
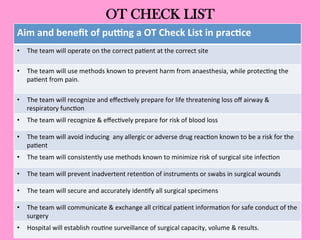
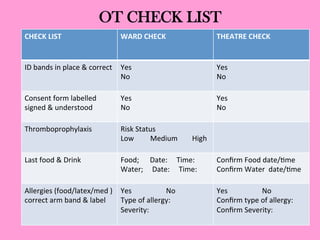


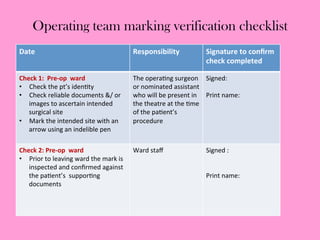
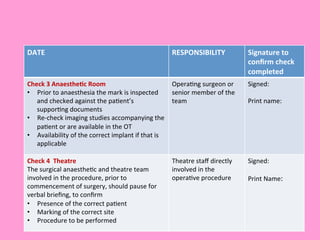
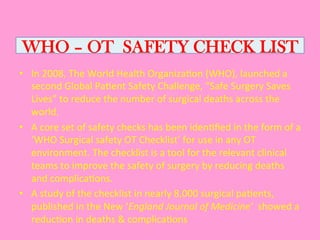
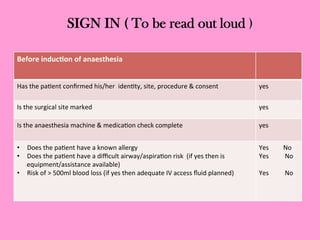
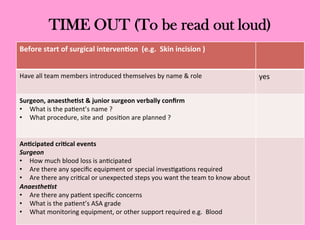
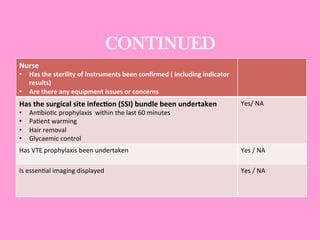
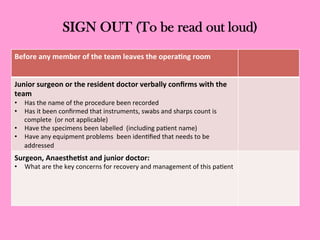
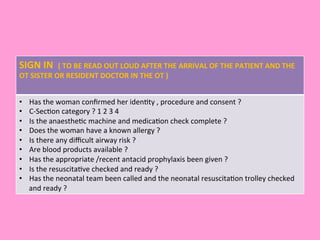
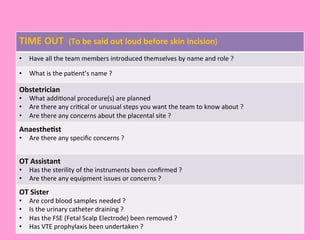
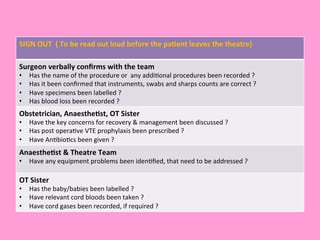
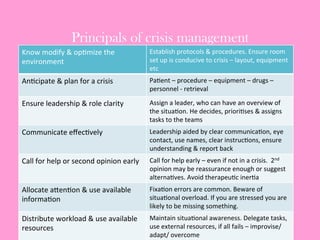
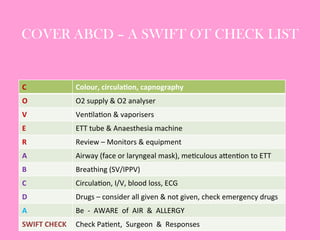




The document provides an operating theatre (OT) checklist to help ensure patient safety during surgical procedures. It lists several checks that the operating team should complete in the ward and theatre before surgery, including correctly identifying the patient, marking the intended surgical site, checking for allergies and previous medical history, and confirming critical patient information has been exchanged. The goal is for the team to operate on the right patient and site, take appropriate precautions, and communicate effectively to safely conduct the surgery and prevent errors.























































































