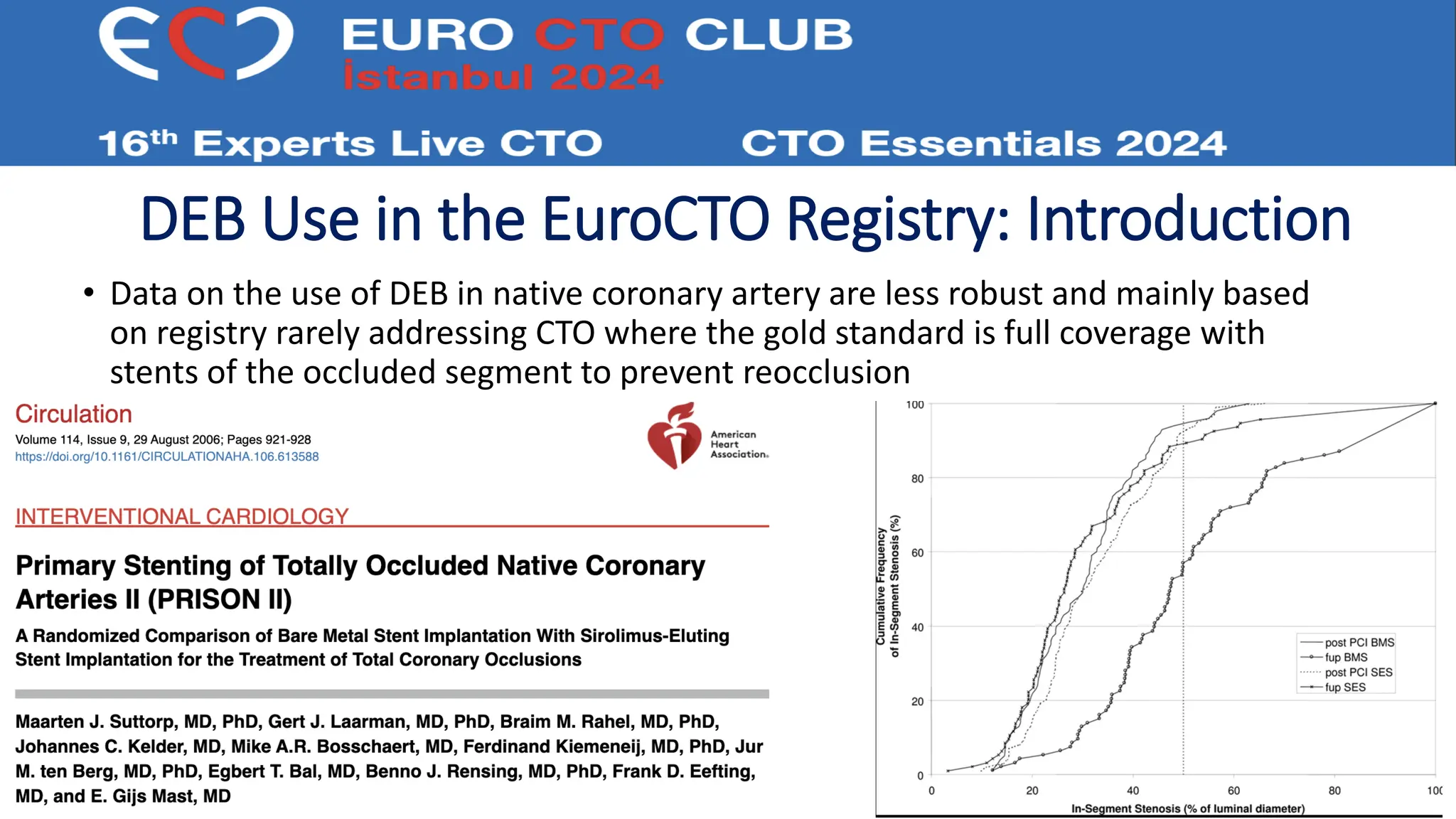
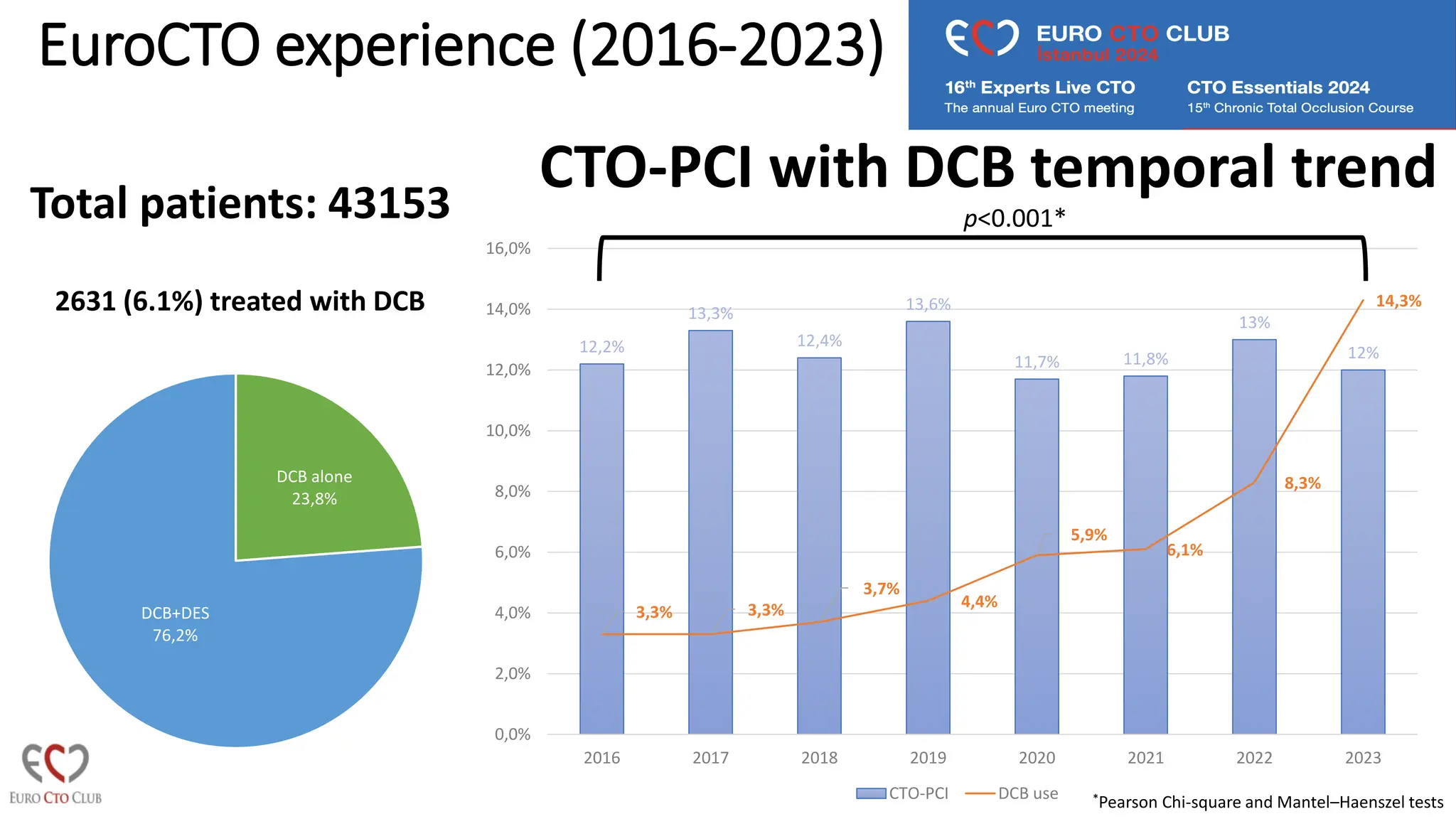
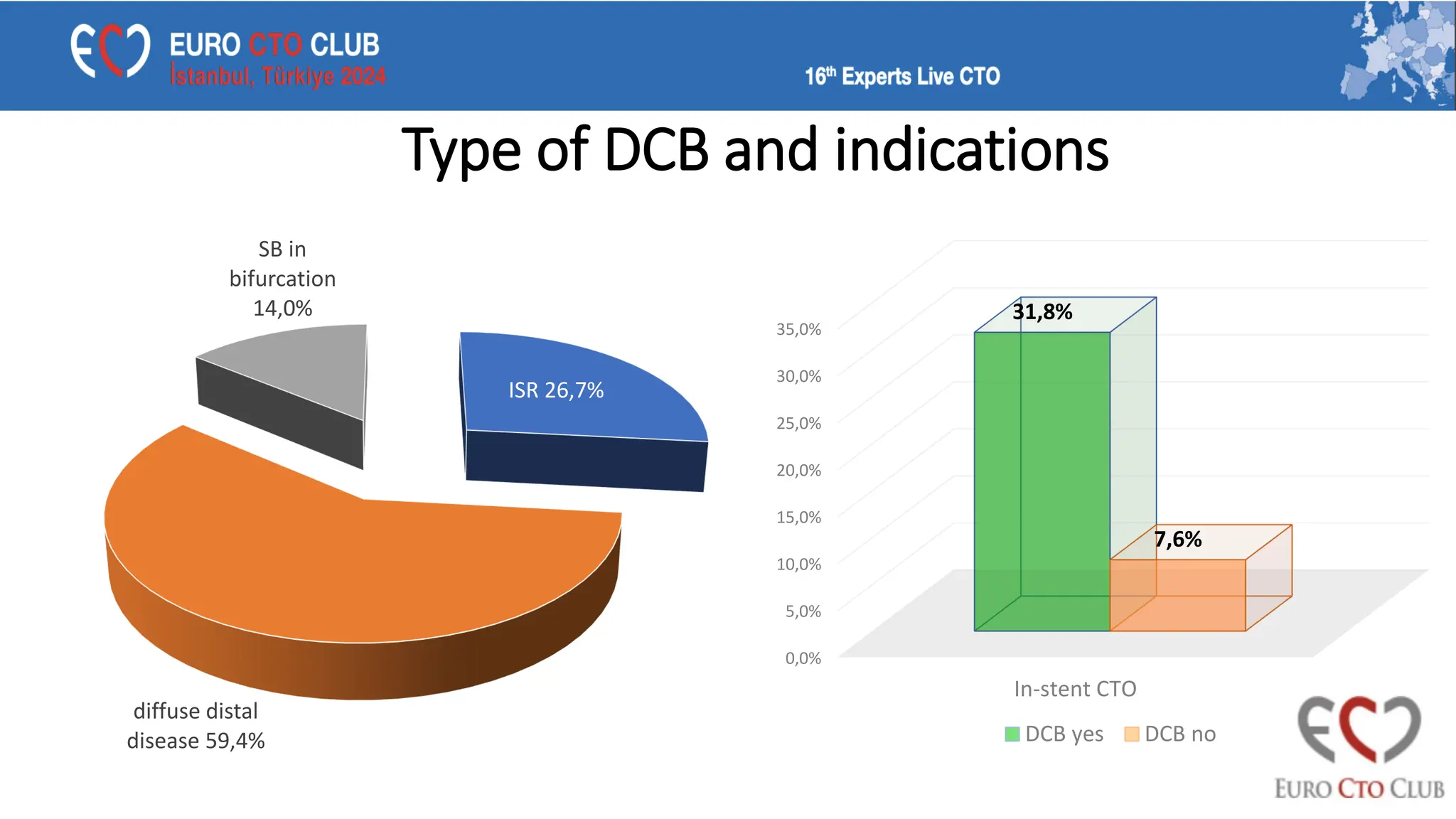
