Ent part ii
•
0 likes•287 views

material used during final exam preparation hope benefit for all *at own risk

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Ent part ii
Similar to Ent part ii (20)
More from farranajwa
More from farranajwa (20)
Recently uploaded
Recently uploaded (20)
Ent part ii
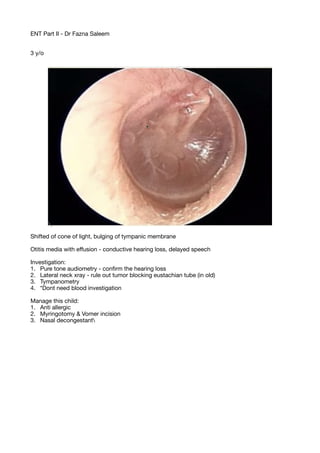
- 1. ENT Part II - Dr Fazna Saleem 3 y/o Shifted of cone of light, bulging of tympanic membrane Otitis media with e ff usion - conductive hearing loss, delayed speech Investigation: 1. Pure tone audiometry - con fi rm the hearing loss 2. Lateral neck xray - rule out tumor blocking eustachian tube (in old) 3. Tympanometry 4. *Dont need blood investigation Manage this child: 1. Anti allergic 2. Myringotomy & Vomer incision 3. Nasal decongestant
- 2. Tympanic membrane is retracted, Handle of malleus - more prominent, long process and short hand of incus Pathophysiology: Eustachian tube edema - negative pressure in middle ear Valsalva manuevre - no movement/ no changes in total perforation, movement present in TM retraction
- 3. On right side tympanogram shows curve is fl at and no value (type B) - fl uid in middle ear or tympanic membrane perforation The left side is normal tympanogram - Type A which is Normal
- 4. Elderly, chronic discharge, foul smelling Erythema, Cone of light slightly shifted, granulation tissue in (attic) pars fl accida, yellowish mass, no perforation, no pus, no discharge Most likely - CSOM Atticoantral type Cholesteatoma Management: Examination under microscope Audiometry , Pus culture and sensitivity, Mastoid xray Tx: Aural toilet, painkillers, systemic antibiotic, removal of granulation tissue by surgery (mastoidectomy)
- 5. Grommet tube / Tympanostomy tube Indication: 4. Otitis media with e ff usion 5. Retracted tympanic membrane - to allow ventilation 6.
- 6. Fever, ear pain, hearing loss Tympanic membrane shows tense and bulging, no perforation, erythematous Most likely: Acute otitis media
- 7. Cotton wool appearance Most likely: Otomycosis ( fungal infection ) CF: itchiness, irritation, discharge Investigation: Swab culture ssnsitivity, examination under microscope Mx: Aural toilet, Topical antifungal
- 9. Patient has on and o ff persistent discharge for 2 years, hearing loss Findings: Perforation of tympanic membrane on pars tensa, angle of malleus, pars fl accida is intact Dx: Inactive CSOM with tubotympanic (central perforation) Mx: Surgery (myringoplasty) - since it is inactive; no discharge, no fever
- 10. Pure tone audiometry of right ears shows air bone gap with moderate conductive hearing loss (Di ff erences should be more than 20 to be signi fi cant)
- 11. Pure tone audiometry of both ears is between 70-90, air conduction isair bone gap is present which suggest bilateral severe mix type of hearing loss of severe degree Possible causes: Conductive: Otitis media, externa, impacted ear wax, e ff usion, FB Sensorineural: labyrinthitis, ototoxicity drugs Audiometry fi ndings: 1. Conductive - bone conduction is Normal (C), air conduction is abnormal, (around 20), Positive Air bone gap 2. Sensorineural - Bone conduction is abnormal, Air conduction is abnormal, no air bone gap 3. Mix - bone conduction abnormal (below 20), air conduction is abnormal, present of air bone gap
- 12. Peak on negative zone, shows Type C tympanogram Causes: 1. Early Otitis media with e ff usion 2. Eustachian tube dysfunction
