Downloaded 30 times

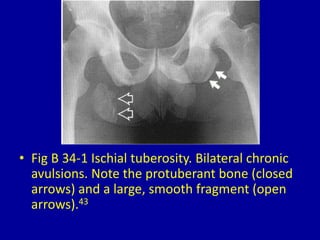


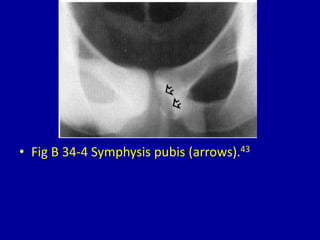
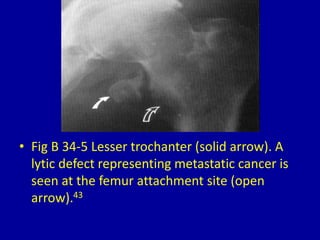


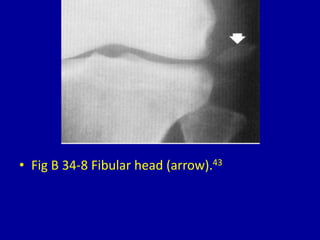
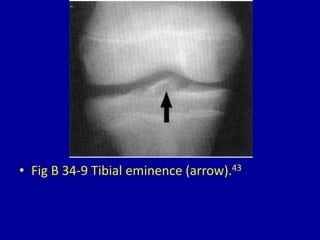
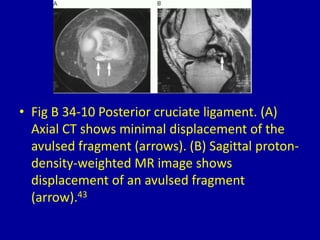
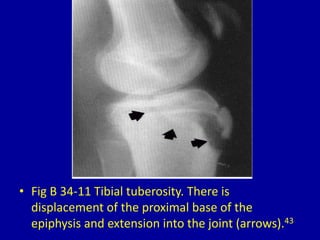
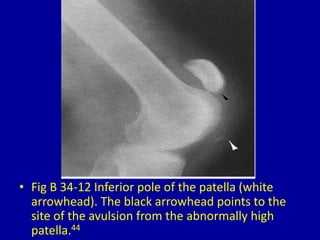

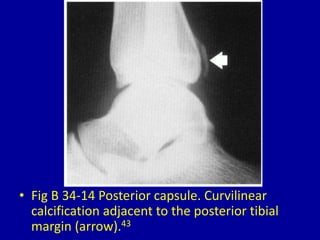
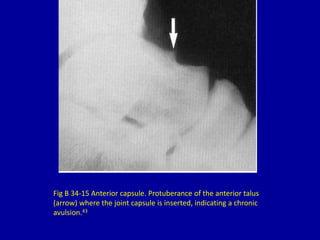
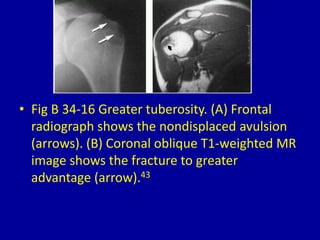



This document provides descriptions and images of avulsion injuries at various anatomical locations in the body. Avulsion injuries refer to the tearing away of a tendon, ligament, or muscle from the bone. The document lists 17 figures showing examples of avulsion injuries at locations such as the ischial tuberosity, anterior superior iliac spine, anterior inferior iliac spine, symphysis pubis, lesser trochanter, greater trochanter, fibular head, tibial eminence, posterior cruciate ligament, tibial tuberosity, inferior pole of the patella, calcaneal tuberosity, anterior and posterior capsule of the ankle joint, greater and lesser tuberosity of the























































































