
Recommended
Recommended
More Related Content
Similar to Running Head CRITIQUE OF OCEAN TEMPERATURES IN CORAL REEFSCRIT.docx
Similar to Running Head CRITIQUE OF OCEAN TEMPERATURES IN CORAL REEFSCRIT.docx (20)
More from healdkathaleen
More from healdkathaleen (20)
Recently uploaded
Recently uploaded (20)
Running Head CRITIQUE OF OCEAN TEMPERATURES IN CORAL REEFSCRIT.docx
- 1. Running Head: CRITIQUE OF OCEAN TEMPERATURES IN CORAL REEFS CRITIQUE OF OCEAN TEMPERATURES IN CORAL REEFS Madison McNeill Introduction Coral reef ecosystems are the most diverse marine ecosystem in the world. They provide a home to thousands of species of plants and animals. In the last few decades, global warming has caused increased temperatures, resulting in ocean acidification and increasing surface temperatures of the ocean. This can lead to the bleaching of coral reefs as well as the death of coral reef fishes due to their inability to acclimate to the elevated temperature. These three papers were chosen, because they illustrate the environmental impact higher temperatures have on these coral reefs and the organisms that live within them. · Dias, M., Ferreira, A., Gouveia, R., Cereja, R., & Vinagre, C. (2018). Mortality, growth and regeneration following fragmentation of reef-forming corals under thermal stress. Journal of Sea Research, 141, 71-82. doi: 10.1016/j.seares.2018.08.008. · De'ath, G., Lough, J., & Fabricius, K. (2009). Declining Coral Calcification on the Great Barrier Reef. Science, 323(5910), 116-119. doi: 10.1126/science.1165283. · Nilsson, G., Östlund-Nilsson, S., & Munday, P. (2010). Effects of elevated temperature on coral reef fishes: Loss of hypoxia tolerance and inability to acclimate. Comparative Biochemistry and Physiology Part A: Molecular & Integrative Physiology, 156(4), 389-393. doi: 10.1016/j.cbpa.2010.03.009. Dias (2018) evaluated how elevated surface temperatures of the ocean affected growth, mortality, and regeneration following the fragmentation of nine coral species in the Indo-Pacific, while De'ath (2009) suggested that the ability of coral in the Great Barrier Reef may have depleted due to a decrease in the saturation state of aragonite and rising temperature stress in this
- 2. region. The third paper evaluated, Nilsson (2010), examined whether or not an elevated temperature decreased tolerance levels for low-oxygen regions in two species of coral reef fishes. This experiment used adults fishes of two species and tested their ability to acclimate to changes in higher temperatures, which differed from the other two studies in that Dias and De’Ath did not study the fishes in the ecosystems, only the coral there. Dias found that whether or not a coral had previous injury did not impact the mortality, partial mortality, or rate of growth of each fragment. However, the species of coral and the ocean temperature had significant impacts on the results for each fragment. Although the cause for coral calcification of Great Barrier Reef corals was not determined by the De'ath’s study, he did find that it was largely related to increasing temperatures of oceans, which caused more thermal stress in coral populations. This differed from the Nilsson paper, which showed that certain species of coral reef fishes were unable to adjust to higher ocean temperatures, a phenomenon that has occurred due to global warming and ocean acidification. Analysis Introduction When the three articles’ introductions were evaluated, some similarities as well as dissimilarities stood out. For example, the titles of the articles varied in appropriateness. Nilsson's title was too long. The paper had a title that told its audience what the researchers hoped to get out of it, but the title seemed long and bulky. The title, in my opinion, could have been shortened or rephrased to one that grabbed the audience’s attention more quickly, even a change as simple as changing the title to, “Effects of elevated temperature on coral reef fishes.” However, Dias’s title was accurate and concise. “Mortality, growth and regeneration following fragmentation” was a title that accurately explained what was being examined within the confines of this study. De'ath had a title that matched the contents of the paper as well.
- 3. The abstract’s statement of purpose of all three articles matched the introductions. For the Dias article, they stressed that the impacts of thermal stress on fragments of regenerating coral species needed to quickly be explored, while De'ath’s abstract was well written, telling readers how many coral colonies were studied and what the results showed. The abstract of Nilsson’s paper plainly stated what occurred within the first two sentences. The abstract’s statement of purpose for this article was to display how two species of coral reef fishes in the Great Barrier Reef are failing to acclimate to higher sea surface temperatures. This was plainly stated in both the abstract and introduction of the article. The hypotheses of the three articles varied greatly. Dias stated that the change in the global climate has led to rising sea surface temperatures and ocean acidification, which jeopardized coral reef survival. With this sentence, Dias made it clear why his study efforts were so urgent. Nilsson followed a similar pattern when he clearly stated his concerns for the inability of coral reef fishes to acclimate to rising water temperatures. De'ath’s hypothesis was stated in the abstract, which said that his study suggested that the increasing thermal stress may be depleting the ability of Great Barrier Reef corals to deposit calcium carbonate. Thus, the hypotheses of all three articles were given. I also found that Dias, De'ath, and Nilsson all had a nice way of arranging their data, which allowed the information to build to what the experimental design included and what the researchers were hoping to accomplish from this experiment. Methods The sample selection among the three articles showed great contrast. The Dias paper used nine reef-forming coral species, while De'ath’s experiment studied 328 colonies of coral from the same genus, Porites, which is a stony coral. Nilsson studied adults of two species of coral reef fishes. For Dias’s paper, the methods were easy to follow and seemed easy to repeat, while De’ath’s methods were harder to follow, for the details did not
- 4. appear to all be listed. The Methods section of the Nilsson article was both valid and delivered with enough detail that another group could perform most of this study again. Only most of the experiment, because although the article listed when and where the experiment was conducted, the number of each species of adult coral reef fish caught and analyzed was not given in the Methods sections of the paper. This information is crucial, because a small sample size could invalidate the data, while a large sample size could support the data more accurately. Furthermore, if one species of coral reef fishes had a much larger or small number than the other species, the data would also not be well represented in the results found by this study. The number of samples for both of the other articles were given. While some articles had strong Methods sections, others were missing key components. The experimental design for the three articles chosen all seemed valid. De’ath’s study seemed valid for the experiment being conducted, though I am unsure that this study could be repeated using the paper alone. The experimental design did make sense overall, in that Porites is commonly chosen for sclerochronological analyses because they have annual density bands that are widely distributed. Portites coral also has the capability of growing for hundreds of years, so choosing this genus of coral for a large analysis made sense. Using the three growth parameters De’ath mentioned—skeletal density, calcification rate, and annual extension rate—are good parameters to look at in a genus of coral that has such a long life span. Dias justified every step of his experimental design, making it easy to repeat the process. For instance, Dias utilized contrasting morphologies, because they have different susceptibilities to thermal stress, giving the overall results more credit. These corals were held in captivity for several years, giving the researchers knowledge of the corals’ thermal history. Twenty fragments were cut from each of the nine species, half of which were used as a control. Sources of variations were eliminated in this process by cutting only one coral from each
- 5. colony. These methods appear valid, and each is given a reason as to why a scientist would conduct the experiment in this way, making the overall flow of the methods logical and easy to follow. This was similar to De’ath’s paper in that De’ath listed the parameters used to test the samples, and he mention that Porites has such a long lifespan, so these types of corals have been proven to record environmental changes within their skeletons. This statement justified why De’ath chose this coral and explained why these particular parameters were chosen. However, he did not specify how to conduct these analyses. Also, although the data was collected within a two-month period for both Dias and Nilsson’s experiments, De’ath’s experiments was a composite collection from the years 1900-2006, containing over sixteen thousand annuals records with corals ranging from ten to 436 years old. Hence, the broad range of years the specimens were collected was overwhelming, not to mention the three growth parameters the paper mentioned but again failed to explain. Lastly, for Nilsson’s experimental design, I found that it was carried out well, using adults of the two species of coral reef fishes and varying temperatures that supported their hypothesis. However, not including the number of each species caught negates the data to a certain degree. Overall, I found that the Methods section of Nilsson’s paper was logical, but it did not contain details that were pertinent to this experiment, whereas Dias included all pertinent information and De’ath failed to include how he performed the parameters that were chosen. Results Since the concentration for each study varied, the results were also quite different in composition. Dias et al. (2018) found that injury—whether present or absent—had no impact on the death or growth rate of the coral fragments studied. The researchers determined that the true factors that impacted death and growth rate of the corals analyzed were temperature and the coral species itself. These results were illustrated using tables and figures. Table 1 was difficult to follow, because some of