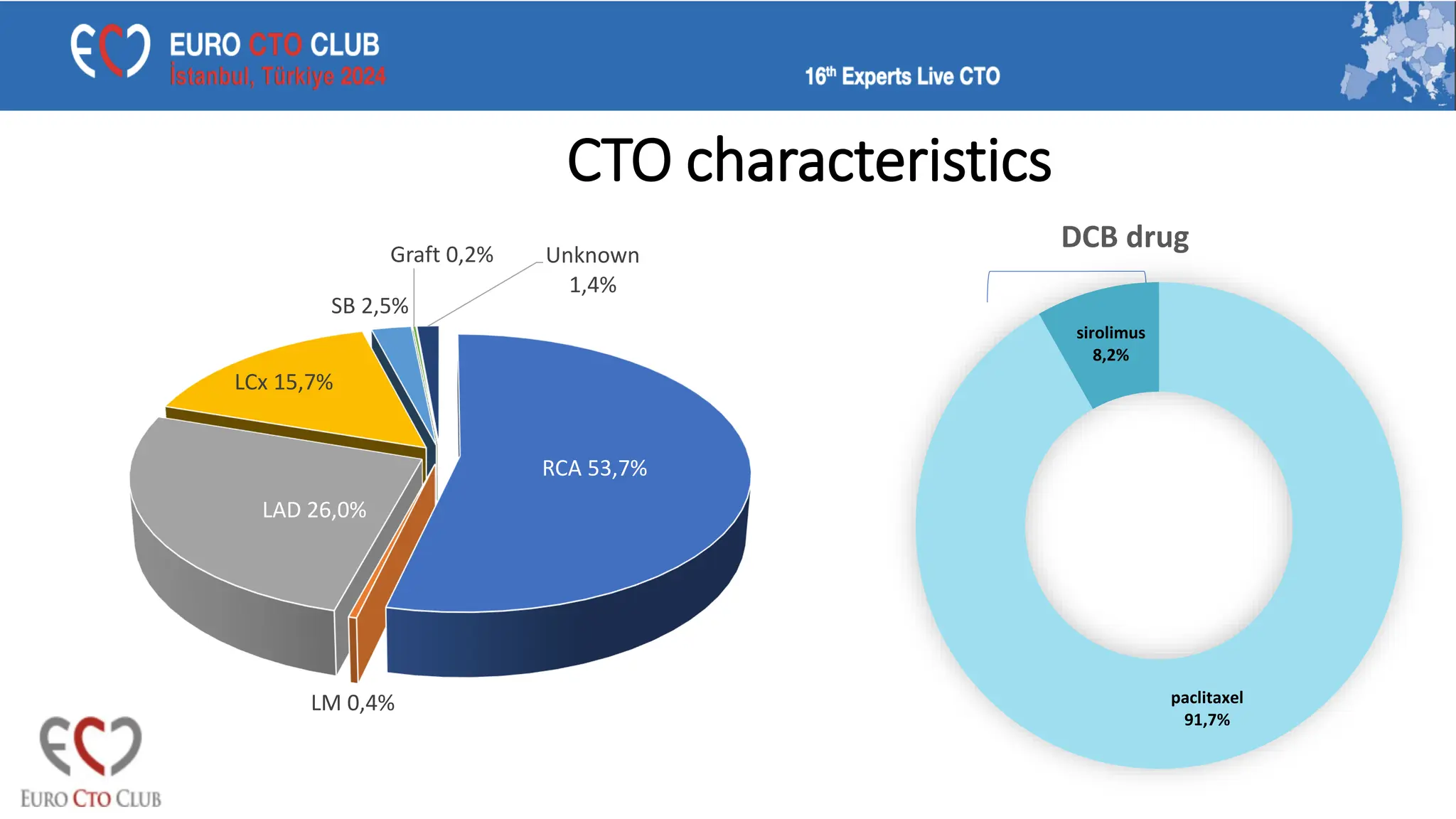
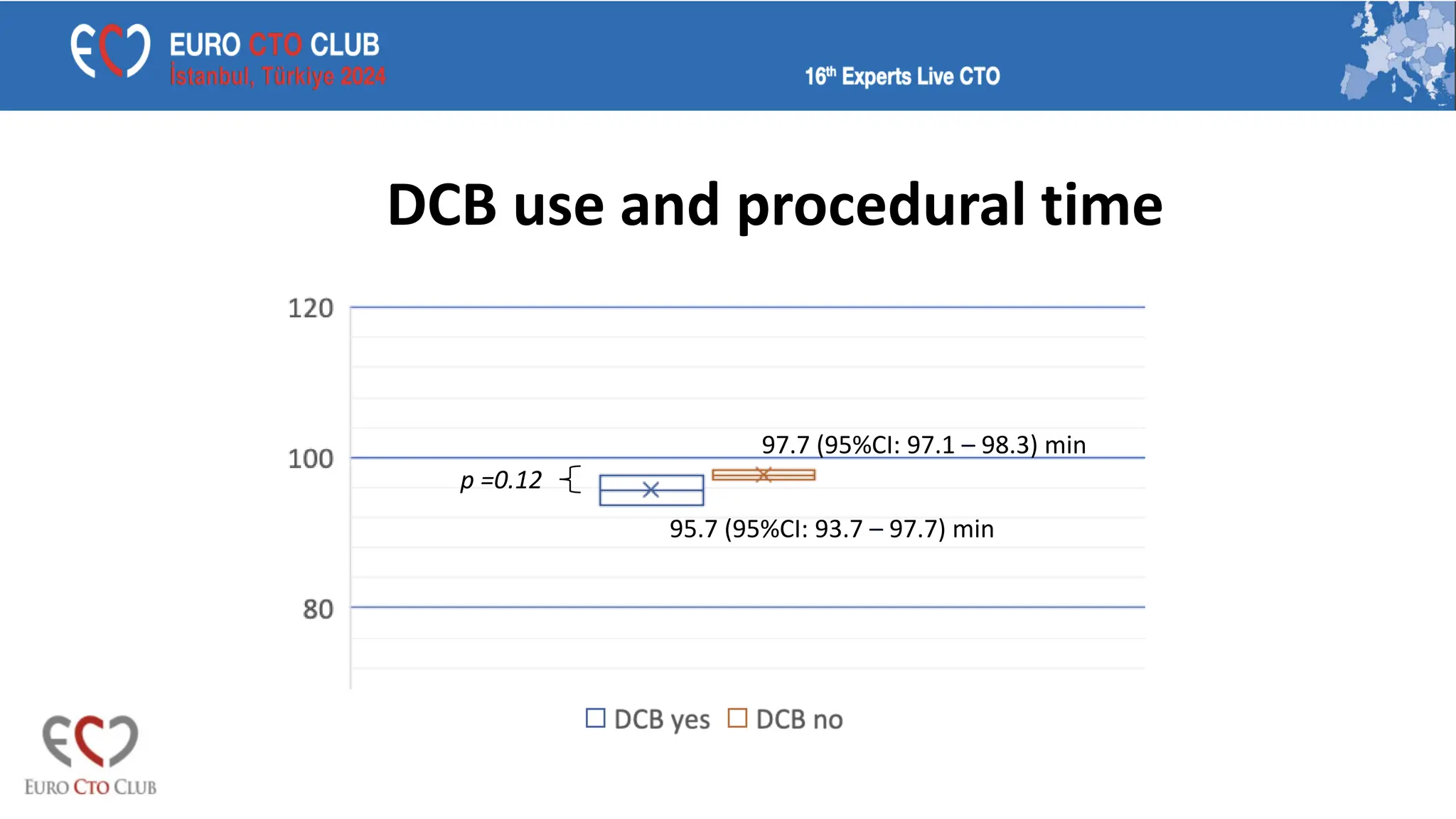
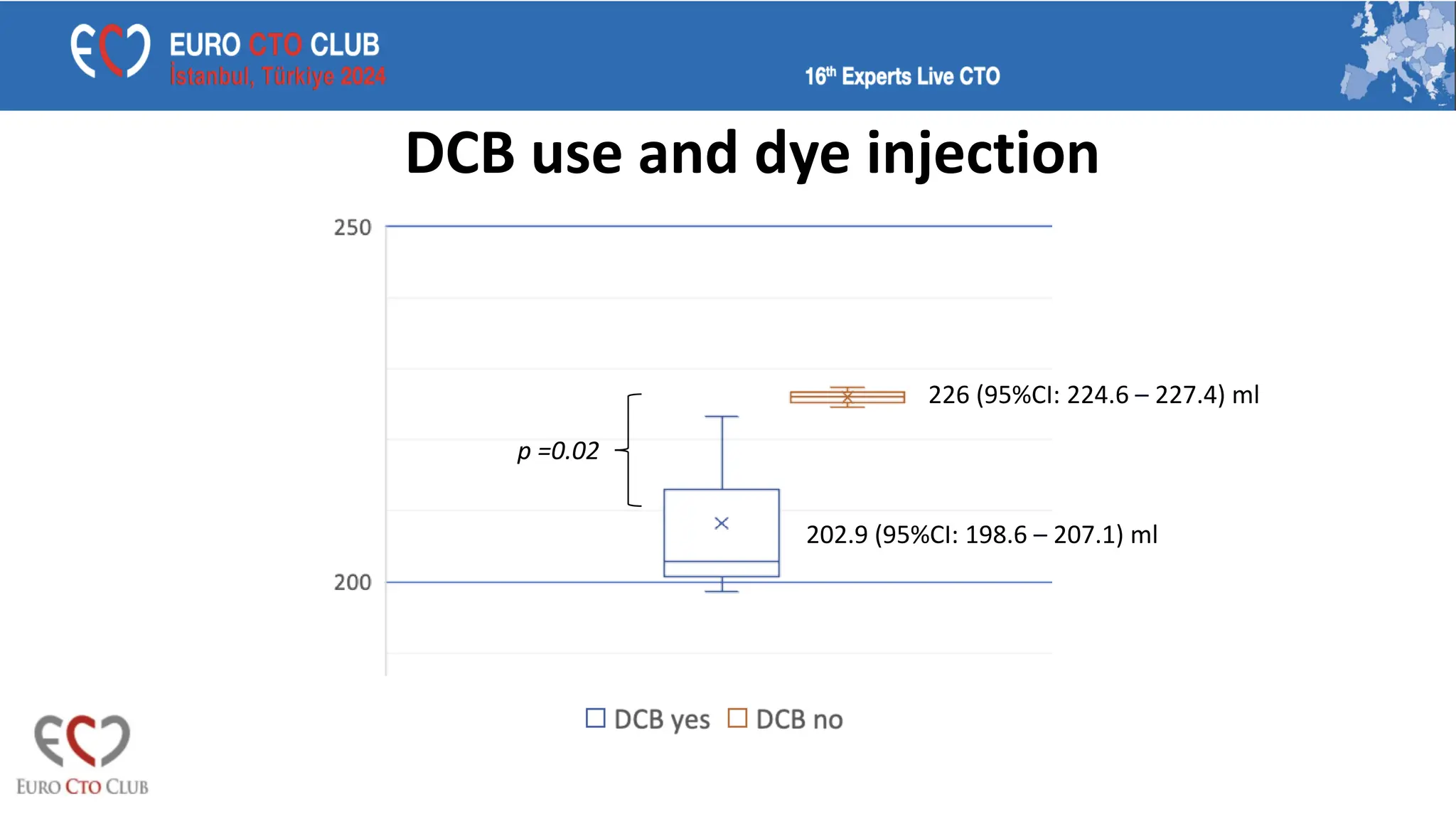
