ËÅÍ´àÅ×Í´¹Ñ¹ÍÂÙ·»ÃÐÁÒ³ 85-100%(7) áÅÐÀÒÇÐá·Ã¡«ŒÍ¹·Õà¡Ô´
Õ é ‹ Õè è
¢Ö¹¾ºä´Œ¹Í ઋ¹ non target embolization ËÃ×Í puncture site complication ໚¹µŒ¹
é Œ
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Miller KS, McAninch JW. Radiographic assessment of renal trauma: our 15-year experience. J Urol 1995;
154:352–5.
2. Hagiwara A, Sakaki S, Goto H, et al. The Role of Interventional Radiology in the Management of Blunt Renal
Injury: A Practical Protocol J Trauma. 2001;51:526–31.
3. .lacker R, Paolini RM, Lima S. Management of traumatic hematuria by selective renal artery embolization. J
Urol 1984;132:662-7.
4. Drooz AT, Curtis AL, Allen TE, et al. Quality improvement guidelines for percutaneous transcatheter embolization.
J Vasc Interv Radiol 2004;14:S237-42.
5. Haan JM, Biffl W, Knudson M. Splenic embolization revisited: a multicenter review. J Trauma 2004;56:542-7.
6. .angio P, Asehnoune K, Edouard A, et al. Early embolization and vasopressor administration for management
of life-threatening hemorrhage from pelvic fracture. J Trauma 2005;58:978-84.
7. Teitelbaum GP, Reed RA, Larsen D, et al. Microcatheter embolization of non-neurologic traumatic vascular
lesions. J Vasc Interv Radiol 1993;4:149-54.
8. Michael J. Pentecost. Interventional therapies of hepatic malignancy. In: Stanley Baum, Michael J. Pentecost,
eds. Abrams’ Angiography Interventional radiology. Philadelphia: Lippincott Williams & Wilkins, 2006:516-35.
532.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 505
70
¹Í¹¡Ã¹áÅÐÀÒÇÐËÒÂ㨼Դ»¡µÔ¢³ÐËÅѺª¹Ô´ÍØ´¡Ñé¹
(Snoring and Obstructive Sleep Disordered Breathing; OSDB)
¼ÙŒª‹ÇÂÈÒʵÃÒ¨Òà¹ÒÂá¾·ÂÇÔª ºÃóËÔÃÑ
ÀÒ¤ÇÔªÒâʵ ¹ÒÊÔ¡ ÅÒÃÔ§«Ç·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ÔÔ
¹Í¹¡Ã¹à»š¹ÍÒ¡ÒÃÍ‹ҧ˹֧«Ö§¾ºä´ŒºÍÂÁÒ¡áÅÐà¡Ô´¢Ö¹ä´Œã¹·Ø¡à¾È ·Ø¡ÇÑ àÊÕ§¡Ã¹à¡Ô´
è è ‹ é
¨Ò¡¡Ò÷ÕÅÁËÒÂ㨡íÒÅѧà¤Å×͹¼‹Ò¹·Ò§à´Ô¹ËÒÂã¨Ê‹Ç¹µŒ¹·Õµºá¤ºÅ§ ã¹ÅѡɳзÕ໚¹ turbulent flow
è è è Õ è
áÅзíÒãËŒà¡Ô´¡ÒÃÊѹÊÐà·×͹¢Í§à¹×ÍàÂ×ÍÃͺ¢ŒÒ§ â´ÂµíÒá˹‹§·Õ᤺¢Í§·Ò§à´Ô¹ËÒÂ㨠ÍÒ¨àÃÔÁµÑ§áµ‹
è é è è è é
¨ÁÙ¡ (nasal cavity) â¾Ã§ËÅѧ¨ÁÙ¡ (nasopharynx) ྴҹ͋͹ (soft palate) ¤ÍËÍ (oropharynx)
µ‹ÍÁ·ÍÅ«Ô¹ (tonsils) ⤹ÅÔ¹ (base of tongue) ¨¹¶Ö§ºÒ§Ê‹Ç¹¢Í§¡Å‹Í§àÊÕ§ (larynx) ·Ñ§¹ÕàÊÕ§¡Ã¹
é é é
¹Í¡¨Ò¡¨Ð¡‹ÍãËŒà¡Ô´¤ÇÒÁÃíÒ¤ÒÍ‹ҧÁÒ¡ ¡Ñº¤Ù¹Í¹ ËÃ×ͼٷ¾¡ÍÒÈÑÂËÇÁ´ŒÇ ÂѧÍҨ໚¹ÍÒ¡ÒÃáÊ´§
‹ Œ Õè Ñ
(sign) ·ÕÊÒ¤ÑÍ‹ҧ˹֧¢Í§¡ÅØÁâäÀÒÇÐËÒÂ㨼Դ»¡µÔ¢³ÐËÅѺª¹Ô´ÍØ´¡Ñ¹ (obstructive sleep-
èí è ‹ é
disordered breathing; OSDB) â´Ââä¡ÅØ‹Á¹ÕéËÒ¡àÃÕ§µÒÁÅíҴѺ¤ÇÒÁÃعáç¨Ò¡¹ŒÍÂä»ÁÒ¡
¨Ð»ÃСͺ´ŒÇ ÀÒÇй͹¡Ã¹¸ÃÃÁ´Ò (primary snoring), ¡ÅØÁÍÒ¡Òèҡ·Ò§à´Ô¹ËÒÂã¨Ê‹Ç¹µŒ¹µÕº
‹
᤺ (upper airway resistance syndrome; UARS) ¡ÅØÁÍÒ¡ÒÃËÂØ´ËÒÂ㨢³ÐËÅѺª¹Ô´ÍØ´¡Ñ¹
‹ é
(obstructive sleep apnea (OSA) ËÃ×Í obstructive sleep apnea hypopnea syndrome; OSAHS)
áÅкҧ¤Ãѧ ÍÒ¨¨Ñ´ obesity hypoventilation (Pickwickian) syndrome ÃÇÁÍÂÙ´ÇÂ(1)
é ‹ Œ
514 ¹Í¹¡Ã¹áÅÐÀÒÇÐËÒÂ㨼Դ»¡µÔ¢³ÐËÅѺª¹Ô´ÍØ´¡Ñ¹
é
3.2.1 ¡ÒÃʋͧ¡ÅŒÍ§ÀÒÂã¹·Ò§à´Ô¹ËÒÂã¨Ê‹Ç¹µŒ¹ (Upper airway endoscopy) ÊÒÁÒö
㪌䴌·§ flexible ËÃ×Í rigid endoscope â´Â·íÒã¹¢³Ð·Õ¼»ÇÂÍÂÙã¹·‹Ò¹Ñ§ËÃ×Í·‹Ò¹Í¹¡çä´Œ ¹Í¡¨Ò¡
Ñé è ÙŒ † ‹ è
¹Õ§ÍÒ¨µÃǨ㹼ٻǺҧÃÒ¢³Ð·ÕËÅѺ (sleep endoscopy) «Ö§¨Ðä´Œ¢ÍÁÙÅ·Õ໚¹¶Ù¡µŒÍ§ÁÒ¡¢Ö¹(31)
é Ñ Œ † è è Œ è é
3.2.2 ¡Òö‹ÒÂÀÒ¾ÃѧÊÕ (X-ray) ºÃÔàdz¡ÐâËÅ¡ÈÕÃÉРઋ¹ film lateral skull, lateral
cephalometry, ËÃ×Í panoramic view à¾×Í´Ùâ¤Ã§ÊÌҧ¡Ãд١ãºË¹ŒÒ ¢Ò¡ÃÃä¡Ã áÅÐà¹×ÍàÂ×ͧ͢·Ò§
è é è
à´Ô¹ËÒÂã¨Ê‹Ç¹º¹ ઋ¹ »ÃÐàÁÔ¹¢¹Ò´¢Í§µ‹ÍÁ adenoid ËÃ×Í¡ÒÃÇҧἹ¼‹ÒµÑ´ºÃÔàdz¢Ò¡ÃÃä¡Ã
(jaw surgery) ໚¹µŒ¹
3.2.3 ¡ÒõÃǨ¾ÔàÈÉÍ×¹ æ ઋ¹ CT scan, MRI, fluoroscopy of airway ËÃ×Í acoustic
è
analysis »˜¨¨Øº¹Âѧ㪌ã¹à¾×ͧҹÇÔ¨Â໚¹ËÅÑ¡ ᵋäÁ‹¹ÂÁ㪌㹷ҧ»¯ÔºµÔ(32)
Ñ è Ñ Ô Ñ
3.3 ¡ÒõÃǨËÒâäµÒÁÃкº (Systemic assessment)
à¾×ÍËÒâäËÇÁáÅлÃÐàÁÔ¹ÀÒÇÐá·Ã¡«ŒÍ¹¨Ò¡ OSA ËÃ×Íà¾×ÍàµÃÕÂÁ¡Òü‹ÒµÑ´ ·Ñ§¹Õé
è è é
¤ÇþԨÒóÒÊ‹§µÃǨ 㹡óշʧÊÑÂ໚¹ÃÒÂæ ä» àª‹¹ ¡ÒõÃǨ CBC (complete blood count)
Õè
à¾×Í´ÙÀÒÇÐ polycythemia ¡Òö‹ÒÂÀÒ¾ x-ray ·Ãǧ͡à¾×Í»ÃÐàÁÔ¹ÀÒÇÐ right heart failure ËÃ×Í
è è
cor pulmonale ¡ÒõÃǨ arterial blood gas áÅСÒõÃǨà¡ÕÂǡѺµ‹ÍÁä¸ÃÍ´ ઋ¹ thyroid
è
function test ໚¹µŒ¹
¡ÒÃÃÑ¡ÉÒ
á¹Ç·Ò§¡ÒÃÃÑ¡ÉҼٻǷÕÁÀÒÇÐËÒÂ㨼Դ»¡µÔ¢³ÐËÅѺª¹Ô´ÍØ´¡Ñ¹¹Ñ¹ ¢Ö¹ÍÂÙ¡ºËÅÒ»˜¨¨ÑÂ
Œ † è Õ é é é ‹ Ñ
ઋ¹ ÊÒà˵ØáÅФÇÒÁÃعáç¢Í§âä ¤ÇÒÁµŒÍ§¡ÒÃáÅФÇÒÁËÇÁÁ×ͧ͢¼Ù»Ç µÅÍ´¨¹ ¢ŒÍ´Õ¢ÍàÊÕÂ
Œ † Œ
ËÃ×Í¢ŒÍ¨íÒ¡Ñ´¢Í§¡ÒÃÃÑ¡ÉÒᵋÅÐẺ ´Ñ§¹Ñ¹¡‹Í¹¡ÒõѴÊÔ¹ã¨àÅ×Í¡ÇÔ¸¡ÒÃÃÑ¡ÉÒ á¾·ÂáÅмٻǤÇÃ
é Õ Œ †
ÁÕ¡ÒþԨÒóÒËÇÁ¡Ñ¹ â´Â¼Ù»Ç¤ÇÃ䴌ú¤íÒá¹Ð¹íÒà¾×ÍãËŒµÃÐ˹ѡ¶Ö§ÍѹµÃÒµ‹Ò§æ ·ÕÍÒ¨à¡Ô´¢Ö¹
Œ † Ñ è è é
¨Ò¡âä¹ÕéËÒ¡»Å‹Í·Ôé§äÇŒ Í‹ҧäáçµÒÁËÒ¡ÊÒÁÒöàÅ×Í¡¡ÒÃÃÑ¡ÉÒ䴌͋ҧ¶Ù¡µŒÍ§áÅÐàËÁÒÐÊÁ
¨Ðª‹ÇÂãˌ͵ÃÒ¡ÒÃàÊÕªÕǵ¡‹Í¹àÇÅÒÍѹ¤ÇÃŴŧ áÅзíÒãËŒ¤³ÀÒ¾ªÕǵ¢Í§·Ñ§¼Ù»Ç´բ¹
Ñ Ô Ø Ô é Œ † Öé
â´Â·ÑÇä» àÃÒ¹ÔÂÁẋ§¡ÒÃÃÑ¡ÉÒÍ͡໚¹ËÅÒ¡ÅØÁ ´Ñ§¹Õé
è ‹
1. ¡ÒÃÃÑ¡ÉÒẺ͹ØÃÑ¡É (Conservative treatment)
¡ÒÃÃÑ¡ÉÒ¡ÅØÁ¹Õ¤ÇÃ໚¹¾×¹°Ò¹·ÕÊÒ¤ÑÊíÒËÃѺ¼Ù»Ç·ءÃÒ äÁ‹ÇÒ¨ÐÁÕ¤ÇÒÁÃعáçÃдѺ
‹ é é èí Œ † ‹
ã´ ¨Ø´»ÃÐʧ¤ ËÅÑ¡¢Í§¡ÒÃÃÑ¡ÉÒ´ŒÇÂÇÔ¸¹Õé ¨Ð์¹à¡ÕÂǡѺ¡Òû¯Ôºµàº×ͧµŒ¹¢Í§¼Ù»ÇÂàͧ µÑÇÍ‹ҧ
Õ è Ñ Ô é Œ †
·ÕÊÒ¤Ñ àª‹¹
èí
1.1 ¡ÒÃÅ´¹éÒ˹ѡ (Weight reduction) àËÁÒÐÊíÒËÃѺ¼Ù·Íǹ (obesity) ËÃ×Í ¼Ù·ÁÕ
í Œ Õè Œ Œ Õè
¹éÒ˹ѡà¡Ô¹ (overweight) «Ö§¨Ðª‹ÇÂÅ´¤ÇÒÁÃعáç¢Í§âäŧ䴌 à¹×ͧ¨Ò¡¡ÒÃÅ´¹éÒ˹ѡ¨Ðª‹ÇÂÅ´
í è (33)
è í
»ÃÔÁÒµÃà¹×ÍàÂ×Íä¢Áѹ (fatty tissue) 㹺ÃÔàdz·Ò§à´Ô¹ËÒÂã¨Ê‹Ç¹º¹ áÅÐ ª‹ÇÂãËŒÃкº¡ÒÃËÒÂã¨
é è
â´ÂÃÇÁ´Õ¢Öé¹ ·Ñ駹ÕéÇÔ¸Õ¡Ò÷Õèä´ŒÊíҤѷÕèÊØ´ÊíÒËÃѺ¼Å´Õã¹ÃÐÂÐÂÒÇ µŒÍ§ÍÒÈѤÇÒÁµÑé§ã¨¨Ãԧ㹡ÒÃ
à»ÅÕè¹ÃٻẺ¡ÒÃ㪌ªÕÇÔµ (life style change) ·Ñ駡ÒäǺ¤ØÁÍÒËÒà ÃÇÁ¶Ö§ ¡ÒÃÍÍ¡¡íÒÅѧ¡ÒÂ
·ÕàËÁÒÐÊÁ ໚¹µŒ¹
è
520 ¹Í¹¡Ã¹áÅÐÀÒÇÐËÒÂ㨼Դ»¡µÔ¢³ÐËÅѺª¹Ô´ÍØ´¡Ñ¹
é
7. Teloken PE, Smith EB, Lodowsky C, .reedom T, Mulhall JP. Defining association between sleep apnea
syndrome and erectile dysfunction. Urology. 2006;67(5):1033-7.
8. Capdevila OS, Kheirandish-Gozal L, Dayyat E, Gozal D. Pediatric obstructive sleep apnea: complications,
management, and long-term outcomes. Proceedings of the American Thoracic Society. 2008;5(2):274-82.
9. Lugaresi E C., Coccagna G, Baruzzi A. . Snoring and the obstructive apnea syndrome. Electroencephalogr
Clin Neurophysiol (Suppl) 1982;35:421-30.
10. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing
among middle-aged adults. N Engl J Med. 1993;328(17):1230-5.
11. Schechter MS. Technical report: diagnosis and management of childhood obstructive sleep apnea syndrome.
Pediatrics. 2002;109(4):e69.
12. Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):242-
52.
13. Wanaporn Anuntaseree M, Korpong Rookkapan M, Surachai Kuasirikul M, Paramee Thongsuksai M. Snoring
and obstructive sleep apnea in Thai school-age children: Prevalence and predisposing factors Pediatric
Pulmonology 32 ( 3):222 - 7
14. Silber MH, Ancoli-Israel S, Bonnet MH, Chokroverty S, Grigg-Damberger MM, Hirshkowitz M, et al. The visual
scoring of sleep in adults. J Clin Sleep Med. 2007;3(2):121-31.
15. Carskadon MA DW. Normal human sleep: an overview. Kryer MH, Roth T, Dement WC, eds Principles and
practice of sleep medicine, 4th ed Philadelphia: WB Saunders,2005:16-28.
16. .ogel RB MA, White DP. Sleep. 2: pathophysiology of obstructive sleep apnoea/hypopnoea syndrome.
Thorax 2004;59(2):159-63.
17. Schwab RJ, Gupta KB, Gefter WB, Metzger LJ, Hoffman EA, Pack AI. Upper airway and soft tissue anatomy
in normal subjects and patients with sleep-disordered breathing. Significance of the lateral pharyngeal walls.
Am J Respir Crit Care Med. 1995;152(5 Pt 1):1673-89.
18. Akay M, Leiter JC, Daubenspeck JA. Reduced respiratory-related evoked activity in subjects with obstructive
sleep apnea syndrome. J Appl Physiol. 2003;94(2):429-38.
19. Durmer JS, Dinges D.. Neurocognitive consequences of sleep deprivation. Semin Neurol. 2005;25(1):117-29.
20. Engleman H, Joffe D. Neuropsychological function in obstructive sleep apnoea. Sleep Med Rev. 1999;3(1):59-
78.
21. Hamilton GS, Solin P, Naughton MT. Obstructive sleep apnoea and cardiovascular disease. Internal medicine
journal. 2004;34(7):420-6.
22. Golbin JM, Somers VK, Caples SM. Obstructive sleep apnea, cardiovascular disease, and pulmonary
hypertension. Proceedings of the American Thoracic Society. 2008;5(2):200-6.
23. Piccirillo J. TS. Sleep-disordered breathing. In: Cummings Otolaryngology Head & Neck Surgery, 3rd ed St
Louis: Mosby-Year Book. 1998:1546-71.
24. Peng B, Li SW, Kang H, Huang XZ. Cognitive and emotional impairment in obstructive sleep apnea syndrome.
Chinese medical sciences journal = Chung-kuo i hsueh k’o hsueh tsa chih / Chinese Academy of Medical
Sciences. 2004;19(4):262-5.
25. Greene MG, Carroll JL. Consequences of sleep-disordered breathing in childhood. Curr Opin Pulm Med.
1997;3(6):456-63.
26. Owens JA. Neurocognitive and behavioral impact of sleep disordered breathing in children. Pediatric pulmonology.
2009;44(5):417-22.
27. Kushida CA, Littner MR, Morgenthaler T, Alessi CA, Bailey D, Coleman J, Jr., et al. Practice parameters for
the indications for polysomnography and related procedures: an update for 2005. Sleep. 2005;28(4):499-521.
548.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 521
28. Ruehland WR, Rochford PD, O’Donoghue .J, Pierce RJ, Singh P, Thornton AT. The new AASM criteria for
scoring hypopneas: impact on the apnea hypopnea index. Sleep. 2009;32(2):150-7.
29. Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques
in clinical research. The Report of an American Academy of Sleep Medicine Task .orce. Sleep. 1999;22(5):667-
89.
30. Redline S, Budhiraja R, Kapur V, Marcus CL, Mateika JH, Mehra R, et al. The scoring of respiratory events
in sleep: reliability and validity. J Clin Sleep Med. 2007 15;3(2):169-200.
31. Thakkar K, Yao M. Diagnostic studies in obstructive sleep apnea. Otolaryngol Clin North Am. 2007;40(4):785-
805.
32. Stuck BA, Maurer JT. Airway evaluation in obstructive sleep apnea. Sleep Med Rev. 2008;12(6):411-36.
33. Newman AB, .oster G, Givelber R, Nieto .J, Redline S, Young T. Progression and regression of sleep-
disordered breathing with changes in weight: the Sleep Heart Health Study. Arch Intern Med. 2005;165(20):2408-
13.
34. Penzel T, Moller M, Becker H., Knaack L, Peter JH. Effect of sleep position and sleep stage on the
collapsibility of the upper airways in patients with sleep apnea. Sleep. 2001;24(1):90-5.
35. Peppard PE, Austin D, Brown RL. Association of alcohol consumption and sleep disordered breathing in men
and women. J Clin Sleep Med. 2007;3(3):265-70.
36. Stewart MG. Identification and management of undiagnosed and undertreated allergic rhinitis in adults and
children. Clin Exp Allergy. 2008;38(5):751-60.
37. Morgenthaler TI KS, Lee-Chiong T, Alessi C, Boehlecke B, Brown T, Coleman J, .riedman L, Kapur V, Owens
J, Pancer J, Swick T; Standards of Practice Committee; American Academy of Sleep Medicine. Practice
parameters for the medical therapy of obstructive sleep apnea. Sleep. 2006;29(8):1031-5.
38. Kushida CA, Littner MR, Hirshkowitz M, Morgenthaler TI, Alessi CA, Bailey D, et al. Practice parameters for
the use of continuous and bilevel positive airway pressure devices to treat adult patients with sleep-related
breathing disorders. Sleep. 2006;29(3):375-80.
39. Pepin JL, Leger P, Veale D, Langevin B, Robert D, Levy P. Side effects of nasal continuous positive airway
pressure in sleep apnea syndrome. Study of 193 patients in two .rench sleep centers. Chest. 1995;107(2):375-
81.
40. Kushida CA, Morgenthaler TI, Littner MR, Alessi CA, Bailey D, Coleman J, Jr., et al. Practice parameters for
the treatment of snoring and Obstructive Sleep Apnea with oral appliances: an update for 2005. Sleep.
2006;29(2):240-3.
41. Powell NB, Zonato AI, Weaver EM, Li K, Troell R, Riley RW, et al. Radiofrequency treatment of turbinate
hypertrophy in subjects using continuous positive airway pressure: a randomized, double-blind, placebo-controlled
clinical pilot trial. The Laryngoscope. 2001;111(10):1783-90.
42. Zeng B NA, Qian J, Petocz P, Darendeliler MA, Cistulli PA. Influence of nasal resistance on oral appliance
treatment outcome in obstructive sleep apnea. Sleep. 2008;31(4):543-7.
43. Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics.
2002;109(4):704-12.
44. Mitchell RB, Kelly J, Call E, Yao N. Long-term changes in quality of life after surgery for pediatric obstructive
sleep apnea. Archives of otolaryngology—head & neck surgery. 2004;130(4):409-12.
45. Woodson BT, Robinson S, Lim HJ. Transpalatal advancement pharyngoplasty outcomes compared with
uvulopalatopharygoplasty. Otolaryngol Head Neck Surg. 2005;133(2):211-7.
46. Powell N, Riley R, Guilleminault C, Troell R. A reversible uvulopalatal flap for snoring and sleep apnea
syndrome. Sleep. 1996;19(7):593-9.
549.
522 ¹Í¹¡Ã¹áÅÐÀÒÇÐËÒÂ㨼Դ»¡µÔ¢³ÐËÅѺª¹Ô´ÍØ´¡Ñ¹
é
47. Pang KP, Tan R, Puraviappan P, Terris DJ. Anterior palatoplasty for the treatment of OSA: three-year results.
Otolaryngol Head Neck Surg. 2009;141(2):253-6.
48. .riedman M, Ibrahim H, Joseph NJ. Staging of obstructive sleep apnea/hypopnea syndrome: a guide to
appropriate treatment. The Laryngoscope. 2004;114(3):454-9.
49. .erguson KA, Heighway K, Ruby RR. A randomized trial of laser-assisted uvulopalatoplasty in the treatment of
mild obstructive sleep apnea. Am J Respir Crit Care Med. 2003;167(1):15-9.
50. Pang KP, Terris DJ. Modified cautery-assisted palatal stiffening operation: new method for treating snoring and
mild obstructive sleep apnea. Otolaryngol Head Neck Surg. 2007;136(5):823-6.
51. Rombaux P, Hamoir M, Bertrand B, Aubert G, Liistro G, Rodenstein D. Postoperative pain and side effects
after uvulopalatopharyngoplasty, laser-assisted uvulopalatoplasty, and radiofrequency tissue volume reduction
in primary snoring. The Laryngoscope. 2003;113(12):2169-73.
52. Back LJ, Hytonen ML, Roine RP, Malmivaara AO. Radiofrequency ablation treatment of soft palate for
patients with snoring: a systematic review of effectiveness and adverse effects. The Laryngoscope.
2009;119(6):1241-50.
53. Kezirian EJ, Powell NB, Riley RW, Hester JE. Incidence of complications in radiofrequency treatment of the
upper airway. The Laryngoscope. 2005;115(7):1298-304.
54. Porter MW, Hales NW, Nease CJ, Krempl GA. Long-term results of inferior turbinate hypertrophy with
radiofrequency treatment: a new standard of care? The Laryngoscope. 2006;116(4):554-7.
55. Woodson BT, Steward DL, Weaver EM, Javaheri S. A randomized trial of temperature-controlled radiofrequency,
continuous positive airway pressure, and placebo for obstructive sleep apnea syndrome. Otolaryngol Head
Neck Surg. 2003;128(6):848-61.
56. Kezirian EJ, Goldberg AN. Hypopharyngeal surgery in obstructive sleep apnea: an evidence-based medicine
review. Archives of otolaryngology—head & neck surgery. 2006;132(2):206-13.
57. Lin HC, .riedman M, Chang HW, Gurpinar B. The efficacy of multilevel surgery of the upper airway in adults
with obstructive sleep apnea/hypopnea syndrome. The Laryngoscope. 2008;118(5):902-8.
58. Bowden MT, Kezirian EJ, Utley D, Goode RL. Outcomes of hyoid suspension for the treatment of obstructive
sleep apnea. Archives of otolaryngology—head & neck surgery. 2005;131(5):440-5.