- 6. the columns were abbreviated using terms not explained within the content of the article. However, the numbers in the table coincide with the text, showing that injury did not impact the growth or mortality rate of the coral fragments used in this experiment. The results found in De'ath’s paper were easy to follow, but showed that the cause of decline in coral populations in the GBR were still not known. Within the Results section of the articles written by Nilsson and De’ath, I saw that the figures and tables matched the text without repeating the same information to the audience. The figures and tables were accurate with what the text had previously stated, showing P values that were statistically significant, and the data was very easy to understand. The table in Dias’s article could have been better presented if the abbreviations used had some type of key that denote what each header meant. I did not find any discrepancies among the figures and text of the three articles as far as percentages were concerned. The results found in the three studies did test the hypothesis of the researchers. For Dias’s paper, these results were shown in Figure 1, which illustrated that as temperature increased, the mortality rate of coral species also increased. As Dias mentioned in the Abstract section, there were two coral species that survived this experiment, Turbinaria reniformis and Galaxea fascicularis. However, the results of the Nilsson paper were to test the hypothesis of the researchers in that study, which was that after a given number of days in varying temperatures, the coral reef fishes studied would fail to acclimate to those temperature changes. Again, in the third paper, De’ath’s results tested the hypothesis, including 328 colonies of massive corals form 69 various reefs, which made the results more broad. Discussion I found that none of the three articles repeated the same information in both the figures and the text of the article. From the Discussion section of the Dias paper, a reader could tell the main points of the article, which were to show that there was
- 7. variability in the susceptibility to thermal stress of different coral reef species. These coral reef species had the lowest mortality, partial mortality, and levels of bleaching at 26 degrees Celsius, while their growth rate was at its zenith at this temperature. Dias found that the regeneration rate of corals generally increased as the temperature increased. These results also show that the bleaching resistance capacity of most of the corals analyzed was overcome at 32 degrees Celsius. Because this paper is so new—published in 2018—I could not find its interpretations to be supported by other research. However, the article does list the direction in which the research is headed and lists other studies similar to this one. The findings of De'ath’s and Dias’s articles were supported by each other, as well as many other articles over coral reef ecology. However, I found very few articles that supported the conclusions drawn by Nilsson (2010) about the effects increasing temperatures had on two species of coral reef fishes, which was a weakness for the paper. In all three journal articles, I found that the interpretation of data was logical. Conclusion Summary The three articles, overall, had both strengths and weaknesses. For instance, all three papers were peer reviewed. Nilsson’s paper had few other articles that backed up its findings, while Dias and De’ath backed up each other’s paper. The article by Dias (2018) was very recent, which made it one of the newest published papers in its field, while the De'ath and Nilsson papers were a few years older. Although the Dias paper had tables and figures that were not entirely straight forward, the content of the article itself was very easy to follow. Each section within the article was set apart, whereas in the article by De’ath, the sections (introduction, methods, etc.) were not separated from each other. The Dias and De’ath papers had appropriate titles, while Nilsson’s title was too long. The abstracts and introductions match for all three articles. The pace for the Dias article is great, leading the audience straight
- 8. into the hypothesis and objectives for the analysis, while De’ath failed to separate his paper into different sections. Overall, Dias and the other researchers took many steps to ensure accurate results, and the Methods section of this article is explained well enough to be repeated, which differed from Nilsson’s paper in that Nilsson did not include his sample size. When it came to reproducing the experiment, Dias included all pertinent information, but De’ath failed to include how he performed the parameters that were chosen. De’ath had a concise paper with text that accurately related to the figures mentioned. Overall, the article was concise in its findings, but not as easy to follow as it could have been if the proper sections and subsections had been utilized. The title seemed appropriate, and readers know from the statement of purpose and the introduction that the primary goal of this study was to help determine what is causing the decline in corals’ ability to lay down a calcium carbonate skeleton to more efficiently build coral reef ecosystems. The De'ath paper used a large sample selection, which made the results seem more inclusive as opposed to Dias’s samples size of nine species of corals using twenty fragments of each species. Nilsson’s article had excellent figures that were easy to interpret, in contrast to Dias’s paper that did not explain what some of the abbreviations meant in the tables. The strengths and weaknesses of the three papers varied greatly. Significance When evaluating the role these articles play in the world, striking similarities were found. Nilsson’s article showed primary concerns toward two populations of fish species that lived in the Great Barrier Reef, while De’ath and Dias wrote papers over the reactions of different coral species to increasing surface temperatures. De’ath’s article has practical significance similar to the Dias paper, in that major ecosystems are dying as a result of rising ocean surface temperatures, and these researchers tried to find ways to explain these issues. Nilsson’s article examined whether or not increasing temperatures
- 9. reduced the hypoxia tolerance of coral reef fishes. It has been cited sixty-nine times, cited in papers involving hypoxia tolerance of coral reef fishes, how temperature and hypoxia play a role in respiratory performance of certain tropical fishes, and many other similar studies (Nilsson et al.). De'ath et al. has been cited twenty-four times, which sparked interest for similar research in the Great Barrier Reef in the last decade. The Dias et al. paper was only published in 2018, so not many other researchers have cited this paper yet. This can be seen as a potential problem; however, the article was peer-reviewed by individuals who are well-educated in this particular field. The currency of the Dias article may also be seen as a good attribute, showing that this information was some of the newest in its field of interest. The research among all three articles has significance to today’s society, in that the bleaching of coral reefs has become a growing problem, and without more research to determine what factors are causing this issue, large hypoxic zones in aquatic ecosystems may result. Overall, all three of these articles illustrated environmental significance. Human survival depends on the biodiversity of plants and animals, and many animals live in these coral reef ecosystems. Works Cited De'ath, G., Lough, J., & Fabricius, K. (2009). Declining Coral Calcification on the Great Barrier Reef. Science, 323(5910), 116-119. doi: 10.1126/science.1165283 Dias, M., Ferreira, A., Gouveia, R., Cereja, R., & Vinagre, C. (2018). Mortality, growth and regeneration following fragmentation of reef-forming corals under thermal stress. Journal of Sea Research, 141, 71-82. doi: 10.1016/j.seares.2018.08.008 Nilsson, G., Östlund-Nilsson, S., & Munday, P. (2010). Effects of elevated temperature on coral reef fishes: Loss of hypoxia tolerance and inability to acclimate. Comparative Biochemistry
- 10. and Physiology Part A: Molecular & Integrative Physiology, 156(4), 389-393. doi: 10.1016/j.cbpa.2010.03.009 [Type here] 2 9 QUESTION 1 Naïve Bayesian Classifiers are among the most successful known algorithms for learning to classify text documents and they are used to detect fraud. True False QUESTION 2 What is the most accurate statement that describe what “Leaf Nodes” are in a decision tree? Decisions that are often used as components in ensemble techniques predictive models which will all vote. The nature of the variable, you may need to include an equal to component on one branch. Decision at the end of the last branch on the tree. These represent the outcome of all the prior decisions. They are the class labels, or the segment in which all observations that
