Download to read offline
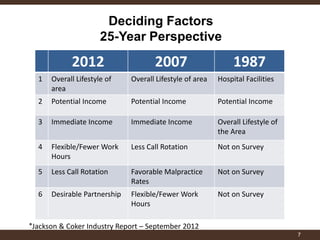
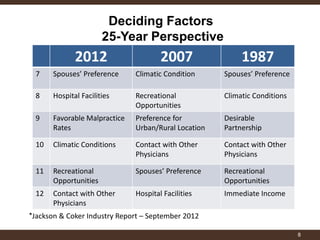


This document discusses the changing landscape of recruiting physicians to medical practices. It outlines key reasons why physicians join practices, including financial factors, lifestyle preferences, and positive group dynamics. Younger physicians tend to prioritize lifestyle, while experienced physicians aged 50-65 are considering reducing hours or retiring. The document also notes challenges practices face when physicians leave or retire, such as increased costs and difficulties replacing physicians. Overall, it provides an overview of trends in physician recruitment and retention.











































































































