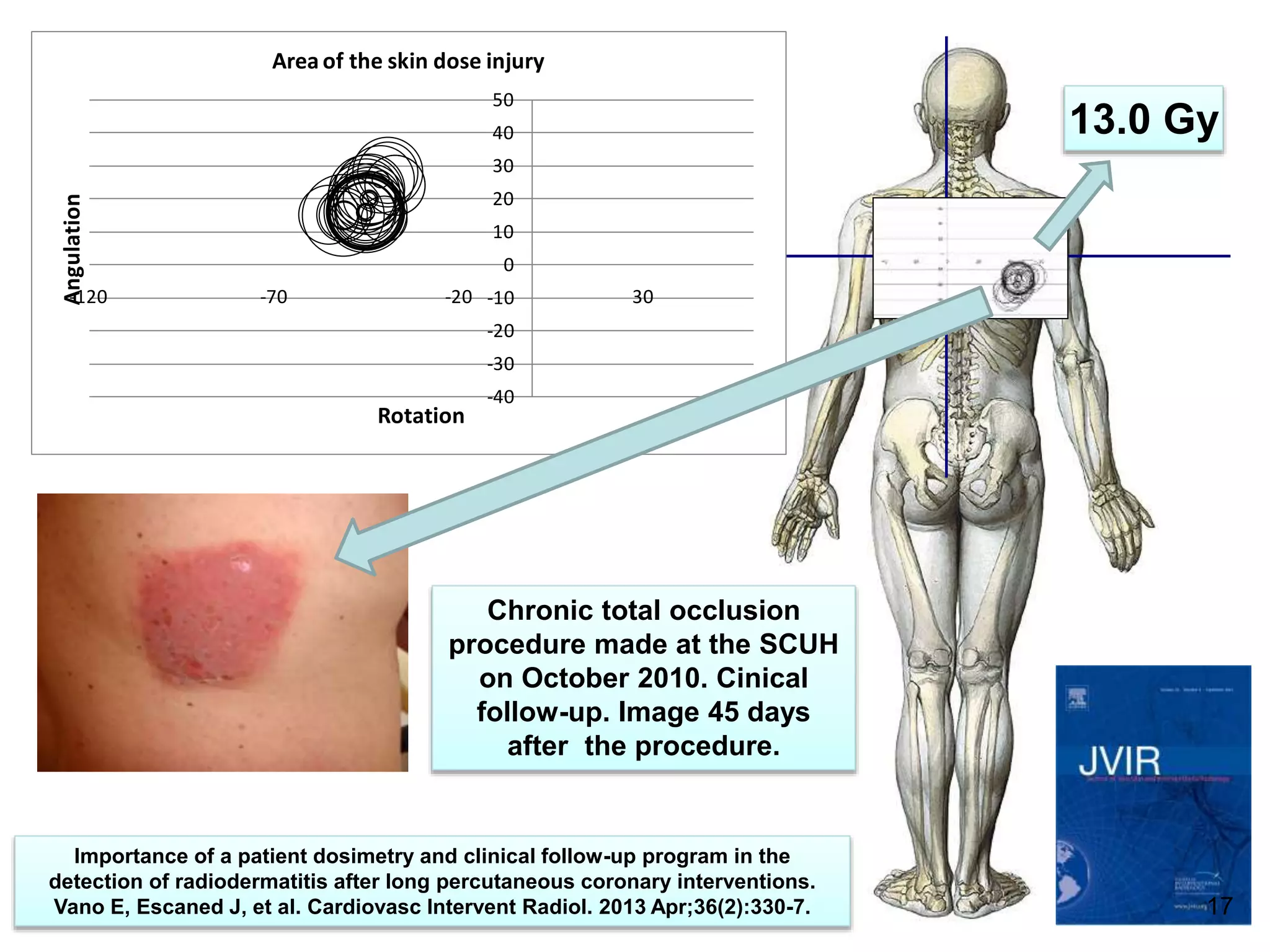
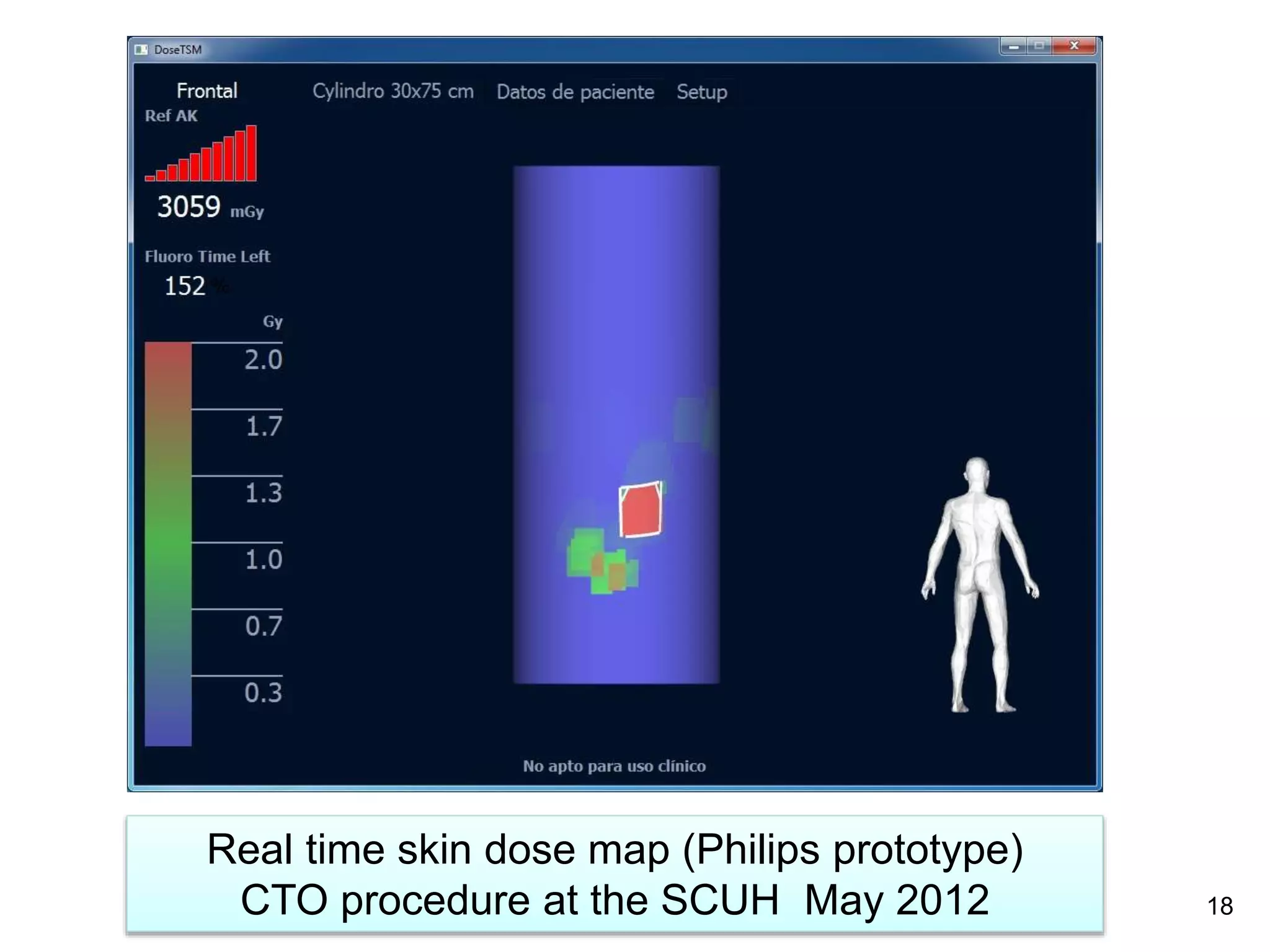
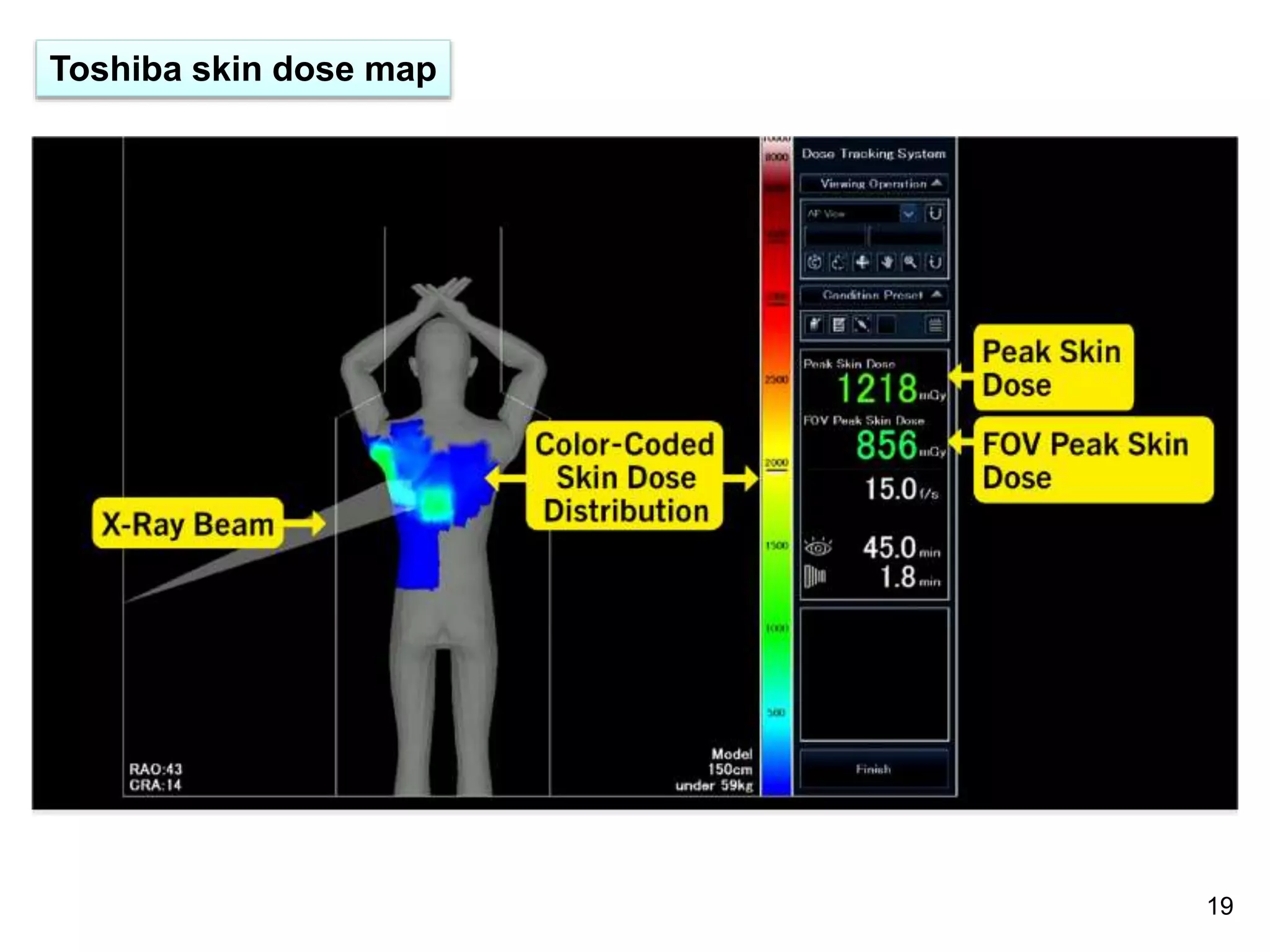