59. Zafereo ME, Taylor RJ, Pereira KD. Supraglottoplasty for laryngomalacia with obstructive sleep apnea. The
Laryngoscope. 2008;118(10):1873-7.
60. Li KK, Powell NB, Riley RW, Troell RJ, Guilleminault C. Long-Term Results of Maxillomandibular Advancement
Surgery. Sleep Breath. 2000;4(3):137-40.
61. Li KK, Riley RW, Powell NB, Guilleminault C. Patient’s perception of the facial appearance after maxillomandibular
advancement for obstructive sleep apnea syndrome. J Oral Maxillofac Surg. 2001;59(4):377-80; discussion
80-1.
62. Kezirian EJ, Weaver EM, Yueh B, Deyo RA, Khuri S., Daley J, et al. Incidence of serious complications after
uvulopalatopharyngoplasty. The Laryngoscope. 2004;114(3):450-3.
63. Chung SA, Yuan H, Chung .. A systemic review of obstructive sleep apnea and its implications for
anesthesiologists. Anesthesia and analgesia. 2008;107(5):1543-63.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 527
! Modafinil ÂÒµÑǹÕé㪌¡Ñ¹á¾Ã‹ËÅÒ ¡Åä¡¡ÒÃÍÍ¡Ä·¸Ôì¤Ô´Ç‹Ò¹‹Ò¨Ðà¡Ô´¨Ò¡¡ÒÃà¾ÔèÁ
dopamine áÅÐ norepinephine ¢ŒÍ´Õ¤ÍäÁ‹Ãº¡Ç¹¡Òù͹µÍ¹¡ÅÒ§¤×¹áÅÐÂѺÂѧ
× é
REM sleep ·Õ¨ÐࢌÒÊ٪ǧµ×¹ä´Œ´Õ »˜¨¨Øº¹ÂѧäÁ‹ÁÂÒ¹Õã¹»ÃÐà·Èä·Â
è ‹ ‹ è Ñ Õ é
¢. ¡ÒÃÃÑ¡ÉÒ cataplexy (43-44)
! Tricyclic antidepressants áÅÐ selective serotonin reuptake inhibitor (SSRI)
! Sodium oxybate ໚¹ÂÒ·Õ໚¹ÃѺÃͧâ´Âͧ¤¡Òà .DA ã¹ÊËÃÑ°ÍàÁÃÔ¡ÒÃ㹡ÒÃÃÑ¡ÉÒ
è
cataplexy ÂѧäÁ‹Á¨Ò˹‹ÒÂã¹»ÃÐà·Èä·Â
Õí
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Zeman, A, Britton, T, Douglas, N, et al. Narcolepsy and excessive daytime sleepiness. BMJ 2004; 329:724.
2. Broughton R, Mullington J. Chronobiological aspects of narcolepsy. Sleep 1994;17(8suppl.):s35-44.
3. Hublin C, Partinen M, Kaprio J, et al. Epidemiology of narcolepsy. Sleep 1994;17(Suppl.):S7-12.
4. Silber MH, Krahn LE, Olson EJ, et al. The epidemiology of narcolepsy in Olmstead County, Minnesota: a
population based study. Sleep 2002;25:197-202.
5. Mignot E. Genetic and familial aspects of narcolepsy. Neurology 1998;50(Suppl.):S54-S59.
6. Honda Y. Census of narcolepsy, cataplexy and sleep life among teenagers in .ujisawa city. Sleep Res
1979;8:191.
7. Tashiro T, Kanbayashi T, Hishikawa Y. An epidemiological study of narcolepsy in Japanese. Ann Neurol
1994;35:709-716.
8. Longstreth, WT Jr, Koepsell, TD, Ton, TG, et al. The epidemiology of narcolepsy. Sleep 2007; 30:13.
9. Ohayon, MM, Priest, RG, Zulley, J, et al. Prevalence of narcolepsy symptomatology and diagnosis in the
European general population. Neurology 2002;58:1826.
10. Coleman, RM, et al. Sleep-wake disorders based on a polysomnographic diagnosis. A national cooperative
study. JAMA 1982;247:997.
11. Silber, MH, Krahn, LE, Olson, EJ, Pankratz, VS. The epidemiology of narcolepsy in Olmsted County, Minnesota:
a population-based study. Sleep 2002;25:197.
12. Okun, ML, Lin, L, Pelin, Z, et al. Clinical aspects of narcolepsy-cataplexy across ethnic groups. Sleep 2002;
25:27.
13. Billiard M, Pasquie-Magnetto V, Heckman M, et al. .amily studies in narcolepsy. Sleep 1994;17(Suppl.):S54-59.
14. Mignot E. Genetics of narcolepsy and other sleep disorders. Am J Hum Genet. Jun 1997;60(6):1289-302.
15. Sakurai, T, Amemiya, A, Ishii, M, et al. Orexins and orexin receptors: a family of hypothalamic neuropeptides
and G protein-coupled receptors that regulate feeding behavior. Cell 1998;92:573.
16. de Lecea, L, Kilduff, TS, Peyron, C, et al. The hypocretins: hypothalamus-specific peptides with neuroexcitatory
activity. Proc Natl Acad Sci USA 1998;95:322.
17. Hagan, JJ, Leslie, RA, Patel, S, et al. Orexin A activates locus coeruleus cell firing and increases arousal in the
rat. Proc Natl Acad Sci USA 1999;96:10911.
18. Bayer, L, Eggermann, E, Serafin, M, et al. Orexins (hypocretins) directly excite tuberomammillary neurons. Eur
J Neurosci 2001;14:1571.
19. Yamanaka, A, Tsujino, N, .unahashi, H, et al. Orexins activate histaminergic neurons via the orexin 2
receptor. Biochem Biophys Res Commun 2002;290:1237.
555.
528 Narcolepsy
20. Eriksson, KS, Sergeeva, O, Brown, RE, Haas, HL. Orexin/hypocretin excites the histaminergic neurons of the
tuberomammillary nucleus. J Neurosci 2001;21:9273.
21. Brown, RE, Sergeeva, O, Eriksson, KS, Haas, HL. Orexin A excites serotonergic neurons in the dorsal raphe
nucleus of the rat. Neuropharmacology 2001;40:457.
22. Saper, CB, Chou, TC, Scammell, TE. The sleep switch: hypothalamic control of sleep and wakefulness.
Trends Neurosci 2001;24:726.
23. Scammell, TE. The neurobiology, diagnosis, and treatment of narcolepsy. Ann Neurol 2003;53:154.
24. Dauvilliers, Y, Baumann, CR, Carlander, B, et al. CS. hypocretin-1 levels in narcolepsy, Kleine-Levin syndrome,
and other hypersomnias and neurological conditions. J Neurol Neurosurg Psychiatry 2003;74:1667.
25. Mignot, E, Lammers, GJ, Ripley, B, et al. The role of cerebrospinal fluid hypocretin measurement in the
diagnosis of narcolepsy and other hypersomnias. Arch Neurol 2002;59:1553.
26. Nishino, S, et al. Hypocretin (orexin) deficiency in human narcolepsy. Lancet 2000;355:39.
27. Kanbayashi, T, Inoue, Y, Chiba, S, et al. CS. hypocretin-1 (orexin-A) concentrations in narcolepsy with and
without cataplexy and idiopathic hypersomnia. J Sleep Res 2002;11:91.
28. Dalal, MA, Schuld, A, Haack, M, et al. Normal plasma levels of orexin A (hypocretin-1) in narcoleptic patients.
Neurology 2001;56:1749.
29. Peyron, C, .araco, J, Rogers, W, et al. A mutation in a case of early onset narcolepsy and a generalized
absence of hypocretin peptides in human narcoleptic brains. Nat Med 2000;6:991.
30. Thannickal, T, et al. Reduced number of hypocretin neurons in human narcolepsy. Neuron 2000;27:469.
31. Crocker, A, Espana, RA, Papadopoulou, M, et al. Concomitant loss of dynorphin, NARP, and orexin in
narcolepsy. Neurology 2005;65:1184.
32. Erlich, SS, Itabashi, HH. Narcolepsy: A neuropathologic study. Sleep 1986;9:126.
33. Broughton, R, Dunham, W, Newman, J, et al. Ambulatory 24 hour sleep-wake monitoring in narcolepsy-
cataplexy compared to matched controls. Electroencephalogr Clin Neurophysiol 1988;70:473.
34. Dantz, B, Edgar, DM, Dement, WC. Circadian rhythms in narcolepsy: studies on a 90 minute day.
Electroencephalogr Clin Neurophysiol 1994;90:24.
35. Guilleminault, C, Gelb, M. Clinical aspects and features of cataplexy. Adv Neurol 1995;67:65.
36. Anic-Labat, S, Guilleminault, C, Kraemer, HC, et al. Validation of a cataplexy questionnaire in 983 sleep-
disorders patients. Sleep 1999;22:77.
37. American Academy of Sleep Medicine. International classification of sleep disorders, second edition: Diagnostic
and coding manual. Westchester, IL American Academy of Sleep Medicine, 2005.
38. Rogers, AE, Aldrich, MS, Lin, X. A comparison of three different sleep schedules for reducing daytime
sleepiness in narcolepsy. Sleep 2001;24:385.
39. Mullington, J, Broughton, R. Scheduled naps in the management of daytime sleepiness in narcolepsy-cataplexy.
Sleep 1993;16:444.
40. Mitler, MM, et al. Narcolepsy and its treatment with stimulants. ASDA standards of practice. Sleep 1994;17:352.
41. Boivin, DB, Montplaisir, J, Petit, D, et al. Effects of modafinil on symptomatology of human narcolepsy. Clin
Neuropharmacol 1993;16:46.
42. Mitler, MM, Hajdukovic, R, Erman, MK. Treatment of narcolepsy with methamphetamine. Sleep 1993; 16:306.
43. Vignatelli, L, D’Alessandro, R, Candelise, L. Antidepressant drugs for narcolepsy. Cochrane Database Syst
Rev 2005;CD003724.
44. Tunnicliff, G. Sites of action of gamma-hydroxybutyrate (GHB)—a neuroactive drug with abuse potential. J
Toxicol Clin Toxicol 1997;35:581.
556.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 529
72
Surgical Treatment for Sleep Disordered Breathing
¼ÙŒª‹ÇÂÈÒʵÃÒ¨Òà¹ÒÂá¾·ÂÇÔª ºÃóËÔÃÑ
ÀÒ¤ÇÔªÒâʵ ¹ÒÊÔ¡ ÅÒÃÔ§«Ç·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ÔÔ
»˜¨¨Øº¹·Ò§àÅ×͡㹡ÒÃÃÑ¡Éҹ͹¡Ã¹áÅÐÀÒÇÐËÂØ´ËÒÂ㨢³ÐËÅѺª¹Ô´ÍØ´¡Ñ¹ (obstructive
Ñ é
sleep apnea : OSA) ÁÕÍÂ٤͹¢ŒÒ§ÁÒ¡ ¡ÒõѴÊÔ¹ã¨àÅ×Í¡ÇԸáÉҹѹ¢Ö¹ÍÂÙ¡ºËÅÒ»˜¨¨Ñ ઋ¹ ¤ÇÒÁ
‹ ‹ ÕÑ é é ‹ Ñ
ÃعáçáÅÐÊÒà˵ط໚¹ä»ä´Œ¢Í§âä ¤ÇÒÁµŒÍ§¡Òâͧ¼Ù»Ç µÅÍ´¨¹¢ŒÍ´Õ ¢ŒÍàÊÕ ËÃ×Í¢ŒÍ¨íÒ¡Ñ´¢Í§
Õè Œ †
¡ÒÃÃÑ¡ÉÒᵋÅÐẺ 㹡óշ¼»ÇÂ໚¹à¾Õ§ÀÒÇй͹¡Ã¹¸ÃÃÁ´Ò (primary snoring) ¡ÒÃÃÑ¡ÉÒ
Õè ÙŒ †
·Õ¹ÂÁÁѡ໚¹áººÍ¹ØÃ¡É (conservative treatment) ઋ¹ ¡ÒÃÅ´¹éÒ˹ѡ ¡ÒûÃѺÊآ͹ÒÁÑ¡ÒÃ
è Ô Ñ í
¹Í¹ (sleep hygiene) ¡ÒÃËÅÕ¡àÅÕ§ÂÒºÒ§ª¹Ô´ ઋ¹ Âҹ͹ËÅѺ ËÃ×Íà¤Ã×ͧ´×Á·Õ¼ÊÁáÍÅ¡ÍÎÍÅ
è è è è
áÅÐÃÑ¡ÉÒâäËÇÁ·Õ¾ºä´ŒºÍ ઋ¹ àÂ×ͺبÁÙ¡ÍÑ¡àʺ¨Ò¡ÀÙÁᾌ ໚¹µŒ¹ ËÃ×Í㹡óշ¼»ÇÂÁÕÀÒÇÐ
è ‹ è Ô Õè ÙŒ †
ËÂØ´ËÒÂ㨢³ÐËÅѺª¹Ô´ÍØ´¡Ñé¹ (OSA) ¡ÒÃ㪌à¤Ã×èͧÊÌҧ¤ÇÒÁ´Ñ¹ÅÁºÇ¡à¾×èÍà»´¢ÂÒ·ҧà´Ô¹
ËÒÂ㨠(continuous positive airway pressure therapy : CPAP) ¨Ñ´Ç‹Ò໚¹ÇԸáÉÒÁҵðҹ·ÕÁÕ ÕÑ è
»ÃÐÊÔ·¸ÔÀÒ¾áÅÐÁÕ¤ÇÒÁ»ÅÍ´ÀÑÂÊÙ§ µÃҺ෋ҷռ»ÇÂÊÒÁÒö㪌à¤Ã×ͧ䴌µÅÍ´·Ø¡¤×¹ Í‹ҧäáçµÒÁ
è ÙŒ † è
¡ÒÃÃÑ¡ÉÒẺµ‹Ò§ æ ¢ŒÒ§µŒ¹ÍÒ¨ÁբͨíÒ¡Ñ´ÍÂÙäÁ‹¹Í ઋ¹ ¼Ù»Ç·չ͹¡Ã¹´Ñ§ÁÒ¡áÁŒÇÒ¨Ð໚¹à¾Õ§
Œ ‹ Œ Œ † è ‹
ÀÒÇСù¸ÃÃÁ´Ò ÍÒ¨ÃÑ¡ÉÒäÁ‹ä´Œ¼Å´ŒÇÂÇÔ¸ÕẺ͹ØÃÑ¡É ËÃ×͡óշÕè¼ÙŒ»†ÇÂÁÕ¢ŒÍº‹§ªÕé㹡ÒÃ㪌
à¤Ã×èͧ CPAP ¡çÂѧÁÕ¼ÙŒ»†Ç¨íҹǹäÁ‹¹ŒÍ ·Õ軯Ôàʸ¡ÒÃ㪌à¤Ã×èͧ ËÃ×ÍäÁ‹ÊÒÁÒö㪌à¤Ã×èͧ䴌Í‹ҧ
àËÁÒÐÊÁ (poor compliance) «Ö§ÃÒ§ҹ㹵‹Ò§»ÃÐà·È¾ºÇ‹Ò ¼Ù»Ç·Õ㪌à¤Ã×ͧ CPAP Í‹ҧÊÁèÒàÊÁÍ
è Œ † è è í
äÁ‹¹ÍÂ¡Ç‹Ò ¤×¹ÅÐ 4 ªÑÇâÁ§ã¹áµ‹ÅÐÊÑ»´ÒË Áչ͡NjÒÃŒÍÂÅÐ 50 ´Ñ§¹Ñ¹¼Ù»ÇÂàËÅ‹Ò¹Õé ÍÒ¨ÁÕ¤ÇÒÁ
Œ è Œ (1)
é Œ †
àËÁÒÐÊÁ¡Ñº¡ÒÃÃÑ¡ÉÒ·Ò§àÅ×Í¡ ઋ¹ ¡Òü‹ÒµÑ´ ÁÒ¡¡Ç‹ÒÇÔ¸¡ÒÃÃÑ¡ÉÒ¢ŒÒ§µŒ¹ «Ö§áÁŒÇҼšÒÃÃÑ¡ÉÒ
Õ è ‹
ÍÒ¨äÁ‹¶§¢Ñ¹ËÒ¢Ҵ ᵋ¼»Ç¨íҹǹäÁ‹¹Íµͺʹͧµ‹Í¡ÒÃÃÑ¡ÉÒ ÁÕ¤ÇÒÁÃعáç¢Í§âäŴŧ
Ö é ÙŒ † Œ
¤Ø³ÀÒ¾ªÕǵ´Õ¢¹ áÅÐÁÕ¤ÇÒÁ¾Ö§¾Í㨨ҡ¡ÒÃÃÑ¡ÉÒ·Õµ¹àͧàÅ×Í¡ (2, 3)
Ô Öé è
á¹Ç·Ò§¡ÒÃÃÑ¡ÉÒâ´ÂÇÔ¸Õ¼‹ÒµÑ´ (Surgical treatment)
¡ÒÃÃÑ¡ÉÒâ´Â¡Òü‹ÒµÑ´ãªŒËÅÑ¡¡Òà ¡ÒÃá¡Œä¢Åѡɳзҧ¡ÒÂÇÔÀÒ¤à¾×Íà¾ÔÁ¢¹Ò´¢Í§·Ò§à´Ô¹
è è
ËÒÂã¨Ê‹Ç¹º¹ 㹺ÃÔàdzµíÒá˹‹§·ÕÍÒ¨à¡Ô´¡ÒÃÍØ´¡Ñ¹ â´ÂÁբͺ‹§ªÕã¹»˜¨¨Øº¹ 䴌ᡋ ¼Ù»Ç·յÃǨ
è é Œ é Ñ Œ † è
¾ºµíÒá˹‹§¢Í§¡ÒÃÍØ´¡Ñé¹·Ò§à´Ô¹ËÒÂã¨ä´ŒªÑ´à¨¹ ËÃ×Í ¡Ã³Õ·Õè¡ÒÃÃÑ¡ÉÒÍ×è¹äÁ‹»ÃÐʺ¼ÅÊíÒàÃç¨
ËÃ×ÍäÁ‹ÊÒÁÒöÃÑ¡ÉÒä´Œâ´ÂÇÔ¸ÕÍ×è¹ ¹Í¡¨Ò¡¹Õé¡Òü‹ÒµÑ´ÍÒ¨ª‹ÇÂàÊÃÔÁãËŒ¡ÒÃÃÑ¡ÉÒ´ŒÇÂÇÔ¸ÕÍ×è¹ àª‹¹
532 Surgical Treatment for Sleep Disordered Breathing
â´ÂÊÃØ» ¡Òü‹ÒµÑ´ÃÑ¡ÉÒÀÒÇй͹¡Ã¹ áÅÐÀÒÇÐËÂØ´ËÒÂ㨢³ÐËÅѺª¹Ô´ÍØ´¡Ñ¹ ÁÕÍÂÙËÅÒÂ
é ‹
ÇÔ¸Õ ÁÕ¤ÇÒÁàÊÕ觵‹ÍÀÒÇÐá·Ã¡«ŒÍ¹ µÅÍ´¨¹¼Å¢Í§¡ÒÃÃÑ¡ÉÒᵡµ‹Ò§¡Ñ¹ ´Ñ§¹Ñé¹ ¡Òü‹ÒµÑ´¨Ðä´Œ
¼ÅÊíÒàÃ稴շʴ ¨Ö§µŒÍ§¤íÒ¹Ö§¶Ö§ÅѡɳТͧâä·Õᵡµ‹Ò§¡Ñ¹ã¹¼Ù»ÇÂᵋÅÐÃÒ â´Âᾷ¤ÇÃãËŒ¢ÍÁÙÅ
Õè Ø è Œ † Œ
á¡‹¼»Ç à¾×ÍãËŒà¡Ô´¤ÇÒÁࢌÒ㨷ն¡µŒÍ§¡‹Í¹¡ÒõѴÊԹ㨼‹ÒµÑ´ à¾×Í»‡Í§¡Ñ¹áÅÐá¡Œä¢ÀÒÇÐá·Ã¡«ŒÍ¹
ÙŒ † è è Ù è
·ÕÍÒ¨à¡Ô´¢Ö¹ä´ŒÍ‹ҧ·Ñ¹·‹Ç§·Õ ÃÇÁ¶Ö§µÔ´µÒÁ¡ÒÃÃÑ¡ÉÒËÅѧ¼‹ÒµÑ´ä´ŒÍ‹ҧµ‹Íà¹×ͧ
è é è
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Kribbs NB, Pack AI, Kline LR, Smith PL, Schwartz AR, Schubert NM, et al. Objective measurement of
patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis 1993;147(4):
887-95.
2. Steward DL, Weaver EM, Woodson BT. Multilevel temperature-controlled radiofrequency for obstructive sleep
apnea: extended follow-up. Otolaryngol Head Neck Surg 2005;132(4):630-5.
3. .erguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep
apnea: a review. Sleep 2006;29(2):244-62.
4. Powell NB, Zonato AI, Weaver EM, Li K, Troell R, Riley RW, et al. Radiofrequency treatment of turbinate
hypertrophy in subjects using continuous positive airway pressure: a randomized, double-blind, placebo-controlled
clinical pilot trial. Laryngoscope 2001;111(10):1783-90.
5. Zeng B, Ng AT, Qian J, Petocz P, Darendeliler MA, Cistulli PA. Influence of nasal resistance on oral appliance
treatment outcome in obstructive sleep apnea. Sleep 2008;31(4):543-7.
6. Zonato AI, Bittencourt LR, Martinho .L, Gregorio LC, Tufik S. Upper airway surgery: the effect on nasal
continuous positive airway pressure titration on obstructive sleep apnea patients. Eur Arch Otorhinolaryngol
2006;263(5):481-6.
7. Gozal D. Sleep-disordered breathing and school performance in children. Pediatrics 1998;102(3 Pt 1):
616-20.
8. .riedman M, Ibrahim H, Bass L. Clinical staging for sleep-disordered breathing. Otolaryngol Head Neck Surg
2002;127(1):13-21.
9. Sher AE, Schechtman KB, Piccirillo J.. The efficacy of surgical modifications of the upper airway in adults with
obstructive sleep apnea syndrome. Sleep 1996;19(2):156-77.
10. Rombaux P, Hamoir M, Bertrand B, Aubert G, Liistro G, Rodenstein D. Postoperative pain and side effects
after uvulopalatopharyngoplasty, laser-assisted uvulopalatoplasty, and radiofrequency tissue volume reduction
in primary snoring. Laryngoscope 2003;113(12):2169-73.
11. .riedman M, Schalch P, Lin HC, Kakodkar KA, Joseph NJ, Mazloom N. Palatal implants for the treatment of
snoring and obstructive sleep apnea/hypopnea syndrome. Otolaryngol Head Neck Surg 2008;138(2):
209-16.
12. Kezirian EJ, Goldberg AN. Hypopharyngeal surgery in obstructive sleep apnea: an evidence-based medicine
review. Arch Otolaryngol Head Neck Surg 2006;132(2):206-13.
13. Li KK, Powell NB, Riley RW, Troell RJ, Guilleminault C. Long-Term Results of Maxillomandibular Advancement
Surgery. Sleep Breath 2000;4(3):137-40.
560.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 533
14. Denbar MA. A case study involving the combination treatment of an oral appliance and auto-titrating CPAP
unit. Sleep Breath 2002;6(3):125-8.
15. Chan AS, Lee RW, Cistulli PA. Dental appliance treatment for obstructive sleep apnea. Chest 2007;132(2):693-
9.
16. Hoffstein V. Review of oral appliances for treatment of sleep-disordered breathing. Sleep Breath 2007;11(1):
1-22.
