Downloaded 43 times



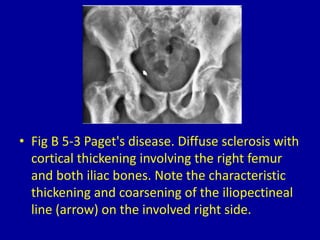
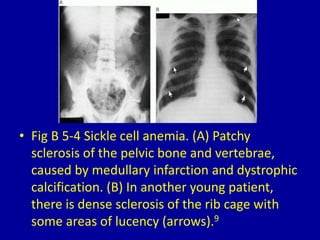
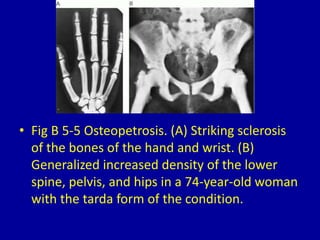













1. The document describes and shows images of various medical conditions that result in generalized osteosclerosis, or increased bone density, seen on clinical imaging. 2. These conditions include myelosclerosis, Paget's disease, sickle cell anemia, osteopetrosis, pyknodysostosis, melorheostosis, fluorosis, progressive diaphyseal dysplasia, polyostotic fibrous dysplasia, renal osteodystrophy, congenital syphilis, sclerotic myeloma, and hereditary hyperphosphatasia. 3. For each condition, the document provides a brief description and labeled image showing the patterns of sclerosis visible on imaging of the



































































