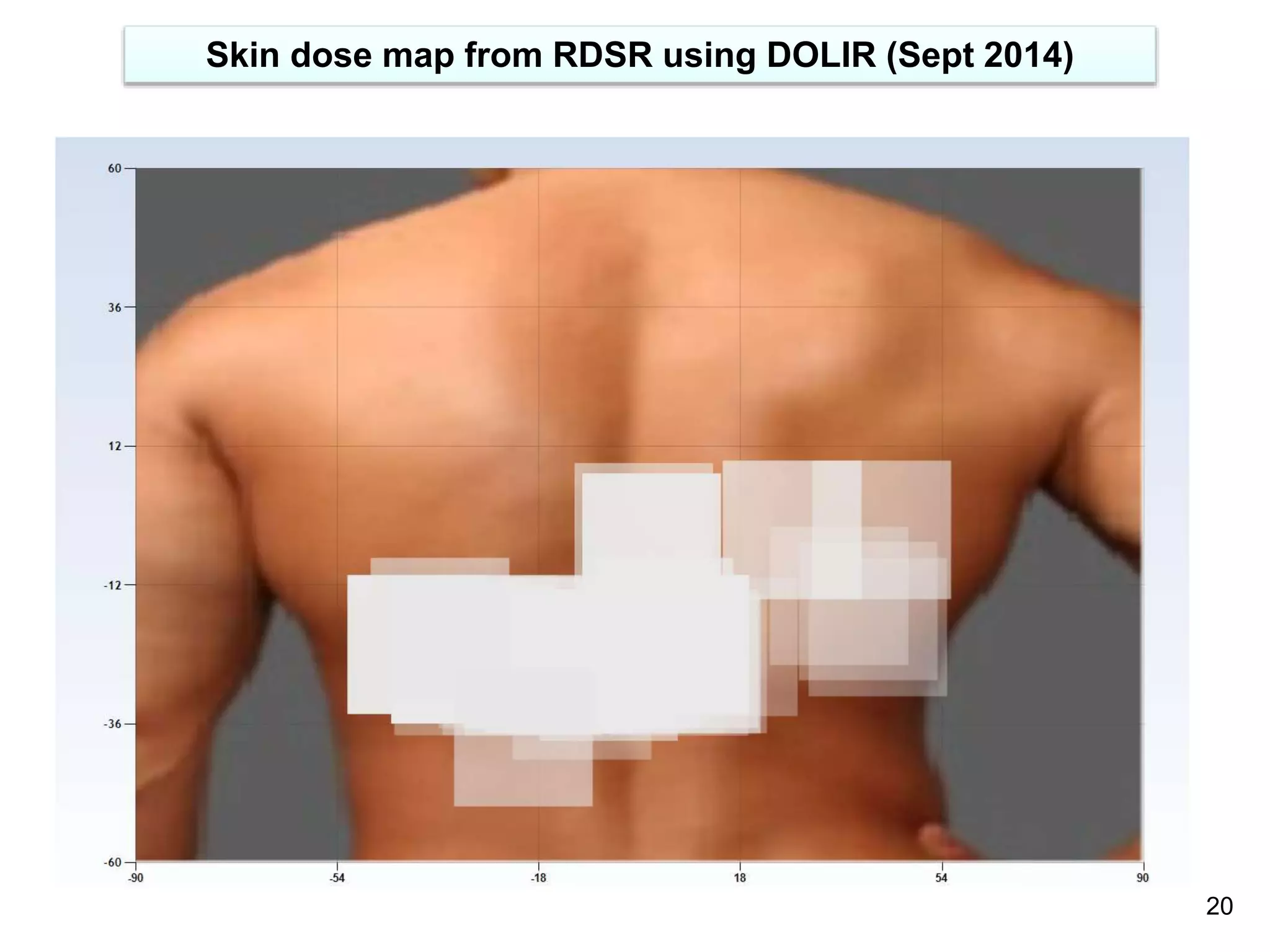
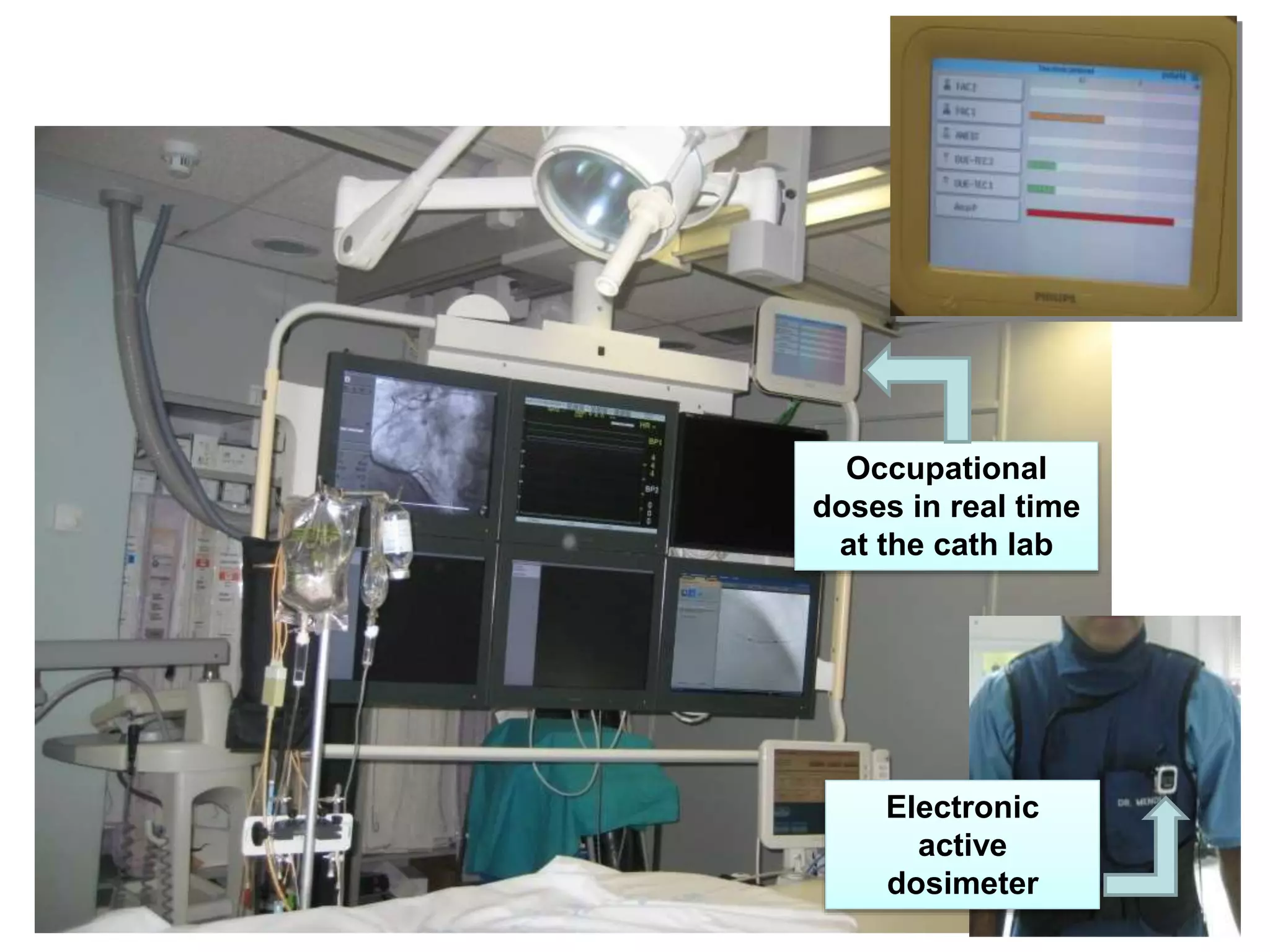
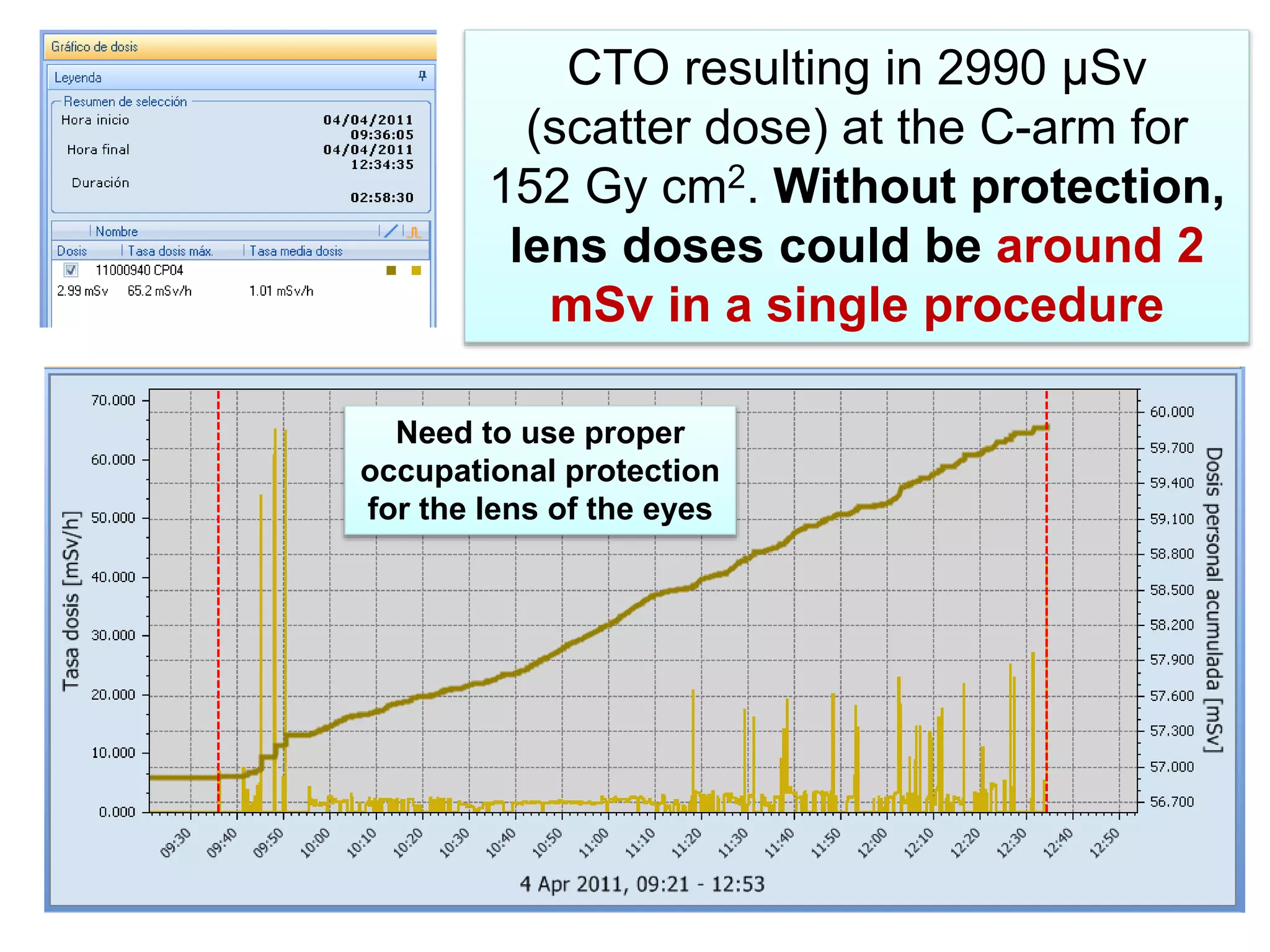
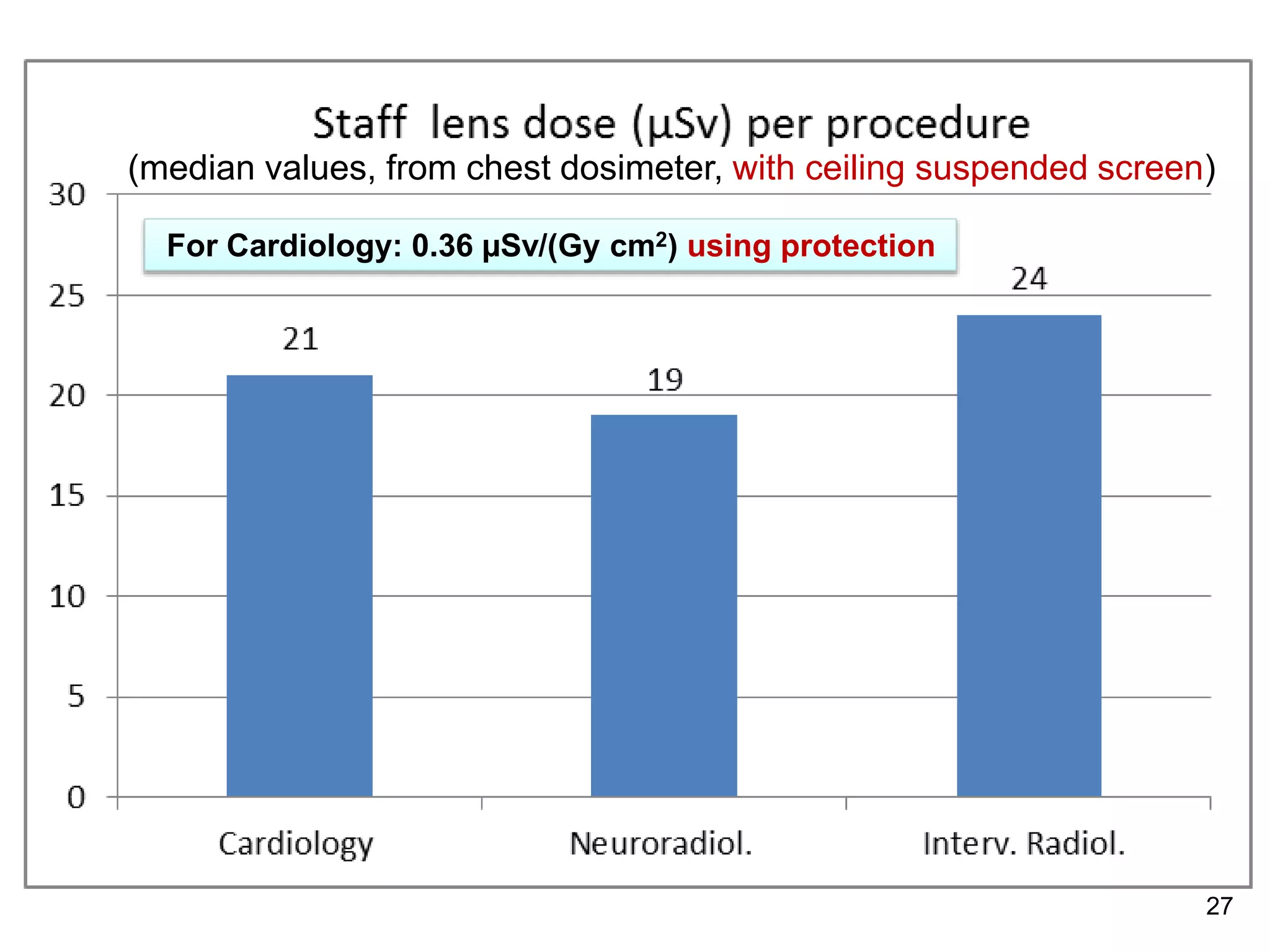