562.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 535
73
Management for Dysphagia Patients
ÃͧÈÒʵÃÒ¨Òà¹ÒÂá¾·Â⪤ªÑ àÁ¸ÕäµÃÃѵ¹
¹Ò§ÊÒÇ๵ÃÒ ºÑÇ¡¹¡
¼ÙŒª‹ÇÂÈÒʵÃÒ¨Òà¹ÒÂá¾·ÂÀÒÇÔ¹ à¡É¡ØÅ
ÍÒ¨Òà¹ÒÂá¾·ÂÇÃصÁ ¾§ÈÒ¾Ôª
ÍÒ¨ÒàᾷÂËÔ§Êعѹ· ͧÍÒ¨
ÀÒ¤ÇÔªÒâʵ ¹ÒÊÔ¡ ÅÒÃÔ§«Ç·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ÔÔ
¡ÒáÅ×¹ (Swallowing or deglutition)
໚¹»˜¨¨Ñ¾׹°Ò¹ÊíÒ¤ÑÍ‹ҧ˹֧µ‹Í¡ÒôíÒçªÕǵ¢Í§Á¹ØÉ à¹×ͧ¨Ò¡Á¹ØɨÒ໚¹µŒÍ§¡Ô¹
é è Ô è í
ÍÒËÒ÷ÕèÁÕ»ÃÐ⪹áÅÐä´Œ»ÃÔÁÒ³à¾Õ§¾Í à¾×èÍãËŒà¡Ô´à»š¹¾Åѧ§Ò¹·Õèà¾Õ§¾Íµ‹Í¡ÒÃà¨ÃÔàµÔºâµ
áÅСԨ¡ÃÃÁµ‹Ò§æ 㹡ÒôíÒçªÕ¾ ¡ÒáÅ׹໚¹¢ºÇ¹¡ÒÃàº×ͧµŒ¹·ÕÁ˹ŒÒ·ÕʧÍÒËÒèҡ·Ò§à´Ô¹
é è Õ è ‹
ÍÒËÒÃʋǹµŒ¹ 䴌ᡋ ª‹Í§»Ò¡ (oral cavity) ¤ÍËÍ (pharynx) áÅÐËÅÍ´ÍÒËÒà (esophagus) ä»Âѧ
·Ò§à´Ô¹ÍÒËÒÃʋǹŋҧ·ÕàÃÔÁµŒ¹¨Ò¡¡ÃÐà¾ÒÐÍÒËÒÃ໚¹µŒ¹ä» ¡ÒáÅ×¹·Õ»¡µÔ¨Ò໚¹µŒÍ§»ÃСͺ´ŒÇÂ
è è è í
â¤Ã§ÊÌҧÍÇÑÂÇдѧ¡Å‹ÒÇ·Õ軡µÔ áÅÐÁÕ¡Ò÷íÒ§Ò¹¢Í§Ãкº¡ÅŒÒÁà¹×éÍ áÅÐÃкº»ÃÐÊÒ··Õè·íÒ§Ò¹
»ÃÐÊÒ¹µ‹Íà¹×ͧ¡Ñ¹à»š¹Í‹ҧ´Õ
è
㹡ÒáÅ×¹¹Ñ¹ àÁ×ÍÍÒËÒÃࢌÒÊ٪ͧ»Ò¡áÅŒÇ ¨Ð¼‹Ò¹Å§ÊÙ¤ÍËÍÂáÅÐËÅÍ´ÍÒËÒà áÅм‹Ò¹
é è ‹ ‹ ‹
µ‹Íŧä»ã¹¡ÃÐà¾ÒÐÍÒËÒÃáÅÐÅíÒäÊŒ«§¨Ñ´à»š¹·Ò§à´Ô¹ÍÒËÒÃʋǹŋҧµ‹Íä» ÊÒÁÒöẋ§¢Ñ¹µÍ¹¢Í§
Öè é
¡ÒáÅ×¹ ãˌࢌÒã¨â´Â§‹ÒÂ໚¹ ó ¢Ñ¹µÍ¹
é
1. ¢Ñ¹µÍ¹ã¹ª‹Í§»Ò¡ (Oral phase)
é
à¡Ô´¢Ö¹àÁ×ÍãÊ‹ÍÒËÒÃࢌÒä»ã¹ª‹Í§»Ò¡ Ëҧ¡Ò¨зíÒ¡ÒÃàµÃÕÂÁʋǹ¢Í§ÍÒËÒÃãËŒÁšɳÐ
é è ÕÑ
àËÁÒÐÊÁ·Ñ§ã¹´ŒÒ¹ÃٻËҧ ¢¹Ò´ áÅФÇÒÁ˹״·ÕàËÁÒÐÊÁà¾×ÍãËŒ¡Å׹䴌Í‹ҧ¤Å‹Í§µÑÇ ´Ñ§¹Ñ¹¢Ñ¹µÍ¹
é è è é é
¹Õ¨ÐµŒÍ§ÍÒÈÑÂÍÇÑÂÇÐËÅÒÂÍ‹ҧ·ÕµÍ§·íҧҹËÇÁ¡Ñ¹ä´ŒÍ‹ҧàËÁÒÐÊÁ 䴌ᡋ ÃÔÁ½‚»Ò¡ (lips) ¡Ãоا
é è Œ Œ
á¡ŒÁ (buccal mucosa) ¡Ãд١¢Ò¡ÃÃä¡Ã (upper and lower jaws) ¿˜¹ (teeth) µ‹ÍÁ¹éÒÅÒ (salivary
í
glands) ÅÔ¹ (tongue) áÅÐྴҹ»Ò¡ (palate)
é
¢Ñ¹µÍ¹ã¹ª‹Í§»Ò¡¹Õé µŒÍ§ÍÒÈÑ¡Ò÷íҧҹËÇÁ¡Ñ¹¢Í§¡ÅŒÒÁà¹×ÍËÅÒÂÁÑ´«Ö§¶Ù¡¤Çº¤ØÁâ´Â
é é è
àÊŒ¹»ÃÐÊÒ·ÊÁͧ¤Ù·Õè 5,7,9,10,11, áÅÐ 12 àÁ×ÍÍÒËÒÃÁÕ¢¹Ò´ ÃٻËҧáÅФÇÒÁ˹״·ÕàËÁÒÐÊÁµ‹Í
‹ è è
¡ÒáÅ×¹áÅŒÇ à¾´Ò¹»Ò¡¨Ð¡µÑÇ¢Öé¹ä»»´â¾Ã§ËÅѧ¨ÁÙ¡ (nasopharynx) »‡Í§¡Ñ¹äÁ‹ãËŒÍÒËÒÃ
ÃÑèǼ‹Ò¹¢Öé¹â¾Ã§¨ÁÙ¡ä´Œ ¢³Ðà´ÕÂǡѹ¡ÅŒÒÁà¹×éÍ⤹ÅÔ鹨ÐË´µÑǵèíÒŧà¾×èÍà»´¤ÍËÍ (pharynx)
ãËŒ¡ÇŒÒ§¢Ö¹ ¨Ò¡¹Ñ¹ÅԹʋǹ˹ŒÒ¨Ð·íÒ˹ŒÒ·Õ¡ÇÒ´ÍÒËÒÃãˌŧä»ã¹¤ÍË͵‹Íä»
é é é è
àǪÈÒʵ÷¹Âؤ 2553
Ñ 541
2. ½ƒ¡¡ÒÃËÒÂã¨ãˌšÁÒ¡¢Ö¹à¾×ͪ‹ÇÂãËŒ¡ÅŒÒÁà¹×ÍÅÔ¹áÅСŋͧàÊÕ§ÁÕ¡ÒÅѧà¾ÔÁ¢Ö¹ Âѧª‹ÇÂÅ´
Ö é è é é í è é
ÍÒ¡ÒÃà¡Ã秢ͧËҧ¡ÒÂ
3. ËŒÒÁÃѺ»ÃзҹÍÒËÒâ³Ð·ÕÍÂÙã¹·‹Ò¤ÃÖ§¹Ñ§¤ÃÖ§¹Í¹ ÍÒ¨·íÒãËŒà¡Ô´ ¡ÒÃäËŢͧ¹éÒËÃ×Í
è ‹ è è è í
ÍÒËÒÃŧÊÙ·Ò§à´Ô¹ËÒÂã¨ä´Œ ¨¹ÍÒ¨à¡Ô´ÀÒÇлʹª×¹ËÃ×ͻʹµÔ´àª×Í àÇÅÒ·Ò¹¹éÒËÃ×ÍÍÒËÒà äËÅ‹
‹ é é í
µŒÍ§µÑ§µÃ§
é
4. ¶ŒÒ¡Å×¹ÍÒËÒÃáŌǵԴ ËŒÒÁ¹Í¹Å§¡Ñº¾×¹ ãˌ¹¢Ö¹áÅŒÇÂ״Ëҧ¡ÒÂʋǹº¹áÅÐà´Ô¹Ãͺæ
é × é
㹪‹Ç§àÇÅÒÊѹæ ÍÒ¨¨Ðª‹ÇÂãËŒÍÒËÒÃäËÅŧ·ŒÍ§ä´Œ
é
5. ¶ŒÒ¿˜¹»ÅÍÁËÅÇÁ¨ÐµŒÍ§á¡Œä¢ãˌṋ¹¢Ö¹ é
6. ËŒÒÁÃѺ»ÃзҹÍÒËÒá‹Í¹¹Í¹ 3 ªÑÇâÁ§ ¶ŒÒÍÒËÒõԴã¹ËÅÍ´ÍÒËÒ÷ѧ¤×¹ÍÒ¨·íÒãËŒ
è é
à¡Ô´ÍÒ¡ÒÃäÁ‹ÊºÒµÑÇáÅÐÍÒ¨à¡Ô´ÍÒ¡ÒÃà¨çºã¹¤Í
¡Òÿ„¹¿Ù·Ò§µÃ§ (Direct therapy)
œ
½ƒ¡â´Â㪌ÍÒËÒÃËÃ×ͧ͢àËÅÇ㹡ÒáÃеع¡Òýƒ¡¡Å×¹
Œ
¡ÒûÃѺà»ÅÕ¹¡ÒáÅ×¹
è
1. µÑ´ÍÒËÒÃáÅŒÇà¤ÕÂÇÍÒËÒÃãˌ໚¹ªÔ¹àÅç¡æ
é é
2. ¶ŒÒËÒ¡Ç‹ÒÁÕ¡ÒÃÊÙàÊÕ¡ÒÃÃѺ¡ÅÔè¹áÅÐÃʪҵÔÍÒËÒà ¨¹·íÒãËŒ¹éíÒÅÒ¼ÅÔµÍÍ¡ÁÒ
äÁ‹à¾Õ§¾Í ÍҨʋ§¼ÅãËŒà¡Ô´ÍÒ¡ÒÃäÁ‹ÍÂÒ¡¡Ô¹ÍÒËÒà «Ö§ÍҨᡌ䢴ŒÇ¡ÒûÃѺà»ÅÕ¹´ŒÇ¡Òõ¡áµ‹§
è è
ÍÒËÒÃãËŒËÅÒ¡ÊÕʹ Ñ
3. 㪌à¤Ã×ͧ´×ÁËÅÒ¡ÊÕʹà¾×ͪ‹Ç¡ÃеعãËŒ¡Å×¹ÍÒËÒü‹Ò¹Å§ä»ä´Œ
è è Ñ è Œ
4. µŒÍ§ÁÕàÇÅÒ·Õà¾Õ§¾Í㹡ÒÃÃѺ»ÃзҹÍÒËÒà äÁ‹¤ÇÃà˧ÃÕºà¡Ô¹ä»
è
5. ËÅÕ¡àÅÕ§¡ÒÃ㪌¿¹¡Ñ´ªŒÍ¹¢³Ð·Õ»Í¹ÍÒËÒà à¾×Í»‡Í§¡Ñ¹»¯Ô¡ÃÂÒ¡ÒáÅ×¹Íѵâ¹ÁѵÔ
è ˜ è ‡ è ÔÔ
6. ÃѺ»ÃзҹÍÒËÒÃã¹Ê¶Ò¹·Õ·Ê§ºáÅÐà§Õº äÁ‹Ááç¡´´Ñ¹¨Ò¡¡ÒÃÂ×¹Áͧ¨Ò¡¤¹Ãͺ¢ŒÒ§
è Õè Õ
7. ¤¹ä¢ŒµÍ§ÍÂÙã¹·‹ÒµÑ§µÃ§ËÅѧ¨Ò¡·Õ¡Å×¹ÍÒËÒÃ令ÃѧáááÅŒÇ »ÃÐÁÒ³ 20 ¹Ò·Õ à¾×ÍãËŒ
Œ ‹ é è é è
ṋã¨Ç‹Ò㹪‹Í§»Ò¡äÁ‹ÁÍÒËÒÃÍÂÙã¹»Ò¡áÅÐã¹µÔ´ã¹ËÅÍ´ÍÒËÒà à¾×Í»‡Í§¡Ñ¹¡ÒáÅ×¹«éÒÍ‹ҧàÃçÇ
Õ ‹ è í
¶ŒÒËÒ¡Ç‹Ò¹íÒÍÒËÒÃãËŒ¤¹ä¢ŒÃͺµ‹Íä»
¡ÒûÃѺà»ÅÕ¹ÍÒËÒÃ
è
¶ŒÒÁÕ»˜ËÒã¹Ê‹Ç¹¢Í§ËÅÍ´ÍÒËÒÃʋǹŋҧ ¡Å×¹áÅŒÇäÁ‹äËż‹Ò¹Å§ä´Œ§‹Ò ¤ÇèÐÁÕ¡ÒÃ
»ÃѺà»ÅÕ¹ÍÒËÒÃãËŒ¹ÁáÅÐàËÅÇ¢Ö¹ ᵋ¡µÍ§ÃÐÇѧ㹡ÒÃà¡Ô´
è Ôè é ç Œ
1. ¡ÒÃäËÅŧ¢Í§ÍÒËÒ÷ÕàÃçÇà¡Ô¹ä» ÂÒ¡µ‹Í¡ÒäǺ¤ØÁ ·íÒãËŒäËÅŧÊÙ·Ò§à´Ô¹ËÒÂã¨áÅÐ
è ‹
»Í´ä´Œ¡Ò÷ÕÍÒËÒÃÁÕ¤ÇÒÁ˹Ò˹״·íÒãËŒà¡Ô´¡ÒÃÃѺÃÙä´Œ§Ò¢³Ð¡Å×¹
è Œ ‹
2. ÍÒËÒ÷ÕÁÃÊà»ÃÕÂÇ·íÒãËŒ¡ÒáÅ×¹ÁÕ»¯Ô¡ÃÂÒ·Õ໚¹Íѵâ¹ÁÑµÔ ÍÂÒ¡µ‹Í¡ÒäǺ¤ØÁ
è Õ é ÔÔ è
3. ÍÒËÒ÷Õ赡ᵋ§ãËŒ´Ù¹‹ÒÃѺ»Ãзҹ¨Ð໚¹µÑÇ¡Ãе،¹¤ÇÒÁÍÂÒ¡ÃѺ»ÃзҹÍÒËÒÃ
¨¹·íÒãˌúÌ͹·ÕÍÂÒ¡¨ÐÃѺ»ÃзҹÍÒËÒÃàÃçÇà¡Ô¹ä»
Õ è
569.
542 Management for Dysphagia Patients
4. ÍÒËÒ÷Õèá¢ç§¤ÇûÃѺà»ÅÕè¹ãËŒ¢Œ¹ËÃ×͹ÔèÁ¢Öé¹áµ‹¡çµŒÍ§Å´¡ÒÃà¤ÕéÂÇãËŒ¹ŒÍÂŧáÅеŒÍ§
㪌áçäÁ‹Áҡ㹡ÒôѹËÃ×Í¡Å×¹ãˌŧä»ÂѧËÅÍ´ÍÒËÒÃ
¡ÒÃàµÃÕÂÁÍÒËÒÃáÅЪ¹Ô´¢Í§ÍÒËÒà 㹡Òýƒ¡¡Å×¹ÁÕ¤ÇÒÁÊÑÁ¾Ñ¹¸¡¹Í‹ҧÁÒ¡àËÁ×͹
Ñ
¡Ñº¡ÒáÒÃàµÃÕÂÁ¤ÇÒÁá¢ç§áç¢Í§¡ÅŒÒÁà¹×Í·Õà¡ÕÂÇ¢ŒÍ§¡Ñº¡ÒáÅ×¹ áÅÐÂѧÃÇÁ¶Ö§¡Ò÷íÒ§Ò¹·ÕàËÁÒÐ
é è è è
ÊÁáÅж١µŒÍ§¢Í§¡Å‹Í§àÊÕ§¢³Ð·ÕÁ¡ÒáÅ×¹
è Õ
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Shipley KG, McAfee JG. Assessment in speech-language pathology. 3rded. Delmar learning: USA, 2004,
390-406
2. Crary MA, Groher ME. Introduction to adult swallowing disorders. Elsevier Science,USA, 2003.
3. Palmer JB, Drennan JC, Baba M. Evaluation and treatment of swallowing impairments. AA.P 2000; Apirl;15.
4. Burkhead LM, Sapienza CM, Rosenbek JC. Strength-training exercise in dysphagia rehabilitation: Principle,
procedures, and directions for future research. Dysphagia 2007;22 :251-265
5. Logemann JA. The role of exercise programs for dysphagia patients. Dysphagia 2005;20:139-140.
6. Johnson A., Jacobson BH. Medical speech-language pathology a practitioner’s guide. Thieme: New York,
1998.
7. McKinstry A, Tranter M, Sweeney J. Outcomes of dysphagia intervention in a pulmonary rehabilitation program.
Dysphagia 2010;25:104-11.
8. Speyer R, Baijens L, Heijnen M, Zwijnenberg I. Effects of therapy in oropharyngeal dysphagia by speech-
language therapist: a systematic review. Dysphagia 2010;25:40-6.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 551
ÀÒ¾»ÃСͺ·Õè 1 bleeding stigmata of recent peptic ulcer
¡Ò÷íÒ routine second look endoscopy ¾ºÇ‹ÒäÁ‹Á»ÃÐ⪹ÁÒ¡¹Ñ¡(11) ¡àÇŒ¹Ç‹Òʋͧ¡ÅŒÍ§
Õ
¤ÃѧááàËç¹äÁ‹ª´à¨¹à¹×ͧ¨Ò¡ÁÕàÅ×Í´¤ŒÒ§ÍÂ٨ҹǹÁÒ¡ ËÃ×;º high risk stigmata ·Õ¼»ÇÂ䴌ú
é Ñ è ‹í è ÙŒ † Ñ
ÂÒ·Õè ÁÕ ¼ ŵ‹ Í ¡ÒÃá¢ç § µÑ Ç ¢Í§àÅ× Í ´ÍÂÙ‹ ËÃ× Í ¼ÙŒ »† Ç ÂÁÕ Í Ò¡ÒÃË¹Ñ ¡ ÁÒ¡äÁ‹ Ê ÒÁÒö·¹µ‹ Í ¡ÒÃà¡Ô ´
re-bleeding ä´Œ ¡Ò÷íÒ second look endoscopy â´Â·Õ§äÁ‹ÁÕ recurrent of bleeding ÍÒ¨ÁÕ»ÃÐ⪹
è Ñ
㹡óնÒà¡Ô´ re-bleeding «Ö§¾ºä´Œ 15-20% áÅÐÁÑ¡à¡Ô´ÀÒÂã¹ 72 ªÑÇâÁ§ááËÅѧ¨Ò¡ÊÒÁÒö
Œ è è
ËÂØ´àÅ×Í´´ŒÇ endoscopic therapy 䴌㹤Ãѧáá á¹Ð¹íÒãËŒ·Òendoscopy «éÒ áÅоÂÒÂÒÁËÂØ´
é í í
àÅ×Í´´ŒÇ endoscopic interventions ÍÕ¡ à¹×ͧ¨Ò¡ÁÕ¡ÒÃÈÖ¡ÉÒ¾ºÇ‹Òª‹ÇÂÅ´âÍ¡ÒÊ surgery áÅÐ
è
äÁ‹à¾ÔÁ mortality ¢Í§¼Ù»Ç Í‹ҧäáçµÒÁ¡Ò÷íÒ surgery ·ÕªÒà¡Ô¹ä»ã¹ÃÒ·ÕÁ¤ÇÒÁ¨íÒ໚¹¹Ñ¹ ¡çà¾ÔÁ
è Œ † è Œ è Õ é è
¤ÇÒÁàÊÕ§µ‹Í¼Ù»Ç´ŒÇ ´Ñ§¹Ñ¹¡Ò÷íҧҹËÇÁ¡Ñ¹ÃÐËNjҧᾷÂÍÒÂØáÃÃÁáÅÐÈÑÅ¡ÃÃÁ¨Ö§ÁÕ¤ÇÒÁ
è Œ † é
ÊíÒ¤ÑÁÒ¡·Õ¨Ðª‹ÇÂãËŒ¼»ÇÂ䴌ú¡ÒÃÃÑ¡ÉÒ·Õ¶¡µŒÍ§ àËÁÒÐÊÁáÅÐÃÇ´àÃçÇ
è ÙŒ † Ñ è Ù
Surgery
¡ÒÃÃÑ¡ÉҼٻǠupper GI bleeding ã¹·Ò§ÈÑÅ¡ÃÃÁã¹»˜¨¨Øº¹ÁÕº·ºÒ·Å´Å§¨Ò¡à´ÔÁÁÒ¡
Œ † Ñ
à¹×ͧ¨Ò¡¡ÒþѲ¹Ò´ŒÒ¹à·¤â¹âÅÂÕ áÅÐà·¤¹Ô¤ãËÁ‹æ·Ò§´ŒÒ¹ endoscopy Í‹ҧäáçµÒÁã¹¼Ù»ÇÂ
è Œ †
ºÒ§ÃÒ¡çÍÒ¨ÁբͨíҡѴ㹡Ò÷íÒ endoscopic interventions ઋ¹ cancer bleeding, active bleeding
Œ
from posterior wall of duodenum («Ö§àÅ×Í´ÁÑ¡ÍÍ¡¨Ò¡ branch ¢Í§ gastroduodenal artery ·ÕÁ¡
è è Ñ
໚¹á¢¹§¢¹Ò´ãË‹) ËÃ×Í bleeding «Ö§ÍÒ¨à¡Ô´¨Ò¡ aortoenteric fistula ໚¹µŒ¹ ¤ÇûÃÖ¡ÉÒá¾·Â
è
·Ò§ÈÑÅ¡ÃÃÁËÇÁ´ÙáÅ´ŒÇÂàÊÁÍ
àǪÈÒʵ÷¹Âؤ 2553
Ñ 553
continuous high dose IV PPI regimen ´Ñ§¡Å‹ÒÇ¢ŒÒ§µŒ¹¹Ò¹ 3-5 ÇѹµÒÁËÅѧ¡Ò÷íÒ endoscopic therapy
«Ö§¾ºÇ‹ÒÊÒÁÒöŴ re-bleeding áÅÐ surgery ä´Œ(7) áÅмٻǤÇÃ䴌ú¡ÒÃÊѧࡵÍÒ¡ÒÃã¹âç
è Œ † Ñ
¾ÂÒºÒŵ‹ÍÍ‹ҧ¹ŒÍ 72 ªÑÇâÁ§ ËÅѧ¨Ò¡¹Ñ¹ãËŒ¡ÒÃÃÑ¡ÉÒ仵ÒÁᵋª¹Ô´, µíÒá˹‹§áÅÐÊÒà˵آͧ
è é
á¼Å¹Ñ¹ ʋǹ㹡óշÕè endoscopic finding ໚¹ low re-bleeding risk ÊÒÁÒöãËŒ¼»ÇÂàÃÔÁÃѺ
é ÙŒ † è
»ÃзҹÍÒËÒà áÅÐ ÍÍ¡¨Ò¡âç¾ÂÒºÒÅä´ŒàÃçÇ¢Ö¹ÀÒÂã¹ 24 ªÑÇâÁ§
é è
ʋǹ¡ÒÃ㪌 Histamine 2 –receptor antagonist (H2 RA) ¹Ñ¹ÁÕ meta-analysis ¨¹¶Ö§»‚
é
¤.È. 2002 áÊ´§Ç‹Ò H2RA ÁÕ»ÃÐ⪹㹡ÒÃÅ´ÍѵÃÒàÅ×Í´ÍÍ¡«éÒáÅСÒü‹ÒµÑ´ÊíÒËÃѺ gastric ulcer
í
ᵋäÁ‹Á¼Åµ‹Í duodenal ulcer áÅж֧áÁŒ¨ÐãËŒ continuous high dose H2RA ¡çäÁ‹Á¼Åµ‹ÍÍѵÃÒàÅ×Í´
Õ Õ
ÍÍ¡«éÒ ÍѵÃÒµÒÂáÅСÒü‹ÒµÑ´àª‹¹¡Ñ¹ Í‹ҧäáçµÒÁàÁ×ÍÁÕ¡Ò÷íÒ meta-analysis 㹤ÃѧËÅѧæ áÅÐ
í è é
à»ÃÕºà·Õº¡Ñº endoscopic interventions áÅÐ PPI ¡ÅѺ¾ºÇ‹Ò H2RA ÁÕ»ÃÐ⪹¹Í¡NjÒÍ‹ҧ
Œ
ªÑ´à¨¹ ÊÃػ㹻˜¨¨Øº¹äÁ‹á¹Ð¹íÒãˌ㪌 H2RA ໚¹ÂÒËÅѡ㹡ÒÃÃÑ¡ÉÒÀÒÇÐ acute non variceal
(7)
Ñ
upper GI bleeding ÍÕ¡µ‹Íä»
¡ÒÃ㪌 Somatostatin ËÃ×Í Octreotide 㹡ÒÃÃÑ¡ÉÒÀÒÇйÕé ¾ºÇ‹ÒÊÒÁÒöŴ recurrent of
bleeding ä´Œ´¡Ç‹Ò placebo ᵋàÁ×Íà»ÃÕºà·Õº¡Ñº H2RA, PPI áÅÐ endoscopic treatment
Õ è
áÅŒÇäÁ‹¾ºÇ‹Òᵡµ‹Ò§¡Ñ¹Í‹ҧÁÕ¹ÂÊíÒ¤Ñ·Ò§Ê¶ÔµÔ ´Ñ§¹Ñ¹ ¨Ö§äÁ‹á¹Ð¹íÒãˌ㪌ÂÒ¡ÅØÁ¹Õઋ¹¡Ñ¹(7)
Ñ é ‹ é
Helicobactor pylori ¡Ñº¡ÒÃà¡Ô´àÅ×Í´ÍÍ¡ã¹·Ò§à´Ô¹ÍÒËÒÃ
à¹×ͧ¨Ò¡»ÃÐÁÒ³ 70% ¢Í§ acute upper GI bleeding ¹Ñ¹à¡Ô´¨Ò¡ peptic ulcer bleeding
è é
áÅÐ gastric erosions áÅШҡ¡ÒÃÈÖ¡ÉÒ·Õ¼Ò¹ÁÒ¾ºÇ‹Ò H.pylori ¹Ñ¹ÊÑÁ¾Ñ¹¸Í‹ҧªÑ´à¨¹¡Ñº¡ÒÃ
è ‹ é
à¡Ô´ gastric ulcer áÅÐ duodenal ulcer ÁÒ¡¶Ö§ 80-100% Í‹ҧäáçµÒÁÁÕ¢ÍÁÙÅÇ‹Ò¡ÒõÃǨËÒ H.Pylori
Œ
´ŒÇÂÇÔ¸Õ rapid urease test ã¹¢³Ð·ÕÁÕ active bleeding ¹Ñ¹ÍÒ¨ãËŒ¼Å false negative ¨Ò¡¡Ò÷ÕÁàÅ×Í´»¹
è é è Õ
¨Ö§á¹Ð¹íÒãËŒ·Ò¡ÒõÃǨÍ‹ҧ¹ŒÍ 2 ÇÔ¸Õ à¾×Í¡ÒÃÂ×¹Âѹ¼Å¹‹Ò¨ÐÁÕ»ÃÐ⪹¡Ç‹Ò «Ö§äÁ‹¨Ò໚¹µŒÍ§·íÒ
í è è í
·Ñ¹·Õã¹¢³Ð·Õ§ÁÑ»ËÒ active bleeding ÍÂÙ‹ ´Ñ§¹Ñ¹ã¹¼Ù»Ç·ÕÁÒ´ŒÇ»˜ËÒ ulcer bleeding ·Ø¡ÃÒÂ
è Ñ ˜ é Œ † è
ã¹·ÕÊ´¤ÇÃ䴌ú¡ÒõÃǨËÒ H. Pylori àÊÁÍ áÅÐËÒ¡¾ºÇ‹ÒÁÕ¡ÒõԴàª×Í ¤Ç÷íÒ¡ÒÃÃÑ¡ÉÒ à¾ÃÒÐä´Œ
èØ Ñ é
ÃѺ¡ÒÃÂÍÁÃѺNjҪ‹ÇÂÅ´âÍ¡ÒÊà¡Ô´ recurrent peptic ulcer 䴌͋ҧªÑ´à¨¹
References :
1. Grace H. Elta. Yamada Text book of Gastroenterology, 4th ed. 2003:698-723.
2. Christopher S. Huang,David R. Lichtenstein.Nonvariceal upper gastrointestinal bleeding.Gastroenterology clinics
of north America. 2003;32(4):1053-78.
