Downloaded 57 times

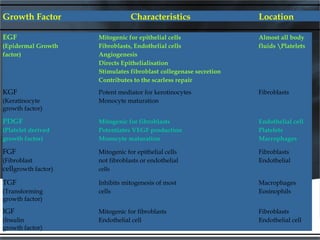
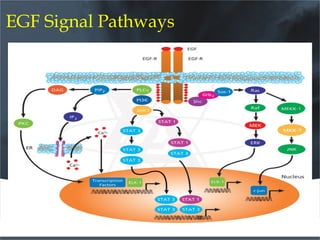
![HEMOSTASIS 1 hour
W
O
U
N
D
I
N
G
Platelets
Fibrin
INFLAMMATION days 1 through 7
Proteoglycans
Neutrophils
Macrophages]
Lymphocytes
PROLIFERATION days 2 through 20
Normal wound
healing
Fibroblasts[produce growth factors]
Collagen
Epithelial Cells
Endothelial Cells
REMODELING 1 week to 6 months
Collagen Fibril Cross linking
Scar Maturation
Time from injury](https://image.slidesharecdn.com/1362575848growthfactospresentationabal-151026141656-lva1-app6891/85/1362575848-growth-factos-presentation-a-bal-3-320.jpg)
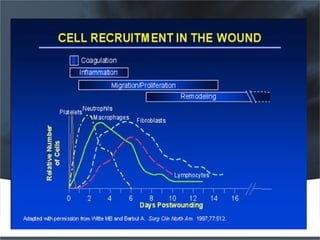




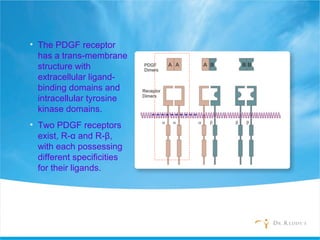
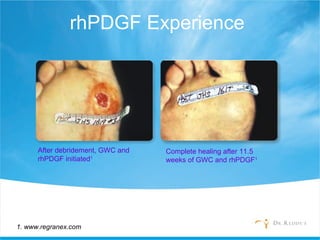
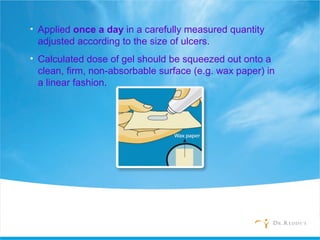
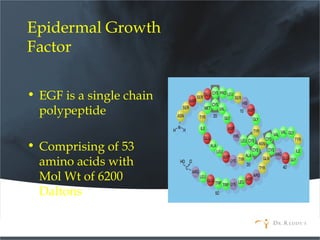
![Dose calculation
The intended dose is around 7μg /cm² of ulcer per
day for topical application.
(For an average man of around 50kg weight)
Tube Size Formula
7. 5g/15 g tube [Length (cm) X Width (cm) ÷ 4]*
*Greatest length of the ulcer multiplied with greatest width](https://image.slidesharecdn.com/1362575848growthfactospresentationabal-151026141656-lva1-app6891/85/1362575848-growth-factos-presentation-a-bal-38-320.jpg)



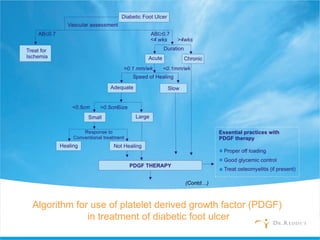
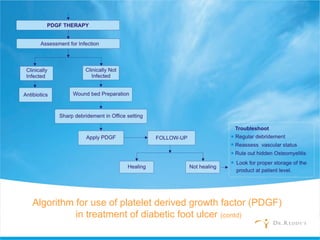
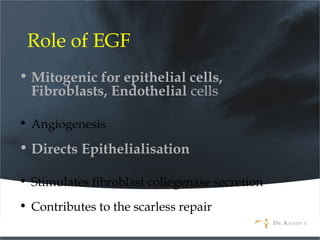


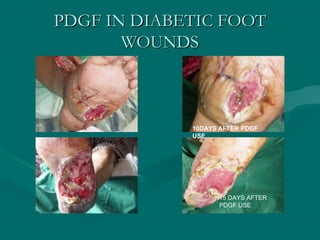



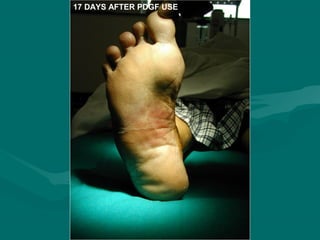





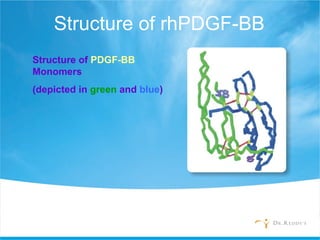
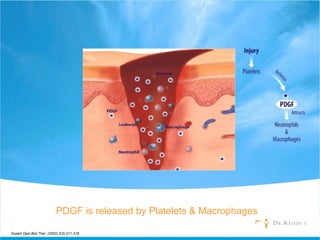
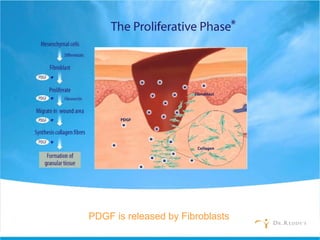
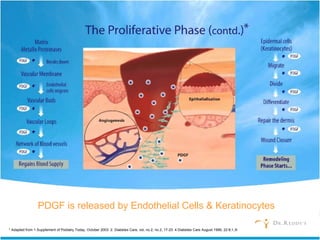
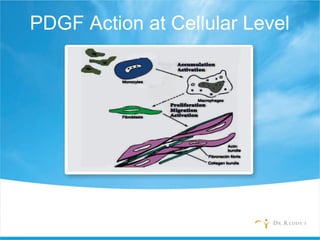
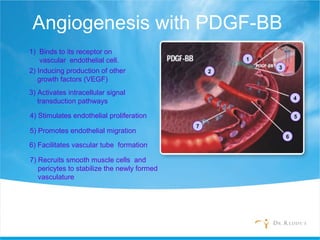
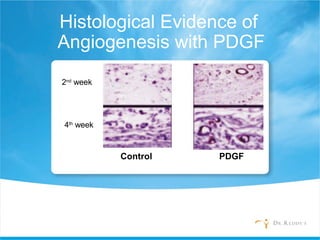
Growth factors play an essential role in diabetic foot ulcer management. Platelet-derived growth factor (PDGF) is a significant growth factor that is released during wound healing and promotes angiogenesis, fibroblast proliferation, and re-epithelialization. Recombinant human PDGF-BB (rhPDGF-BB) has been shown to accelerate wound healing in diabetic foot ulcers by stimulating cellular processes involved in repair when applied topically according to dosage guidelines.


















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

