Downloaded 622 times
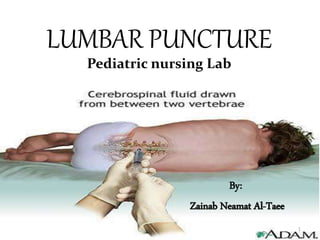
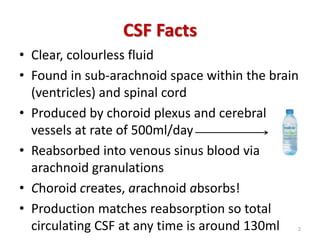

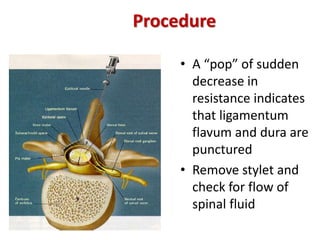

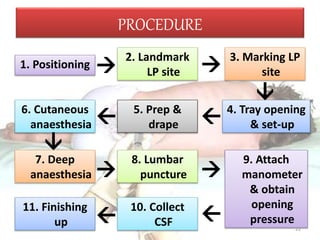
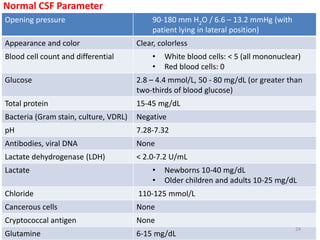
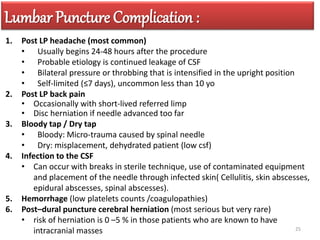
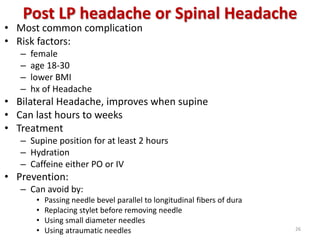


The document provides a comprehensive overview of lumbar puncture procedures in pediatric nursing, detailing indications, contraindications, equipment needed, and the steps for performing the procedure. It emphasizes the importance of patient positioning and technique to minimize complications such as post-LP headaches and infections. Additionally, the document outlines the normal parameters for cerebrospinal fluid analysis and the management of potential complications.



































