- 13. Redness/ Eythema on skin over mastoid Tenderness on mastoid bone Most likely: Acute mastoiditis Xray of mastoid bone - looking for air cells Culture and sensitvity for discharge Mx: Admit + IV Antibiotic, can change to oral antibiotic later
- 14. Face - unilateral palsy, angle mouth deviation towards left side, inable to closure of eyelids of right, nasolabial fold is less prominent on right side Most likely: Right facial nerve palsy Ear - redness, crusting, pinna vesicles Most likely: Herpes Zoster - Ramsay Hunt syndrome
- 15. Shows tympanic membrane with central perforation on pars tensa, with tympanic sclerosis (calcium sclerotic patches) Myringoplasty - graft from tragus/ subcutaneos fascia. Only repair the tympanic membrane without exploration Tympanoplasty - done in case when ossciles destroyed, atticoantral - so repair part of the middle ear with tympanic membrane repair (with exploration of middle ear)
- 16. Mass with pale, glossy appearance originate from above, no discharge, no mucus Most likely: Nasal polyp Nasal polyp vs turbinate Polyp - pale, glossy appearance Turbinate - fl eshy, originate from lateral wall Probe the mass - if painful (turbinate) Gross appearance - 2 types of nasal polyp: 1. Ethmoidal polyp 2. Anthrocoanal polyp
- 17. CT scan of Paranasal sinus - right maxillary sinus is denser (congested), left side is congested with hypoechoic area (normal - fi lled with air), hypertrophy of right turbinate Bilateral maxillary sinusitis (right side is more severe) CF: 1. Fever 2. Purulent nasal discharge 3. Headache
- 18. There is Perforated nasal septum with eryhthema surrounding peforation, no discharge Causative of perforation; 1. chronic infection like Tb 2. Sni ffi ng drugs 3. Trauma - surgical or nasal bone fracture Symptoms: 1. Whistling breathing 2. Crusting sensation 3. Epistaxis
- 19. Discoloration, erythema, swelling of left vestibule, some discharge, crusting formation Dx: Vestibulitis Mx: 1. Admit and IV antibiotic (due to Danger’s area) 2. Removal of crusting
- 20. Showing of bilateral septal hematoma (originate from medial wall) Causes: 1. Bleeding disorder 2. Nasal trauma 3. Surgery Investigation: 1. Blood coagulation pro fi le Tx: 1. Aspiration with wide bore needle or 2. Incision and drainage 3. To avoid recurrence - bilateral nasal packing + prophylactic antibiotic Complications: 1. Septal perforatio 2. Septal abscess
- 21. Xray of paranasal sinus, Waters view shows hyperdense of right maxillary sinus
- 22. History: 2 weeks of high fever, purulent nasal discharge Redness and edema around left eye Most likely dx: Periorbital cellulitis complication from Ethmoidal sinusitis Complications: Orbital cellulitis Orbital abscess Cavernous sinus thrombosis Investigation: 1. CT scan (to rule out complication and extend of diseases) 2. Naso endoscopy (to look for discharge, status of sinus, inferior meatus etc) Mx: 1. Admit and IV antibiotic 2. Monitor progress - if worsening - incision and drainage
- 23. Swelling at lower lobe of ear at angle of mandible, rounded swelling, surface is smooth, overlying skin is …, approximate size 2 by 2 cm, Di ff erential diagnosis: 1. Lymphadenopathy Investigation: 1. Full blood count 2. FNAC 3. USG of swelling - to see whether its fl uid- fi lled and rule out other diagnosis
- 24. A. Posterior Nasal Packing B. Posterior nasal bleeding due to uncontrolled htn, bleeding disorder,tumors C.
