Download to read offline

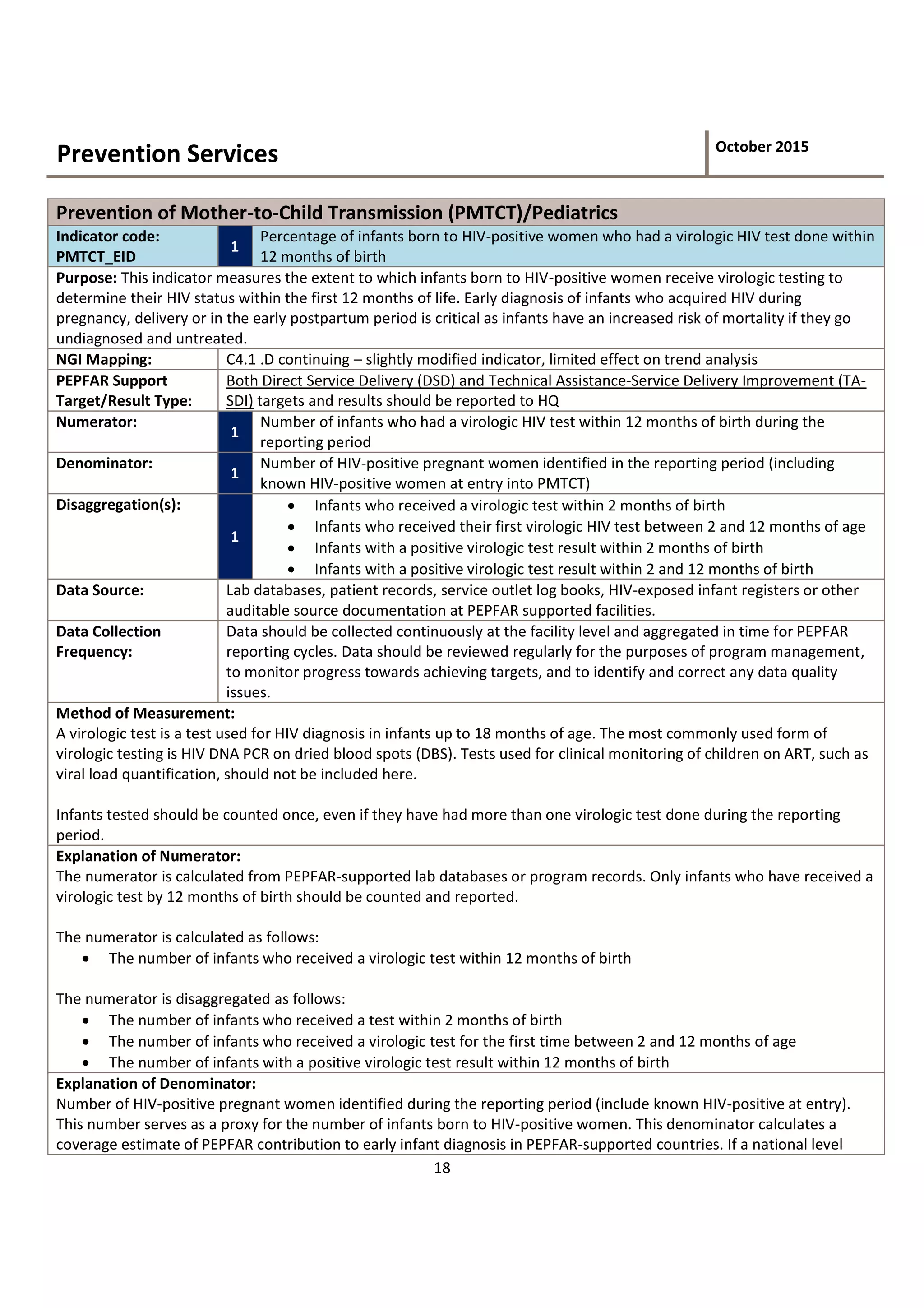



This document defines the indicator "Percentage of infants born to HIV-positive women who had a virologic HIV test done within 12 months of birth". It provides details on the numerator, denominator, and disaggregation categories for this indicator, which measures how many exposed infants receive early testing to determine their HIV status. Early diagnosis is critical to ensure untreated infants receive necessary treatment. The document also describes how to calculate and interpret this indicator, and what types of PEPFAR support can be counted.






















































































