Downloaded 129 times



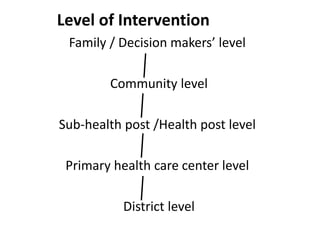

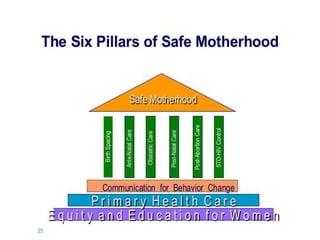




This document discusses reproductive health and safe motherhood. It defines reproductive health and outlines its key components, including family planning, antenatal care, obstetric care, postnatal care, post-abortion care, and STD/HIV control. These components form the six pillars of safe motherhood. The document also examines major reproductive health problems like maternal and gynecological morbidities. It discusses Nepal's national reproductive health strategies and approaches to addressing RH problems through an integrated health package delivered at various levels of intervention. Finally, it introduces the concept of safe motherhood and the three delays model of barriers to accessing maternal healthcare.












































![REPRODUCTIVE_HEALTH[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/reproductivehealth1-230228203244-2c7bd2f8-thumbnail.jpg?width=640&height=640&fit=bounds)

































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)