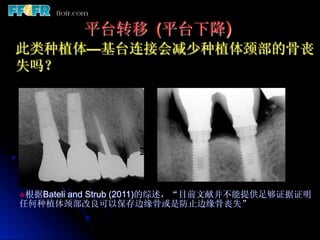
锆基台与锆支架
应用于美学区
基台
l 减少菌斑聚集
l 更美观
l 高折断率
支架
l 崩瓷高发
l 不推荐应用于后牙
Courtesy Dr. A. Sharma
68.
v Visitffofr.org forhundreds of additional lectures
on Complete Dentures, Implant Dentistry,
Removable Partial Dentures, Esthetic Dentistry
and Maxillofacial Prosthetics.
v The lectures are free.
v Our objective is to create the best and most
comprehensive online programs of instruction in
Prosthodontics