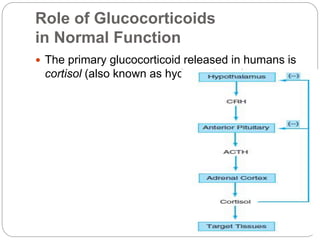
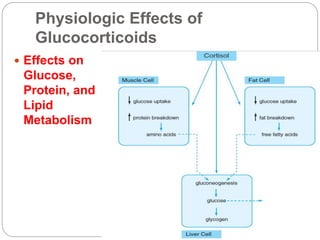
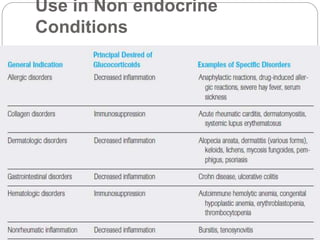
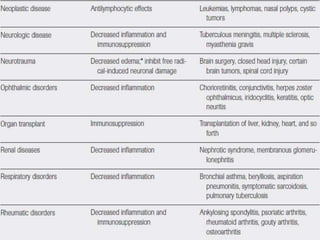
This document discusses adrenocorticosteroids and their roles and effects in the body. It focuses on glucocorticoids like cortisol which regulate glucose, stress response, and inflammation. Glucocorticoids work by entering cells and activating receptors that travel to DNA to inhibit inflammatory genes. The document also discusses mineralocorticoids like aldosterone which regulate sodium and fluid balance. Therapeutic uses of glucocorticoids include replacement therapy for adrenal insufficiency and treatment of inflammatory/autoimmune conditions. Side effects include adrenal suppression and Cushing's syndrome.