3. Chen IC, Hung MS et al. Risk scoring systems to predict need for clinical intervention for patients with
nonvariceal upper gastrointestinal tract bleeding. Am J Emerg Med. 2007;25(7):774-9.
4. Robert A Enns,Yves M Gagnon et al. Validation of the Rockall scoring system for outcomes from non-variceal
upper gastrointestinal bleeding in a Canadian setting. World J Gastroenterology. 2006;12(28):7779-85.
581.
554 ÀÒÇÐàÅ×Í´ÍÍ¡ã¹·Ò§à´Ô¹ÍÒËÒÃʋǹº¹
5. Hamid Hussain,Seth Lapin et al.Clinical scooring systems for determining the Prognosis of Gastrointestinal
bleeding. Gastroenterology clinics of north America. 2000;29(2):445-64.
6. Thomas J. Savides, Dennis M.Jensen.Therapeutic Gastroenterology clinics of north America Endoscopy for
Nonvariceal Gastrointestinal Bleeding. 2000;29(2):465-88.
7. Alan Barkun,Marc Bardou et al.Concensus Recommendation for Managing Patients with Nonvariceal Upper
Gastrointestinal Bleeding.Ann Intern Med. 2003;139:843-57.
8. Mitshell S. Cappell, David .rieddel.Medical Clinic of North America. 2008;92:491-509.
582.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 555
75
Management of Esophageal Varices and
Esophageal Variceal Hemorrhage
¼ÙŒª‹ÇÂÈÒʵÃÒ¨ÒàᾷÂËÔ§ÈÔÇоà äªÂ¹ØÇѵÔ
ÍÒ¨ÒàᾷÂËÔ§¹¹·ÅÕ à¼‹ÒÊÇÑÊ´Ôì
ÍÒ¨Òà¹ÒÂá¾·ÂÊؾ¨¹ ¹ÔèÁ͹§¤
ÀÒ¤ÇÔªÒÍÒÂØÃÈÒʵà ¤³Ðá¾·ÂÈÒʵÃÈÔÃÔÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ÀÒÇÐ portal hypertension (PH) ¤×Í ÀÒÇзÕèÁÕ¤‹Ò¤ÇÒÁᵡµ‹Ò§ÃÐËÇ‹Ò§¤ÇÒÁ´Ñ¹ã¹
ËÅÍ´àÅ×Í´´íÒ portal áÅÐËÅÍ´àÅ×Í´´íÒãË‹ (inferior vena cava) à¡Ô¹ 5 mmHg â´Â»¡µÔ
¤ÇÒÁᵡµ‹Ò§ÃÐËÇ‹Ò§¤ÇÒÁ´Ñ¹ã¹ËÅÍ´àÅ×Í´´íÒ¾Í÷Š(portal pressure gradient) ¨ÐÍÂÙÃÐËÇ‹Ò§
Ñ ‹
1-5 mm Hg ¹Í¡¨Ò¡¹Õã¹ÀÒÇÐ PH ÂѧÁÕ¡ÒÃà»ÅÕ¹àÊŒ¹·Ò§äËÅàÇÕ¹¢Í§àÅ×Í´â´Â¡ÒÃÊÌҧ portal
é è
systemic collaterals ¢Ö¹ÁÒ໚¹·Ò§ÅÑ´¢Í§àÅ×Í´«Ö§¨Ð·íÒãËŒÁ¡ÒÃäËÅàÇÕ¹¢Í§àÅ×Í´¨Ò¡ portal system
é è Õ
ࢌÒä»ÊÙÃкº¡ÒÃäËÅàÇÕ¹ systemic â´ÂµÃ§â´ÂàÅ×Í´¨ÐäÁ‹¼Ò¹µÑº àÊŒ¹àÅ×Í´ collaterals ·Õà¡Ô´¢Ö¹
‹ ‹ è é
䴌ᡋàÊŒ¹àÅ×Í´¢Í´ã¹ËÅÍ´ÍÒËÒÃ-¡ÃÐà¾ÒÐÍÒËÒà (gastroesophageal varices) àÁ×ÍÁÕ portal pressure
è
ÊÙ§¢Ö¹àÃ×ÍÂæ ¡ç¨ÐÁÕ¡ÒÃ⻆§µÑǢͧàÊŒ¹àÅ×Í´¢Í´àËÅ‹Ò¹ÕáÅÐà¡Ô´àÅ×Í´ÍÍ¡ã¹·ÕÊ´ (variceal bleeding)
é è é èØ
Esophageal varices and esophageal variceal hemorrhage
¤ÇÒÁªØ¡¢Í§àÊŒ¹àÅ×Í´¢Í´ã¹ËÅÍ´ÍÒËÒâͧ¼ÙŒ»†Ç·ÕèÁÕÀÒÇеѺá¢ç§·Õèä´ŒµÃǨʋͧ¡ÅŒÍ§
·Ò§à´Ô¹ÍÒËÒÃʋǹµŒ¹ (esophagogastroduodenoscopy, EGD) »ÃÐÁҳÌÍÂÅÐ 30-40 áÅоº
àÊŒ¹àÅ×Í´¢Í´ã¹ËÅÍ´ÍÒËÒö֧ 60% ã¹¼ÙŒ»†ÇµѺá¢ç§ÃÐÂÐÊØ´·ŒÒ (decompensated cirrhosis)
¨Ò¡¡ÒÃÈÖ¡ÉÒ¡ÒÃà¡Ô´¢Í§àÊŒ¹àÅ×Í´ã¹ËÅÍ´ÍÒËÒà (esophageal varices, EV) â´Â Groszmann áÅÐ
¤³Ð¾ºÇ‹Ò¤‹Ò hepatic venous pressure gradient (HVPG) ·ÕÁÒ¡¡Ç‹Ò 10 mmHg ໚¹»˜¨¨Ñº‹§ºÍ¡
è
(predictor) ·ÕÊÒ¤Ñ㹡ÒÃà¡Ô´ EV
èí
Íغµ¡Òó¢Í§¡ÒÃà¡Ô´àÊŒ¹àÅ×Í´¢Í´ã¹ËÅÍ´ÍÒËÒÃ㹼ٻǵѺá¢ç§¾º»ÃÐÁҳÌÍÂÅÐ 5-8
Ñ Ô Œ †
µ‹Í»‚áÅÐàÊŒ¹àÅ×Í´¢Í´¢¹Ò´àÅç¡ (small EV) ¨Ðâµ¢Ö¹¢ÂÒµÑÇ໚¹¢¹Ò´ãË‹ (large EV) ã¹ÍѵÃÒ
é
ÃŒÍÂÅÐ 5-30 µ‹Í»‚ âÍ¡ÒÊ·Õà¡Ô´àÊŒ¹àÅ×Í´ÍÍ¡¨Ò¡àÊŒ¹àÅ×Í´¢Í´áµ¡»ÃÐÁҳÌÍÂÅÐ 15 µ‹Í»‚ àÁ×Íà¡Ô´
è è
ÀÒÇÐàÅ×Í´ÍÍ¡¨Ò¡àÊŒ¹àÅ×Í´¢Í´ã¹ËÅÍ´ÍÒËÒüٻǨÐÁÕ͵ÃÒàÊÕªÕǵ¶Ö§ÃŒÍÂÅÐ 15-20
Œ † Ñ Ô
àǪÈÒʵ÷¹Âؤ 2553
Ñ 563
¡Òû‡Í§¡Ñ¹àÅ×Í´ÍÍ¡«éíÒ (secondary prophylaxis)
¼Ù»Ç·ÕÃÍ´ªÕǵ¨Ò¡ÀÒÇÐàÅ×Í´ÍÍ¡¨Ò¡àÊŒ¹àÅ×Í´¢Í´ã¹ËÅÍ´ÍÒËÒûÃÐÁÒ³ 1 ã¹ 3 ¨ÐÁÕ
Œ † è Ô
àÅ×Í´ÍÍ¡«éÒä´ŒÀÒÂã¹ 6 ÊÑ»´ÒËáÅÐÃŒÍÂÅÐ 40-60 ¢Í§¼Ù»Ç¡ÅØÁ¹Õ¨ÐàÊÕªÕǵ䴌 ´Ñ§¹Ñ¹¡Òû‡Í§¡Ñ¹
í Œ † ‹ é Ô é
àÅ×Í´ÍÍ¡«éÒ¨Ö§ÁÕ¤ÇÒÁÊíÒ¤Ñ ·Ò§àÅ×Í¡¢Í§¡Òû‡Í§¡Ñ¹ 䴌ᡋ ¡ÒÃʋͧ¡ÅŒÍ§ ¡ÒÃãËŒÂÒ non-selective
í
ß-blocker + nitrate, TIPS ËÃ×Í¡Òü‹ÒµÑ´ ¶Ö§áÁŒ¨ÐÁÕ·Ò§àÅ×Í¡Áҡᵋ͵ÃÒ¡ÒÃàÊÕªÕǵ¡çÁ䴌Ŵ¹ŒÍÂ
Ñ Ô Ô
ŧÍ‹ҧªÑ´à¨¹ áÊ´§ãËŒàËç¹Ç‹Ò¼Ù»Ç¡ÅØÁ¹ÕÁ¡àÊÕªÕǵà¹×ͧ¨Ò¡¤ÇÒÁÃعáç¢Í§µÑÇâäàͧÁÔ㪋¨Ò¡
Œ † ‹ é Ñ Ô è
àÅ×Í´ÍÍ¡â´ÂµÃ§
¡ÒÃ㪌ÂÒ non-selective ß-blocker ઋ¹ propranolol ¤ÇÃà¾ÔÁ¢¹Ò´ÂÒ¨¹ÊÒÁÒöŴªÕ¾¨Ãŧ
è
ÃŒÍÂÅÐ 25 ËÃ×ÍÁÕ͵ÃҢͧªÕ¾¨Ã 50-55 ¤Ãѧ/¹Ò·Õ ʋǹ nadolol 䴌ú¤ÇÒÁ¹ÔÂÁÁÒ¡¢Ö¹à¹×ͧ¨Ò¡ãËŒ
Ñ é Ñ é è
¡Ô¹ÇѹÅФÃѧ䴌·ÒãËŒÊдǡ¡Ñº¼Ù»Ç (ᵋÂÒ¹ÕäÁ‹Áã¹»ÃÐà·Èä·Â) ã¹ÃÒ·ÕÁ¼Å¢ŒÒ§à¤Õ§¢Í§ÂÒËÃ×Í
é í Œ † é Õ è Õ
ÁÕ¢ÍËŒÒÁ㹡ÒÃ㪌ઋ¹à»š¹âä¶Ø§ÅÁ⻆§¾Í§ ÊÒÁÒöãËŒÂÒ isosorbide mononitrate ËÇÁä´Œ ¾ºÇ‹Ò
Œ
¨Ðª‹ÇÂÅ´ portal pressure ä´Œ´Õ¢Öé¹àÁ×èÍà·Õº¡Ñº¡ÒÃ㪌 propranolol Í‹ҧà´ÕÂÇ Ê‹Ç¹¡ÒáíҨѴ
àÊŒ¹àÅ×Í´¢Í´ã¹ËÅÍ´ÍÒËÒÃâ´Â¡ÒÃʋͧ¡ÅŒÍ§áÅзíÒ EVS ËÃ×Í EVL ¤Ç÷íÒ·Ø¡ 3-4 ÊÑ»´Ò˨¹¡Ãзѧ è
äÁ‹ÁÕàÊŒ¹àÅ×Í´¢Í´ËÅѧ¨Ò¡¹Ñ鹤Ç÷íÒ¡ÒÃʋͧ¡ÅŒÍ§«éíÒ·Ø¡ 6 à´×͹ ¡ÒÃÈÖ¡ÉÒà¾×èÍà»ÃÕºà·Õº
»ÃÐÊÔ·¸ÔÀÒ¾¢Í§ÇÔ¸¡Òû‡Í§¡Ñ¹µ‹Ò§æ ÊÃØ»Ç‹Ò ¡ÒÃ㪌 non-selective ß-blocker ËÇÁ¡Ñº EVL ¹Ñ¹ÁÕ
Õ é
»ÃÐÊÔ·¸ÔÀÒ¾·Õ´·Ê´ ÊíÒËÃѺ¼Ù»Ç·Õ§ÁÕàÅ×Í´ÍÍ¡«éҷѧæ·Õ䴌ú·Ñ§ÂÒáÅСÒÃʋͧ¡ÅŒÍ§áÅŒÇ á¹Ð¹íÒ
è Õ Õè Ø Œ † è Ñ í é è Ñ é
ãËŒ·Ò TIPS ʋǹ¡Ò÷íÒ¡Òü‹ÒµÑ´ shunt ¹Ñ¹ ¾ºÇ‹Òª‹ÇÂÅ´âÍ¡ÒÊà¡Ô´àÅ×Í´ÍÍ¡«éÒᵋäÁ‹ä´ŒÅ´ÍѵÃÒ
í é í
¡ÒÃàÊÕªÕǵ¨Ö§¤Ç÷íÒ㹼ٻǷÕäÁ‹µÍºÊ¹Í§µ‹Í¡ÒÃÃÑ¡ÉÒ´ŒÇÂÇԸ͹áÅŒÇ෋ҹѹ ¹Í¡¨Ò¡¹Ñ¹ã¹¼Ù»ÇÂ
Ô Œ † è Õ ×è é é Œ †
·ÕÁÀÒÇÐàÅ×Í´ÍÍ¡«éÒ¤ÇþԨÒóҡÒÃà»ÅÕ¹µÑº (liver transplantation) ËÇÁ´ŒÇÂ
è Õ í è
568 Embolization for Upper Gastrointestinal Hemorrhage
¢Í§¡ÒÃÃÑ¡ÉÒ´ŒÇÂÇÔ¸¡ÒÃÍØ´¡Ñ¹ËÅÍ´àÅ×Í´àÁ×Íà·Õº¡Ñº¡ÒÃʋͧ¡ÅŒÍ§àÍç¹â´Ê⤻ËÃ×Í¡Òü‹ÒµÑ´¤×Í
Õ é è
äÁ‹ÊÒÁÒö·íÒä´Œá¾Ã‹ËÅÒÂã¹âç¾ÂÒºÒÅ·ÑÇæ ä» Â¡àÇŒ¹Ê¶ÒºÑ¹·Ò§¡ÒÃá¾·ÂãË‹æ ËÃ×ÍâçàÃÕ¹
è
á¾·Âà·‹Ò¹Ñé¹ ¡ÒÃÃÑ¡ÉÒÀÒÇÐàÅ×Í´ÍÍ¡ã¹·Ò§à´Ô¹ÍÒËÒäÇ÷íÒ¡ÒÃÍØ´¡Ñé¹ËÅÍ´àÅ×ʹËÇÁ¡Ñº
¡ÒÃʋͧ¡ÅŒÍ§àÍç¹â´Ê⤻ 㹡óբͧ¼Ù»Ç·ÕÁÕ massive arterial bleeding ¤Ç÷íÒ angiography
Œ † è
áÅÐ embolization ¡‹Í¹ ʋǹ¼Ù»Ç intermittent bleeding ¤ÇÃ䴌ú¡ÒÃʋͧ¡ÅŒÍ§àÍç¹â´Ê⤻¡‹Í¹
Œ † Ñ
´Ñ§¹Ñé¹ ¤ÇÒÁÊíÒàÃç¨ã¹¡ÒÃÃÑ¡ÉÒ¼ÙŒ»†Ç¨֧¢Öé¹ÍÂÙ‹¡Ñº¤ÇÒÁËÇÁÁ×͡ѹÍ‹ҧ´ÕÃÐËÇ‹Ò§ÍÒÂØÃá¾·ÂáÅÐ
ÈÑÅÂá¾·ÂÃкº·Ò§à´Ô¹ÍÒËÒà ËÇÁ¡ÑºÃѧÊÕᾷ´ҹÃѧÊÕÃÇÁÃÑ¡ÉÒ
Œ ‹
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Baum ST. Arteriographic diagnosis and treatment of gastrointestinal bleeding. In: Baum ST, Pentecost MJ,
eds. Abram’s angiography interventional radiology. 2nd ed. Philadelphia, Pa: Lippincott, Williams & Wilkins,
2006;488-513.
2. Lee EW, Laberge JM. Differential diagnosis of gastrointestinal bleeding. Tech Vasc Interv Radiol 2005;7:112-
22.
3. Kuo W, Lee DE, Saad WE, Patel N, Sahler lG, Waldman DL. Superselective microcoil embolization for the
treatment of lower gastrointestinal hemorrhage. J Vasc Interv Radiol 2003;14:1503-9.
596.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 569
77
General Aspects of Tumor Microenvironment
Assistant Professor Peti Thuwajit, M.D. Ph.D.
Department of Immunology, .aculty of Medicine Siriraj Hospital, Mahidol University
Cancer is still a major problem in medicine. It is the leading cause of death in Thai
people within many years. Cancer cells could be developed from each cell type in the whole
body, especially epithelial cells. Normally epithelial cells could function as protector and
transporter, which supported by a various type of the cells beneath and nearby including connective
tissue cells, vascular cells and muscle cells. When tissues are going to pathological stage, the
immunological cells will infiltrate and play role in both promoting and repairing of the abnormal
conditions. This could be showing as inflammation and repairing processes, including fibrosis
and angiogenesis, even though the pathological stage is still exist. Carcinogenesis is one of the
inflammatory conditions which involved a numbers of cells. After epithelial cells turning to
malignant, the cancer cells will be going to infiltrate the underlying tissue layers and the cells
lying beneath become closer. They still have interaction with neighboring cells and environment
and also need supporting from their surrounding environment too.(1,2) On the other hand,
microenvironment in tumor area could suppress or destroy the cancer cells too.(1,2) The major
cells that play roles in tumor progression are including the resident cells and the infiltrated
migratory cell, for example, the circulating immunological cells. The most common resident cell
found in tumor microenvironment is fibroblast.(3) It could not only produce collagens and
extracellular matix for structural support but it could also produce a lot of peptides or small
signaling molecules that could affect tumor cell growth, survival and metastasis.(3,4) So the
control of fibroblast should be a target for cancer management.(5) Immunological cells are the
most abundant infiltrating cell in tumor microenvironment. Some of immunological cells are
residence, for example, macrophages and dendritic cells. The immunological cells which are
the major infiltrating cell in tumor microenvironment are including polymorphonuclear cells and
lymphocytes. One of the examples of the importance of immunological cells in tumor biology is
from the recent studies that showed the effect of NKG2D ligand expression in tumor biology.(6)
597.
570 General Aspects of Tumor Microenvironment
NKG2D is the lectin family receptor presented on membrane of many types of immune cells
including natural killer (NK) cells, cytotoxic T lymphocyte, !" T lymphocyte, macrophages and
some groups of helper T cell. The finding showed that regulation of NKG2D by NKG2D ligends
could affect the activity of NK cell and tumor survival. (6) In Thai people there are a polymorphism
of many types of NKG2D ligands have been reported.(7,8)
There are not only cells play role in tumor microenvironment, the extracellular matrix
molecules are also having the effect on tumor progression. Collagen could retard the migration
of cancer cells by its structure but it may promote epithelial-mesenchymal transition (EMT) and
stimulate cell migration by itself.(9) Small molecules which have cell signaling effects to tumor
cells are using this space for their actions. These small molecules could be proteins, peptides,
steroids, etc. They could regulate tumor cell growth, metastasis and also angiogenesis. Some
proteins could help tumor cells evade from immune system. One of the examples for this group
of protein is mucin. Mucin is a family of protein with heavy glycosylation. MUC1 is a mucin
found in many types of cancers, including cholangiocarcinoma. It has been hypothesized that
MUC1 production could protect tumor cells from the recognition by immune cell due to its
glycosylation as a barrier for detection.(10) In cholangiocarcinoma, MUC1 has been reported its
association with poor prognosis.(10,11) Unlike MUC1, MUC5AC and MUC6 are mucins found
increased expression in cholangiocarcinoma too but they did not show the association with
poor prognosis.(11-13) MUC6 seems to associate with good prognosis of cholangiocarcinoma in
one study.(13)
Trefoil factor family is a group of protein that could regulate the migration and invasion
in cancer metastasis process. T..1 and T..2 are found in cholangiocarcinoma but not show
association with survival of the patients.(12,13) However, due to their function, T..s are considered
as a target for study their roles in cancer metastasis. Another interesting protein is periostin, a
protein that could be produced from cancer cells and fibroblast in extracellular matrix and has
many effects to cancer including activation of cell growth, induce invasion and promote
angiogenesis. It has been reported the over-expression in cholangiocarcinoma with in vitro tumor
promoting effect.(14)
Tumor metastasis and angiogenesis are the hot topic for studying. Both processes are
needed tumor microenvironment for promoting their progression. So, tumor microenvironment
should involve in all steps of tumor progression and cells or molecules inside should be considered
as targets for studying and controlling of tumor progression. In this session will discuss about
tumor microenvironment in the current study and its propose as the target for cancer therapy.
598.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 571
References
1. Mbeunkui ., Johann DJ Jr. Cancer and the tumor microenvironment: a review of an essential relationship.
Cancer Chemother Pharmacol. 2009;63(4):571-82.
2. Witz IP. The tumor microenvironment: the making of a paradigm. Cancer Microenviron. 2009;2 Suppl 1:
9-17.
3. Pietras K, Ostman A. Hallmarks of cancer: interactions with the tumor stroma. Exp Cell Res. 2010;316(8):1324-
31.
4. Chuaysri C, Thuwajit P, Paupairoj A, Chau-In S, Suthiphongchai T, Thuwajit C. Alpha-smooth muscle actin-
positive fibroblasts promote biliary cell proliferation and correlate with poor survival in cholangiocarcinoma.
Oncol Rep. 2009;21(4):957-69.
5. Plz?k J, Lacina L, Chovanec M, Dvor?nkov? B, Szabo P, Cada Z, Smetana K Jr. Epithelial-stromal interaction
in squamous cell epithelium-derived tumors: an important new player in the control of tumor biological properties.
Anticancer Res. 2010;30(2):455-62.
6. Champsaur M, Lanier LL. Effect of NKG2D ligand expression on host immune responses. Immunol Rev.
2010;235(1):267-85.
7. Romphruk AV, Romphruk A, Naruse TK, Raroengjai S, Puapairoj C, Inoko H, Leelayuwat C. Polymorphisms
of NKG2D ligands: diverse RAET1/ULBP genes in northeastern Thais. Immunogenetics. 2009;61(9):
611-7.
8. Jumnainsong A, Romphruk AV, Jearanaikoon P, Klumkrathok K, Romphruk A, Luanrattanakorn S, Leelayuwat
C. Association of polymorphic extracellular domains of MICA with cervical cancer in northeastern Thai population.
Tissue Antigens. 2007;69(4):326-33.
9. Medici D, Nawshad A. Type I collagen promotes epithelial-mesenchymal transition through ILK-dependent
activation of N.-kappaB and LE.-1. Matrix Biol. 2010;29(3):161-5.
10. Park SY, Roh SJ, Kim YN, Kim SZ, Park HS, Jang KY, Chung MJ, Kang MJ, Lee DG, Moon WS. Expression
of MUC1, MUC2, MUC5AC and MUC6 in cholangiocarcinoma: prognostic impact. Oncol Rep. 2009;22(3):
649-57.
11. Boonla C, Sripa B, Thuwajit P, Cha-On U, Puapairoj A, Miwa M, Wongkham S. MUC1 and MUC5AC mucin
expression in liver fluke-associated intrahepatic cholangiocarcinoma. World J Gastroenterol. 2005 28;11(32):4939-
46.
12. Thuwajit P, Chawengrattanachot W, Thuwajit C, Sripa B, May .E, Westley BR, Tepsiri NN, Paupairoj A,
Chau-In S. Increased T..1 trefoil protein expression in Opisthorchis viverrini-associated cholangiocarcinoma is
important for invasive promotion. Hepatol Res. 2007;37(4):295-304.
13. Thuwajit P, Chawengrattanachot W, Thuwajit C, Sripa B, Paupairoj A, Chau-In S. Enhanced expression of
mucin 6 glycoprotein in cholangiocarcinoma tissue from patients in Thailand as a prognostic marker for
survival. J Gastroenterol Hepatol. 2008;23(5):771-8.
14. Utispan K, Thuwajit P, Abiko Y, Charngkaew K, Paupairoj A, Chau-in S, Thuwajit C. Gene expression profiling
of cholangiocarcinoma-derived fibroblast reveals alterations related to tumor progression and indicates periostin
as a poor prognostic marker. Mol Cancer. 2010;9:13.
600.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 573
78
Cancer-associated .ibroblasts in Tumor Progression
Assistant Professor Chanitra Thuwajit, Ph.D., M.D.
Department of Immunology .aculty of Medicine Siriraj Hospital, Mahidol University
Tumor progression requires a crosstalk between cancer cells and tumor microenvironment
via several interactions of both cell-to-cell and substance-to-cell manners. Among these interactions,
cancer-associated fibroblasts (CA.s) are the most attention both as recipients to the signals
from cancer cells, immune cells and extracellular matrix (ECM); and as producers of pro-
tumorigenic signals which can facilitate the progression and aggressiveness of the cancers.