- 11. follow the path to the leaf would be placed. None of the above. QUESTION 3 What is confusion matrix and what are the values, rates, metrics associated with the matrix? ANS: QUESTION 4 Decision Trees are a flexible method very commonly deployed in data mining applications. There are two types of decision trees. What are the two trees and the descriptions of both? ANS: QUESTION 5 Decision Trees take only categorical variables. They cannot handle many distinct values such as the zip code in the data and are limited to only one attribute. True False QUESTION 6 Time Series Analysis is the analysis of sequential data across equally spaced units of time. Time Series is a basic research methodology in which data for one or more variables are collected for many observations at different time periods. What are the two main objectives in Time Series Analysis? ANS: QUESTION 7
- 12. In the Box-Jenkins model, Autoregressive (AR) models can be coupled with moving average (MA) models to form: The input for the model that trend and are seasonality adjusted in time series and the output that provides an expected future value of the time series. The next stage to determine the p and q in the ARIMA (p, d, q) model. The assurance level of obtaining the highest forecasting accuracy possible in terms of the variables on which the forecast is based. A general and useful class of time series models called Autoregressive Moving Average (ARMA) models. QUESTION 8 The Information Gain is defined as the difference between the base entropy and the conditional entropy of the attribute. True False QUESTION 9 "Pure enough" usually means that other information can be gained by splitting on other attributes. True False QUESTION 10
- 13. The key application of Time Series Analysis is in forecasting. In regard to Time Series data, what are the 6 fields in society that Time Series data provide useful information about the physical, biological, social or economic systems generating the time series? ANS: Overweight, obesity and risk of liver cancer: a meta-analysis of cohort studies SC Larsson*,1 and A Wolk1 1 Division of Nutritional Epidemiology, The National Institute of Environmental Medicine, Karolinska Institutet, PO Box 210, Stockholm SE-17177, Sweden Cohort studies of excess body weight and risk of liver cancer were identified for a meta-analysis by searching MEDLINE and EMBASE databases from 1966 to June 2007 and the reference lists of retrieved articles. Results from individual studies were combined using a random-effects model. We identified 11 cohort studies, of which seven on overweight (with a total of 5037 cases) and 10 on obesity (with 6042 cases) were suitable for meta-analysis. Compared with persons of normal weight, the summary relative risks of liver cancer were 1.17 (95% confidence interval (CI): 1.02 – 1.34) for those who were overweight and 1.89 (95% CI: 1.51 – 2.36) for those
- 14. who were obese. This meta-analysis finds that excess body weight is associated with an increased risk of liver cancer. British Journal of Cancer (2007) 97, 1005 – 1008. doi:10.1038/sj.bjc.6603932 www.bjcancer.com Published online 14 August 2007 & 2007 Cancer Research UK Keywords: body mass index; cohort studies; liver cancer; meta- analysis; obesity; review �� � � � � � � � � � � � � � � � � � � � � � � � � �
- 15. � � � � � � � Although relatively rare in the United States and other developed countries, liver cancer is the third most common cause of death from cancer worldwide (Parkin et al, 2005). It is rarely detected early and is often fatal within a few months of diagnosis. The 5-year survival rate is only about 6 – 11% (Coleman et al, 2003; Ries et al, 2006). The age-adjusted incidence and mortality rates of liver cancer have been increasing rapidly in the United States since the mid-1980s (Ries et al, 2006). While approximately half of this increase can be attributable to hepatitis C virus infection, a minimal or no increase has been related to hepatitis B virus and alcoholic liver disease (El-Serag and Mason, 2000; Hassan et al, 2002). Given that about half of the increase in liver cancer incidence is not related to hepatitis, the major risk factor in a significant proportion of the cases has yet to be identified. Coinciding with the rising incidence of liver cancer, the prevalence of obesity has been increasing markedly over the past two decades worldwide (Larsson and Wolk, 2006). Obesity has been recognised as a risk factor for several malignancies, including cancer of the breast (in premenopausal women), endometrium,
- 16. kidney (renal cell), colon, pancreas, gallbladder, and esophagus (adenocarcinoma) (IARC, 2002; Larsson et al, 2007; Larsson and Wolk, 2007). Accumulating epidemiologic evidence also indicates that excess body weight may be a risk factor for liver cancer, but the evidence has not been quantitatively summarised. We have therefore quantitatively assessed the associations of overweight and obesity with liver cancer risk in a meta-analysis of cohort studies. MATERIALS AND METHODS Study selection A literature search was conducted in the MEDLINE and EMBASE databases for pertinent studies published in any language from 1966 to June 2007. We used the keywords ‘body mass index’, ‘BMI’, or ‘obesity’ in combination with ‘hepatocellular carcinoma’, ‘liver cancer’, or ‘liver neoplasm’. Moreover, we manually reviewed the reference lists of retrieved articles to search for more studies. Studies were included in the meta-analysis if they fulfilled the following criteria: (1) cohort study in which liver cancer incidence or mortality was an outcome; (2) the exposure of interest was overweight and/or obesity defined by body mass index (BMI) (the weight in kilograms divided by the square of height in meters); and (3) relative risk estimates (rate ratio or standardized incidence
- 17. ratio) with corresponding 95% confidence intervals (CIs) were reported. Data extraction For each study, the following information was extracted: first author’s last name; publication year; country in which the study was performed; sample size; method of assessing weight and height; type of outcome (incidence or mortality); variables adjusted for in the analysis; and the relative risks with 95% CIs for overweight and obesity vs normal weight. From each study, we extracted the most fully adjusted relative risks. Statistical analysis The relative risks and corresponding standard errors (derived from the CIs) from individual studies were logarithmically transformed to stabilize variances and normalize the distributions. We calculated summary relative risks for overweight (defined as Received 13 June 2007; revised 12 July 2007; accepted 17 July 2007; published online 14 August 2007 *Correspondence: Dr SC Larsson; E-mail: [email protected] British Journal of Cancer (2007) 97, 1005 – 1008 & 2007 Cancer Research UK All rights reserved 0007 – 0920/07 $30.00 www.bjcancer.com E p
- 18. id e m io lo g y http://dx.doi.org/10.1038/sj.bjc.6603932 http://www.bjcancer.com mailto:[email protected] http://www.bjcancer.com BMI 25 – 30 kg m�2) and obesity (BMI X30 kg m�2) vs normal weight (BMI 18.5 – 24.9 kg m�2). For two studies (Calle et al, 2003; Kuriyama et al, 2005) that reported relative risks for two categories of BMI that fell into the category representing overweight or obesity, we pooled the relative risks and used the pooled estimate in the meta-analysis. Study-specific relative risks were combined using the DerSimonian and Laird random-effects model (DerSimonian and Laird, 1986). Thus, each summary relative risk was a weighted average of the study-specific relative risk, where the weight for each study is the inverse of the sum of the within- study variance for that study, and the between-study variance.
- 19. Statistical heterogeneity among studies was evaluated with the Q and I2 statistics (Higgins and Thompson, 2002). For the Q statistic, statistical significance was set at Po0.1. We used funnel plots (i.e. plots of study results against precision) to assess publication bias, and tested the symmetry of the funnel plot using Egger’s test (Egger et al, 1997). Results are presented graphically, whereby squares represent study-specific relative risks and diamonds represent summary relative risks. The area of each square is proportional to the inverse of the variance of the logarithm of the relative risk; 95% CIs for individual studies are represented by horizontal lines and for the summary estimates by the width of the diamonds. Statistical analyses were performed with Stata, version 9.0 (StataCorp, College Station, TX, USA). Population attributable risk (PAR) for liver cancer was estimated for individuals with excess body weight (BMIX25 kg m�2) compared to those of normal weight (BMIo25 kg m�2). The PAR describes the theoretic proportion of cases that would be prevented if all individuals were moved into the exposure level associated with the lowest risk for that factor. The PAR (PAR%) was calculated as: PAR% ¼ (p � [RR – 1]/ [p � (RR – 1) þ 1]) � 100%, where p represents the prevalence in the population and RR the relative risk. Prevalence data were obtained from the National Health and Nutrition Examination Survey that assessed the prevalence of overweight and obesity
- 20. in a representative sample of the US population (Ogden et al, 2006). In that survey, 39.7% of the men were overweight and 31.1% were obese. Among women, 28.6% were overweight and 33.2% were obese. PARs were calculated for the overweight and obese categories using the obtained summary relative risks, and then summarized across the two categories for men and women separately. RESULTS We identified 11 eligible cohort studies (Møller et al, 1994; Wolk et al, 2001; Nair et al, 2002; Calle et al, 2003; Samanic et al, 2004, 2006; Batty et al, 2005; Kuriyama et al, 2005; Oh et al, 2005; Rapp et al, 2005; N’Kontchou et al, 2006), of which 7 on overweight (with a total of 5037 cases) (Calle et al, 2003; Batty et al, 2005; Kuriyama et al, 2005; Oh et al, 2005; Rapp et al, 2005; N’Kontchou et al, 2006; Samanic et al, 2006) and 10 on obesity (with a total of 6042 cases) (Møller et al, 1994; Wolk et al, 2001; Nair et al, 2002; Calle et al, 2003; Samanic et al, 2004, 2006; Batty et al, 2005; Oh et al, 2005; Rapp et al, 2005; N’Kontchou et al, 2006) were suitable for meta- analysis. Characteristics of the studies are shown in Table 1. Seven studies were conducted in Europe, two in the United States, and
