
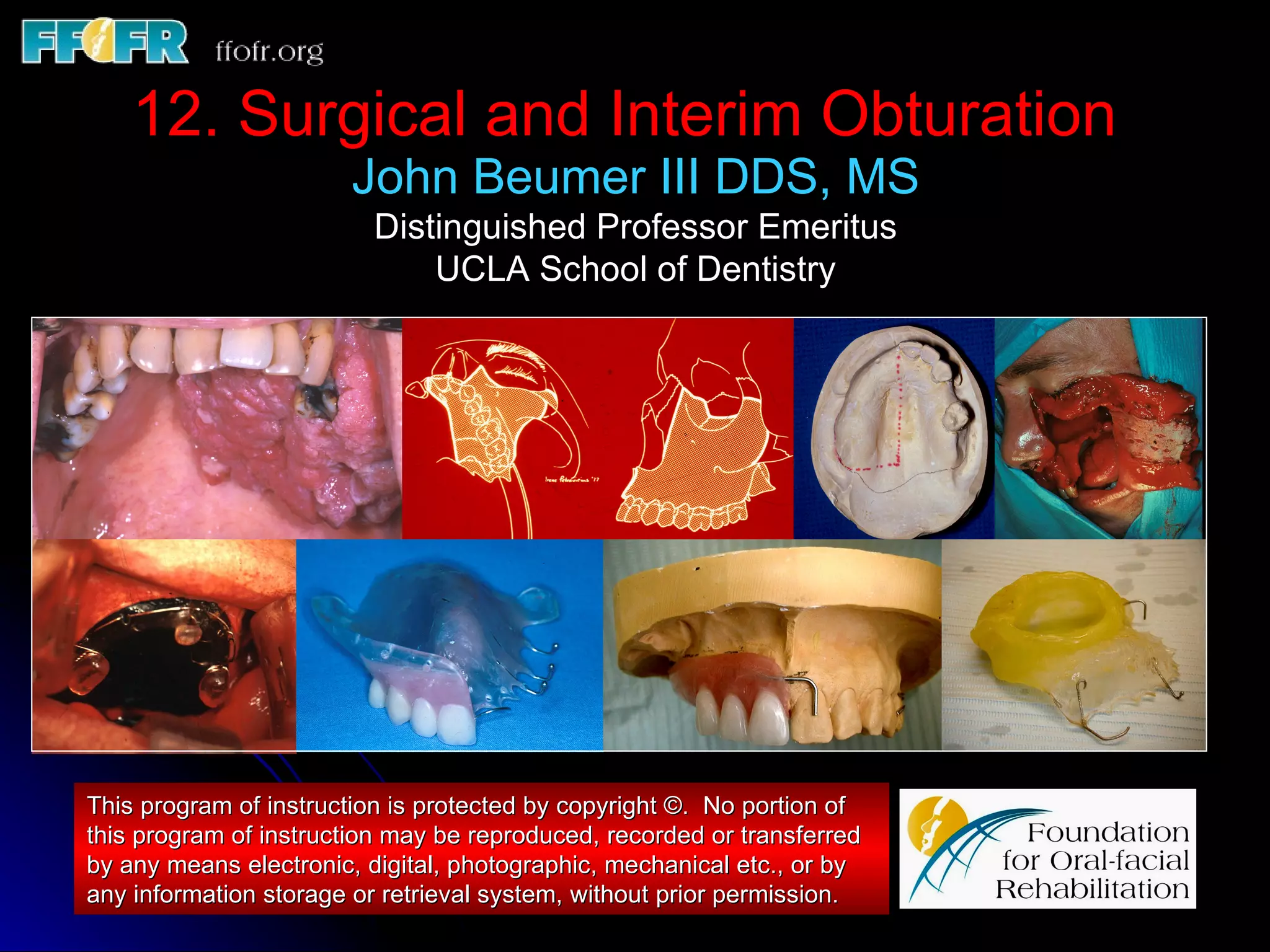
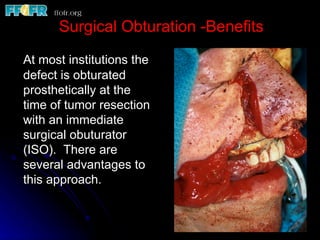
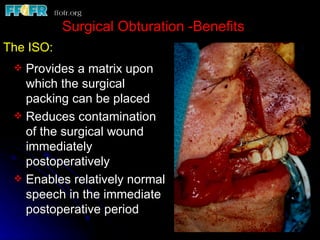
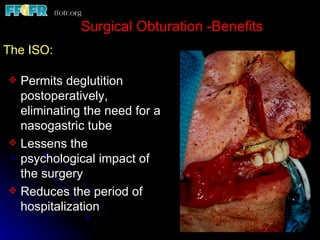
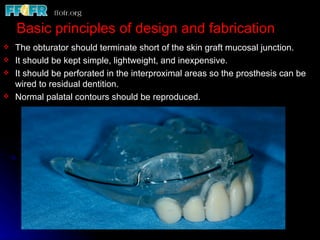
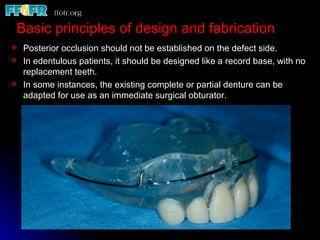

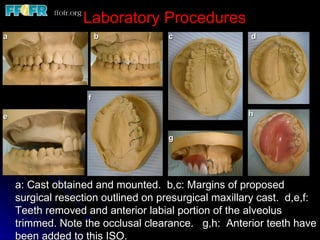
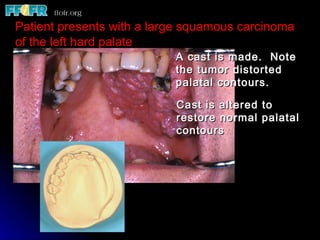
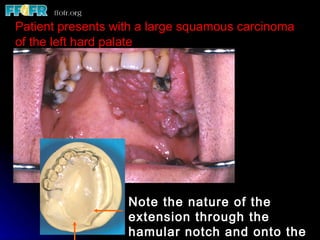
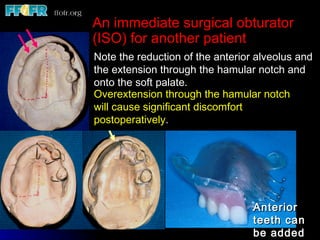
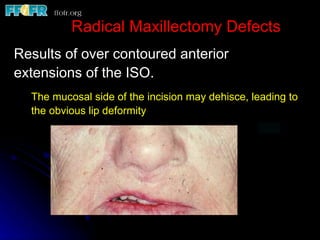

The document discusses surgical and interim obturation following maxillectomy. It describes how an immediate surgical obturator (ISO) provides benefits such as serving as a matrix for surgical packing and enabling speech and swallowing postoperatively. Principles for designing and fabricating ISO's are presented, along with examples of ISO use. Interim obturation is also discussed as a way to serve patients until wound healing is complete.






























































































