1. Acute appendicitis is an inflammation of the appendix that can range from mild to severe. It is most commonly caused by an obstruction in the appendix, often by a fecalith.
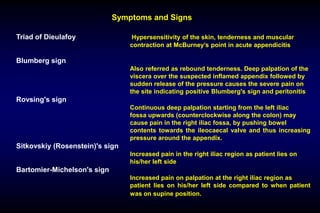
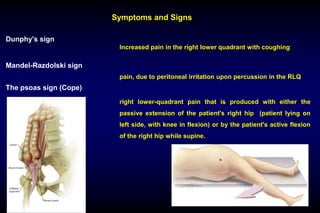
2. The symptoms of acute appendicitis include sudden onset of abdominal pain localized to the right lower quadrant, nausea, vomiting, and low-grade fever. On examination, tenderness may be found at McBurney's point.
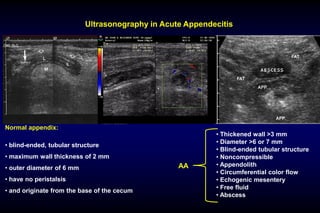
3. Diagnosis is usually made clinically but can be supported by blood tests, ultrasound, or CT scan. Treatment involves surgical removal of the appendix (appendectomy) to prevent complications like perforation and peritonitis. Differential diagnoses include other abdominal conditions presenting with similar symptoms