Damage to the skin or deeper tissues caused by sun, hot liquids, fire, electricity or chemicals.
Most burns happen accidentally. The degree of severity of most burns is based on the size and depth of the burn. Electrical burns, however, are more difficult to diagnose because they're capable of causing significant injury beneath the skin without showing any signs of damage on the surface.


![.
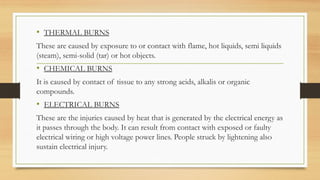
Deep second degree burns
• Injury to deeper layers of dermis, i.e., reticular dermis.
• Appears pale & mottled.
• Do not blanch to touch.
• Capillary return sluggish or absent.
• Less painful, remain painful to pinprick.
• Takes 14 to 35 days to heal by re-epithelialization from hair follicles & sweat
gland, keratinocytes often with severe scarring.
• Contractures possible.[ restriction in patients ability to move]](https://image.slidesharecdn.com/burns-250619092240-e1d524d2/85/Burns-types-and-its-management-pptx-13-320.jpg)
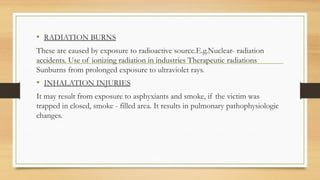
![Immediate Management
• Airway management
• Hyperbaric oxygen therapy [HBOT]
• Fluid management [ Ringer lactate and Normal saline]
• Wound management
• Analgesic and Sedation](https://image.slidesharecdn.com/burns-250619092240-e1d524d2/85/Burns-types-and-its-management-pptx-27-320.jpg)
![Burns_UPDATED34566467567544433334[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/burnsupdated1-251001060239-3786d1e6-thumbnail.jpg?width=640&height=640&fit=bounds)




![nursing management of burn wounds.. [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/burns-classnotes-250310073133-5480c852-thumbnail.jpg?width=640&height=640&fit=bounds)


































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)