The purpose of this talk is to introduce the importance of CA.s in cancer which have
been made during the last several years. These include the explanation of what CA.s originate
from, the specific characters and genetic status of CA.s, and roles of CA.s in particular in
cancer progression. The translational studies of using CA.s as therapeutic targets is of great
interest to mention herein. .inally, our data of CA.s in cholangiocarcinoma (CCA) which is
nowadays the major health problem in the North and Northeastern parts of the country will be
mentioned.
The origin of CA.s
CA.s are simply defined as fibroblasts found in cancers. They have specific characters
in particular the expression of activated fibroblast markers importantly !-smooth muscle actin
(!-SMA), fibroblast-activated protein (.AP). Several researches indicate distinct CA.s subsets
probably originated from different sources. There are three main explanations regarding the
origin of CA.s. Local fibroblasts or fibroblast precursors, stimulated by members of growth
factors and cytokines, have generally been considered as the major source of CA.s.
The experiment in mouse models demonstrated bone marrow-derived precursor cells in the
contribution of CA.s population.(1) Moreover, it has been suggested that CA.s are derived from
malignant epithelial cells or endothelial cells undergoing mesenchymal transitions. (2, 3)
601.
574 Cancer-associated .ibroblasts in Tumor Progression
The genetic alterations of CA.s
What is egg or chicken between the abnormalities of CA.s and the mutations occurred
in tumor cells is still not clear. The controversial results showed that characters of CA.s have
been maintained both in the absence and the presence of malignant cells. In case of CA.s
stability in the absence of malignant cells, the genetic and epigenetic alterations within CA.s
are involved. Using microdissected fibroblasts from breast cancer and head and neck squamous
cell carcinoma, p53 mutations and loss-of-heterozygosity are common events.(4, 5) Moreover,
epigenetic alterations in CA.s have been detected from fibroblasts isolated from breast and
prostate cancers.(6, 7)
Roles of CA.s in cancer progression
There is a complex interplay of reciprocal stromal-epithelial interactions resulting in
changes in the ECM and the tumor stroma. Carcinogenesis arises from the loss or breakdown
of this interaction rather than from epithelial or stromal mutation alone.(8) Several studies in
mouse models of genetically altered fibroblasts demonstrated a direct involvement of resident
fibroblasts in the initiation of cancer. However, many more research works so far have been
performed and indicated roles of CA.s in cancer progression. It is more than believable that
CA.s are sources of secreted growth factors, ECM-degrading proteases, invasive factors, and
angiogenic factors. .or example, CA.s are known to produce insulin-like growth factors in head
and neck cancer.(9) The ECM components such as various types of collagen have been
demonstrated the cross-link to the malignant cells which then cause integrin ligation leading to
PI3K and AKT survival signaling pathways. Matrix metalloproteases (MMPs), cathepsins, and
plasminogen activators are produced from CA.s and needed for cancer invasion and
metastasis.(10) To induce neovascular formation and the recruitment of endothelial progenitor
cells, CA.s are sources of vascular endothelial growth factors, fibroblast growth factor-2, and
stomal-derived factor-1.
Clinical implications of CA.s
The more evidence of CA.s in the progression of several cancers leading to the provincing
value of using CA.s in the clinical application. A key study regarding gene expression profile in
breast cancer revealed the significance of genes expressed in stromal cells as prognostic
predictors.(11) In addition, in colorectal cancer CA.s abundance has been shown to associate
with bad prognosis.(12, 13)
602.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 575
CA.s can be the therapeutic targets through either the interfering with the recruitment
or expansion of CA.s in cancer tissues or the interfering with secreted CA.s-derived pro-
tumorigenic signals. Members of the platelet-derived growth factor (PDG.) family of growth
factors are well established regulator of tumor fibroblasts and pericytes.(14) Targeting of stromal
PDG. receptors, in experimental tumors, increase tumor drug uptake. In addition, inhibition of
stromal PDG. receptors induce anti-tumoral effects in cervix and colorectal cancers. Several
tyrosine kinase inhibitors with anti-PDG.R activity, such as imatinib, sorafenib, and sunitinib,
are presently approved and under clinical development.
Recently, CA.s have been proven to secrete CXCL14 chemokine(15), suggesting this
protein and its yet-to-be identified receptor as the targets for inhibition. Newly published studies
have been performed to find out the specific signal pathway in CA.s to be inhibited including a
recent finding of hedgehog-signaling as a novel pathway for anti-stromal therapy.(16) .inally,
immunotherapy-approached have been employed to target CA.s in particular .AP antibody are
the most attractive candidate drug with the committed effects in animal models.(17) Though
clinical studies are more needed, it is promising for targeting CA.s as the treatment in cancer
patients.
Cholangiocarcinoma-associated fibroblasts and role in cancer
progression
Our group has recently reported the in vitro tumorigenic effects of CA.s derived from
CCA patients through both contact and non-contact fashions.(18) In addition, the result supported
the previous findings in other cancers that the abundance of !-SMA positive fibroblasts correlated
to the short survival time of CCA patients. In order to identify the tumorigenic genes in CCA
fibroblasts, the gene expression profile of CA.s isolated from CCA patients undergone
hepatectomy was performed in comparison to that of normal fibroblasts.(19) Oligonucleotide
microarrays were used and certain genes involved in induction of cancer progression have been
proposed. Of most interest, periostin (PN) has been confirmed the expression in only CA.s
whereas no expressions in cancer cells or other stromal cells. In addition, patients who have
high level of PN had shorter survival time than the ones with low PN level. The in vitro studies
on roles of PN indicated the effects of PN to induce cancer cell proliferation and invasion.
Taken together, it is promising that in CCA, fibroblasts take part in cancer progression and
fibroblast-derived substances at least PN could be used as the poor prognostic markers. The
mechanism of action of PN on CCA cells and its effect in induction of MMPs are under
investigating in our lab. In addition, the other CA.s-derived substances in particular growth
603.
576 Cancer-associated .ibroblasts in Tumor Progression
factors, cytokines, chemokines represented from the oligonucleotide microarray and from the
study using protein chip assay (unpublished data) are of value to explore their roles in CCA. The
ultimate goal is to challenge targeting CA.s to attenuate tumorigenic induction and progression
in CCA patients.
References
1. Direkze NC, Hodivala-Dilke K, Jeffery R, Hunt T, Poulsom R, Oukrif D, et al. Bone marrow contribution to
tumor-associated myofibroblasts and fibroblasts. Cancer Res. 2004;64(23):8492-5.
2. Radisky DC, Kenny PA, Bissell MJ. .ibrosis and cancer: do myofibroblasts come also from epithelial cells via
EMT? J Cell Biochem. 2007;101(4):830-9.
3. Zeisberg EM, Potenta S, Xie L, Zeisberg M, Kalluri R. Discovery of endothelial to mesenchymal transition as
a source for carcinoma-associated fibroblasts. Cancer Res. 2007;67(21):10123-8.
4. Patocs A, Zhang L, Xu Y, Weber ., Caldes T, Mutter GL, et al. Breast-cancer stromal cells with TP53
mutations and nodal metastases. N Engl J Med. 2007;357(25):2543-51.
5. Weber ., Xu Y, Zhang L, Patocs A, Shen L, Platzer P, et al. Microenvironmental genomic alterations and
clinicopathological behavior in head and neck squamous cell carcinoma. JAMA. 2007;297(2):187-95.
6. Hu M, Yao J, Cai L, Bachman KE, van den Brule ., Velculescu V, et al. Distinct epigenetic changes in the
stromal cells of breast cancers. Nat Genet. 2005;37(8):899-905.
7. Hanson JA, Gillespie JW, Grover A, Tangrea MA, Chuaqui R., Emmert-Buck MR, et al. Gene promoter
methylation in prostate tumor-associated stromal cells. J Natl Cancer Inst. 2006;98(4):255-61.
8. Weaver VM, Gilbert P. Watch thy neighbor: cancer is a communal affair. J Cell Sci. 2004;117(Pt 8):1287-90.
9. Strnad H, Lacina L, Kolar M, Cada Z, Vlcek C, Dvorankova B, et al. Head and neck squamous cancer stromal
fibroblasts produce growth factors influencing phenotype of normal human keratinocytes. Histochem Cell Biol.
2010;133(2):201-11.
10. Joyce JA, Pollard JW. Microenvironmental regulation of metastasis. Nat Rev Cancer. 2009;9(4):239-52.
11. .inak G, Bertos N, Pepin ., Sadekova S, Souleimanova M, Zhao H, et al. Stromal gene expression predicts
clinical outcome in breast cancer. Nat Med. 2008;14(5):518-27.
12. Tsujino T, Seshimo I, Yamamoto H, Ngan CY, Ezumi K, Takemasa I, et al. Stromal myofibroblasts predict
disease recurrence for colorectal cancer. Clin Cancer Res. 2007;13(7):2082-90.
13. Henry LR, Lee HO, Lee JS, Klein-Szanto A, Watts P, Ross EA, et al. Clinical implications of fibroblast
activation protein in patients with colon cancer. Clin Cancer Res. 2007;13(6):1736-41.
14. Ostman A, Heldin CH. PDG. receptors as targets in tumor treatment. Adv Cancer Res. 2007;97:247-74.
15. Augsten M, Hagglof C, Olsson E, Stolz C, Tsagozis P, Levchenko T, et al. CXCL14 is an autocrine growth
factor for fibroblasts and acts as a multi-modal stimulator of prostate tumor growth. Proc Natl Acad Sci U S A.
2009;106(9):3414-9.
16. Rudin CM, Hann CL, Laterra J, Yauch RL, Callahan CA, .u L, et al. Treatment of medulloblastoma with
hedgehog pathway inhibitor GDC-0449. N Engl J Med. 2009;361(12):1173-8.
17. Loeffler M, Kruger JA, Niethammer AG, Reisfeld RA. Targeting tumor-associated fibroblasts improves cancer
chemotherapy by increasing intratumoral drug uptake. J Clin Invest. 2006;116(7):1955-62.
604.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 577
18. Chuaysri C, Thuwajit P, Paupairoj A, Chau-In S, Suthiphongchai T, Thuwajit C. Alpha-smooth muscle actin-
positive fibroblasts promote biliary cell proliferation and correlate with poor survival in cholangiocarcinoma.
Oncol Rep. 2009;21(4):957-69.
19. Utispan K, Thuwajit P, Abiko Y, Charngkaew K, Paupairoj A, Chau-in S, et al. Gene expression profiling of
cholangiocarcinoma-derived fibroblast reveals alterations related to tumor progression and indicates periostin as
a poor prognostic marker. Mol Cancer. 2010;9:13.
582 Digital ImageProcessing and Data Management for Clinical Registry and Clinical Research
ã¹á§‹¢Í§¼Ù㪌¨ÐàËç¹Ç‹Ò ¢Ñ¹µÍ¹ã¹¡ÒáÃÍ¡¢ŒÍÁÙÅŧà¤Ã×ͧ¤ÍÁ¾ÔÇàµÍèÐËÒÂä» ¼Ù㪌¨ÐÃÙÊ¡
Œ é è Œ ŒÖ
àÊÁ×Í¹Ç‹Ò ¢ŒÍÁÙÅ·Õ¡Ã͡ŧ¡ÃдÒɨж١á»Å§ãˌ໚¹¢ŒÍÁÙÅã¹ÃÙ»´Ô¨µÍÅ ¾ÃŒÍÁÊíÒËÃѺ¡ÒùíÒä»ãªŒ§Ò¹
è Ô
ä´Œ·Ñ¹·Õ ¹Í¡¨Ò¡¹ÕéÃкº¡ÒÃÊ᡹ÀÒ¾·íҧҹ䴌ÃÇ´àÃçÇ¡Ç‹Ò¡ÒÃ㪌਌Ò˹ŒÒ·Õè¡ÃÍ¡¢ŒÍÁÙÅÁÒ¡
ẺÊͺ¶ÒÁ¨íҹǹ¡Ç‹Ò 2,000 ªØ´ÊÒÁÒöá»Å§áÅйíÒ¢ŒÍÁÙÅä»ÇÔà¤ÃÒÐ˼Åä´ŒÀÒÂã¹ 2 Çѹ
´ŒÇ¤ÇÒÁáÁ‹¹ÂíÒ¡Ç‹ÒÃŒÍÂÅÐ 99.5 ´ŒÇÂÃкºÊ᡹·Õ¾²¹Ò¢Ö¹¹Õé ¼Ù㪌¨§ÊÒÁÒö·ØÁà·ä»·Õ»ÃÐà´ç¹
è Ñ é Œ Ö ‹ è
ÊíҤѢͧâ¤Ã§¡Òà 䴌ᡋ¡ÒÃÍ͡ẺáÅеѴÊԹ㨠à¾×èÍà¡çº¢ŒÍÁÙÅãËŒ¤Ãº¶ŒÇ¹áÅÐà¡Ô´»ÃÐ⪹
ÇҧἹ¡ÒÃÇÔà¤ÃÒÐËáÅСÒ÷íÒÃÒ§ҹ·ÕÁ»ÃÐÊÔ·¸ÔÀÒ¾ â´ÂäÁ‹µÍ§¡Ñ§ÇšѺ§Ò¹¡ÃÍ¡¢ŒÍÁÙÅ·Õ§ÂÒ¡
è Õ Œ è Ø‹
áÅÐÁÕâÍ¡ÒʼԴ¾ÅÒ´ÊÙ§
ÃкºÊ᡹ÀÒ¾¢Í§Ë¹‹ÇªÕÇÊÒÃʹà·È
ã¹Ê‹Ç¹µ‹Í¨Ò¡¹Õé ¼Ùà¢Õ¹¨Ð͸ԺÒÂÃÒÂÅÐàÍÕ´¢Í§ÃкºÊ᡹ ÊíÒËÃѺ·‹Ò¹¼Ùʹ㨡Ò÷íÒ§Ò¹
Œ Œ
¢Í§Ãкº «Ö§¨Ðä´Œ·ÃÒº¶Ö§à·¤â¹âÅÂշ㪌áÅТŒÍ¨íÒ¡Ñ´·ÕÁÍÂÙã¹¢³Ð¹Õé
è Õè è Õ ‹
¡ÒÃÊ᡹ÀÒ¾
ÀÒ¾·ÕÊ᡹ࢌÒÁÒÊÙÃкº¨Ð¶Ù¡á»Å§ãˌ໚¹ÀÒ¾¢ÒÇ´íÒ ¤ÇÒÁÅÐàÍÕ´ 200 dpi «Ö§à¾Õ§¾Í
è ‹ è
·Õ¨Ð¹íÒä»ãªŒã¹¡ÒûÃÐÁÇżÅÀÒ¾áÅÐÍ‹Ò¹ÅÒÂÁ×Íâ´ÂÃкºà¤Ã×Í¢‹ÒÂã»ÃÐÊÒ· (neural network)
è
áÅÐÁÕ¢¹Ò´äÁ‹ãË‹à¡Ô¹ä» à¾×ͤÇÒÁàÃçÇ㹡ÒÃÃѺʋ§¢ŒÍÁÙÅáÅлÃÐËÂÑ´¾×¹·Õà¡çº¢ŒÍÁÙÅã¹à¤Ã×ͧáÁ‹¢ÒÂ
è é è è ‹
(server)
¡ÒÃÍ‹Ò¹ºÒÃ⤌´
ÀÒ¾·Õ¶¡Ê᡹ࢌÒÁҨж١¹íÒä»»ÃÐÁÇżŴŒÇÂâ»Ãá¡ÃÁÍ‹Ò¹ºÒÃ⤌´ ·ÕÍÂÙÊǹº¹¢Í§áºº
è Ù è ‹‹
¿ÍÃÁ ´Ñ§µÑÇÍ‹ҧÃÙ»·Õè 1
610.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 583
ÃÙ»·Õè 1 áÊ´§ÀҾẺ¿ÍÃÁ¡ÃдÒÉáÅкÒÃ⤌´
à¾×èÍãËŒÃкº·ÃҺNjÒẺ¿ÍÃÁ·ÕèÊ᡹ࢌÒÁÒ¹Ñé¹à»š¹¢Í§â¤Ã§¡ÒÃã´ áÅÐÁÕ¨íҹǹ¡Õè˹ŒÒ
à¾×Í㪌㹡ÒõÃǨÊͺNjÒÀÒ¾·ÕÊ᡹ࢌÒÁÒÁըҹǹ˹ŒÒ¤Ãº¶ŒÇ¹ËÃ×ÍäÁ‹
è è í
¡ÒûÃѺᵋ§ÀÒ¾
àÁ×͵ÃǨÊͺÃËÑʺÒÃ⤌´áÅФÇÒÁ¤Ãº¶ŒÇ¹àÃÕºÌÍÂáÅŒÇ ÀÒ¾¨Ð¶Ù¡Ê‹§µ‹ÍÁÒÂѧâ»Ãá¡ÃÁ
è
·ÕÊͧ à¾×Í»ÃÐàÁÔ¹ÀҾNjÒÁÕ¨´ÊÑÒ³¡Ç¹ (noise) ÁÒ¡¨¹ÍÒ¨¨Ðú¡Ç¹¡ÒÃá»Å§¢ŒÍÁÙÅËÃ×ÍäÁ‹
è è Ø
¶ŒÒËÒ¡ÁÕÁÒ¡à¡Ô¹ä» ¨Ð㪌෤¹Ô¤ã¹¡ÒèѴ¡ÒÃÀÒ¾à¾×ÍÅ´¨Ø´Ãº¡Ç¹Å§ (despeckle) áÅлÃÐàÁԹNjÒ
è
ÀÒ¾àÍÕ Â §ËÃ× Í äÁ‹ «Öè § ໚ ¹ »˜ ËÒ·Õè ¾ ºº‹ Í Â à¹×è Í §¨Ò¡¡Ò÷í Ò §Ò¹¢Í§ÅÙ ¡ ¡ÅÔé § ´Ö § ¡ÃдÒɢͧ
à¤Ã×ͧÊ᡹à¹Í÷ҧҹäÁ‹ÊÍ´¤ÅŒÍ§¡Ñ¹ »˜ËÒÁÑ¡¨Ðà¡Ô´¢Ö¹àÁ×ÍÁÕ¡ÒÃÍÒÂØ㪌§Ò¹¢Í§ÅÙ¡¡ÅÔ§à¾ÔÁÁÒ¡¢Ö¹
è í é è é è é
ËÃ×Í໚¹»˜ËÒ·Õ¡ÃдÒÉàͧ ·ÕÍÒ¨¨ÐÁÕÃÍÂÂѺ ËÒ¡ÀÒ¾·ÕÊ᡹ࢌÒÁÒàÍÕ§à¡Ô¹ä»¨Ð·íÒãËŒµÒá˹‹§
è è è í
·Õè ¡í Ò Ë¹´äÇŒ Êí Ò ËÃÑ º ¡ÒÃá»Å§¢Œ Í ÁÙ Å ¤ÅÒ´à¤Å×è Í ¹¨Ö § µŒ Í §ãªŒ à ·¤¹Ô ¤ ¡Òäí Ò ¹Ç³Ç‹ Ò ÀÒ¾àÍÕ Â §ä»
¡ÕͧÈÒáÅÐËÁعÀÒ¾à¾×Íãˌ䴌ÀÒ¾·ÕÍÂÙã¹á¹ÇµÑ§
è è è ‹ é
611.
584 Digital ImageProcessing and Data Management for Clinical Registry and Clinical Research
¡Òô֧¢ŒÍÁÙŨҡµíÒá˹‹§·Õè¡íÒ˹´äÇŒÊíÒËÃѺá»Å§¢ŒÍÁÙÅ
¢ŒÍÁÙŨҡÀÒ¾·Õ¶¡»ÃѺãËŒàËÁÒÐÊÁáŌǨж١´Ö§ÍÍ¡ÁÒ¨Ò¡µíÒá˹‹§µ‹Ò§ æ ·Õ¡Ò˹´äÇŒáÅŒÇ
è Ù è í
â´ÂàÁ×ÍÃкº·íҧҹ䴌¶¡µŒÍ§ ÀÒ¾·ÕÍÂÙ㹡Ãͺ·Ø¡¡Ãͺ¨Ð¶Ù¡´Ö§ÍÍ¡ÁÒ´ŒÇ¤ÇÒÁáÁ‹¹ÂíÒ ÁÕ¤ÇÒÁ
è Ù è ‹
¼Ô´¾ÅÒ´äÁ‹à¡Ô¹ 2 ¨Ø´¾Ô¡à«Å (pixels) ´Ñ§µÑÇÍ‹ҧÃÙ»·Õè 2
¡) Checkbox ¢) ÅÒÂÁ×͵ÑÇàÅ¢
ÃÙ»·Õè 2 áÊ´§¤ÇÒÁáÁ‹¹ÂíÒ㹡ÒûÃѺµíÒá˹‹§¢Í§¡Ãͺ㹡ÒõѴ¢Íº
â´Â·ÑÇä» â»Ãá¡ÃÁã¹ÅѡɳйÕÁ¡¨Ð´Ö§¢ŒÍÁÙÅ´ŒÇ¡ÒÃ͌ҧÍÔ§µíÒá˹‹§¡Ãͺ¨Ò¡àÊŒ¹¢ÍºËÅÑ¡
è é Ñ
෋ҹѹ (ÃÙ»·Õè 1) ᵋ·Ò§Ë¹‹ÇÂÏ ¾ºÇ‹Ò¡ÒÃ͌ҧÍԧ෋ҹѹÂѧäÁ‹Á¤ÇÒÁáÁ‹¹ÂíÒ¾Í Ë¹‹ÇÂÏ ¨Ö§µŒÍ§¾Ñ²¹Ò
é é Õ
à·¤¹Ô¤ã¹¡ÒûÃѺµíÒá˹‹§ÊíÒËÃѺ¡Ãͺ·Ø¡¡ÃͺãËŒáÁ‹¹ÂíÒ¢Öé¹ ·íÒãËŒ¡ÒÃá»Å§ÅÒÂÁ×Íã¹¢Ñ鹵͹
µ‹Íä»·íҧҹ䴌¶¡µŒÍ§ÁÒ¡¢Ö¹Í‹ҧªÑ´à¨¹
Ù é
¡ÒÃÍ‹Ò¹ÅÒÂÁ×Íà¾×èÍá»Å§¢ŒÍÁÙÅÀҾ໚¹´Ô¨ÔµÍÅ
¢ŒÍÁÙÅÀÒ¾¨Ò¡áµ‹ÅСÃͺ¨Ð¶Ù¡¹íÒÁÒ»ÃÐÁÇżŴŒÇÂÃкºà¤Ã×Í¢‹ÒÂã»ÃÐÊÒ· (neural
network) à¾×è͵ѴÊԹNjÒÅÒÂÁ×Íã¹ÀÒ¾¹Ñé¹à»š¹ÍÐäà ª¹Ô´¢ŒÍÁÙÅËÅÑ¡·Õè˹‹ÇÂÏ㪌§Ò¹ÍÂÙ‹ã¹¢³Ð¹Õé¤×Í
¢ŒÍÁÙÅ»ÃÐàÀ· checkbox áÅеÑÇàÅ¢ ¡ÒûÃÐÁÇżŠcheckbox ¹Ñ鹨Ч‹Ò¡NjҡÒÃÍ‹Ò¹ÅÒÂÁ×Í
µÑÇàÅ¢ÁÒ¡ ¨Ö§äÁ‹à»š¹»˜ËÒà·‹Ò㴹ѡ ᵋ¡ÒÃÍ‹Ò¹ÅÒÂÁ×͵ÑÇàÅ¢ÁÕ¤ÇÒÁ«Ñº«ŒÍ¹ÁÒ¡ áÅÐâ»Ãá¡ÃÁ
612.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 585
Í‹Ò¹ÅÒÂÁ×Í·Õè«×éÍÅÔ¢ÊÔ·¸Ôì¨Ò¡µ‹Ò§»ÃÐà·È¡çäÁ‹ÊÒÁÒöãËŒ¼Å´Õà·‹Ò·ÕèºÃÔÉÑ·¡Å‹ÒÇ͌ҧ à¾ÃÒСÒÃà¢Õ¹
µÑÇàÅ¢¢Í§¤¹ä·Â¨ÐÁÕ¤ÇÒÁᵡµ‹Ò§¨Ò¡µ‹Ò§»ÃÐà·È ઋ¹¤¹ä·Âà¢Õ¹àÅ¢ 1 áÅÐ 2 ËÅÒÂẺ
ÁÑ¡¨Ðà¢Õ¹àÅ¢ 7 Ẻ·ÕÁ¢´¤Ñ¹µÃ§¡ÅÒ§ àÅ¢ 9 ·Õà¢Õ¹Ëҧ⤌§ ËÃ×͵ç (ÃÙ»·Õè 3)
è Õ Õ è è
ÃÙ»·Õè 3 áÊ´§µÑÇàÅ¢·ÕèÁÕ¡ÒÃà¢Õ¹µ‹Ò§¡Ñ¹
·Ò§Ë¹‹ Ç ÂÏ ¨Ö § ½ƒ ¡ Ãкºà¤Ã× Í ¢‹ Ò Âã»ÃÐÊÒ·àͧ´Œ Ç Â¢Œ Í ÁÙ Å ÀÒ¾ÅÒÂÁ× Í ¨ÃÔ § ÁÒ¡¡Ç‹ Ò
700,000 ÀÒ¾ ·íÒãËŒ¤ÇÒÁáÁ‹¹ÂíÒ㹡ÒÃÍ‹Ò¹ÅÒÂÁ×͵ÑÇàŢ㹻˜¨¨Øº¹ÊÙ§¡Ç‹ÒÃŒÍÂÅÐ 99
Ñ
¡ÒõÃǨ·Ò¹¢ŒÍÁÙÅ
¤ÇÒÁáÁ‹¹ÂíÒÁÒ¡¡Ç‹ÒÃŒÍÂÅÐ 99 Âѧ¤§äÁ‹à¾Õ§¾ÍÊíÒËÃѺ§Ò¹·ÕÁ¤ÇÒÁÊíÒ¤ÑÁÒ¡·ÕµÍ§¡ÒÃ
è Õ è Œ
¤ÇÒÁ¶Ù¡µŒÍ§ÊÙ§ÊØ´ ¢ŒÍÁÙÅ¡ÒÃá»Å§ÀÒ¾·Ñ§ËÁ´¨Ö§¶Ù¡¹íÒÁÒµÃǨÊͺÍÕ¡¤Ãѧ´ŒÇÂ਌Ò˹ŒÒ·Õ¢Í§Ë¹‹ÇÂÏ
é é è
·íÒãˌ䴌¤³ÀÒ¾ã¹ÅѡɳТͧ¡Ò÷íÒ double data entry â´Ââ»Ãá¡ÃÁ¤ÍÁ¾ÔÇàµÍ÷Ò˹ŒÒ·Õ㹡ÒÃ
Ø í è
¡ÃÍ¡¢ŒÍÁÙŤÃÑé§áá áÅÐÁÕ¡ÒõÃǨÊͺ«éíÒ´ŒÇÂ਌Ò˹ŒÒ·Õè¢Í§Ë¹‹ÇÂÏ â´Â¡ÒÃ㪌à¤Ã×èͧÁ×͵‹Ò§ æ
·Õ˹‹ÇÂÏ ¾Ñ²¹Ò¢Ö¹ ·íÒãËŒ¤ÇÒÁ¶Ù¡µŒÍ§ã¹»˜¨¨Øº¹ÁÕÁÒ¡¡Ç‹ÒÃŒÍÂÅÐ 99.5
è é Ñ
¡ÒèѴà¡çºáÅСÒô֧¢ŒÍÁÙÅä»ãªŒ
¢ŒÍÁÙÅ·ÕµÃǨÊͺ¤ÇÒÁ¶Ù¡µŒÍ§áŌǨж١¨Ñ´à¡çºã¹°Ò¹¢ŒÍÁÙÅ (relational database) ÊÒÁÒö
è
´Ö§¢ŒÍÁÙÅÍÍ¡ÁҷѧËÁ´ËÃ×ͺҧʋǹ µÒÁà§×͹䢷ռ㪌¡Ò˹´ä´ŒÍ‹ҧÊдǡÃÇ´àÃçÇ áÅÐÊÒÁÒöʋ§
é è è ÙŒ í
¢ŒÍÁÙÅãËŒ¼ãªŒä´Œã¹ÃٻẺ·ÕµÍ§¡Òà ઋ¹ã¹ÃٻẺä¿ÅµÇÍÑ¡Éà (text file) ä¿ÅÊÒËÃѺ Microsoft Excel
ÙŒ è Œ Ñ í
ä¿ÅÊíÒËÃѺ¡ÒÃÇÔà¤ÃÒÐË´ŒÇÂâ»Ãá¡ÃÁ·Ò§Ê¶ÔµÔ ઋ¹ SPSS áÅÐÊÌҧÃÒ§ҹµÒÁ·Õè¼ÙŒãªŒÍ͡Ẻ
¢ŒÍÁÙŷѧËÁ´¨ÐÁÕ¡Ò÷íÒÊíÒÃͧà¾×ͤÇÒÁ»ÅÍ´ÀÑ¢ͧ¢ŒÍÁÙÅ áÅСíÒ˹´ÊÔ·¸Ô¢Í§¼Ù㪌㹡ÒÃࢌҶ֧
é è Œ
¢ŒÍÁÙÅ
613.