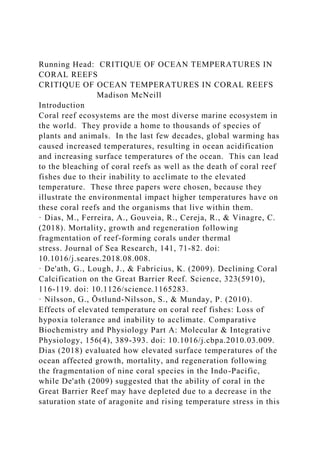
- 21. two in Asia. Weight and height were measured in six studies and self-reported in two studies; in three studies, obesity was defined by a discharge diagnosis of obesity. The outcome was incidence of liver cancer in all but two studies (Calle et al, 2003; Batty et al, 2005) in which the outcome was mortality from liver cancer. Two studies were based on standardized incidence ratio (Møller et al, 1994; Wolk et al, 2001). Two studies consisted of patients with cirrhosis (Nair et al, 2002; N’Kontchou et al, 2006). Relative risks of liver cancer for overweight and obese individuals compared to those of normal weight for individual studies (separately for men and women wherever this data were available) and all studies combined are shown in Figure 1. Meta- analysis of all studies found that compared to individuals with normal weight, those who were overweight or obese had a 17 and 89%, respectively, increased risk of liver cancer. There was statistically significant heterogeneity among the results of indivi- dual studies (Figure 1). The summary relative risk for obesity was statistically significantly higher (P ¼ 0.03) for men (RR: 2.42; 95% CI: 1.83 – 3.20; n ¼ 7 studies) than for women (RR: 1.67; 95% CI: Table 1 Characteristics of cohort studies included in the meta- analysis Study Country No. of cases
- 22. (men/women) Study participants Assessment of exposure Adjustments Møller et al (1994) Denmark 22/36 Men: 14 531 Women: 29 434 Discharge diagnosis of obesity Age Wolk et al (2001) Sweden 15/13 Men: 8165 Women: 19 964 Discharge diagnosis of obesity Age, calendar year Nair et al (2002) USA 659a Men and women: 19 271a Measured Age, sex, race, diabetes Calle et al (2003) USA 620/345 Men: 404 576 Women: 495 477 Self-reported Age, race, education, marital status, smoking, physical activity, aspirin use, estrogen-replacement therapy (women), alcohol, dietary factors Samanic et al (2004) USA 322 whites/38 blacks White men: 3 668 486 Black men: 832 214
- 23. Discharge diagnosis of obesity Age, calendar year Kuriyama et al (2005) Japan 69/31 Men: 12 485 Women: 15 054 Self-reported Age, type of health insurance, smoking, intakes of alcohol, meat, fish, fruits, vegetables, bean-paste soup b Batty et al (2005) UK 51 Men: 18 403 Measured Age, employment grade, marital status, physical activity, smoking, other c Oh et al (2005) Korea 3347 Men: 781 283 Measured Age, area of residence, family history of cancer, smoking, exercise, alcohol Rapp et al (2005) Austria 57 Men: 67 447 Measured Age, occupational group, smoking N’Kontchou et al (2006) France 220a Men and women: 771a Measured Age, sex, cirrhosis cause, diabetes Samanic et al (2006) Sweden 297 Men: 362 552 Measured Age, smoking a Patients with cirrhosis. b
- 24. Odds ratios for women were further adjusted for age at menarche, age at end of first pregnancy, and menopausal status. c Other factors adjusted for include disease at entry, weight loss in the last year, height- adjusted FEV1, triceps skinfold thickness, blood pressure- lowering medication, blood pressure, plasma cholesterol, glucose intolerance, and diabetes. Overweight, obesity and gallbladder cancer SC Larsson and A Wolk 1006 British Journal of Cancer (2007) 97(7), 1005 – 1008 & 2007 Cancer Research UK E p id e m io lo g y 1.37 – 2.03; n ¼ 3 studies). There was no evidence for
- 25. publication bias on the funnel plot (data not shown) or by Egger’s test (P ¼ 0.31 for overweight and P ¼ 0.21 for obesity). In a sensitivity analysis excluding the two studies that consisted of patients with cirrhosis (Nair et al, 2002; N’Kontchou et al, 2006), the summary relative risks were 1.07 (95% CI: 1.01 – 1.15) for overweight and 1.85 (95% CI: 1.44 – 2.37) for obesity. With stratification by assessment of obesity, the summary relative risks for the association between obesity and liver cancer were 2.15 (95% CI: 1.66 – 2.77) for studies based on measured or self-reported weight and height (Nair et al, 2002; Calle et al, 2003; Batty et al, 2005; Oh et al, 2005; Rapp et al, 2005; N’Kontchou et al, 2006; Samanic et al, 2006) and 1.61 (95% CI: 1.14 – 2.27) for studies based on a discharge diagnosis of obesity (Møller et al, 1994; Wolk et al, 2001; Samanic et al, 2004). The PAR for excess body weight was calculated using the estimates of prevalence in the United States (Ogden et al, 2006) and the obtained summary relative risks of 1.17 and 1.89 for overweight and obesity, respectively. We estimated that 28% of liver cancer cases among men and 27% among women could be attributable to excess body weight (BMIX25 kg m�2). DISCUSSION This is the first meta-analysis on overweight and obesity in relation to liver cancer risk and it indicates that excess body weight is associated with increased risk. Summary results showed that the
- 26. risk was 17 and 89% higher among persons who were overweight and obese, respectively, compared with those of normal weight. The relation between obesity and liver cancer seemed to be stronger in men than in women. Although there was statistically significant heterogeneity among study results, the relation between obesity and risk of liver cancer was consistent. Differences in the relative risk estimates were largely in the magnitude rather than the direction of the association. All but 1 out of the 14 relative risk estimates for the association between obesity and liver cancer were above one (ranging from 1.44 to 3.76), and 12 of these estimates were statistically significant. A potential limitation of this meta-analysis is that individual studies may have failed to control for potential known or unknown confounders. The most important risk factors for the development of liver cancer are chronic infections with hepatitis B virus and hepatitis C virus. Heavy, long-term alcohol consumption is also a risk factor (Yu and Yuan, 2004). None of the studies adjusted for hepatitis B or C virus infections, and only three (Calle et al, 2003; Kuriyama et al, 2005; Oh et al, 2005) controlled for alcohol intake. It is unlikely, however, that these risk factors are strongly related to body weight and entirely explain the observed relationship between excess body weight and liver cancer risk. Another limitation is that we could not examine whether the association
- 27. between excess body weight and liver cancer was modified by hepatitis virus infections and alcohol intake because the studies included in this meta-analysis did not provide results stratified by these factors. As this meta-analysis was based on published studies, possible publication bias could have affected the results. However, neither funnel plots nor formal statistical tests showed evidence for publication bias. The observed increased risk of liver cancer associated with excess body weight may be mediated through the development of non-alcoholic fatty liver disease (NAFLD), a chronic liver disease that occurs in non-drinkers. NAFLD is characterized by a spectrum of liver tissue changes, ranging from accumulation of fat in the liver to non-alcoholic steatohepatitis (NASH), cirrhosis, and liver cancer at the most extreme end of the spectrum. Up to 90% of obese individuals have some degree of fatty liver, and approximately 25 – 30% have NASH (Neuschwander-Tetri and Caldwell, 2003). Relative risk 0.5 0.7 1.0 1.5 2.0 3.0 4.5 6.0 Relative risk (95% CI) Overweight Calle et al (2003) (M) 1.13 (0.94–1.34) Calle et al (2003) (W) 1.02 (0.80–1.31) Kuriyama et al (2005) (M) 0.91 (0.52–1.59)
- 28. Kuriyama et al (2005) (W) 1.13 (0.57–2.27) Batty et al (2005) (M) 0.99 (0.53–1.88) Oh et al (2005) (M) 1.05 (0.97–1.14) Rapp et al (2005) (M) 1.32 (0.73–2.37) N'Kontchou et al (2006) (M/W) 2.00 (1.40–2.70) Samanic et al (2006) (M) 1.29 (1.00–1.68) Summary estimate 1.17 (1.02–1.34) Obesity Møller et al (1994) (M) 1.90 (1.20–2.90) Møller et al (1994) (W) 1.90 (1.40–2.70) Wolk et al (2001) (M) 3.60 (2.00–6.00) Wolk et al (2001) (W) 1.70 (1.10–2.50) Nair et al (2002) (M/W ) 1.65 (1.22–2.22) Calle et al (2003) (M) 2.41 (1.92–3.01) Calle et al (2003) (W) 1.47 (1.08–2.00) Samanic et al (2004) (M, whites) 1.44 (1.28–1.61) Samanic et al (2004) (M, blacks) 0.68 (0.49–0.94) Batty et al (2005) (M) 3.76 (1.36–10.4) Oh et al (2005) (M) 1.56 (1.15–2.12) Rapp et al (2005) (M) 1.67 (0.75–3.72) N'Kontchou et al (2006) (M/W) 2.80 (2.00–4.00) Samanic et al (2006) (M) 3.62 (2.62–5.00) Summary estimate 1.89 (1.51–2.36) Figure 1 Relative risks of liver cancer associated with overweight and obesity. Relative risk estimates are for overweight and obese persons compared with normal weight persons. Tests for heterogeneity: overweight, Q ¼ 16.83, P ¼ 0.03; I2 ¼ 52.5%; obesity, Q ¼ 88.03, Po0.001; I2 ¼ 86.4%. M ¼ men; W ¼ women. Overweight, obesity and gallbladder cancer
- 29. SC Larsson and A Wolk 1007 British Journal of Cancer (2007) 97(7), 1005 – 1008& 2007 Cancer Research UK E p id e m io lo g y In summary, this meta-analysis supports evidence of an increased risk of liver cancer among overweight and obese persons. These findings indicate that liver cancer may, in part, be prevented by maintaining a healthy body weight. ACKNOWLEDGEMENTS This work was supported by grants from the Swedish Cancer Society. REFERENCES Batty GD, Shipley MJ, Jarrett RJ, Breeze E, Marmot MG, Smith