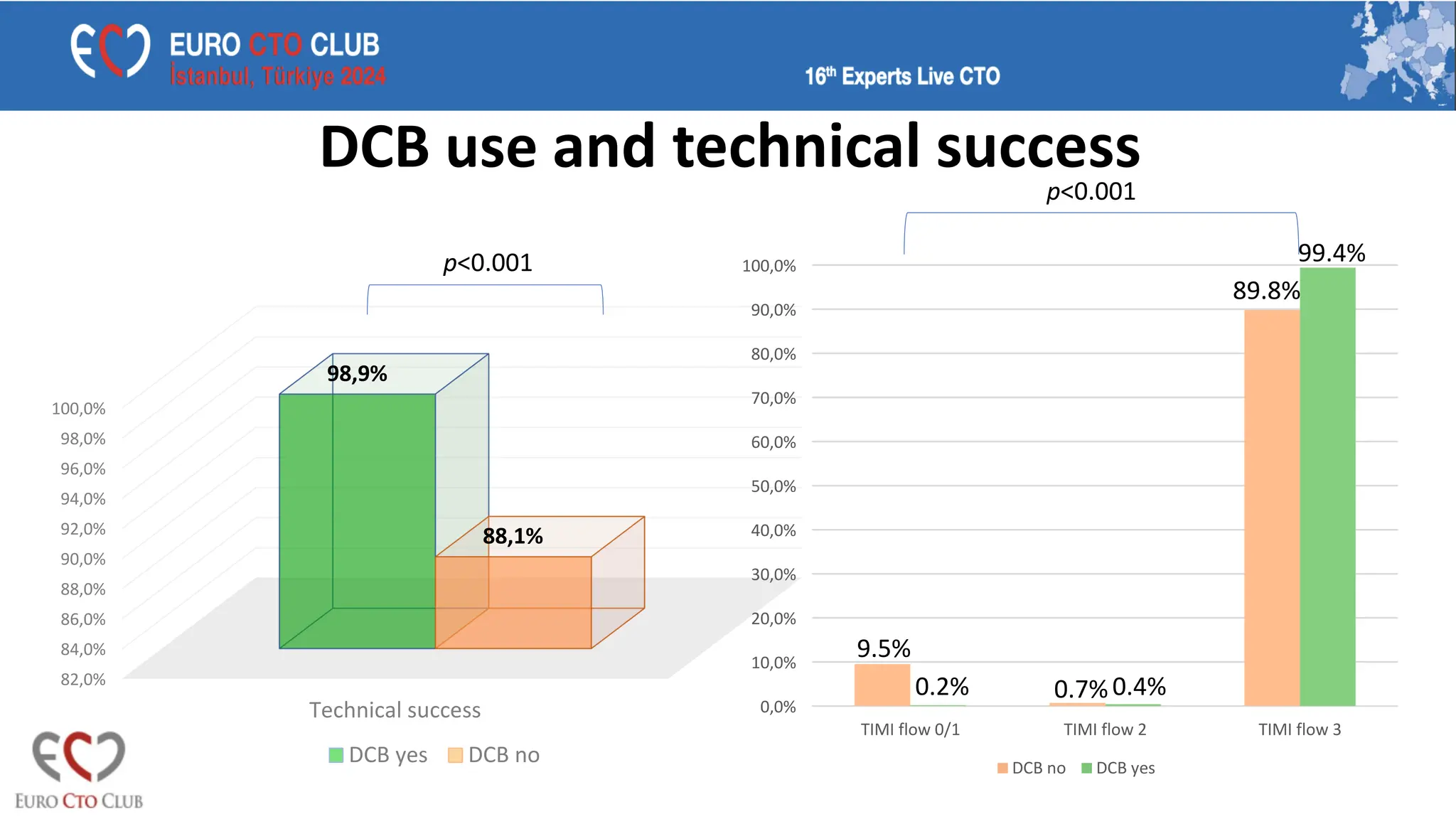
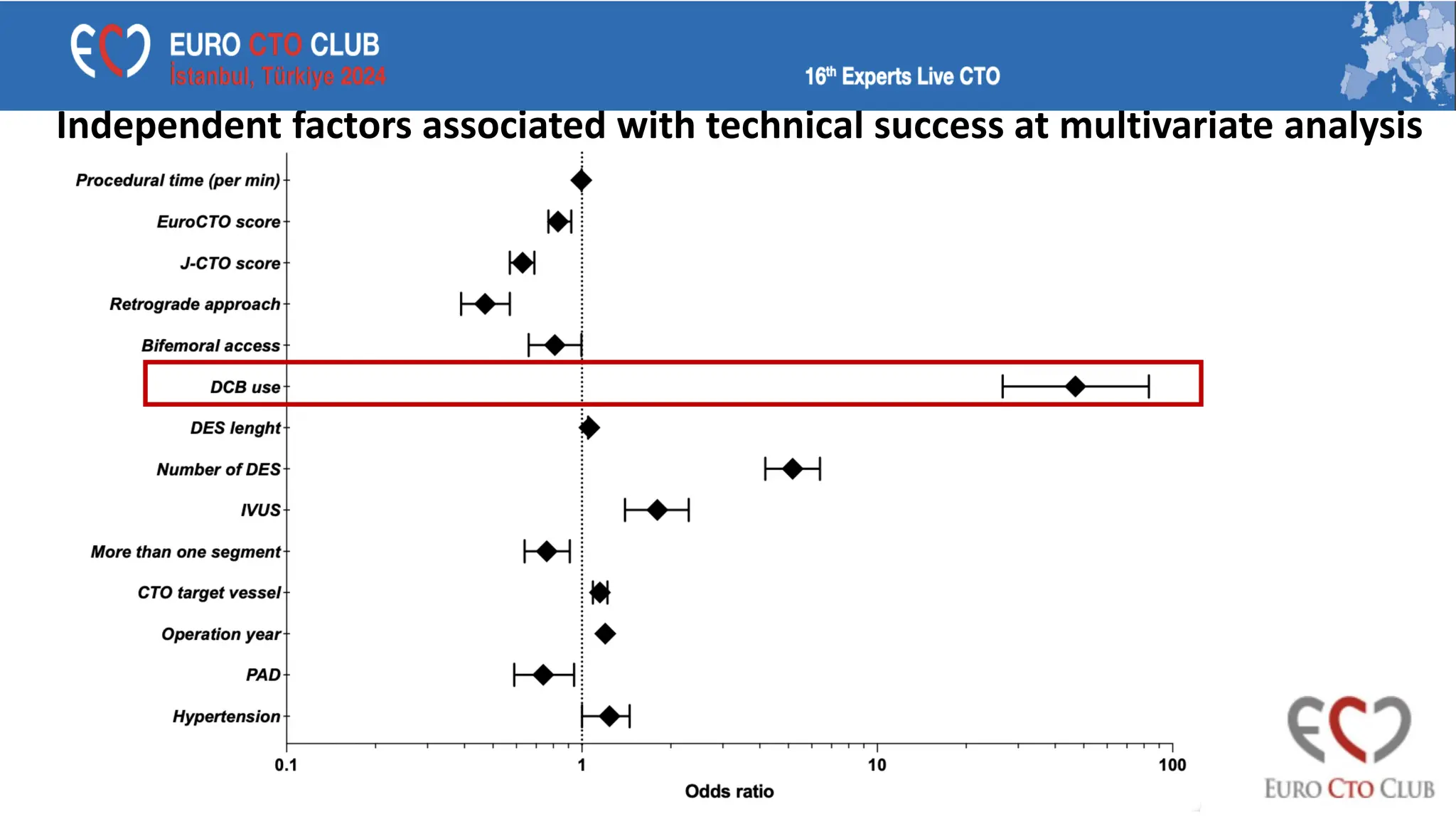