586 Digital ImageProcessing and Data Management for Clinical Registry and Clinical Research
¢ŒÍ¨íÒ¡Ñ´¢Í§Ãкºã¹»˜¨¨ØºÑ¹
ã¹»˜¨¨Øº¹ Ãкº·íҧҹ䴌´ÁÒ¡¡Ñº¢ŒÍÁÙÅ checkbox áÅеÑÇàÅ¢ ᵋ¤ÇÒÁÊÒÁÒö㹡ÒÃÍ‹Ò¹
Ñ Õ
µÑÇÍÑ¡ÉÃÀÒÉÒÍѧ¡ÄÉÂѧ·íÒä´ŒäÁ‹´¹¡ ¨íÒ໚¹µŒÍ§ÊÐÊÁ¢ŒÍÁÙÅà¾ÔÁàµÔÁà¾×Í㪌㹡Òýƒ¡à¤Ã×Í¢‹ÒÂãÂ
Õ Ñ è è
»ÃÐÊÒ· ʋǹµÑÇÍÑ¡ÉÃÀÒÉÒä·ÂÂѧäÁ‹ÊÒÁÒö㪌§Ò¹ä´Œ â´Â·ÑÇ仢ŒÍ¨íÒ¡Ñ´àËÅ‹Ò¹ÕäÁ‹à»š¹»˜ËÒà·‹Ò
è é
㴹ѡ à¾ÃÒТŒÍÁÙÅʋǹãË‹¨ÐÍÂÙã¹ÃÙ» checkbox áÅеÑÇàÅ¢ÍÂÙáÅŒÇ Ê‹Ç¹¢ŒÍÁÙŵÑÇÍÑ¡ÉÃÁÑ¡¨ÐÊÒÁÒö
‹ ‹
á»Å§ãˌ໚¹µÑÇàŢ䴌 ¨Ö§ÁÕ¢ÍÁÙÅ·Õ໚¹µÑÇÍÑ¡ÉèÃÔ§ÍÂÙäÁ‹ÁÒ¡¹Ñ¡ã¹â¤Ã§¡Ò÷ÑÇä»
Œ è ‹ è
ʶҹ·ÕèµÔ´µ‹ÍÊíÒËÃѺ¼ÙŒ·Õèʹã¨ÃкºÊ᡹ÀÒ¾
˹‹ÇªÕÇÊÒÃʹà·ÈáÅШѴ¡ÒâŒÍÁÙÅÇԨ ʶҹʋ§àÊÃÔÁ¡ÒÃÇÔ¨Â
Ñ Ñ
µÖ¡Í´ØÅÂà´ªÇÔ¡ÃÁ ªÑ¹ 12 ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
é ÔÔ
â·Ã. 02-419- 6666-70 ËÃ×Í VPN 08-8227-5937
614.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 587
80
Research and Road to Innovation and Business
ÃͧÈÒʵÃÒ¨ÒàÇÃóРÁËÒ¡ÔµµÔ¤Ø³
ÀÒ¤ÇÔªÒ»ÃÊÔµÇÔ·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
ÔÔ
¾ÔÁ¾»ÃÐä¾ ¸ÕÃЪվ
ÈٹºÃÔËÒ÷ÃѾÂʹ·Ò§»˜Ò ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô
¸ÒÃÔ¹ àÍÕèÂÁྪÃÒ¾§È
ºÃÔɷËÇÁ·Ø¹ÊµÒ§¤ ¨íÒ¡Ñ´
Ñ
¼ÙŒª‹ÇÂÈÒʵÃÒ¨Òà´Í¡àµÍø¹¾Å ÇÕÃÒÊÒ
ÇÔ·ÂÒÅѨѴ¡Òà ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
¤ÇÒÁËÁÒ¢ͧ¡ÒÃÇÔ¨ÂÁÕ¤Ò¨íÒ¡Ñ´¤ÇÒÁä´ŒËÅÒ¤ÇÒÁËÁÒ ¡Å‹ÒÇâ´ÂÃÇÁ ¡ÒÃÇÔ¨ÂËÁÒ¶֧
Ñ í Ñ
¡Òõѧ¤íÒ¶ÒÁËÃ×Í¡Ãкǹ¡ÒäԴ áÅйíÒÁÒ´íÒà¹Ô¹¡ÒÃÍ‹ҧ໚¹Ãкºà¾×ÍËÒ¤íҵͺ (ͧ¤¤ÇÒÁÃÙŒ
é è
ãËÁ‹) ãËŒ¡º»˜ËÒ·Õà¡Ô´¢Ö¹·Ø¡ª¹Ô´·Ñ§·Ò§ÇÔ·ÂÒÈÒʵÃáÅÐÊѧ¤ÁÈÒʵà ¹Ñ¡ÇԨ¤×ͼٷ´Òà¹Ô¹¡ÒÃ
Ñ è é é Ñ Œ Õè í
¤Œ¹¤ÇŒÒËÒ¤ÇÒÁÃÙŒáÅФíҵͺ㹻ÃÐà´ç¹·ÕèʧÊÑ â´ÂÁÕÃÐàºÕºÇÔ¸ÕÍѹ໚¹·ÕèÂÍÁÃѺã¹áµ‹ÅÐÈÒʵÃ
·Õèà¡ÕèÂÇ¢ŒÍ§ «Ö觤Ãͺ¤ÅØÁ·Ñé§á¹Ç¤Ô´ Áâ¹·Ñȹ áÅÐÇÔ¸Õ¡Ò÷Õè㪌㹡ÒÃÃǺÃÇÁ áÅÐÇÔà¤ÃÒÐË¢ŒÍÁÙÅ
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å໚¹Ê¶ÒºÑ¹¡ÒÃÈÖ¡ÉҪѹ¹íҢͧ»ÃÐà·È ໚¹·Õ衵‹ÍÊÒ¸Òóª¹ã¹´ŒÒ¹¡ÒÃ໚¹
é è ÙŒ Ñ
ÁËÒÇÔ·ÂÒÅÑÂáË‹§¡ÒÃÇԨѠ«Öè§ÁÕ§Ò¹·ÕèÁÕÅѡɳÐÊÌҧÊÃä ´íÒà¹Ô¹¡ÒÃÍ‹ҧ໚¹Ãкºà¾×èÍà¾ÔèÁ¾Ù¹
¤Åѧ¤ÇÒÁÃÙŒ ·Ñ駤ÇÒÁÃÙŒ·Õèà¡ÕèÂǡѺÁ¹ØÉ ÇѲ¹¸ÃÃÁ áÅÐÊѧ¤Á áÅÐÁÕ¡ÒÃ㪌¤ÇÒÁÃÙŒàËÅ‹Ò¹Õé à¾×èÍ¡ÒÃ
»ÃдÔÉ°Š¤´¤Œ¹ÊÔ§ãËÁ‹æ ·ÕÁ»ÃÐ⪹ â´Â䴌ʹѺʹعãËŒ¹¡ÇÔ¨ÂÊÌҧ¼Å§Ò¹¤Ø³ÀÒ¾ ÊÒÁÒö¹íÒ§Ò¹
Ô è è Õ Ñ Ñ
ÇÔ¨Â仵‹ÍÂÍ´µÒÁ¤ÇÒÁµŒÍ§¡ÒâͧªØÁª¹ Êѧ¤ÁáÅлÃÐà·È «Ö§¡ÒÃÇԨ»ÃÐÂØ¡µ (applied research)
Ñ è Ñ
¹Ñºà»š¹¡ÒÃÇÔ¨ÑÂÍÕ¡´ŒÒ¹Ë¹Öè§ ·ÕèÁØ‹§¹íҼšÒÃÇÔ¨ÑÂä»ãªŒ»ÃÐ⪹ ÍÒ·Ôઋ¹ ¡ÒùíҼŧҹä»ãªŒ
ã¹àªÔ§¾Ò³ÔªÂáÅÐÀÒ¤ÍصÊÒË¡ÃÃÁ 㹡ÒùÕÁ¡ÁÕàÃ×ͧà¡ÕÂǡѺ§Ò¹·ÃѾÂʹ·Ò§»˜ÒÁÒà¡ÕÂÇ¢ŒÍ§
é Ñ è è Ô è
µÑ Ç Í‹ Ò §¼Å§Ò¹ÇÔ ¨Ñ  àªÔ § »ÃÐÂØ ¡ µ ã ¹ÀÒ¤ÇÔ ª Ò»ÃÊÔ µ ÇÔ · ÂÒ ¤³Ðá¾·ÂÈÒʵà ÈÔ ÃÔ Ã Òª¾ÂÒºÒÅ
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å ·ÕÊÒÁÒö¹íÒ§Ò¹¹Çѵ¡ÃÃÁ·Õä´ŒÁÒ¡‹Í»ÃÐ⪹àªÔ§¾Ò³ÔªÂ 䴌ᡋ ÍØ»¡Ã³¡¡½Ø¹
è è Ñ †
à¤Ã×ͧᡵÑÇäýع à¤Ã×ͧãËŒàÅ×Í´ÂاÍѵâ¹ÁÑµÔ à»š¹µŒ¹
è † è
615.
588 Research and Road to Innovation and Business
ÃÙ»·Õè 1. ÍØ»¡Ã³¡¡½Ø¹
Ñ † ÃÙ»·Õè 2. à¤Ã×ͧᡵÑÇäýع
è † ÃÙ»·Õè 3. à¤Ã×ͧãËŒàÅ×Í´ÂاÍѵâ¹ÁѵÔ
è
(Siriraj dust trap) (Mite Isolator)
ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Åä´Œ´íÒà¹Ô¹¡ÒÃÊ‹§àÊÃÔÁãËŒà¡Ô´¼Å§Ò¹ÇÔ¨ÑÂãˌ䴌ͧ¤¤ÇÒÁÃÙŒãËÁ‹ÍÂÙ‹Í‹ҧ
µ‹Íà¹×ͧ áÅÐÁռŧҹÇÔ¨Âã¹ÅѡɳÐͧ¤¤ÇÒÁÃٷ䴌ú¡ÒÃà¼Âá¾Ã‹ã¹ÇÒÃÊÒùҹҪҵÔ໚¹¨íҹǹ
è Ñ Œ Õè Ñ
ÁÒ¡Í‹ҧÊÁèÒàÊÁÍ ã¹»˜¨¨Øº¹¼Å§Ò¹ÇԨ¢ͧÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å໚¹·ÕÂÍÁÃѺáÅлÃШѡɵÍÊѧ¤Á
í Ñ Ñ è ‹
·Ñ§ã¹»ÃÐà·Èä·Âàͧ áÅÐã¹ÃдѺ¹Ò¹ÒªÒµÔ 㹨íҹǹ¼Å§Ò¹ÇԨ·Õ໚¹Í§¤¤ÇÒÁÃÙ¹Á¨Ò¹Ç¹Ë¹Ö§
é Ñ è Œ Õé Õ í è
·ÕèÊÒÁÒö¹íÒä»»ÃÐÂØ¡µáÅС‹ÍãËŒà¡Ô´à·¤â¹âÅÂÕãËÁ‹æ µÅÍ´¨¹à¡Ô´¤ÇÒÁ¾ÃŒÍÁ·Õè¨Ð¶‹Ò·ʹ
à·¤â¹âÅÂÕãˌᡋÀÒ¤àÍ¡ª¹à¾×èÍ¡‹ÍãËŒà¡Ô´»ÃÐ⪹µ‹ÍÊѧ¤Áâ´ÂÃÇÁáÅлÃÐ⪹ã¹àªÔ§¾Ò³ÔªÂ
ÁËÒÇÔ·ÂÒÅÑÂÁËԴŨ֧䴌¨´µÑ§ÈٹºÃÔËÒ÷ÃѾÂʹ·Ò§»˜Ò ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å «Ö§à»š¹Ë¹‹Ç§ҹ
Ñ é Ô è
·Õú¼Ô´ªÍºã¹¡ÒùíҼŧҹÇÔ¨Âà¾×Í»ÃÐÂØ¡µãªŒã¹àªÔ§¾Ò³ÔªÂÍ‹ҧÁÕ»ÃÐÊÔ·¸ÔÀÒ¾
èÑ Ñ è
¡ÒôíÒà¹Ô¹§Ò¹¢Í§ÈٹºÃÔËÒ÷ÃѾÂÊÔ¹·Ò§»˜Ò
ẋ§ä´Œà»š¹ 4 ʋǹ 䴌ᡋ ¡ÒÃÊÌҧ·ÃѾÂʹ·Ò§»˜Ò (creation) ¡ÒäØÁ¤Ãͧ·ÃѾÂʹ
Ô Œ Ô
·Ò§»˜Ò (protection) ¡ÒùíÒ·ÃѾÂʹ·Ò§»˜Òä»ãªŒ»ÃÐ⪹ (exploitation) áÅСÒû¡»‡Í§
Ô
ÊÔ·¸Ôã¹·ÃѾÂʹ·Ò§»˜Ò (enforcement) «Ö§áµ‹ÅÐʋǹ¨ÐÁÕº·ºÒ·áÅÐ˹ŒÒ·ÕáÅСÒôíÒà¹Ô¹§Ò¹
Ô è è
´Ñ§¹Õé
¡ÒÃÊÌҧ·ÃѾÂʹ·Ò§»˜Ò
Ô
à¾×ÍʹѺʹعáÅÐÊ‹§àÊÃÔÁãËŒà¡Ô´¡ÒÃÊÌҧ·ÃѾÂʹ·Ò§»˜Ò ¨Ö§ÁÕ¡ÒôíÒà¹Ô¹¡ÒÃ㹡ÒÃÊÌҧ
è Ô
¤ÇÒÁࢌÒã¨ã¹àÃ×ͧ·ÃѾÂʹ·Ò§»˜Òãˌᡋ¼»¯Ôºµ§Ò¹ã¹ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å ÃÇÁ¶Ö§ãËŒàÅç§àË繶֧
è Ô ÙŒ Ñ Ô
»ÃÐ⪹¨Ò¡¡ÒÃ㪌·ÃѾÂÊÔ¹·Ò§»˜Òà¾×è;Ѳ¹ÒÊѧ¤Á »ÃÐà·ÈªÒµÔ â´Â¡ÒûÃЪÒÊÑÁ¾Ñ¹¸
¨Ñ´ÍºÃÁÊÑÁÁ¹Ò ãËŒ¤ÇÒÁÃÙàÃ×ͧ·ÃѾÂʹ·Ò§»˜Ò ã¹´ŒÒ¹µ‹Ò§æ ÃÇÁ¶Ö§¡ÒÃÊ׺¤Œ¹¢ŒÍÁÙÅ·ÃѾÂʹ
Œ è Ô Ô
·Ò§»˜Ò ઋ¹ ÊÔ·¸ÔºÑµÃá¡‹¼ÙŒ»¯ÔºÑµÔ§Ò¹áÅйѡÈÖ¡ÉÒ áÅÐãËŒºÃÔ¡ÒÃᡋ˹‹Ç§ҹÀÒ¹͡
¾ÃŒÍÁ·Ñ§¨Ñ´ãËŒÁ¼»ÃÐÊÒ¹§Ò¹´ŒÒ¹·ÃѾÂʹ·Ò§»˜Òà¾×Í»ÃÐÊÒ¹§Ò¹áÅÐàª×ÍÁâ§໚¹à¤Ã×Í¢‹ÒÂ
é Õ ÙŒ Ô è è
㹡Ò÷íҧҹËÇÁ¡Ñ¹ áÅÐʹѺʹع áÅмÅÑ¡´Ñ¹ãËŒà¡Ô´¡ÒÃËÇÁÁ×͡ѺÀÒ¤ÍصÊÒË¡ÃÃÁ㹡ÒÃÊÌҧ
¼Å§Ò¹·ÃѾÂʹ·Ò§»˜Ò à¾×ÍãËŒà¡Ô´¡ÒùíÒä»ãªŒ»ÃÐ⪹䴌¨ÃԧᡋÀÒ¤ÍصÊÒË¡ÃÃÁ áÅзíÒ¡ÒÃ
Ô è
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 597
82
¤ÇÒÁ¼Ô´»¡µÔ¢Í§ÊÒÂàÊÕ§
(Vocal folds mucosal disorders)
ÍÒ¨Òà¹ÒÂá¾·Â侺ÙÅ ÊØÃÕ¾§É
ÀÒ¤ÇÔªÒ âʵ ¹ÒÊÔ¡ ÅÒÃÔ§«Ç·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ÔÔ
Vocal nodule
à¡Ô´ºÃÔàdzÃ͵‹ÍÃÐËÇ‹Ò§´ŒÒ¹Ë¹ŒÒ 1/3 µ‹Í¡Ñº´ŒÒ¹ËÅѧ 2/3 ¢Í§ÊÒÂàÊÕ§ ÁÑ¡à¡Ô´·Ñ§Êͧ¢ŒÒ§
é
à¡Ô´¨Ò¡¡ÒúÇÁ¹éÒºÃÔàdz submucosa ÁÑ¡à¡Ô´ã¹¤¹·Õ㪌àÊÕ§ÁÒ¡ 㪌àÊÕ§¼Ô´ÇԸ໚¹àÇÅÒ¹Ò¹ 㹪‹Ç§
í è Õ
áᶌҾѡ¡ÒÃ㪌àÊÕ§ àÊÕ§¨Ð¤‹ÍÂæ´Õ¢¹ä´Œ ᵋ¶ÒÂѧ¤§ãªŒàÊÕ§¼Ô´ÇÔ¸µÍ仨ÐÁÕ¾§¼×´à¢ŒÒÁÒá·¹·Õè ·íÒãËŒ
Öé Œ Õ ‹ Ñ
àÊÕ§´Õ¢¹ªŒÒŧ ¨ÐÁÕÍÒ¡ÒÃàÊÕ§á˺ÁÒ¡ËÃ×͹ŒÍÂä´Œã¹ÃÐËÇ‹Ò§Çѹᵋ㹪‹Ç§ÊÒÂæÁÑ¡¨Ð໚¹ÁÒ¡¡Ç‹Ò
Öé
ª‹Ç§àªŒÒ à¹×ͧ¨Ò¡¼Ù»ÇÂä´Œ¾¡àÊÕ§㹵͹¡ÅÒ§¤×¹áÅÐàÃÔÁ㪌àÊÕ§ËÅѧ¨Ò¡µ×¹¹Í¹ ¡ÒÃÃÑ¡ÉÒâ´Â
è Œ † Ñ è è
¡Òþѡ¡ÒÃ㪌àÊÕ§áÅСÒýƒ¡¾Ù´ã¹¡Ã³Õ·¼»ÇÂÁÕ¡Òþٴ·Õ¼´ÇÔ¸Õ ¹Í¡¨Ò¡¹Ñ¹¤ÇõŒÍ§ãËŒÊÒÂàÊÕ§
Õè ÙŒ † è Ô é
ÁÕ¤ÇÒÁªØÁª×¹â´Â¡Òô×Á¹éÒÁÒ¡æ áÅФÇÃËÅÕ¡àÅÕ§ÍÒËÒ÷շÒãËŒ¤ÍáËŒ§àª‹¹ ÍÒËÒ÷ʹ ¡Òá¿
‹ é è í è è í
໚¹µŒ¹ ¡ÒÃ㪌ÂÒÍÒ¨¨Ð㪌à¾×ÍÅ´¡ÒúÇÁ໚¹¾Ç¡ steroid ·Ò¹ã¹ª‹Ç§ÊÑ¹æ ¡Òü‹ÒµÑ´¨Ð·íÒ㹡óÕ
è é
·Õè vocal nodule ·ÕÁ¾§¼×´à¢ŒÒÁÒá·¹·ÕáÅŒÇ áÅÐ䴌ú¡ÒÃÃÑ¡ÉÒâ´Â¡ÒÃ㪌ÂÒáÅСÒû¯ÔºµµÇÍ‹ҧ
è Õ Ñ è Ñ Ñ Ô Ñ
¹ŒÍ 3 à´×͹áÅŒÇÍÒ¡ÒÃäÁ‹´¢¹à·‹Ò¹Ñ¹Õ Öé é
625.
598 ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ÊÒÂàÊÕ§
Vocal fold hemorrhage áÅÐ Vocal fold (hemorrhagic) polyp
à¡Ô´¨Ò¡¡ÒõÐ⡹áçæáŌǷíÒãËŒàÊŒ¹àÅ×Í´·ÕÊÒÂàÊÕ§ᵡà¡Ô´ÁÕàÅ×Í´ÍÍ¡ÍÂÙ㹪ѹ¼ÔǢͧ
è ‹ é
ÊÒÂàÊÕ§ ËÃ×Íà¡Ô´ã¹¼Ù»Ç·աÒÅѧ䴌úÂÒÅÐÅÒÂÅÔÁàÅ×Í´«Ö§â´Â·ÑÇä»ÁÑ¡¨ÐËÒÂä»ä´ŒÀÒÂã¹ 2 ÊÑ»´ÒË
Œ † è í Ñ è è è
ᵋÍ‹ҧäáçµÒÁÍÒ¨¨Ðà¡Ô´¡Òç͡¢Öé¹ÁҢͧʌ¹àÅ×Í´·ÕèÍÂÙ‹¢ŒÒ§ãµŒ·íÒãËŒà¡Ô´à»š¹µÔè§à¹×é͹ٹ¢Öé¹ÁÒä´Œ
àÃÕ¡ hemorrhagic polyp â´ÂÁÑ¡¨Ðà¡Ô´·ÕÊÒÂàÊÕ§¢ŒÒ§à´ÕÂÇ෋ҹѹ ¡ÒÃÃÑ¡ÉÒãËŒËÂØ´ÂÒÅÐÅÒÂÅÔÁàÅ×Í´
è é è
ã¹ÃÒ·աÒÅѧ䴌úÂÒÍÂÙ‹ áÅÐà¹×ͧ¨Ò¡¡Ã´·ÕäËÅŒ͹¢Ö¹ÁÒ¨Ò¡¡ÃÐà¾ÒТֹÁҷաŋͧàÊÕ§¨Ð·íÒãËŒ
è í Ñ è è é é è
àÊŒ¹àÅ×Í´¢ÂÒµÑÇÁÒ¡¢Ö鹴ѧ¹Ñ鹨֧¤ÇäǺ¤ØÁ¡Ã´äËÅŒ͹´ŒÇ áÅФÇÃá¹Ð¹íÒ¼ÙŒ»†ÇÂãˌ㪌àÊÕ§
Í‹ҧ¶Ù¡ÇÔ¸Õâ´ÂËÅÕ¡àÅÕ§¡ÒõÐ⡹àÊÕ§´Ñ§ÁÒ¡æ áÅÐá¹Ð¹íÒÇÔ¸Õ´ÙáÅàÊŒ¹àÊÕ§â´ÂãËŒ´×èÁ¹éíÒÁÒ¡æ
äÁ‹¾Ù´à¤Œ¹àÊÕ§ ËÅÕ¡àÅÕè§ÍÒËÒ÷Õè·íÒãËŒÊÒÂàÊÕ§áËŒ§àª‹¹¡Òá¿áÅТͧ·Í´ ã¹ÃÒ·Õè polyp
ÁÕ¢¹Ò´àÅç¡ÍÒ¨¨ÐËÒÂä»àͧ䴌ã¹àÇÅÒ໚¹à´×͹æ ᵋâ´Â·ÑÇä»ÁÑ¡¨ÐµŒÍ§¼‹ÒµÑ´ÍÍ¡ â´Â·Õ¾ÂÒÂÒÁ
è è
à¡çº mucosa ·Õ´äÇŒãËŒÁÒ¡·ÕÊ´ à¾×ͷըзíÒãËŒ¡ÒÃà¤Å×͹äËǢͧ¼ÔǢͧÊÒÂàÊÕ§¨Ð¡ÅѺÁÒã¡ÅŒà¤Õ§
è Õ èØ è è è
»¡µÔÁÒ¡·ÕÊ´ èØ
Intracordal cyst (¶Ø§¹éíÒ·ÕèÊÒÂàÊÕ§)
626.