- 30. GD (2005) Obesity and overweight in relation to organ-specific cancer mortality in London (UK): findings from the original Whitehall study. Int J Obes (Lond) 29: 1267 – 1274 Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ (2003) Overweight, obesity, and mortality from cancer in a prospectively studied cohort of US adults. N Engl J Med 348: 1625 – 1638 Coleman MP, Gatta G, Verdecchia A, Esteve J, Sant M, Storm H, Allemani C, Ciccolallo L, Santaquilani M, Berrino F (2003) EUROCARE- 3 summary: cancer survival in Europe at the end of the 20th century. Ann Oncol 14(Suppl 5): v128 – v149 DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7: 177 – 188 Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta- analysis detected by a simple, graphical test. BMJ 315: 629 – 634 El-Serag HB, Mason AC (2000) Risk factors for the rising rates of primary liver cancer in the United States. Arch Intern Med 160: 3227 – 3230 Hassan MM, Frome A, Patt YZ, El-Serag HB (2002) Rising
- 31. prevalence of hepatitis C virus infection among patients recently diagnosed with hepatocellular carcinoma in the United States. J Clin Gastroenterol 35: 266 – 269 Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta- analysis. Stat Med 21: 1539 – 1558 IARC (2002) IARC handbooks of cancer prevention. Weight control and physical activity. Vol. 6, Lyon, France: IARC Press Kuriyama S, Tsubono Y, Hozawa A, Shimazu T, Suzuki Y, Koizumi Y, Ohmori K, Nishino Y, Tsuji I (2005) Obesity and risk of cancer in Japan. Int J Cancer 113: 148 – 157 Larsson SC, Orsini N, Wolk A (2007) Body mass index and pancreatic cancer risk: A meta-analysis of prospective studies. Int J Cancer 120: 1993 – 1998 Larsson SC, Wolk A (2006) Epidemiology of obesity and diabetes: prevalence and trends. In Obesity and Diabetes, Mantzoros C (ed) pp 15 – 36. Boston: Humana Press Larsson SC, Wolk A (2007) Obesity and the risk of gallbladder cancer: a meta-analysis. Br J Cancer 96: 1457 – 1461
- 32. Møller H, Mellemgaard A, Lindvig K, Olsen JH (1994) Obesity and cancer risk: a Danish record-linkage study. Eur J Cancer 30A: 344 – 350 Nair S, Mason A, Eason J, Loss G, Perrillo RP (2002) Is obesity an independent risk factor for hepatocellular carcinoma in cirrhosis? Hepatology 36: 150 – 155 Neuschwander-Tetri BA, Caldwell SH (2003) Nonalcoholic steatohepatitis: summary of an AASLD Single Topic Conference. Hepatology 37: 1202 – 1219 N’Kontchou G, Paries J, Htar MT, Ganne-Carrie N, Costentin L, Grando- Lemaire V, Trinchet JC, Beaugrand M (2006) Risk factors for hepatocellular carcinoma in patients with alcoholic or viral C cirrhosis. Clin Gastroenterol Hepatol 4: 1062 – 1068 Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM (2006) Prevalence of overweight and obesity in the United States, 1999 – 2004. JAMA 295: 1549 – 1555 Oh SW, Yoon YS, Shin SA (2005) Effects of excess weight on cancer incidences depending on cancer sites and histologic findings among men: Korea national health insurance corporation study. J Clin
- 33. Oncol 23: 4742 – 4754 Parkin DM, Bray F, Ferlay J, Pisani P (2005) Global cancer statistics, 2002. CA Cancer J Clin 55: 74 – 108 Rapp K, Schroeder J, Klenk J, Stoehr S, Ulmer H, Concin H, Diem G, Oberaigner W, Weiland SK (2005) Obesity and incidence of cancer: a large cohort study of over 145 000 adults in Austria. Br J Cancer 93: 1062 – 1067 Ries LAG, Harkins D, Krapcho M, Mariotto A, Miller AB, Feuer EJ, Clegg L, Eisner MP, Horner MJ, Howlader N, Hayat M, Hankey BF, Edwards BK (2006) SEER cancer statistics review, 1975 – 2003. Bethesda, MD: National Cancer Institute, 2006 http://seer.cancer.gov/csr/1975_2003/ (accessed 30 June 2007) Samanic C, Chow WH, Gridley G, Jarvholm B, Fraumeni JF (2006) Relation of body mass index to cancer risk in 362 552 Swedish men. Cancer Causes Control 17: 901 – 909 Samanic C, Gridley G, Chow WH, Lubin J, Hoover RN, Fraumeni Jr JF (2004) Obesity and cancer risk among white and black United States veterans. Cancer Causes Control 15: 35 – 43
- 34. Wolk A, Gridley G, Svensson M, Nyren O, McLaughlin JK, Fraumeni JF, Adam HO (2001) A prospective study of obesity and cancer risk (Sweden). Cancer Causes Control 12: 13 – 21 Yu MC, Yuan JM (2004) Environmental factors and risk for hepatocellular carcinoma. Gastroenterology 127: S72 – S78 Overweight, obesity and gallbladder cancer SC Larsson and A Wolk 1008 British Journal of Cancer (2007) 97(7), 1005 – 1008 & 2007 Cancer Research UK E p id e m io lo g y http://seer.cancer.gov/csr/1975_2003/Overweight, obesity and risk of liver cancer: a meta-analysis of cohort studiesMATERIALS AND METHODSStudy selectionData extractionStatistical analysisRESULTSDISCUSSIONFigure 1
- 35. Relative risks of liver cancer associated with overweight and obesity.Table 1 Characteristics of cohort studies included in the meta-analysisACKNOWLEDGEMENTSREFERENCES Hindawi Publishing Corporation ISRN Preventive Medicine Volume 2013, Article ID 680536, 16 pages http://dx.doi.org/10.5402/2013/680536 Review Article The Association between Obesity and Cancer Risk: A Meta-Analysis of Observational Studies from 1985 to 2011 M. Dobbins,1 K. Decorby,1 and B. C. K. Choi2 1 School of Nursing, McMaster University, 1280 Main Street West, 3N25G, Hamilton, ON, Canada L8N 3Z5 2Department of Epidemiology and Community Medicine, University of Ottawa, Ottawa, ON, Canada K1H 8M5 Correspondence should be addressed to M. Dobbins; [email protected] Received 10 January 2013; Accepted 10 February 2013 Academic Editors: C. R. González Bonilla, C. Grandjean, and F. Mawas Copyright © 2013 M. Dobbins et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Cancer and cardiovascular diseases are the leading
- 36. causes of mortality and morbidity worldwide. The purpose of this meta-analysis is to synthesize the evidence evaluating the association between obesity and 13 cancers shown previously to be significantly associated with obesity. Methods. Relevant papers from a previously conducted review were included in this paper. In addition, database searches of Medline and Embase identified studies published from the date of the search conducted for the previous review (January, 2007) until May, 2011. The reference lists of relevant studies and systematic reviews were screened to identify additional studies. Relevance assessment, quality assessment, and data extraction for each study were conducted by two reviewers independently. Meta-analysis was performed for men and women separately using DerSimonian and Laird’s random effectsmodel.Results. A total of 98 studies conducted in 18 countries from 1985 to 2011 were included.Data extractionwas completed on the 57 studies judged to be of strong and moderate methodological quality. Results illustrated that obese men were at higher risk for developing colon (Risk Ratio (RR), 1.57), renal (1.57), gallbladder (1.47), pancreatic (1.36), andmalignant melanoma cancers (1.26). Obese women were at higher risk for esophageal adenocarcinoma (2.04), endometrial (1.85), gallbladder (1.82), renal (1.72), pancreatic (1.34), leukemia (1.32), postmenopausal breast (1.25), and colon cancers (1.19). Conclusions. The results of this meta- analysis illustrate a significant, positive, and, for some cancers, strong association between obesity and cancer incidence. Given that approximately 23% of Canadians are obese, a significant proportion of cancer in Canada could be avoided if obesity was eliminated
- 37. or significantly reduced. 1. Introduction Chronic diseases are the leading cause of mortality and mor- bidity and contribute significantly to the overall health expen- ditures from both a societal perspective as well as an individ- ual one [1]. Common chronic diseases include heart disease, stroke, cancer, emphysema, diabetes, and osteoporosis. Fur- thermore, cancer and cardiovascular diseases are the leading causes of mortality andmorbidity worldwide [2], with cancer expected to result in 75,000 deaths per year in Canada [3] and 571,950 in the US [4]. While the leading risk factor for cancer continues to be tobacco use, evidence shows that obesemen andwomen have a greater likelihood of developing and dying from cancer than those who are not [2, 5–7]. Obesity is defined as a Body Mass Index (BMI) of 30 kg/m2 or greater. Approximately a quarter of Canadianmen and women are considered obese [9].There are many contributing factors to obesity such as physical inactivity, unhealthy diet, genetics, and others such as meta- bolic, environmental, social, economic, and psychological factors. It is estimated that globally, every year, three to four million cases of cancer could be prevented by eating healthier and being more physically active [2]. With respect to morbidity, research demonstrates that obesity increases the risk of cancers of the esophagus, breast (postmenopausal), endometrium, colon and rectum, kidney, pancreas, thyroid, gallbladder, and possibly other cancers as well [8]. Other evidence suggests that obesity leads to an increased risk for thirteen cancers including esophageal adenocarcinoma, thyroid, colon, rectal, renal, endometrial, pancreatic, gallbladder, postmenopausal breast, malignant
- 38. melanoma, multiple myeloma, leukemia, and non-Hodgkin 2 ISRN Preventive Medicine lymphoma [6].The cost of obesity to the health care system in Canada is estimated to be 4.3 billion per year [10]. Elsewhere the cost of obesity to the health care system has been found to represent 2.3% of annual hospital care costs [11]. Physical inactivity, which contributes to obesity, has been associated with significant health care expenditures for numerous chronic diseases including cancer. Canadian research esti- mates the economic burden of obesity as $2.1 billion in both direct and indirect costs [12]. Data from that same study sug- gests that a 10% decrease in inactivity would result in health savings of $150 million per annum [13]. The purpose of this meta-analysis is to synthesize the evi- dence evaluating the association between obesity and cancer. Specifically the association between obesity and thirteen can- cers shown previously [6] to be significantly associated with obesity is the focus of this meta-analysis. In addition, among cancers for which a statistically significant positive associa- tion with obesity is observed, population-attributable risk for the Canadian population is calculated and reported. 2. Methods 2.1. Search Strategy. Several activities were included in the search strategy to identify primary studies for this paper. An overview of the review process is depicted in Figure 1. First, the primary studies included in Renehan et al., for which significant associations between obesity and cancer were reported, were identified and retrieved in full document version. The search strategy employed by Renehan et al.
