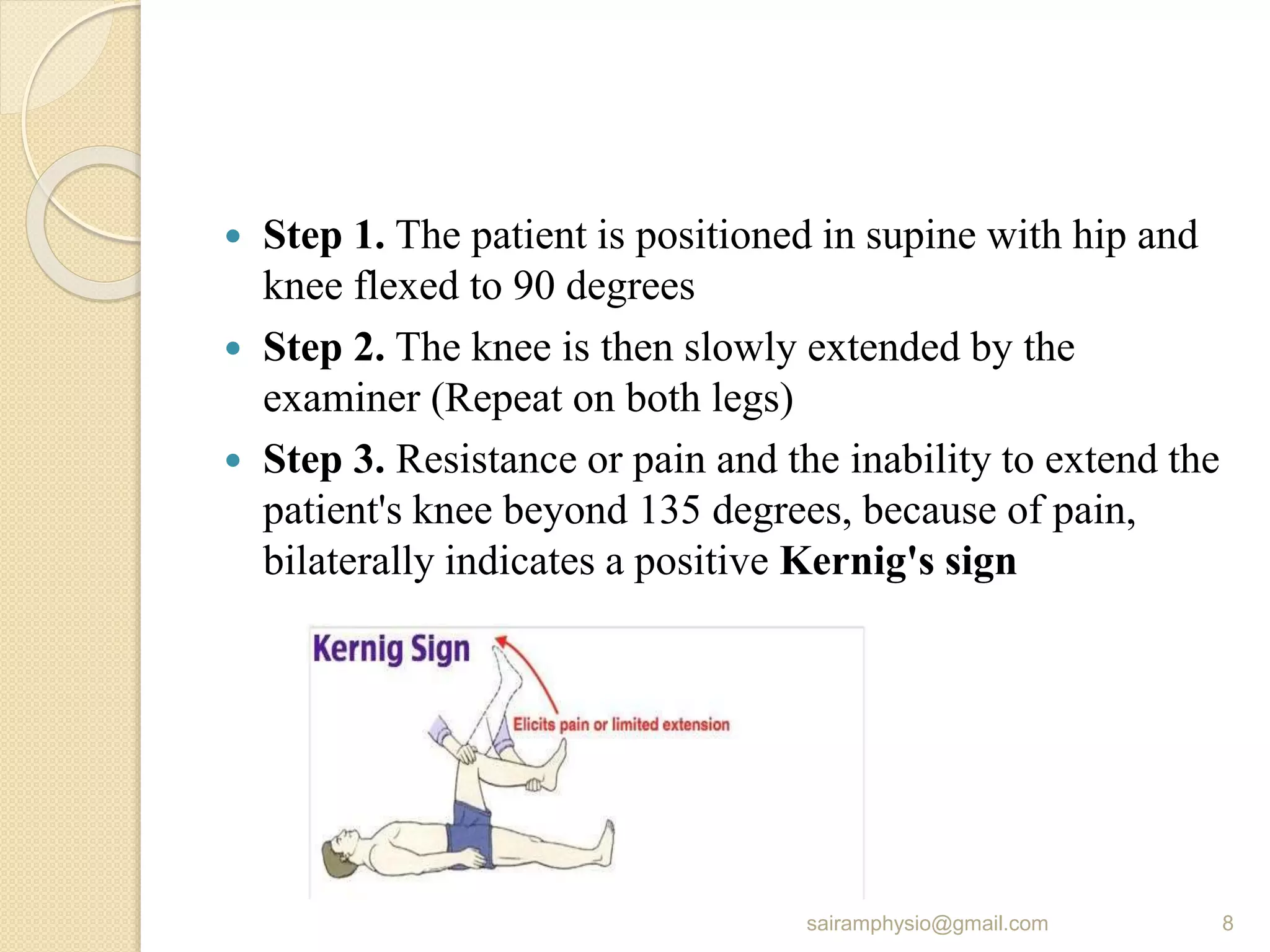
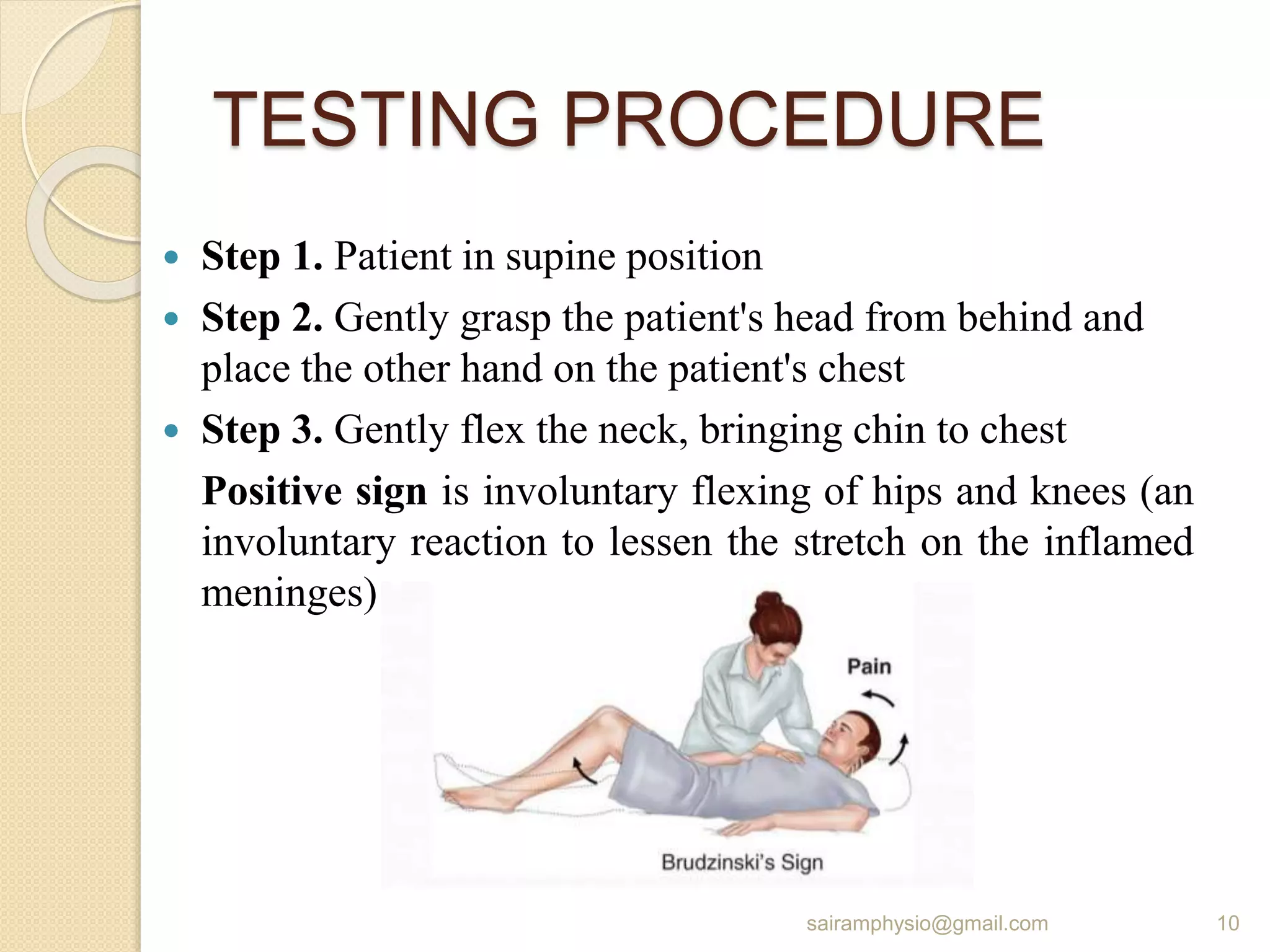
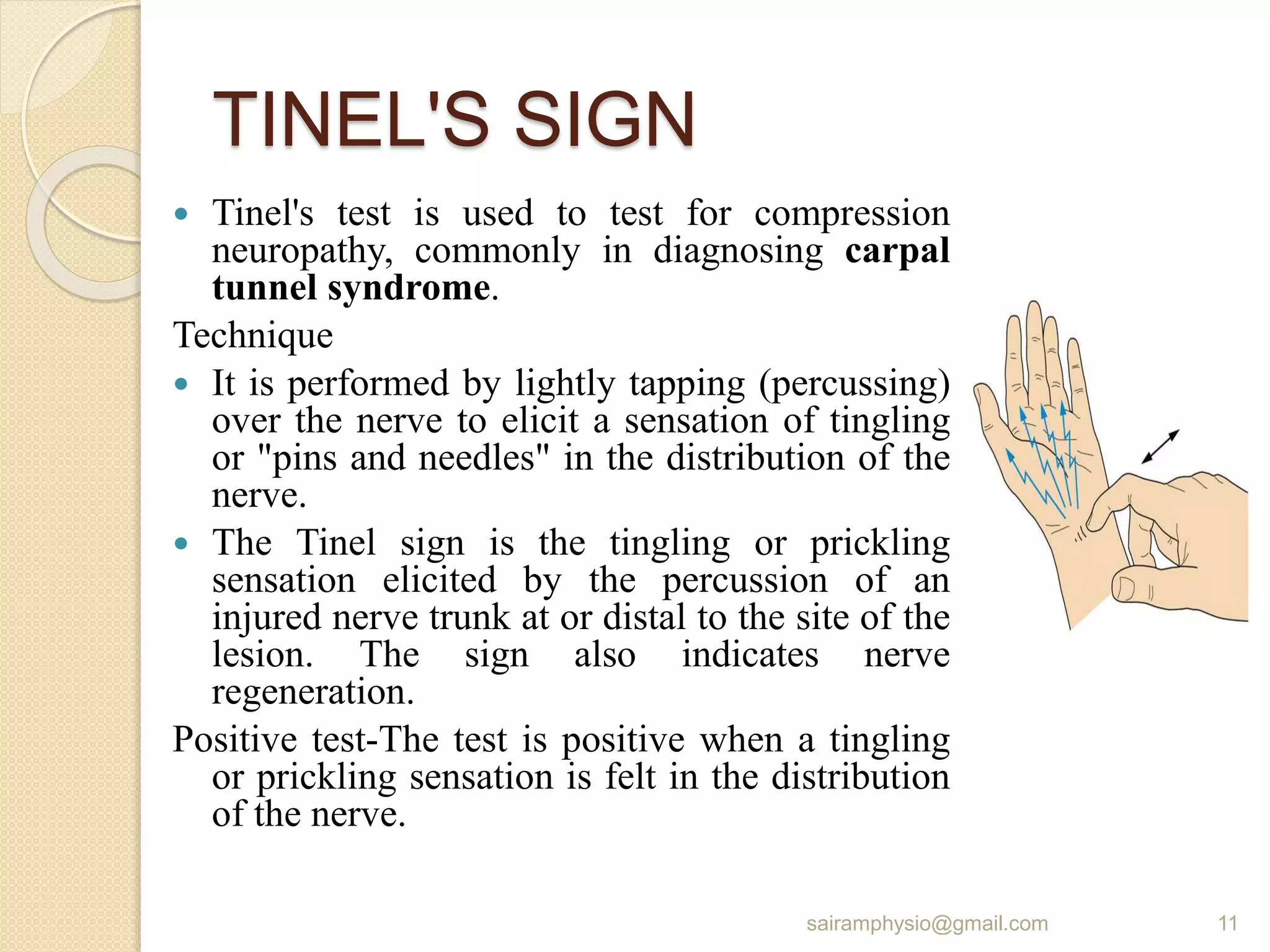
The document outlines various special tests used in clinical settings, particularly in neurology, detailing their purpose and procedures. Tests include Romberg’s test for balance, Kernig's and Brudzinski's signs for meningitis, Tinel's sign for nerve compression, and others like Gower’s sign and the sunset sign for specific conditions. Each test is described with steps for administration and interpretation of results, along with their clinical significance.















































![5._CNS_ _MSK_(1)[1].pdf central nerveous](https://cdn.slidesharecdn.com/ss_thumbnails/5-251222065741-742ca3b9-thumbnail.jpg?width=640&height=640&fit=bounds)










