- 25. A. Saddle nose deformity B. Nasal bone fracture, trauma, nasal tumor, septal abscess C. Surgical procedure - rhinoplasty or septoplasty or septorhinoplasty
- 26. Nasal endoscopic pictures show middle meatus with purulent discharge Nasal polyp
- 27. Greyish, glistening, pale - polyp
- 28. Findings: Swelling over mandible which is size, shape, surface, skin, Most likely: Pleomorphic adenoma (swelling of parotid gland) Investigation; 1. FNAC 2. USG
- 29. Deviated Nasal Septum (bony projection) Hematoma - should be on both side
- 30. Bilateral, Sessile swelling on anterior 1/3 to posterior 2/3 junction of vocal cord Dx: Vocal cord nodules Mx: Voice rest, speech therapy Usually singer, teacher
- 31. Findings: Uvula is enlarged, tonsils is bilaterally enlarged, no exudate Grading of tonsils: 1. Grade 1 - cover the anterior pillar 2. Grade 2 - just reach the posterior pillar 3. Grade 3 - cant visualize the posterior pillar 4. Grade 4 - both of tonsils reach midline
- 32. Lateral neck xray shows Thumb sign appearance Acute epiglotitis CF: 1. Stridor 2. Drooling of saliva (severe odynophagia) 3. High fever, toxic looking 4. Sign - tripod sign (chin lifted - to increase airway) Management: 1. ABC - secure airway, secure IV line 2. Admit the patient 3. IV antibiotics with O2 supplementation No endoscopy, no tongue depression
- 33. Tonsillectomy Indications: 1. Recurrent infection of tonsil 2. Recurrent peritonsilar abscess 3. Obstructive symptoms with chronic hypertrophied tonsils Contraindications: 1. Bleeding disorder 2. Active infection on going Complications 1. Injury to other structures (tooth, oropharyngeal) 2. Aspiration 3. Hemorrhage Late complications: Secondary bleeding, infarction Check for Hb, coagulation pro fi le
- 34. Findings: Oropharynx wall - edematous vesicular lesion, cobblestone appearance Diagnosis: Chronic pharyngitis Features: 1. Uneasiness of throat 2. Foreign body sensation Management: Antiseptic gargling Cauterisation - to remove hypertophy (in very severe cases)
- 35. 1. Tracheostomy 2. Indication: Epiglotitis, laryngeal edema, prolong intubation, laryngeal tumors, laryngomalacia, retained secretion in lung, spinal trauma, bulbar palsy, respiratory insu ffi ciency, fi brosis, chronic lung diseases 3. 4 complications: Injury to RLN, hemorrhage, injury to thyroid, subcutaneous emphysema (very common), apnoea (less CO2 to drive for respiration- which lead to paradoxical apnoea) 4. Post operative management and care - make sure no bleeding, daily dressing, supply with oxygen, regular suction
- 36. Left side of soft palate is swollen, uvula shifted to right Diagnosis: Peritonsilar abscess (Quinsy) Causes; 1. Recurrent tonsillitis 2. Foreign body throat Management: 1. Admit 2. Analgesics 3. Incision and drainage
- 37. Single, Unilateral, Pedunculated swelling on anterior 1/3 of right vocal cord Dx: Vocal cord polyp Symptoms; 1. Diplophonia 2. Hoarseness of voice 3. Dysphonia 4. Stridor 5. Obstructive symptoms Treatment: 1. Mainstay - surgery (microlaryngeal surgery with poypectomy)
- 38. Nasopharynx shows edematous lesion with bleeding, shiny and bulging appearance which arise from fossa of Rosenmüller Dx: Nasopharyngeal carcinoma Symptoms: Early 1. Unexplained epistaxis 2. Unexplained lymph node swelling 3. Commonest cranial nerve involvement (abducens nerve - lateral rectus palsy - medial squint) Late presentation 1. Naso obstruction (late presentation, when mass is big) 2. Hearing loss Treatment: 1. Radiotherapy and chemotherapy