- 39. identified studies published between 1985 and 2007, indexed in Medline and Embase. Three additional studies, noted by Renehan et al., but published after their search was con- ducted, and therefore not included in their review, were also retrieved. Second, a search for studies, conducted since the Renehan et al. search for primary studies was completed, was con- ducted using the following search strategy. The electronic searches performed by Renehan et al. were replicated from January 2007 to May 2011 in Medline and Embase through OVID. Titles and abstractswere screened for relevance by two independent reviewers. All references chosen by one or both of the reviewers as being potentially relevant were selected for further review and imported into Systematic Review Software (SRS) from the Centre for Evidence-Based Medicine. All potentially relevant studies were retrieved in PDF version. Finally, the reference lists of relevant studies were screened to identify additional potentially relevant studies, as well as the reference lists of published systematic reviews or meta- analyses on this topic. 2.2. Relevance Assessment. Two reviewers independently screened all retrieved articles using an existing relevance assessment tool. The following four criteria were used to assess relevance to the research question: (1) is the article a primary study; (2) is the focus of the study to explore the rela- tionship between obesity and cancer incidence in adults aged 18 years and older; (3) does the study report on any one or more of the following 13 cancers: esophageal adenocarci- noma, thyroid, colon, renal, endometrial, gallbladder, rectal, malignant melanoma, postmenopausal breast, pancreatic, leukemia, multiple myeloma, and non-Hodgkin lymphoma; (4) is data on the risk ratio or odds ratio between obesity and incidence of any one or more of the 13 cancers in adults aged
- 40. 18 years and over provided. Both reviewers independently assessed each study for relevance and met to resolve discrep- ancies through discussion. All articles referring to the same study were considered as one study. 2.3. Methodological Quality Assessment. All studies judged to be relevant were assessed for methodological quality by two independent reviewers using an existing quality assessment tool, based on the work of the Evidence-based Medicine group at McMaster University. The assessment criteria con- sisted of the following components: (1) research design; (2) identification of comparison groups, (3) comparison groups compared on important confounders at baseline, (4) out- comes and exposures measured in the same way in all groups being compared, (5) data collection tools shown to be valid, (6) data collection tools shown to be reliable, (7) follow up sufficiently long for the outcome(s) of interest; (8) com- pleteness of followup, (9) temporality (exposure is known to precede outcome), (10) dose-response gradient, (11) signifi- cant baseline differences controlled for in the analysis, (12) appropriate statistical tests for the research design, (13) pre- cision of estimate of effect, and (14) sufficient detail describ- ing study participants. Points were assigned to each criterion according to an a priori scale. Studies were given an overall score out of 20 possible points and were then classified into three categories: strong, moderate, and weak. Studies receiving an overall rating of 16 ormore points were rated as strong.Those obtain- ing a score of 11–15 points received a rating of moderate, and those obtaining a score of 10 or less were rated as weak. Reviewers independently rated each study andmet to resolve discrepancies in overall ratings through discussion. Stud- ies deemed as being of weak methodological quality were excluded from further analysis as the validity of the results was questionable given themany limitations inherent in these
- 41. studies. 2.4. Data Extraction. Data on the population, studymethods, and outcomeswere extracted for each study independently by two reviewers. Discrepancies were resolved through discus- sion. 2.5. Data Analysis. Estimates of association were measured as a risk ratio and meta-analysis performed as a weighted average of the log risk ratios and 95% confidence intervals. In instances where odds ratios were reported for primary studies (e.g., case-control studies) these were first converted into risk ratios as suggested by Renehan et al., and then the log risk ratios and coinciding 95% confidence intervals were calculated. Tests of heterogeneity were conducted among studies using a Chi square procedure, where� < 0.05was considered ISRN Preventive Medicine 3 Search strategy development Electronic database (1723)Original lancet review (141) Review reference lists (69) Relevance assessment of full documents (202) = 101 unique studies 3 studies excluded: outcomes reported on subgroups Quality assessment of relevant studies (98 projects)
- 42. Weak project accounts removed based on quality assessment (41) Colon (26) Endometrial (17) Esophageal (7) Gallbladder (5) Leukemia (4) Malignant melanoma (7) Non-hodgkin lymphoma (14) Rectal (19) Thyroid (7)Postmenopausal breast (27) Renal (7)Pancreatic (23) Multiple myeloma (7) Data extraction from relevant project accounts (57) (1 strong; 56 moderate) Figure 1: Overview of review process. an indication of heterogeneity. Risk ratios were pooled using the DerSimonian and Laird random effects model, given that there was considerable variation in how independent and
- 43. dependent variables were measured across studies, and because in most cases statistically significant heterogeneity across study results was observed. Risk ratios/odds ratios and 95% confidence intervals extracted from each primary study, where those that adjusted for the greatest number of confounding variables including behavioural factors. Anal- yses were performed and reported separately by sex. In all instances reference body mass index (BMI) was 18.5–24.99 which was compared to the BMI category of 30 or more. 2.6. Population-Attributable Risk. Population-attributable risk (PAR) is the portion of the incidence of a disease in the population that is due to exposure. PAR% is the percent of the incidence of a disease in the population that is due to exposure. It is the percent of the incidence of the disease in the population that would be eliminated if exposure was eliminated. PAR% = [P(RR − 1)]/[1 + P(RR − 1)], where, P is the population prevalence of obesity, and RR is the pooled risk ratio [12]. The most current obesity rates for men and women available in Canada [9] were used to represent population prevalence. The same formula was used to com- pute the 95% confidence interval of PAR%. 3. Results 3.1. Search Results. In total 141 articles were identified from Renehan et al., 1723 from the database searches and 69 from reference lists; the total is 1933 papers. Of the 141 articles included in Renehan et al., 94 articles were relevant to the 13 cancers included in this paper. The remaining 47 articles from Renehan et al’s review explored the association between 4 ISRN Preventive Medicine
- 44. obesity and cancers other than the thirteen of interest in this paper, and therefore were excluded. Of the 1723 articles identified in the database searches, 75 were judged to be rele- vant. Finally, of the 69 articles identified from the reference lists of relevant studies, 33 were deemed relevant. A total of 202 articles were deemed relevant for this paper. When papers were grouped according to independent studies, a total of 101 unique studies were relevant. The Kappa score for agreement between reviewers on relevance assessment was 0.835, indicating high agreement. Reasons studies found to be not relevant were data not reported on the 13 cancers, and/or the association between obesity and cancer in adults aged 18 years and older was not the focus of the study. 3.2. Methodological Quality Assessment. One hundred and one studies were assessed for methodological quality. It was identified during quality assessment that three studies (judged to be of moderate quality) reported data in a way that was inconsistent with the other studies, therefore could not be aggregated with other studies.These studies were excluded from the meta-analysis. Of the remaining 98 studies one was assessed as being of strong methodological quality, 56 were rated as moderate and 41 as weak. Data was extracted on the 57 strong and moderate studies. The following criteria distinguished strong andmoderate studies fromweak studies: strong andmoderate studies tended to usemeasurement tools with proven validity and reliability, demonstrated that obesity preceded cancer incidence, and established a dose-response gradient. Studies of weakmethodological quality rated poorly on these criteria as well as research design. A summary of the quality assessment of the 57 studies included in the meta- analysis is presented in Figure 1. Quality assessment of the weak studies not included in this publication can be requested from the primary author.