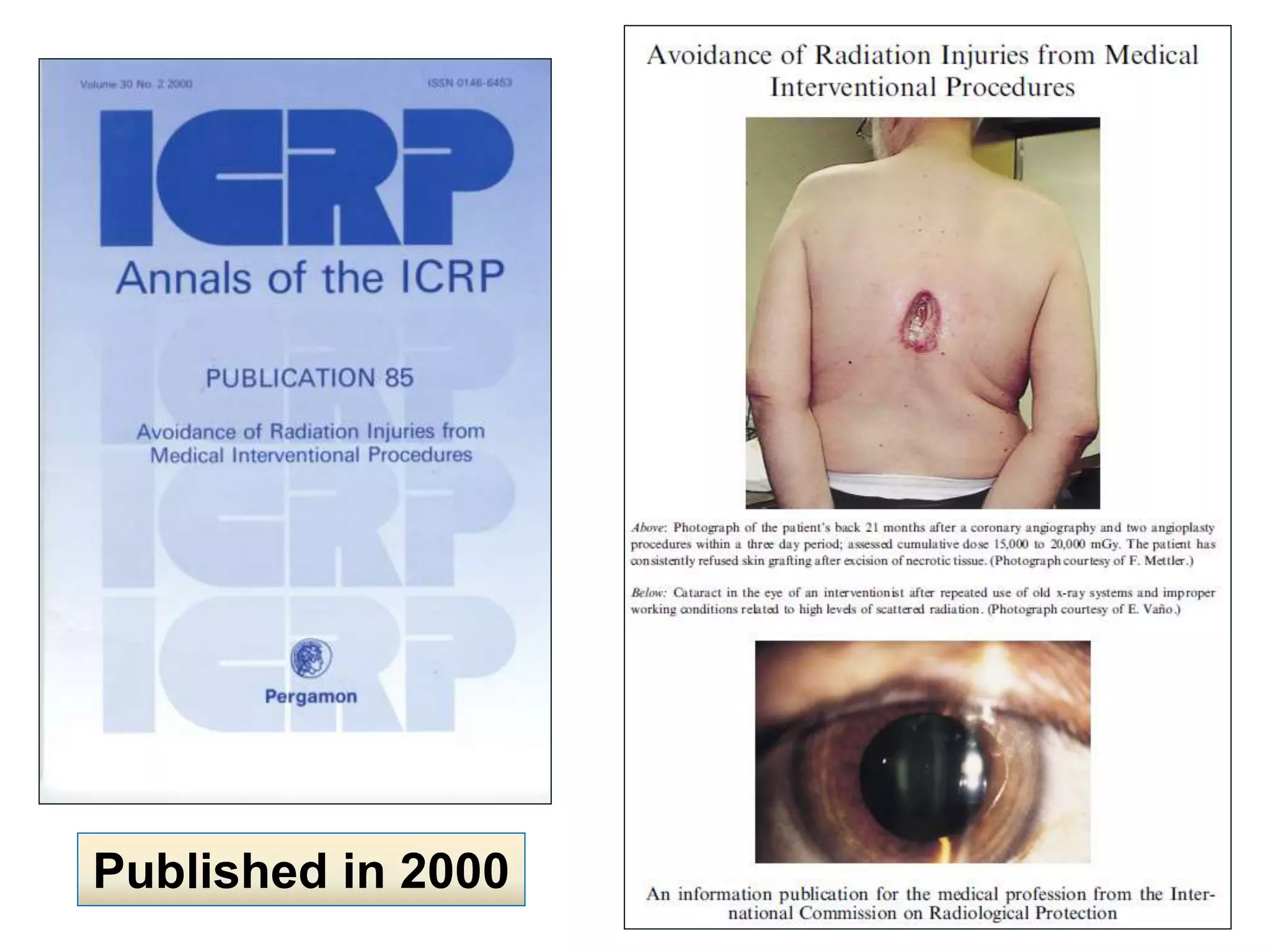
This document discusses decreasing x-ray exposure in complex coronary total occlusion (CTO) procedures. It notes that CTO procedures can result in several grays of radiation exposure to the skin of patients, increasing their risk of radiation injury. It also notes that without proper protection, interventional staff could receive milligrays of exposure per procedure to the lens of their eyes, increasing their risk of radiation-induced cataracts. The document recommends maintaining radiation doses as low as reasonably achievable for both patients and staff by following diagnostic reference levels, avoiding injuries through clinical follow-up of high dose procedures, and using protective equipment to reduce staff occupational exposures.