Download as PDF, PPTX



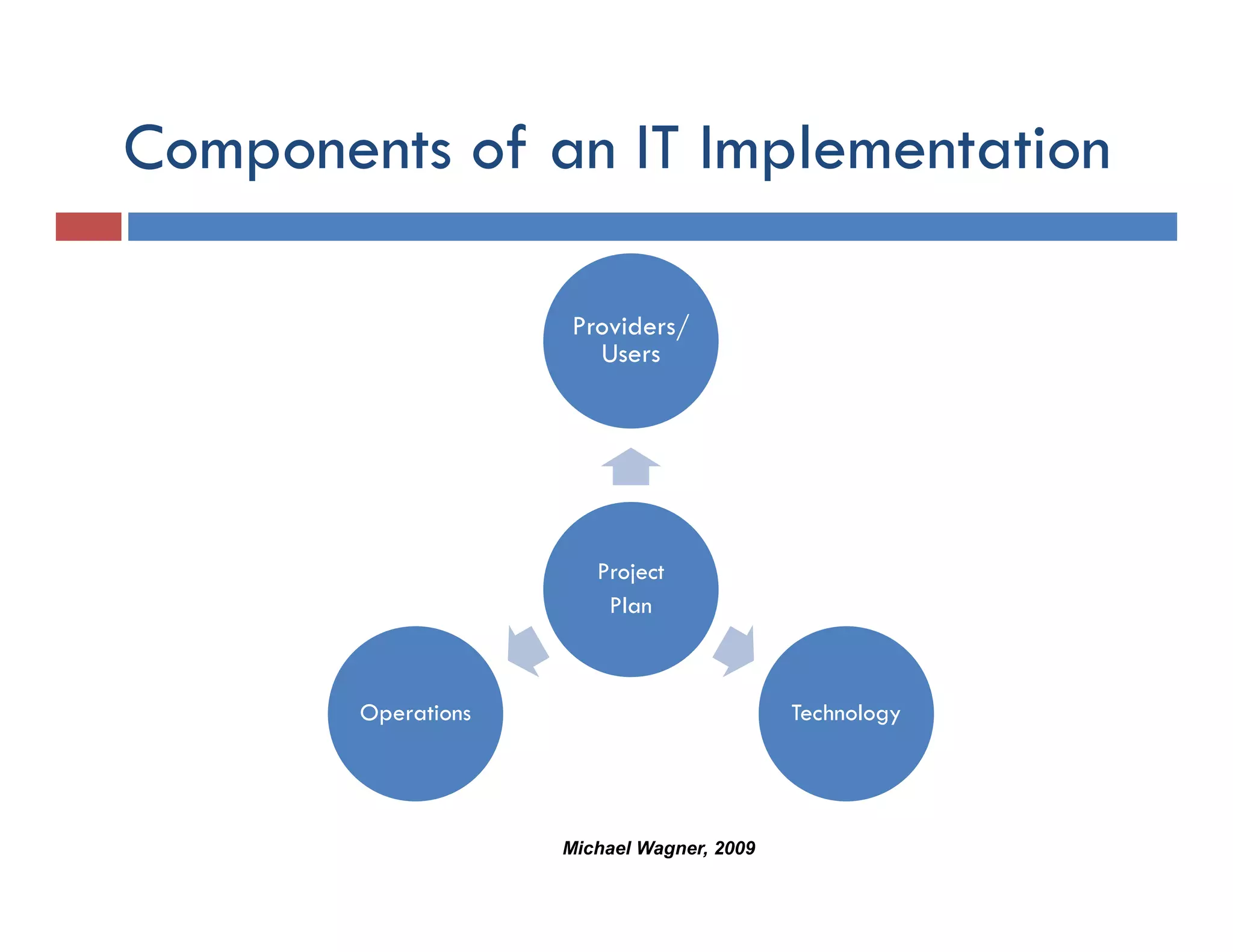
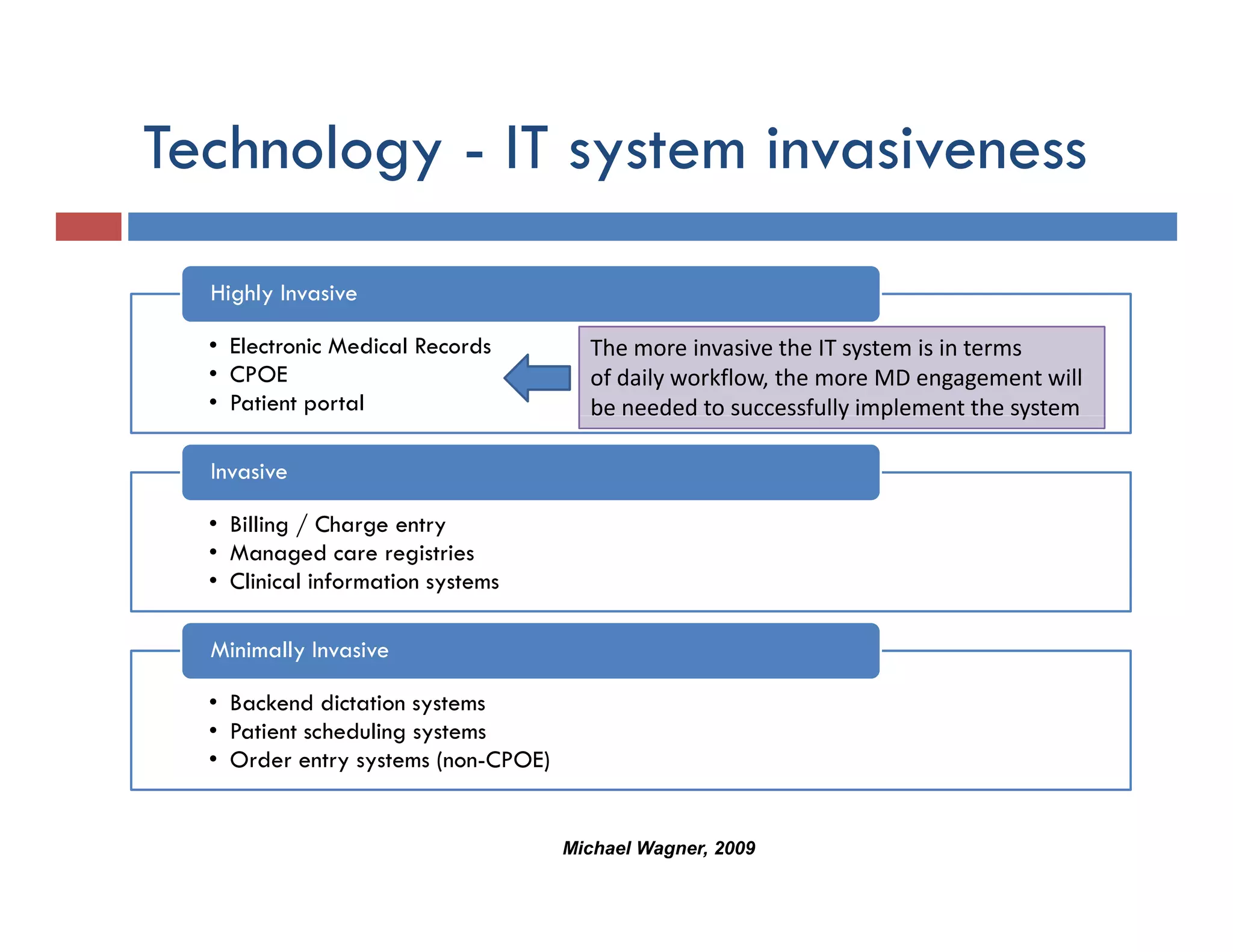

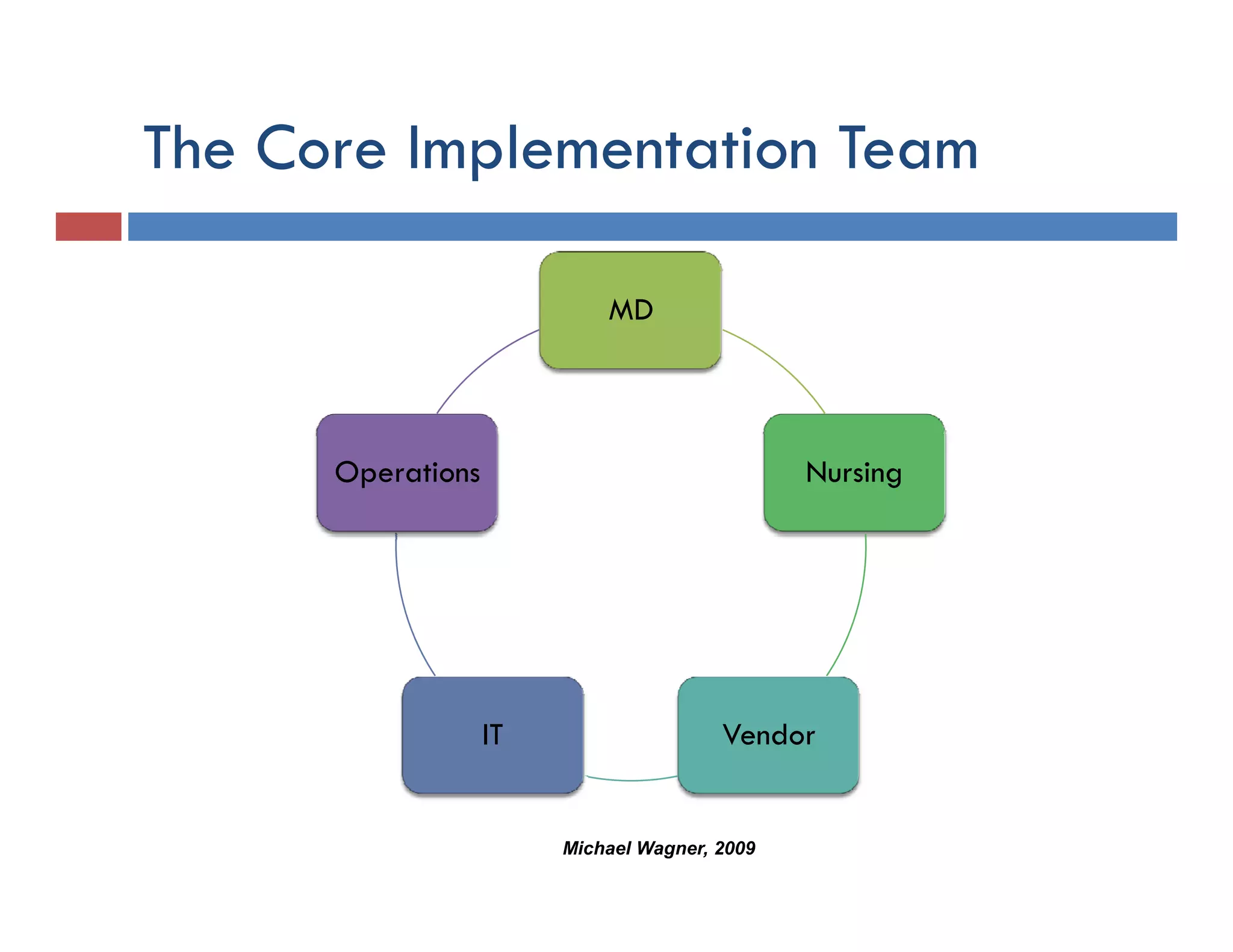

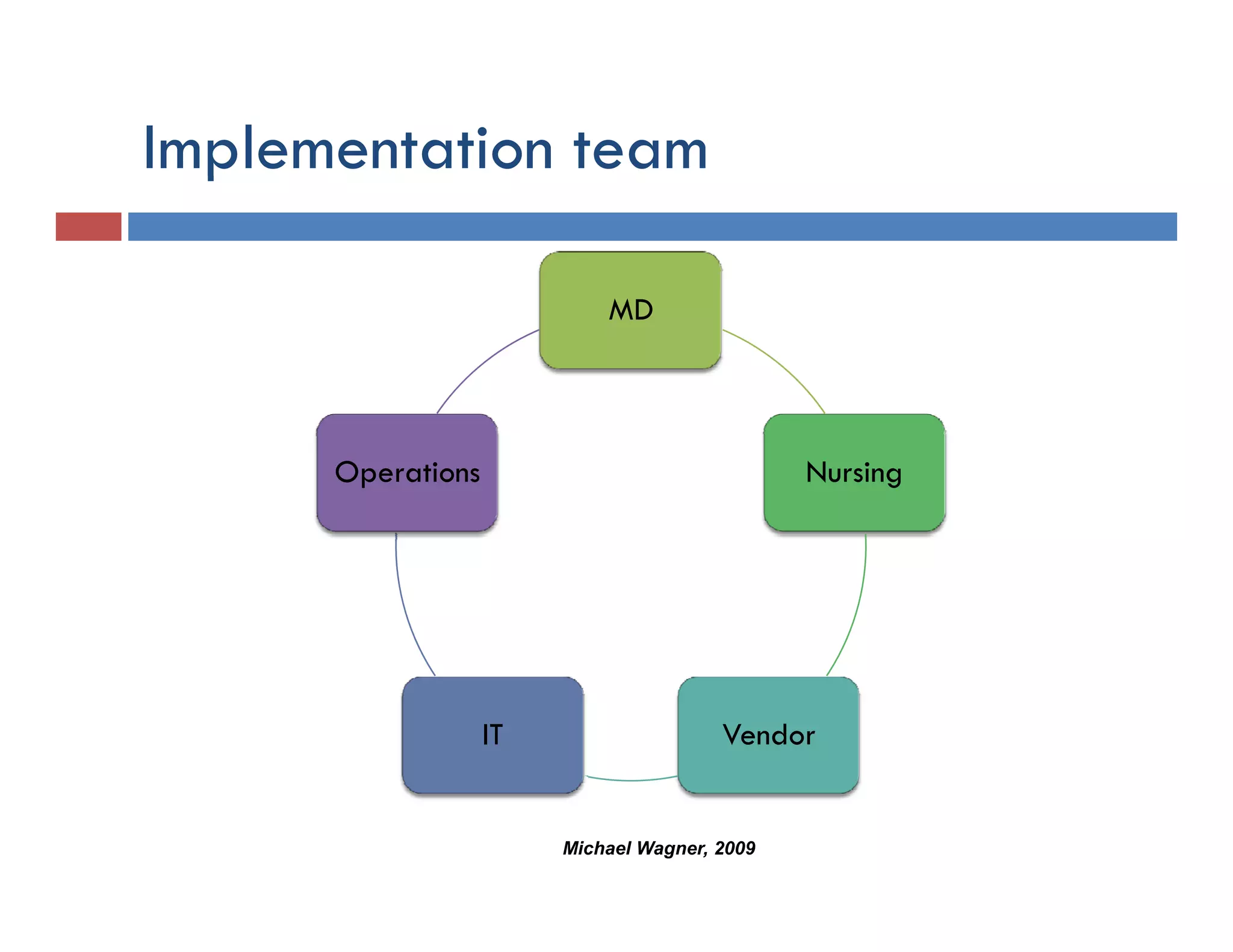



This document discusses achieving physician buy-in for effective IT adoption and engagement. It begins with biographical information about the speaker, Dr. Michael Wagner, who has experience leading IT projects in both academic and community physician practices. The presentation outlines key factors to consider for a successful IT implementation, including engaging physician leadership, understanding how invasive the new technology will be, ensuring appropriate organizational support, and addressing provider concerns. Effective project management and establishing a core implementation team are also emphasized.

































