- 45. 3.3. Study Characteristics. The study designs included 43 cohort and 14 case-control studies published between 1985 and 2011. The majority of studies were conducted in the United States (19), followed by Sweden (7), Norway (4), and Japan (5). Most studies had follow-up rates of 80% or greater. Education level ranged from primary school to postsec- ondary. Among the cohort studies participants were followed up between 6 and 39 years. 3.4. Association between Obesity and Cancer Incidence 3.4.1. Colon Cancer. Sixteen studies were included in the meta-analysis assessing the association between obesity and colon cancer among men (Figure 2(a)) and 13 studies among women (Figure 2(b)). The pooled risk ratio illustrated that obese men had an increased risk of colon cancer compared to men of normal weight (RR 1.57; 95% confidence interval 1.48 to 1.65).There was no significant heterogeneity across studies (heterogeneity� = 0.68).Thepooled risk ratio illustrated that obesewomen had an increased risk of colon cancer compared to women of normal weight (RR 1.19; 95% confidence interval 1.04 to 1.36). There was significant heterogeneity observed across studies (heterogeneity � = 0.08). 3.4.2. Endometrial Cancer. The pooled risk ratio from 16 studies illustrated that obese women had an increased risk of endometrial cancer compared to women of normal weight (RR 1.85; 95% confidence interval 1.3 to 2.65) (Figure 3).There was significant heterogeneity across studies (heterogeneity � = 0.00001). 3.4.3. Esophageal Adenocarcinoma. There were 3 studies that assessed the association between obesity and esophageal adenocarcinoma in men (Figure 4(a)) and 4 studies among women (Figure 4(b)). The pooled risk ratio demonstrated that obese men did not have an increased risk for esophageal
- 46. adenocarcinoma compared to men of normal weight (RR 1.23; 95% confidence interval 0.58 to 2.60). There was sig- nificant heterogeneity across studies (heterogeneity � = 0.02). Among obese women, however, the pooled risk ratio indicated a sizable increased risk of esophageal adenocar- cinoma compared to women of normal weight (RR 2.04; 95% confidence interval 1.18 to 3.55). There was significant heterogeneity across studies (heterogeneity � = 0.003). 3.4.4. Gallbladder Cancer. Therewere 3 studies each assessing the association between obesity and gallbladder cancer in men (Figure 5(a)) and women (Figure 5(b)). The pooled risk ratio illustrated that obese men had an increased risk of gallbladder cancer compared to normal weight men (RR 1.47; 95% confidence interval 1.17 to 1.85).There was no significant heterogeneity across studies (heterogeneity � = 0.77). Simi- larly, among obesewomen the pooled risk ratio demonstrated an increased risk of gallbladder cancer compared towomenof normal weight (RR 1.82; 95% confidence interval 1.32 to 2.50). There was no significant heterogeneity across studies (hetero- geneity � = 0.15). 3.4.5. Leukemia. There were 2 studies that assessed the association between obesity and leukemia among men (Figure 6(a)) and women (Figure 6(b)). The pooled risk ratio illustrated that obese men had no increased risk of leukemia compared to men of normal weight (RR 1.16; 95% confidence interval 0.88 to 1.52). For obese women, however, the pooled risk ratio illustrated an increased risk of leukemia compared to women of normal weight (RR 1.32; 95% confidence interval 1.08 to 1.60). There was no significant heterogeneity across studies for either men or women. 3.4.6.MalignantMelanoma. Four studies assessed the associ- ation between obesity and malignant melanoma among men (Figure 7(a)) and 3 among women (Figure 7(b)). The pooled
- 47. risk ratio illustrated that obese men had an increased risk of malignant melanoma compared to men of normal weight (RR 1.26; 95% confidence interval 1.07 to 1.48). There was no significant heterogeneity across studies (heterogeneity � = 0.28). The pooled risk ratio for obese women showed no increased risk of malignant melanoma compared to women of normal weight (RR 0.95; 95% confidence interval 0.84 to 1.07). There was no significant heterogeneity across studies (heterogeneity � = 0.83). ISRN Preventive Medicine 5 Study or subgroup Log (risk ratio) 0.79299 0.712949 0.42527 0.39878 1.08181 0.4947 0.262364 0.47 0.412 0.48858 0.65233 0.33646 0.44469 0.55389 0.57661 0.35066 SE
- 49. 1.1% 0.6% 2.0% 12.1% 2.4% 2.8% IV, random, 95% CI 2.21 [1.29, 3.78] 2.04 [1.56, 2.66] 1.53 [1.23, 1.90] 1.49 [1.39, 1.60] 2.95 [1.00, 8.74] 1.64 [0.92, 2.92] 1.30 [0.31, 5.37] 1.60 [1.03, 2.48] 1.51 [1.00, 2.28] 1.63 [0.87, 3.04] 1.92 [1.14, 3.22] 1.40 [0.70, 2.80] 1.56 [1.06, 2.30] 1.74 [1.48, 2.04] 1.78 [1.24, 2.55] 1.42 [1.02, 1.98] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 15.88 (� < 0.00001) Total (95% CI) 100.0% 1.57 [1.48, 1.65] Heterogeneity: �2 = 0.00; �2 = 12.01, df = 15 (� = 0.68); �2 = 0%
- 50. Batty et al. (2009) Campbell et al. (2007) Chang et al. (2006, 2007) Engeland et al. (2004) Ford (1999) Gaard et al. (1997) Kuriyama et al. (2005) Larsson et al. (2005) MacInnis et al. (2004, 2006) Nock et al. (2008) Oh et al. (2005) Otani et al. (2005) Rapp et al. (2005) Samanic et al. (2006) Sun et al. (2008) Stolzenberg-Solomon et al. (2002, 2008) (a) Study or subgroup Log (risk ratio) 0.343589 0.2469 0.06766 1.0079 0.0198 0.8109 0.5481 0 0.4121 0.0099
- 52. 1.41 [0.89, 2.23] 1.28 [0.97, 1.69] 1.07 [1.02, 1.12] 2.74 [1.04, 7.24] 1.02 [0.53, 1.97] 2.25 [0.95, 5.33] 1.73 [1.05, 2.85] 1.00 [0.69, 1.44] 1.51 [0.86, 2.64] 0.50 [0.18, 1.40] 1.01 [0.72, 1.42] 1.52 [1.00, 2.31] 0.95 [0.67, 1.34] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 −0.6931 −0.0513 Test for overall effect: � = 2.54 (� = 0.01) Total (95% CI) 100.0% 1.19 [1.04, 1.36] Heterogeneity: �2 = 0.02; �2 = 19.57, df = 12 (� = 0.08); �2 = 39% Bostwik et al. (1994) Chang et al. (2006, 2007) Engeland et al. (2004) Ford (1999) Gaard et al. (1997) Kuriyama et al. (2005)
- 53. Lin et al. (2004) MacInnis et al. (2004, 2006) Nock et al. (2008) Otani et al. (2005) Sun et al. (2008) Suzuki et al. (2006) Terry et al. (2001, 2002) (b) Figure 2: (a) Obesity and colon cancer in men. (b) Obesity and colon cancer in women. 3.4.7. Multiple Myeloma. Only one study for men (Figure 8(a)) and two studies for women (Figure 8(b)) assessed the association between obesity and multiple myeloma.The results reported by Samanic et al., 2006 showed obese men had significantly lower risk of multiple myeloma compared tomen of normal weight (RR 0.58; 95% confidence interval 0.36 to 0.93). The pooled ratio for women showed an increased risk of multiple myeloma compared to women of normal weight, although the 95% confidence interval was just short of reaching statistical significance (RR 1.20; 95% confidence interval 0.99 to 1.45). There was no significant heterogeneity across the two studies (heterogeneity� = 0.39). 3.4.8. Non-Hodgkin Lymphoma. Four studies in men (Figure 9(a)) and six in women (Figure 9(b)) assessed the 6 ISRN Preventive Medicine Study or subgroup