àǪÈÒʵ÷¹Âؤ 2553
Ñ 599
à¡Ô´¡ÒÃÍØ´µÑ¹¢Í§µ‹ÍÁ·ÕèÍÂÙ‹ºÃÔàdzªÑé¹¼ÔǢͧÊÒÂàÊÕ§ â´ÂÊÒà˵ØÍÒ¨à¡Ô´¨Ò¡¡ÒõÐ⡹
㪌àÊÕ§ÁÒ¡áŌǷíÒãËŒà¡Ô´¾Ñ§¼×´·ÕÃà»´¢Í§µ‹ÍÁ·ÕÊÌҧàÁ×Í¡ (mucous) ºÃÔàdzÊÒÂàÊÕ§·íÒãËŒà¡Ô´¡ÒÃ
èÙ è
ÍØ´µÑ¹¢Í§µ‹ÍÁáÅŒÇà¡Ô´à»š¹¶Ø§¹éÒµÒÁÁÒ ã¹ºÒ§ÃÒ¶ا¹éÒÍҨᵡàͧ䴌 ᵋºÒ§ÃÒ¡礧ÍÂÙÍ‹ҧ¹Ñ¹
í í ‹ é
·íÒãËŒà¡Ô´ÍÒ¡ÒÃàÊÕ§á˺µÅÍ´àÇÅÒ ¡ÒÃÃÑ¡ÉÒâ´Â¡Òü‹ÒµÑ´àÍҶا¹éÒÍÍ¡(excision) ËÃ×Íà»´·Ò§
í
ãËŒ¹Ò㹶ا¹éÒÊÒÁÒöÃкÒÂÍÍ¡ÁÒä´Œ (marsupialization)
éí í
Bilateral diffuse polyposis (Reinke’s edema or smoker’s polyposis)
ÁÕ¡ÒúÇÁ㹪ѹ㵌àÂ×ÍºØ¼Ç (Reinke’s space) ·ÑÇæä»·ÕÊÒÂàÊÕ§·Ñ§ 2 ¢ŒÒ§ ÁÑ¡¨Ðà¡Ô´¨Ò¡
é è Ô è è é
¡ÒÃÃФÒÂà¤×ͧ¨Ò¡¤ÇѹºØËÃÕÃÇÁ¡ÑºÁÕ¡ÒÃ㪌àÊÕ§ÁÒ¡ ¼Ù»Ç¨оٴÁÕàÊÕ§µèÒ¡Ç‹Ò»¡µÔ (lower pitch)
è‹ Œ † í
áÅÐäÁ‹ÊÒÁÒö¢Öé¹àÊÕ§Ê٧䴌àËÁ×͹à´ÔÁ µÃǨ´Ù¨Ð¾ºÊÒÂàÊÕ§ºÇÁ¹éíÒµÅÍ´á¹Ç¢Í§ÊÒÂàÊÕ§
ÍÒ¨µŒÍ§à¨ÒдÙÃдѺÎÍÃâÁ¹ä·ÃÍ´´ŒÇÂ㹡óշÕèʧÊÑÂÃдѺÎÍÃâÁ¹µèíÒà¹×èͧ¨Ò¡·íÒãËŒÊÒÂàÊÕ§
ºÇÁ䴌ઋ¹¡Ñ¹ ¡ÒÃÃÑ¡ÉÒâ´Â¡ÒÃãËŒ¼»ÇÂËÂØ´ÊÙºººØËÃÕáÅоѡ¡ÒÃ㪌àÊÕ§ ã¹ÃÒ·ÕÍÒ¡ÒÃäÁ‹´¢¹
ÙŒ † è è Õ Öé
ÍÒ¨·íÒ¡Òü‹ÒµÑ´â´Â¡ÒÃÅÍ¡àÍÒʋǹ¼ÔÇ·ÕºÇÁÍÍ¡ºÒ§Ê‹Ç¹à¾×Í·íÒãËŒàÊÕ§´Õ¢¹
è è Öé
Contact ulcer ËÃ×Í Granuloma
627.
600 ¤ÇÒÁ¼Ô´»¡µÔ¢Í§ÊÒÂàÊÕ§
ÁÑ¡¨Ðà¡Ô´¨Ò¡¡¡Ò÷աô¨Ò¡¡ÃÐà¾ÒÐÍÒËÒÃäËÅŒ͹¢Ö¹ÁÒ·Õ¤ÍáÅСŋͧàÊÕ§·Ò§´ŒÒ¹ËÅѧ
è é è
·íÒãËŒà¡Ô´à»š¹á¼Å¢Ö¹ÁÒºÃÔàdz¡Å‹Í§àÊÕ§¤‹Í¹ÁÒ·Ò§´ŒÒ¹ËÅѧ ( vocal process of arythenoid )
é
â´Â·ÕËÅѧ¨Ò¡¡ÒÃËÒ¢ͧá¼ÅáÅŒÇÍÒ¨à¡Ô´à»š¹ granuloma ¢Ö¹ÁÒ ã¹ºÒ§ÃÒÂÍÒ¨ÁÕ»ÃÐÇѵà¤ÂãÊ‹·Í
è é Ô ‹
ª‹ÇÂËÒÂã¨ÁÒ¡‹Í¹·íÒãËŒà¡Ô´ÁÕá¼Å¨Ò¡¡ÒᴷѺ (pressure necrosis)ºÃÔàdz vocsal process ä´Œ·Ò í
ãËŒà¡Ô´ granuloma µÒÁÁÒ ÃÑ¡ÉÒâ´Â¡ÒÃãËŒÂÒÃÑ¡ÉҡôäËÅŒ͹áÅлÃѺ¾ÄµÔ¡ÃÃÁ¡Ò÷ҹÍÒËÒÃ
áÅСÒù͹ ¡ÒÃ㪌 steroid ÊÒÁÒö·íÒãËŒ granuloma Âغŧ䴌㹺ҧÃÒ ¡Òü‹ÒµÑ´àÍÒ granuloma
Í͡令ÇäԴ¶Ö§à»š¹à»š¹Íѹ´Ñº·ŒÒÂæáÅФÇ÷íÒ㹡óշ¢ÇàÅç¡æ à¹×ͧ¨Ò¡ËÅѧ¡Òü‹ÒµÑ´¨Ðà¡Ô´
Õè Ñé è
á¼Å¢Ö¹ÁÒÍÕ¡·íÒãËŒà¡Ô´ granuloma ¢Ö¹ÁÒãËÁ‹ä´ŒÍ¡
é é Õ
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Bastian RW: Benign Vocal .old Mucosal Disorders, Cummings Otolaryngology Head & Neck Surgery 4th
edition: 2150-2184.
2. Kleinsasser O: Pathogenesis of vocal cord polyps, Ann Otol Rhinol Laryngol 1982; 91:378.
628.
àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 601
83
Hearing Loss in Children: 120 year Evolution in Management
¼ÙŒª‹ÇÂÈÒʵÃÒ¨ÒàᾷÂËÔ§ÊØÇѨ¹Ò ͸ÔÀÒÊ
ÀÒ¤ÇÔªÒâʵ ¹ÒÊÔ¡ ÅÒÃÔ§«Ç·ÂÒ ¤³Ðá¾·ÂÈÒʵÃÈÃÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å
Ô ÔÔ
¡ÒõÃǨ¡ÒÃä´ŒÂÔ¹ã¹à´ç¡
¡ÒõÃǨ¡ÒÃ䴌¹¨Ð·íÒãËŒ·ÃÒºÃдѺ¢Í§¡ÒÃ䴌¹º¡¾Ã‹Í§µÅÍ´¨¹ª¹Ô´¢Í§¤ÇÒÁ¼Ô´»¡µÔ
Ô Ô
ઋ¹ ¡ÒùíÒàÊÕ§º¡¾Ã‹Í§ (conductive hearing loss) ËÃ×Í»ÃÐÊÒ·ÃѺàÊÕ§º¡¾Ã‹Í§ (sensori-neural
hearing loss) à¾×ͨÐ䴌áÉÒËÃ×Í¿„¹¿ÙÊÁÃöÀҾ䴌Í‹ҧàËÁÒÐÊÁ ¡ÒõÃǨ¡ÒÃ䴌¹ã¹à´ç¡
è Ñ œ Ô
¨ÐÁÕǸµÃǨᵡµ‹Ò§¨Ò¡¡ÒõÃǨ㹼ÙãË‹à¹×ͧ¨Ò¡ÇÔ¸µÃǨ·Õ㪌µÒÁ»¡µÔã¹¼ÙãË‹ ઋ¹ Pure tone
ÔÕ Œ è Õ è Œ
audiometry ÍҨ䴌¼ÅäÁ‹á¹‹¹Í¹¶ŒÒà´ç¡äÁ‹à¢ŒÒã¨ÇÔ¸¡ÒõÃǨËÃ×ÍäÁ‹ÃÇÁÁ×Í áÅÐäÁ‹ÊÒÁÒö㪌µÃǨ
Õ ‹
à´ç¡àÅç¡ä´Œ
â´Â·ÑÇä»áŌǡÒõÃǨ¡ÒÃ䴌¹ã¹à´ç¡áº‹§Í͡䴌໚¹ 2 »ÃÐàÀ· ¤×Í
è Ô
1. ¡ÒõÃǨẺÊѧࡵ¾ÄµÔ¡ÃÃÁ¡Òõͺʹͧµ‹ÍàÊÕ§ (Behavioral hearing test)
2. ¡ÒõÃǨâ´ÂÇÑ´¼Å¡Òõͺʹͧ·Ò§ÊÃÕÃÇÔ·ÂÒä¿¿‡Ò (Electrophysiologic test)
¡ÒõÃǨẺÊѧࡵ¾ÄµÔ¡ÃÃÁ¡Òõͺʹͧµ‹ÍàÊÕ§(1,2)
ÁÕËÅÒÂÇÔ¸«§àËÁÒÐÊÁµÒÁᵋÅЪ‹Ç§ÍÒÂØ à¹×ͧ¨Ò¡à´ç¡áµ‹ÅÐÇѨÐÁվĵԡÃÃÁáÅФÇÒÁäÇ
Õ Öè è
㹡ÒáÒõͺʹͧµ‹ÍàÊÕ§ᵡµ‹Ò§¡Ñ¹ 䴌ᡋ
- Behavioral observation audiometry àËÁÒСѺà´ç¡ááà¡Ô´¶Ö§ 2 ¢Çº ໚¹¡ÒÃÊѧࡵ
¾ÄµÔ¡ÃÃÁ¡Òõͺʹͧµ‹ÍàÊÕ§ ઋ¹ ¡ÒáÃоÃÔºµÒ Êдا ËÃ×ÍËѹµÒÁàÊÕ§
Œ
- Visual reinforcement audiometry àËÁÒСѺà´ç¡µÑ§áµ‹ÍÒÂØ 6 à´×͹¢Ö¹ä»¶Ö§ 3 ¢Çº
é é
ÇÔ¸¡ÒõÃǨ¨Ð¡Ãеع¤ÇÒÁʹ㨢ͧà´ç¡ä´ŒÁÒ¡¡Ç‹Ò Behavioral observation audiometry ¨Ö§àË繡ÒÃ
Õ Œ
µÍºÊ¹Í§µ‹ÍàÊÕ§䴌ª´à¨¹¢Ö¹ â´Âà´ç¡¨ÐÃѺÃÙÇÒ¶ŒÒÁÕàÊÕ§´Ñ§áŌǨÐÁÕÀÒ¾ËÃ×ͧ͢àÅ‹¹·Õà¤Å×͹äËÇ
Ñ é Œ‹ è è
ä´ŒµÒÁÁÒãËŒàËç¹
- Speech reception threshold àËÁÒСѺà´ç¡µÑ§áµ‹ÍÒÂØ 2 ¶Ö§ 4 ¢Çº µÃǨâ´ÂãËŒà´ç¡¾Ù´
é
µÒÁËÃ×Í·íÒµÒÁ¤íÒÊѧ§‹ÒÂæ â´Â㪌ÃдѺàÊÕ§µ‹Ò§æ
è
- Conditioned play audiometry àËÁÒСѺà´ç¡µÑ§áµ‹ÍÒÂØ 3 ¢Çº¢Ö¹ä» â´ÂªÇ¹à´ç¡àÅ‹¹ ઋ¹
é é
àÁ×Í䴌¹àÊÕ§¡çãËŒËÂÍ´ÅÙ¡á¡ŒÇŧ¡Å‹Í§ ໚¹µŒ¹
è Ô




















































































































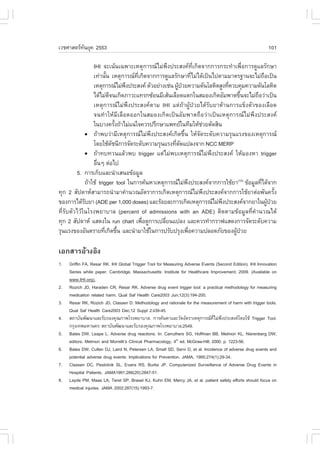








![110 PET/CT for Cancer in Head and Neck Region : Thyroid and Nonthyroid Carcinoma
àÍ¡ÊÒÃ͌ҧÍÔ§
1. Wahl RL. Targeting glucose transporters for tumor imaging: “sweet” idea, “sour ” result. J Nucl Med 1996;
37:1038-41.
2. Kostakoglu L, Agress H Jr, Goldsmith SJ. Clinical role of .DG PET in evaluation of cancer patients. Radiographics
2003;23(2):315-40.
3. Warburg O, Posener K, Negelein E. On the metabolism of cancer cells. Biochem Z 1924;152:319-44.
4. Wong RJ, Lin DT, Sch?der H, Patel SG, Gonen M, Wolden S, et al. Diagnostic and prognostic value of
[(18).]fluorodeoxyglucose positron emission tomography for recurrent head and neck squamous cell carcinoma.
J Clin Oncol 2002;20(20):4199-208.
5. Sch?der H, Yeung HW. Positron emission imaging of head and neck cancer, including thyroid carcinoma.
Semin Nucl Med 2004;34(3):180-97.
6. Sch?der H, Yeung HW, Gonen M, Kraus D, Larson SM. Head and neck cancer: clinical usefulness and
accuracy of PET/CT image fusion. Radiology 2004;231(1):65-72.
7. Blide A, Von Buchwald C, Mortensen J, Marving J, Therkidsen MH, Kirkegaard J, et al. The role of SPECT-
CT in the lymphoscintigraphic identification of sentinel nodes in patients with oral cancer. Acta Otolaryngol
2006;1269(10):1096-103.
8. Haerla SK, Strobel K, Hany T., Sidler D, Stoeckli SJ. (18).-.DG-PET/CT versus panendoscopy for the detection
of synchronous second primary tumors in patients with head and neck squamous cell carcinoma. Head Neck.
2010;32(3):319-25.
9. Yamamoto Y, Wong TZ, Turkington TG, Hawk TC, Coleman RE. Head and neck cancer: dedicated .DG
PET/CT protocol for detection-phantom and initial clinical studies. Radiology 2007;244(1):263-72.
10. Yen R., Hung RL, Pan MH, Wang YH, Huang KM, Lui LT, et al. 18-fluoro-2-deoxy-glucose positron emission
tomography in detecting residual/recurrent nasopharyngeal carcinomas and comparison with magnetic resonance
imaging. Cancer 2003;98(2):283-7.
11. Kao CH, Shiau YC, Shen YY, Yen R.. Detection of recurrent or persistent nasopharyngeal carcinomas after
radiotherapy with technetium-99m methoxyisobutylisonitrile single photon emission computed tomography and
computed tomography: comparison with 18-fluoro-2-deoxyglucose positron emission tomography. Cancer
2002;94(7):1981-6.
12. Kao CH, Tsai Sc, Wang JJ, Ho YJ, Yen R., Ho ST. Comparing 18-fluoro-2-deoxyglucose positron emission
tomography with a combination of technetium 99m tetrofosmin single photon emission computed tomography
and computed tomography to detect recurrent or persistent nasopharyngeal carcinomas after radiotherapy.
Cancer 2001;92(2):434-9.
13. Isles MG, McConkey C, Mehanna HM. A systematic review and meta-analysis of the role of positron emission
tomography in the follow up of head and neck squamous cell carcinoma following radiotherapy or
chemoradiotherapy. Clin Otolaryngol 2008;33(3):210-22.
14. Chen AY, Vilaseca I, Hudgins PA, Schuster D, Halkar R. PET-CT VS contrast-enhanced CT: what is the role
for each after chemoradiation for advanced oropharyngeal cancer? Head Neck 2006;28 (6):487-95.
15. Andrade RS, Heron DE, Degirmenci B, .ilho PA, Branstetter B., Seethala RR, et al. Posttreatment assessment
of response using .DG-PET/CT for patients treated with definitive radiation therapy for head and neck cancers.
Int J Radiat Oncol Biol Phys 2006;65(5):1315-22.](https://image.slidesharecdn.com/all-101224135812-phpapp02/85/53-137-320.jpg)

![112 PET/CT for Cancer in Head and Neck Region : Thyroid and Nonthyroid Carcinoma
32. Singer PA, Cooper DS, Daniels GH, Ladenson PW, Greenspan .S, Levy EG, et al. Treatment guidelines for
patients with thyroid nodules and well-differentiated thyroid cancer. American Thyroid Association. Arch Intern
Med 1996;156(19):2165-72.
33. Wang W, Macapinlac H, Larson SM, Yeh SD, Akhurst T, .inn RD, et al. [18.]-2-fluoro-2-deoxy-D-glucose positron
emission tomography localized residual thyroid cancer in patients with negative 131I whole body scans and
elevated serum thyroglobulin levels. J Clin Endocrinol Metab 1999;84:2291-302.
34. Grunwald ., Schomburg A, Bender H, Klemm E, Menzel C, Bultmann T, et al. .luorine-18 fluorodeoxyglucose
positron emission tomography in the follow-up of differentiated thyroid cancer. Eur J Nucl Med 1996;23:312-9.
35. Chung JK, So Y, Lee JS, Choi CW, Lim SM, Lee DS, et al. Value of .DG PET in papillary thyroid carcinoma
with negative I-131 whole-body scan. J Nucl Med 1999;40(6):986-92.
36. Lind P, Kresnik E, Kumnig G, Gallowitsch HJ, Igerc I, Matschnig S, et al. 18.-.DG-PET in the follow-up of thyroid
cancer. Acta Med Austrica 2003;30(1):17-21.
37. Wang W, Larson SM, .azzari M, Tickoo SK, Kolbert K, Sgouros G, et al. Prognostic value of (18.)
fluorodeoxyglucose positron emission tomographic scanning in patients with thyroid cancer. J Clin Endocrinol
Metab 2000;85(3):1107-13.
38. Phan HT, Jager PL, Plukker JT, Wolffenbuttel BH, Dierckx RA, Links TP. Detection of bone metastases in
thyroid cancer patients: bone scintigraphy or 18.-.DG PET? Nucl Med Commun 2007;28(8):597-602.
39. Ito S, Kato K, Ikeda M, Iwano S, Makino N, Tadokoro M, et al. Comparison of 18.-.DG PET and bone
scintigraphy in detection of bone metastases of thyroid cancer. J Nucl Med 2007;48(6):889-95.
40. Bombardieri E, Buscombe J, Lucignani G, Schober O, editors. Advances in Nuclear Oncology: Diagnosis and
Therapy.1st ed. United kingdom: Informa UK Ltd; 2007.
41. Lin EC, Alavi A, editors. PET and PET/CT: A clinical guide.2nd ed. New York: Thieme Medical Publishers, Inc.;
2009.](https://image.slidesharecdn.com/all-101224135812-phpapp02/85/53-139-320.jpg)







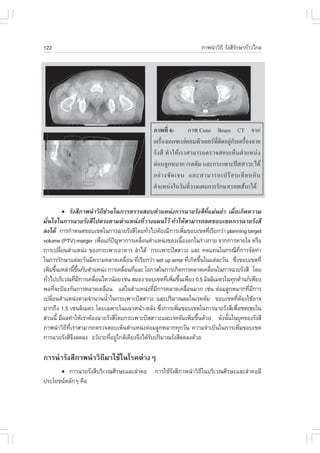







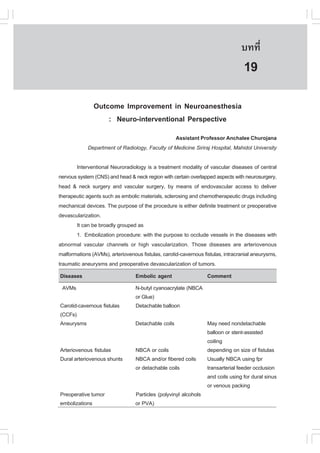






























![àǪÈÒʵ÷¹Âؤ 2553
Ñ 169
18. Gupta V, Posner B. Trauma to the long thoracic nerve and associated scapula winging in a low-velocity rear-
end automobile collision: case report. J Trauma 2004;57(2):402–3.
19. Omar N, Alvi ., Srinivasan MS. An unusual presentation of whiplash injury: long thoracic and spinal accessory
nerve injury. Eur Spine J 2007;16 (Suppl 3):S275–S277.
20. Ronnen HR, de Korte PJ, Brink PR, van der Bijl HJ, Tonino AJ, .ranke CL. Acute whiplash injury: is there a
role for MR imaging?—a prospective study of 100 patients. Radiology 1996;201(1):93–6.
21. Pettersson K, Hildingsson C, Toolanen G, .agerlund M, Bj?rnebrink J. Disc pathology after whiplash injury: a
prospective magnetic resonance imaging and clinical investigation. Spine 1997;22:283–7.
22. Eck JC, Hodges SD, Humphreys SC. Whiplash: a review of a commonly misunderstood injury. Am J Med
2001;110:651–6.
23. Kongsted A, Sorensen JS, Andersen H, Keseler B, Jensen TS, Bendix T. Are early MRI findings correlated
with long-lasting symptoms following whiplash injury? A prospective trial with 1-year follow-up. Eur Spine J
2008;17:996–1005.
24. Juan .J. Use of botulinum toxin-A for musculoskeletal pain in patients with whiplash associated disorders.
BMC Musculoskelet Disord. 2004;5:5(1-10).
25. Borchgrevink GE, Kaasa A, McDonagh D, Stiles TC, Haraldseth O, Lereim I. Acute treatment of whiplash
neck sprain injuries. Spine 1998;23(1):25–31.
26. Rosenfeld M, Seferiadis A, Carlsson J, Gunnarsson R. Active intervention in patient with whiplash-associated
disorder improves long-term prognosis. Spine 2003;28:2491–8.
27. Seferiadis A, Rosenfeld M, Gunnarsson R. A review of treatment interventions in whiplash-associated disorders.
Eur Spine J 2004; 13(5):387-97.
28. Scholten-Peeters G, Bekkering G, Verhagen A, Windt D Van der, Lanser K, Hendricks E, et al. Clinical practice
guideline for the physiotherapy of outpatients with whiplash associated disorders. Spine 2002;27(4):412-22.
29. Conlin A, Bhogal S, Sequeira K, Teasell R. Treatment of whiplash-associated disorders—part I: Non-invasive
interventions. Pain Res Manag 2005;10(1):21-32.
30. .reeman MD, Croft AC, Rossignol AM. Whiplash associated disorders: refining whiplash and it’s management’
by the Quebec Task .orce. Spine 1998,23(9):1043-49.
31. Trinh K, Graham N, Gross A, Goldsmith C, Wang E, Cameron I, et al. Acupuncture for neck disorders. Spine
2007;32(2):236-43.
32. Kong J, .ufa D, Gerber A, Rosman I, Vangel M, Graceley R, et al. Psychophysical outcomes from a
randomised pilot study of manual, electro and sham acupuncture treatment on experimentally induced thermal
pain. Journal of Pain 2005;6(1):55-64.
33. Verhagen AP, Scholten-Peeters G, van Wijngaarden S, de Bie RA, Bierma-Zeinstra SMA. Conservative treatments
for whiplash [Systematic Review]. Cochrane Database Syst Rev2007;4:4.