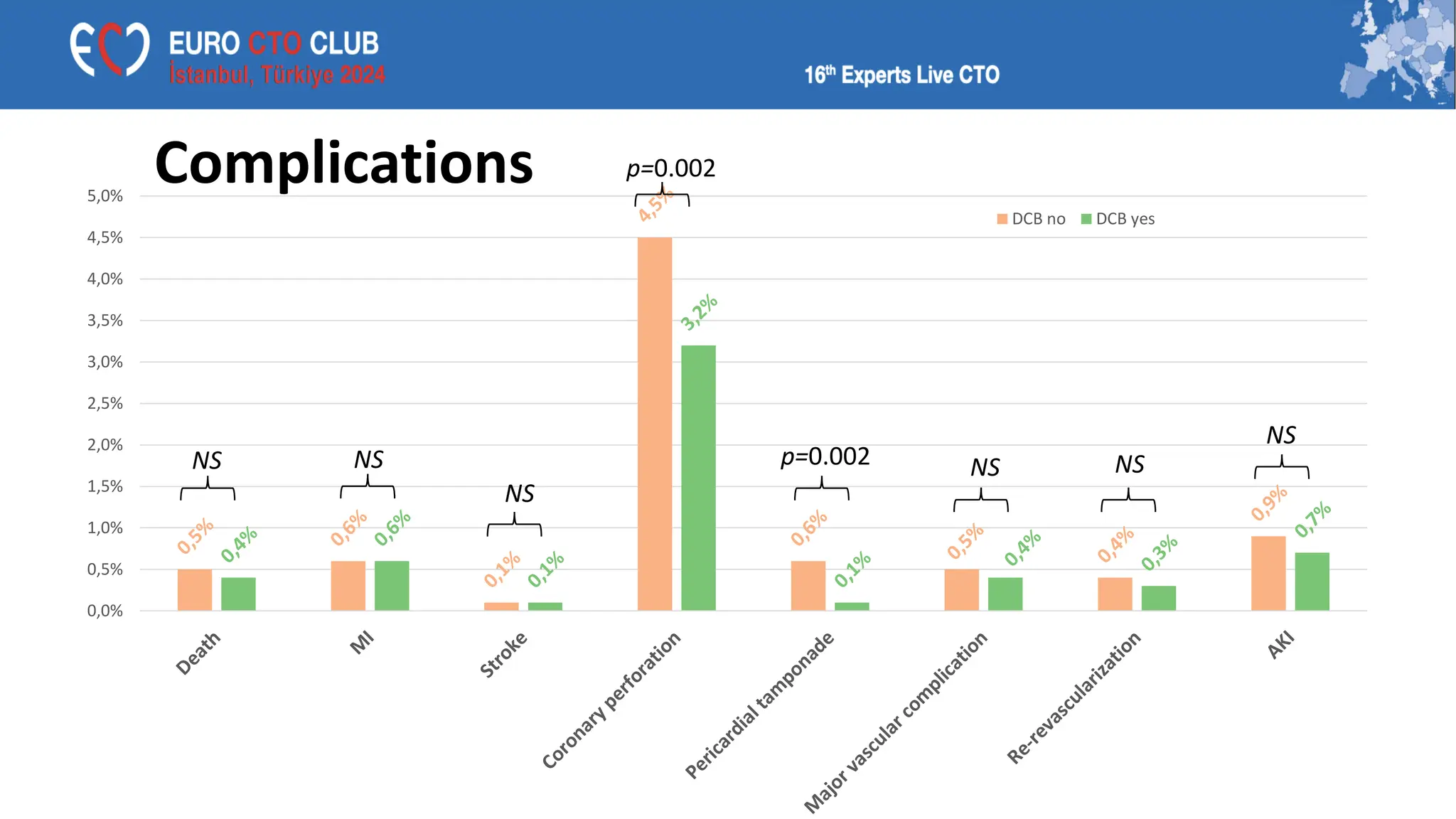
The Eurocto registry analysis covering 43,153 patients from 2016 to 2023 shows a significant increase in the use of drug-eluting balloons (DEBs), primarily for treating distal non-occlusive disease and bifurcations. The study found that DEB use leads to reduced stent lengths and contrast use, while improving technical success rates, although the long-term benefits compared to traditional stenting remain uncertain. The findings suggest DEBs are effective in specific CTO cases, particularly where avoiding over-stenting is desired.