This document discusses oncologic emergencies, focusing on tumor lysis syndrome (TLS). It provides details on:
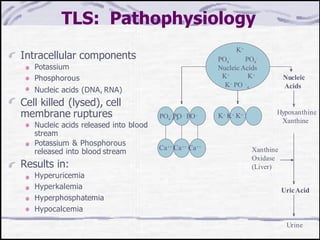
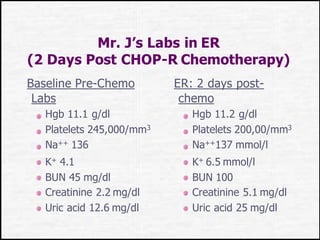
- The pathophysiology of TLS, which is caused by the breakdown of rapidly proliferating malignant cells, releasing intracellular components like potassium, phosphorus, and nucleic acids.
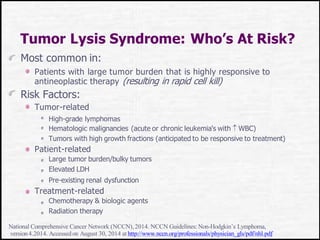
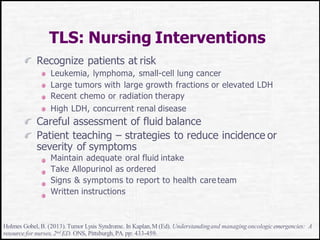
- Risk factors for TLS including certain cancers, large tumor burdens, and chemotherapy or radiation therapy.
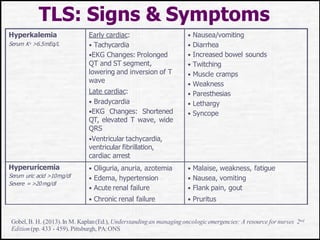
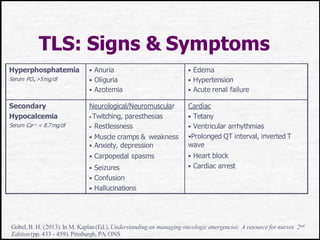
- Clinical manifestations of TLS which are due to electrolyte abnormalities and can include arrhythmias, seizures, and renal failure.
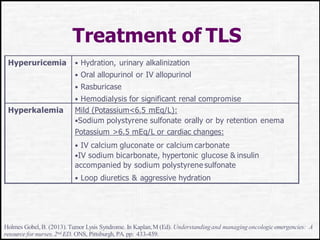
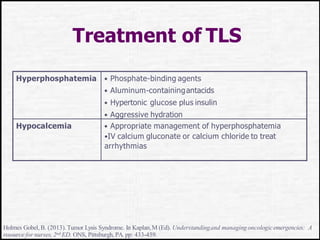
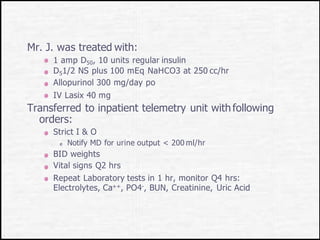
- Prevention strategies like hydration, allopurinol to control uric acid, and rasburicase. Monitoring of at-risk patients is also important.