34. Nijs J, Van Oosterwijck J, De Hertogh W. Rehabilitation of chronic whiplash: treatment of cervical dysfunctions
or chronic pain syndrome? Clin Rheumatol 2009;28(3):243-51.
35. Stewart MJ, Maher CG, Refshauge KM, Herbert RD, Bogduk N, Nicholas M. Randomized controlled trial of
exercise for chronic whiplash-associated disorders. Pain 2007;128:59-68.
36. Jull G, Sterling M, Kenardy J, Beller E. Does the presence of sensory hypersensitivity influence outcomes of
physical rehabilitation for chronic whiplash? - A preliminary RCT. Pain 2007;129(2):28-34.
37. McDonald GJ, Lord SM, Bogduk N. Long-term follow-up of patients treated with cervical radiofrequency
neurotomy for chronic neck pain. Neurosurgery 1999,45:61-8.](https://image.slidesharecdn.com/all-101224135812-phpapp02/85/53-196-320.jpg)


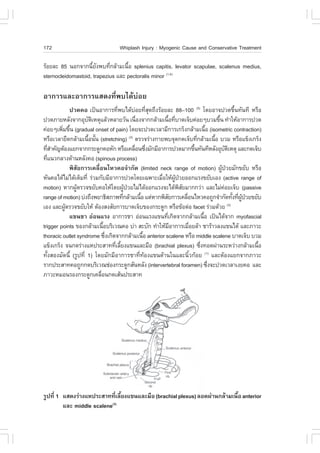



































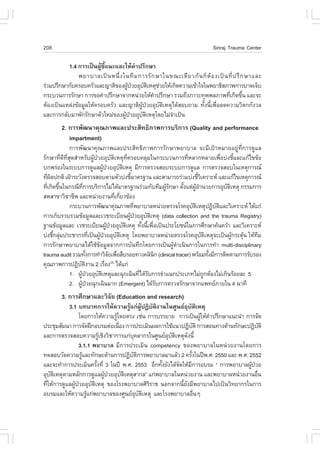






















































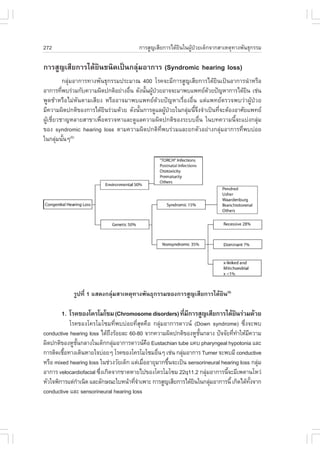























































![330 ÂÒ¨Ò¡ÊÁعä¾Ã¡ÑºàǪÈÒʵÃàªÔ§»ÃШѡÉ
¡Ã³Õ·Õè 3 ÂÒ¨Ò¡ÊÁعä¾Ã·ÕÁ¡ÒÃÈÖ¡ÉÒ¹ŒÍ ¤×Í ÂÒËÍÁ¹Çâ¡°
è Õ
ã¹ÊÀÒ¾¡Ò󻨨غ¹ ÂѧÁÕà¤Ã×ͧÂÒáÅеíÒÃѺÂÒá¼¹ä·ÂÍÕ¡ÁÒ¡·ÕäÁ‹Á¡ÒÃÈÖ¡ÉÒã´æàÅÂ
˜ Ñ è è Õ
ÊÒà˵طÕè¡ÒÃÇԨѷҧ¤ÅÔ¹Ô¡¢Í§ÂÒ¨Ò¡ÊÁعä¾ÃÁÕäÁ‹ÁÒ¡ ÍÒ¨ÁÒ¨Ò¡¢ŒÍ¨íÒ¡Ñ´ËÅÒ»ÃСÒà ઋ¹
¡ÒäǺ¤ØÁ¤Ø³ÀÒ¾¢Í§ÂÒ¨Ò¡ÊÁعä¾Ã·Õ㪌㹡Ò÷´Åͧ ¢ŒÍÁÙŨҡ¡ÒÃÈÖ¡ÉÒã¹ËÅÍ´·´ÅͧËÃ×Í
è
ÊѵǷ´ÅͧäÁ‹à¾Õ§¾Í ·íÒãËŒÁ¢Í«Ñ¡¶ÒÁà¡ÕÂǡѺ¨ÃÔ¸ÃÃÁ¡ÒÃÇÔ¨Â㹤¹ ໚¹µŒ¹ Í‹ҧäáç´Õ “¶Ö§áÁŒ
Õ Œ è Ñ
¨Ð¢Ò´ËÅÑ¡°Ò¹·Õè໚¹ RCT ·Õè¨Ð·íÒãËŒÃдѺ¢Í§ËÅÑ¡°Ò¹ÁÕ¤ÇÒÁ¹‹Òàª×èͶ×Í໚¹ÃдѺ 1 ËÃ×ÍäÁ‹
ÁÕ¡ÒÃÇÔ¨ÑÂã´æàÅ ¡çÁÔä´ŒËÁÒ¤ÇÒÁÇ‹ÒÂÒ¨Ò¡ÊÁعä¾ÃäÁ‹ÁÕ»ÃÐÊÔ·¸ÔÀÒ¾ à¹×èͧ¨Ò¡¡ÒÃ㪌ÂÒ
¨Ò¡ÊÁØ ¹ ä¾Ã໚ ¹ ͧ¤ ¤ ÇÒÁÃÙŒ ·Õè à ¡Ô ´ ¨Ò¡¡ÒÃÊÑè § ÊÁÁÒÍ‹ Ò §ÂÒǹҹ¢Í§á¾·Â á ¼¹ä·Â
(á¼¹âºÃÒ³) áÅÐËÁ;׹ºŒÒ¹ÁÒ¡ÁÒ ´Ñ§¹Ñ¹¡ÒõѴÊÔ¹ã¨àÅ×͡㪌ÂÒÊÁعä¾Ã¨Ö§¤ÇÃ㪌¢ÍÁÙÅ
é é Œ
ËÅÒÂæ ´ŒÒ¹»ÃСͺ¡Ñ¹ ·Ñé§ËÅÑ¡°Ò¹àªÔ§»ÃШѡÉáÅÐͧ¤¤ÇÒÁÃÙŒ´Ñé§à´ÔÁ” äÁ‹¤ÇÃãËŒà¡Ô´¡Ã³Õ
àËÁ×͹㺢ÕàËÅç¡·ÕÁ¡ÒÃÇÔ¨ÂʹѺʹعNjÒÁռŪ‹Ç¤ÅÒ¡ѧÇÅáÅЪ‹ÇÂãËŒ¹Í¹ËÅѺ ¨Ö§ÁÕ¡ÒùíÒÁÒ¼ÅÔµ
é è Õ Ñ
໚¹ÂÒàÁç´áÅÐ᤻«ÙÅà¾×Íãˌú»Ãзҹ䴌§ÒÂàËÁ×͹ÂÒá¼¹»˜¨¨Øº¹ «Ö§µ‹ÍÁÒ¾ºÇ‹Ò·íÒãËŒà¡Ô´ÀÒÇÐ
è Ñ ‹ Ñ è
µÑºÍÑ¡àʺà©Õº¾Åѹ ¨¹Êíҹѡ§Ò¹¤³Ð¡ÃÃÁ¡ÒÃÍÒËÒÃáÅÐÂÒÊѧÃЧѺ¡ÒüÅÔµáÅÐàÃÕ¡à¡çº¤×¹ÂÒ¨Ò¡
è
ÊÁعä¾Ã¢ÕàËÅç¡à´ÕÂÇ·ÕÁ¢Íº‹§ãªŒÊÒËÃѺª‹ÇÂãËŒ¹Í¹ËÅѺ ¡Ã³Õ¹áÊ´§ãËŒàËç¹Ç‹Ò¡ÒÃ㪌ÂÒ¨Ò¡ÊÁعä¾Ã
é è è ÕŒ í (21)
Õé
¤ÇäíÒ¹Ö§¶Ö§Í§¤¤ÇÒÁÃÙ´§à´ÔÁ´ŒÇ à¾ÃÒÐâ´Â·ÑÇä»ÈÒʵáÒÃá¾·Âá¼¹ä·Â¨ÐäÁ‹á¹Ð¹íÒÃѺ»Ãзҹ
Œ Ñé è
ÊÁعä¾ÃµÑÇà´ÕÂÇã¹¢¹Ò´ÊÙ§æ Áѡ㪌»ÃСͺ¡Ñ¹ËÅÒª¹Ô´à»š¹ÂÒµíÒÃѺà¾×ÍàÊÃÔÁÄ·¸ÔËÃ×ÍÅ´¾Ôɺҧè ì
Í‹ҧ¢Í§ÊÁعä¾Ãã¹µíÒÃѺ µÒÁÀÙÁ»Ò¢Í§ä·ÂÇԸú»Ãзҹ㺢ÕàËÅç¡ãËŒ»ÅÍ´ÀѤ×͵ŒÁËÃ×ʹͧ
Ô ˜ ÕÑ é
àËŌҡ‹Í¹ ¨Ö§àÍÒ¹éÒÁÒÃѺ»Ãзҹ ËÃ×ͶŒÒ¨ÐÃѺ»Ãзҹ·Ñ§ãº¡çµÍ§¹íÒä»»Ãا໚¹á¡§¢ÕàËÅç¡
í é Œ é
â´ÂÊÃØ»¡ÒÃãËŒ¤ÇÒÁÊíҤѡѺËÅÑ¡°Ò¹àªÔ§»ÃШѡÉà¾Õ§Í‹ҧà´ÕÂÇÁÒ¡à¡Ô¹ä» ÍÒ¨äÁ‹ÊÒÁÒö
·íÒãËŒ¡ÒÃ㪌ÂÒ¨Ò¡ÊÁعä¾Ãà¡Ô´¤ÇÒÁ»ÅÍ´ÀÑÂáÅÐÁÕ»ÃÐÊÔ·¸Ô¼Å µŒÍ§ÍÒÈÑÂͧ¤¤ÇÒÁÃٷ໚¹ÀÙÁ»Ò Œ Õè Ô ˜
´Ñ§à´ÔÁËÇÁ´ŒÇ ¢³Ðà´ÕÂǡѹ¶ŒÒäÁ‹ÁËÅÑ¡°Ò¹àªÔ§»ÃШѡÉã´æÁÒʹѺʹع ᾷ¼ʧ㪌ÂÒ¨Ò¡ÊÁعä¾Ã
é Õ ÙŒ Ñè
¡ç¤ÇÃ㪌µÒÁËÅÑ¡¡Òâͧ¡ÒÃá¾·Âá¼¹ä·ÂáÅÐÁÕ¡ÒÃཇÒÃÐÇѧµÔ´µÒÁáÅÐà¡çº¢ŒÍÁÙÅãˌ໚¹Ãкº
áÅеŒÍ§ÃÐÇѧ¡ÒÃ㪌ÂÒ¨Ò¡ÊÁعä¾ÃÍ‹ҧäÁ‹ÊÁà˵ØÊÁ¼Åà¹×ͧ¨Ò¡¡ÒÃÍǴ͌ҧÊÃþ¤Ø³·Õà¡Ô¹¨ÃÔ§
è è
àÍ¡ÊÒÃ͌ҧÍÔ§
1. WHO. .act sheet N?134 2008 [cited 2010 May 17]; Available from: http://www.who.int/mediacentre/factsheets/
fs134/en/index.html.
2. Rattanachaiyanont M. Clinical evidence in menopause medicine: Part 2 evaluating the evidence. Siriraj Med
J 2006;58(5).
3. Phillips B, Ball C, Sackett D, et al. Oxford Centre for Evidence-based Medicine Levels of Evidence. 2009
[updated 2009 March; cited 2010 June 08]; Available from: http://www.cebm.net/index.aspx?o=1025.
4. ÁÙŹԸ¿¹¿ÙʧàÊÃÔÁ¡ÒÃá¾·Âä·Âà´ÔÁ, âçàÃÕ¹ÍÒÂØÃàÇ·¸íÒç ʶҹ¡ÒÃá¾·Âá¼¹ä·Â»ÃÐÂØ¡µ ¤³Ðá¾·ÂÈÒʵÃÈÃÔ
Ô „œ ‹ Ô
ÃÒª¾ÂÒºÒÅ ÁËÒÇÔ·ÂÒÅÑÂÁËÔ´Å. µíÒÃÒ¡ÒÃá¾·Âá¼¹ä·Âà´ÔÁ (á¾·ÂÈÒʵÃʧà¤ÃÒÐË ©ºÑºÍ¹ØáÉ) àÅ‹Á·Õè 1 ©ºÑºªíÒÃÐ
Ñ
¾.È.2550 à¹×èͧã¹ÁËÒÁ§¤ÅÇâáÒÊà©ÅÔÁ¾ÃЪ¹ÁÒÂØ 80 ¾ÃÃÉÒ ¾ÃкҷÊÁà´ç¨¾ÃÐ਌ÒÍÂÙ‹ËÑÇÀÙÁÔ¾ÅÍ´ØÅÂà´ª.
¡Ãا෾Ï: ÈØÀǹԪ¡ÒþÔÁ¾; ¾.È.2550.](https://image.slidesharecdn.com/all-101224135812-phpapp02/85/53-357-320.jpg)
![àǪÈÒʵ÷¹Âؤ 2553
Ñ 331
5. ¤³Ð¡ÃÃÁ¡ÒÃáË‹§ªÒµÔ´Ò¹ÂÒ. ºÑªÕÂÒ¨Ò¡ÊÁعä¾Ã ¾.È.2549 µÒÁ»ÃСÒȤ³Ð¡ÃÃÁ¡ÒÃáË‹§ªÒµÔ´Ò¹ÂÒ (©ºÑº·Õè 5)
Œ Œ
¾.È. 2549 àÃ×ͧºÑªÕÂÒËÅÑ¡áË‹§ªÒµÔ ¾.È. 2547 (©ºÑº·Õè 4). ¡Ãا෾Ï: âç¾ÔÁ¾ªÁ¹ØÁÊˡó¡ÒÃà¡ÉµÃáË‹§»ÃÐà·Èä·Â
è Ø
¨íÒ¡Ñ´; 2549.
6. Rotblatt M, Ziment I, editors. Evidence-based herbal medicine. Philadelphia: Hanley&Belfus, INC; 2002.
7. Neha S, Ranvir GD, Jangade CR. Analgesic and antipyretic activities of Curcuma longa rhizome extracts in
Wistar Rats. Veterinary World 2009;2(8):304-6.
8. ÇÔÊ´Ò ÊØÇ·ÂÒÇѲ¹, ¾ÃŒÍÁ¨Ôµ ÈÃÅÑÁ¾, ¹¾ÁÒÈ Êع·Ãà¨ÃÔ¹¹·, áÅФ³Ð. ÂÒ¨Ò¡ÊÁعä¾Ã㹺ѪÕÂÒËÅÑ¡áË‹§ªÒµÔ:
Ø Ô
¢ŒÍÁÙź¹ËÅÑ¡°Ò¹·Ò§ÇÔªÒ¡ÒÃ. ¡Ãا෾Ï: áʧà·Õ¹¡ÒþÔÁ¾; ¾.È. 2552.
9. Chen IN, Chang CC, Ng CC. antioxidant and antimicrobial activity of zingiberaceae plants in Taiwan. Plant
.oods Hum Nutr 2008;63:15–20.
10. Ulbricht CE, editor. Natural standard herb & supplement guide: an evidence-based reference Missouri: Mosby
Inc.; 2010.
11. ´Ç§¡ÁŠʨÔÃÇѲ¹Ò¡ØÅ. ÊÁعä¾Ã¿‡Ò·ÐÅÒÂâ¨ÃʺËÇÑ´2009. ¡Ãا෾¸ØáԨ. ¾.È.2552 Çѹ·Õè 19 ¡Ã¡®Ò¤Á 2552
04:00.
12. Coon JT, Ernst E. Andrographis paniculata in the treatment of upper respiratory tract infections: a systematic
review of safety and efficacy. Planta Med. [Systematic review] 2004;70:293-8.
13. àʧÕÂÁ ¾§ÉÃÍ´. äÁŒà·ÈàÁ×ͧä·Â. ¡Ãا෾Ï: âç¾ÔÁ¾¡Ãا¸¹; ¾.È.2522.
è
14. ÁÐÃØÁ ¾×ª¾×¹ºŒÒ¹ÁËÑȨÃÃÂ. ÇÒÃÊÒÃà¡ÉµÃ¡ÃÃÁ¸ÃÃÁªÒµÔ. ¾.È.2551:11-9.
é
15. Dolly J, Kumar Rai P, Kumar A, Mehta S, Watal G. Effect of Moringa oleifera Lam. leaves aqueous extract
therapy on hyperglycemic rats . J Ethnopharmacol. 2009;123(3):392-6.
16. Anthanont P, Lumlerdkij N, Akarasereenont P, Vannasaeng S, Sriwijitkamol A. Moringa oleifera leaf increases
insulin secretion after single dose administration in healthy subjects: a pilot study. 2010.
17. .ahey JW. Moringa oleifera: A review of the medical evidence for its nutritional, therapeutic, and prophylactic
properties. Part 1. Trees for Life. 2005;1.
18. .akurazi S, Hairuszah I, Nanthini U. Moringa oleifera Lam prevents acetaminophen induced liver injury
through restoration of glutathione level. .ood Chem Toxicol. 2008;46:2611–5.
19. Komal Mehta L, Balaraman R, Amin AH, Bafna PA, Gulati OD. Effect of fruits of Moringa oleifera on the lipid
profile of normal and hypercholesterolaemic rabbit. J Ethnopharmacol. 2003;86:191-5.
20. Siddhuraju P, Becker K. Antioxidant properties of various solvent extracts of total phenolic constituents from
three different agroclimatic origins of drumstick tree (Moringa oleifera Lam.) leaves . J Agric .ood Chem.
2003;51:2144-55.
21. ˹ѧÊ×;ÔÁ¾ä·ÂÃÑ°. ÊѧÃЧѺÂÒÊÁعä¾Ã㺢ÕàËÅç¡à´ÕÂÇ ¾.È.2551 [cited 2551 04-07].
è é è](https://image.slidesharecdn.com/all-101224135812-phpapp02/85/53-358-320.jpg)






















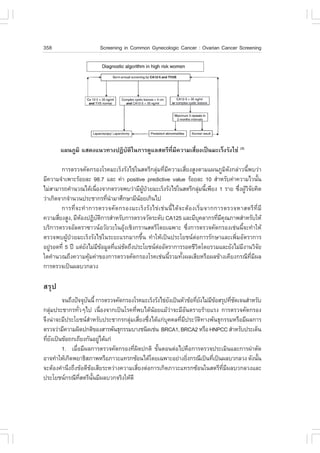


































![àǪÈÒʵ÷¹Âؤ 2553
Ñ º··Õè 401
59
¡ÒÃÈÖ¡ÉҼšÃзºµ‹ÍÊØ¢ÀÒ¾»ÃЪҪ¹·ÕèÍÒÈÑÂÍÂÙ‹
Ãͺ¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´
ÃͧÈÒʵèÒà´Ã. ¹ÔµÂÒ ÇѨ¹ÐÀÙÁÔ
ÃͧÈÒʵÃÒ¨Òà´Ã. ¹Ñ¹·ÇÃó ÇÔ¨ÔµÃÇÒ·¡ÒÃ
¤³ÐÊÒ¸ÒóÊØ¢ÈÒʵà ÁËÒÇÔ·ÂÒÅѸÃÃÁÈÒʵÃ
»ÃÒ³Õ ªÒ³Ã§¤
¤³Ðá¾·ÂÈÒʵà ÁËÒÇÔ·ÂÒÅѸÃÃÁÈÒʵÃ
»ÃÐà·Èä·Âä´ŒÁÕ¡ÒþѲ¹Òã¹ÀÒ¤ÍصÊÒË¡ÃÃÁµ‹Íà¹×èͧ¡Ñ¹ÁÒ໚¹àÇÅÒËÅÒ·ÈÇÃÃÉ
ã¹µŒ¹»‚ ¾.È. 2520 ÁÕ¡ÒüÅÑ¡´Ñ¹â¤Ã§¡ÒÃÍÕÊà·Ôù«ÕºÍô â´ÂÁÕ¡ÒÃÇҧἹ¾Ñ²¹ÒÍ‹ҧµ‹Íà¹×ͧ
è
ÂÒǹҹÃÇÁ 50 »‚ ¡íÒ˹´ãËŒ¾¹·ÕºÃÔàdzáËÅÁ©ºÑ§ ¨Ñ§ËÇÑ´ªÅºØÃÕ à»š¹·ÕÃͧÃѺÍصÊÒË¡ÃÃÁàºÒ ઋ¹
×é è è
¡ÒûÃСͺªÔé¹Ê‹Ç¹ÍØ»¡Ã³ä¿¿‡ÒÍÔàÅç¡·Ã͹ԡÊáÅоÅÒʵԡ áÅо×é¹·ÕèÁÒºµÒ¾Ø´¡íÒ˹´ãˌ໚¹
ࢵ¾Ñ ² ¹ÒÍØ µ ÊÒË¡ÃÃÁË¹Ñ ¡ ·Õè à ¡Õè  ǢŒ Í §¡Ñ º » â µÃàÅÕ Â Á áÅл â µÃà¤ÁÕ ¨í Ò ¹Ç¹ÁÒ¡ ÃÇÁ·Ñé §
ÍصÊÒË¡ÃÃÁÍ×¹ ઋ¹ àËÅç¡ áÅлØÂà¤ÁÕ à»š¹µŒ¹(1) «Ö§ÃÑ°ºÒÅÁÕ¤ÇÒÁÁاËÇѧNjÒâ¤Ã§¡ÒùըзíÒ¤ÇÒÁ
è ‰ è ‹ é
à¨ÃÔ·Ò§àÈÃÉ°¡Ô¨áÅоѲ¹ÒãËŒ»ÃÐà·Èä·Â໚¹»ÃÐà·ÈÍصÊÒË¡ÃÃÁãËÁ‹
ÍصÊÒË¡ÃÃÁ»âµÃàÅÕÂÁáÅÐÍصÊÒË¡ÃÃÁ»âµÃà¤ÁÕ໚¹áËÅ‹§¡íÒà¹Ô´¢Í§ÊÒÃÍÔ¹·ÃÕÂÃÐà˧‹ÒÂ
(Volatile organic compounds [VOCs]) ¡ÒÃÈÖ¡ÉÒ·Ò§¾ÔÉÇÔ·ÂÒ¾ºÇ‹Ò VOCs ºÒ§ª¹Ô´à»š¹ÊÒÃ
¡‹ÍÁÐàÃç§ àª‹¹ benzene áÅÐ vinyl chloride(2,3) áÅСÒÃÊÑÁ¼ÑÊ VOCs ºÒ§ª¹Ô´ã¹»ÃÔÁÒ³ÁÒ¡
ઋ¹ 1,3 butadiene, 1,2-dichloroethene, toluene, benzene, styrene áÅÐ xylene(2,4,5,6,7,8) ÍÒ¨·íÒãËŒ
à¡Ô´ÍÒ¡Ò÷ҧÃкº»ÃÐÊÒ··Ñ§áººà©Õº¾Åѹ áÅÐàÃ×ÍÃѧ ઋ¹ ÍÒ¡ÒäÅ×¹äÊŒ ÍÒà¨Õ¹ ÁÖ¹ÈÕÃÉÐ
é é è
§‹Ç§«ÖÁ «ÖÁàÈÃŒÒ à˹×ÍÂÅŒÒ ¡ÒÃÊÙàÊÕ¡Ò֍µÑÇ ÊÙàÊÕ¤ÇÒÁ·Ã§¨íÒ ¢Ò´ÊÁÒ¸Ô ¡ÅŒÒÁà¹×Í͋͹áç
è é
¹Í¡¨Ò¡¹Õé ¡ÒÃÈÖ¡ÉÒã¹ÊѵǷ´Åͧ¾ºÇ‹Ò¡ÒÃÊÑÁ¼ÑÊ 1,2-dicholroethene Áռŵ‹Í¡ÒÃà¨ÃÔàµÔºâµ¢Í§
µÑÇ͋͹(5) áÅСÒÃÈÖ¡ÉÒ·Ò§ÃкҴÇÔ·ÂÒËÅÒÂÃÒ§ҹ¾ºÇ‹Ò ÁÒôҷÕèÍÒÈÑÂÍÂÙ‹ã¡ÅŒÍصÊÒË¡ÃÃÁ
»âµÃà¤ÁÕËÃ×Íâç¡ÅÑè¹¹éíÒÁѹÁÕâÍ¡ÒÊ·ÕèãËŒ¡íÒà¹Ô´·Òᡋ͹¡íÒ˹´ áÅзÒáÁÕ¹éíÒ˹ѡµèíÒ¡Ç‹Ò
Áҵðҹ (9, 10, 11, 12)
ã¹ÃÐÂÐ 2-3 »‚ ·Õ輋ҹÁÒ »ÃЪҪ¹â´ÂÃͺ¹Ô¤ÁÍصÊÒË¡ÃÃÁÁÒºµÒ¾Ø´ÁÕ¡Òõ×è¹µÑǶ֧
¼Å¡Ãзºµ‹ÍÊØ¢ÀÒ¾·ÕÍҨ䴌ú¨Ò¡ÁžÔÉÍصÊÒË¡ÃÃÁ ᵋ¡ÒÃÈÖ¡ÉÒ·Ò§ÃкҴÇÔ·ÂÒà¡ÕÂǡѺàÃ×ͧ¹Õé
è Ñ è è](https://image.slidesharecdn.com/all-101224135812-phpapp02/85/53-428-320.jpg)