- Ultrasound of the inferior vena cava (IVC) can help assess intravascular volume status and guide fluid management. Measuring the diameter and collapse of the IVC during respiration provides a noninvasive estimate of central venous pressure.
- A case presentation describes a cirrhotic patient with hyponatremia whose IVC ultrasound showed 100% collapse, suggesting intravascular volume depletion. Based on this the patient was given normal saline and fluid restrictions were tightened to treat their mixed hyponatremia.
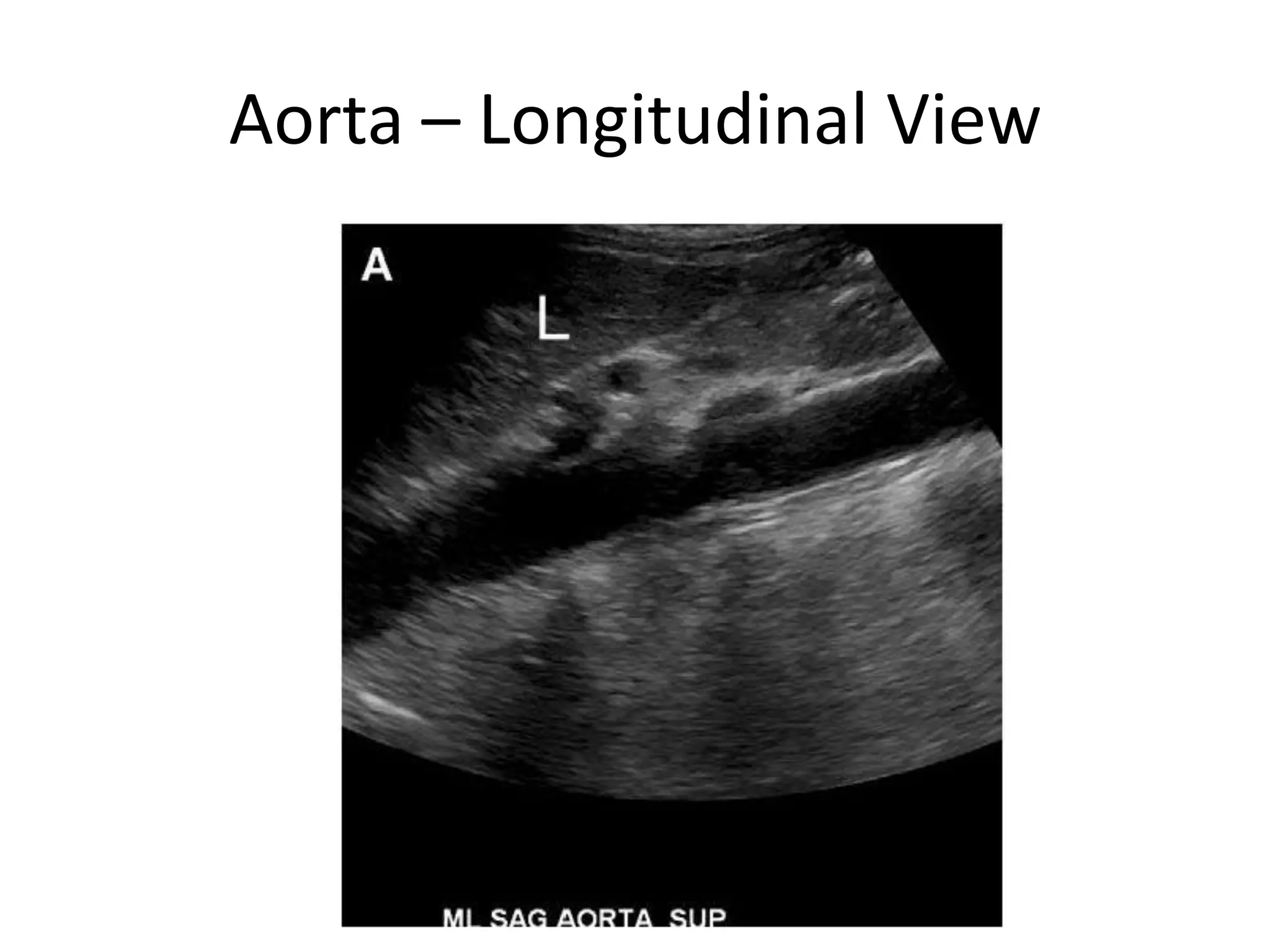
- Proper technique involves imaging the IVC longitudinally below the xiphoid process or in the mid-axillary