- 54. Bostwik et al. (1994) 0.912 1.10856 0.92028 1.1848 0.9439 0.833 1.396 0.519 0.5068 1.264 1.0043 1.2238 SE 0.187 0.099 0.0296 0.182 0.238 0.229 0.6471 0.03 0.121 0.227 0.137 0.0342 0.08977
- 55. 0.124 0.059 0.0593 Weight 6.2% 6.5% 6.7% 6.3% 6.0% 6.0% 3.6% 6.7% 6.5% 6.1% 6.4% 6.7% 6.6% 6.5% 6.6% 6.6% IV, random, 95% CI 2.49 [1.73, 3.59] 3.03 [2.50, 3.68] 2.51 [2.37, 2.66] 3.27 [2.29, 4.67] 2.57 [1.61, 4.10] 2.30 [1.47, 3.60] 4.04 [1.14, 14.36] 0.80 [0.76, 0.85] 1.68 [1.33, 2.13]
- 56. 1.66 [1.06, 2.59] 3.54 [2.71, 4.63] 2.73 [2.55, 2.92] 0.68 [0.57, 0.81] 3.40 [2.67, 4.34] 0.70 [0.62, 0.78] 0.60 [0.53, 0.67] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 −0.219 −0.3895 −0.361 −0.5108 Log (risk ratio) Test for overall effect: � = 3.38 (� = 0.0007) Total (95% CI) 100.0% 1.85 [1.30, 2.65] Heterogeneity: �2 = 0.50; �2 = 16.9827, df = 15 (� < 0.00001); �2 = 99% Chang et al. (2006, 2007) Gaard et al. (1997) Engeland et al. (2004) Feigelson et al. (2004)
- 57. Kawai et al. (2011) Kuriyama et al. (2005) Maso et al. (2011) Morimoto et al. (2002) Nilsen and Vatten (2000) Park et al. (2010) Reeves et al. (2007, 2011) Terry et al. (2001, 2002) Thomas et al. (2009) Yong et al. (1996) Salazar-Martinez et al. (2000) Figure 3: Obesity and endometrial cancer. −0.6349 Study or subgroup Log (risk ratio) 0.04879 1.0006 SE 0.113 0.3639 0.582 Weight 44.9%
- 58. 32.8% 22.4% IV, random, 95% CI 1.05 [0.84, 1.31] 2.72 [1.33, 5.55] 0.53 [0.17, 1.66] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Total (95% CI) 100.0% 1.23 [0.58, 2.60] Heterogeneity: �2 = 0.31; �2 = 7.92, df = 2 (� = 0.02); �2 = 75% Engeland et al. (2004) Samanic et al. (2006) Sun et al. (2008) Test for overall effect: � = 0.54 (� = 0.59) (a) Study or subgroup Log (risk ratio) 0.248
- 59. 1.3083 0.9322 0.89199 SE 0.126 0.617 0.15 0.8 Weight 38.9% 13.9% 37.7% 9.6% IV, random, 95% CI 1.28 [1.00, 1.64] 3.70 [1.10, 12.40] 2.54 [1.89, 3.41] 2.44 [0.51, 11.70]
- 60. Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 2.54 (� = 0.01) Total (95% CI) 100.0% 2.04 [1.18, 3.55] Heterogeneity: �2 = 0.19; �2 = 13.93, df = 3 (� = 0.003); �2 = 78% Engeland et al. (2004) MacInnis et al. (2004, 2006) Reeves et al. (2007, 2011) Sun et al. (2008) (b) Figure 4: (a) Obesity and esophageal adenocarcinoma in men. (b) Obesity and esophageal adenocarcinoma in women. ISRN Preventive Medicine 7 Study or subgroup Log (risk ratio) 0.32208 0.33647 0.50077
- 61. SE 0.16 0.335 0.2 Weight 53.5% 12.2% 34.3% IV, random, 95% CI 1.38 [1.01, 1.89] 1.40 [0.73, 2.70] 1.65 [1.11, 2.44] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 2 5 10 Test for overall effect: � = 3.29 (� = 0.001) Total (95% CI) 100.0% 1.47 [1.17, 1.85] Heterogeneity: �2 = 0.00; �2 = 0.51, df = 2 (� = 0.77); �2 = 0% Engeland et al. (2004)
- 62. Samanic et al. (2006) Sun et al. (2008) (a) Study or subgroup Log (risk ratio) 0.63217 1.4929 0.3646 SE 0.083 0.593 0.197 Weight 58.9% 6.8% 34.3% IV, random, 95% CI 1.88 [1.60, 2.21] 4.45 [1.39, 14.23]
- 63. 1.44 [0.98, 2.12] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 3.69 (� = 0.0002) Total (95% CI) 100.0% 1.82 [1.32, 2.50] Heterogeneity: �2 = 0.04; �2 = 3.84, df = 2 (� = 0.15); �2 = 48% Engeland et al. (2004) Kuriyama et al. (2005) Sun et al. (2008) (b) Figure 5: (a) Obesity and gallbladder cancer in men. (b) Obesity and gallbladder cancer in women. association between obesity and non-Hodgkin lymphoma. The pooled risk ratio indicated there was no increased risk of non-Hodgkin lymphoma among obese men compared to men of normal weight (RR 1.09; 95% confidence interval 0.98 to 1.21). There was no significant heterogeneity across studies (heterogeneity � = 0.46). Among obese women, however, the pooled risk ratio showed a reduced risk of non-Hodgkin lymphoma compared to women of normal weight (RR 0.91; 95% confidence interval 0.86 to 0.97). There was significant heterogeneity across studies (heterogeneity � = 0.0001).
- 64. 3.4.9. Pancreatic Cancer. Nine and ten studies, respectively, assessed the association between obesity and pancreatic cancer in men (Figure 10(a)) and women (Figure 10(b)). The pooled risk ratio illustrated that obese men had an increased risk of pancreatic cancer compared to men of normal weight (RR 1.36; 95% confidence interval 1.07 to 1.73). There was significant heterogeneity across studies (heterogeneity � = 0.01). Among obese women the pooled risk ratio also showed an increased risk of pancreatic cancer compared to women of normal weight (RR 1.34; 95% confidence interval 1.22 to 1.46). There was no significant heterogeneity across studies (heterogeneity � = 0.81). 3.4.10. Postmenopausal Breast Cancer. Eleven studies assess- ed the association between obesity and postmenopausal breast cancer (Figure 11). The pooled risk ratio demonstrated that obese women had an increased risk of postmenopausal breast cancer compared towomenof normalweight (RR, 1.25; 95% confidence interval 1.07 to 1.46). There was significant heterogeneity across studies (heterogeneity � = 0.0001). 3.4.11. Rectal Cancer. There were 11 studies for men (Figure 12(a)) and nine for women (Figure 12(b)) that assess- ed the association between obesity and rectal cancer. The pooled risk ratio illustrated that obese men had no increased risk of rectal cancer compared to men of normal weight (RR 1.22; 95% confidence interval 0.91 to 1.64). There was significant heterogeneity across studies (heterogeneity � = 0.00001). Similarly among obese women the pooled risk ratio illustrated no increased risk of rectal cancer compared to women of normal weight (RR 1.03; 95% confidence interval 0.74 to 1.44). There was significant heterogeneity across studies (heterogeneity � = 0.00001). 3.4.12. Renal Cancer. There were 3 studies each for men
- 65. (Figure 13(a)) and women (Figure 13(b)) that assessed the association between obesity and renal cancer. The pooled risk ratio illustrated that obese men had an increased risk of renal cancer compared to men of normal weight (RR 1.57; 95% confidence interval 1.38 to 1.77).There was no significant heterogeneity across studies (� = 0.76). Similarly, among 8 ISRN Preventive Medicine Study or subgroup Total (95% CI) Log (risk ratio) 0.70803 0.11333 SE 0.589 0.142 Weight 5.5% 94.5% 100.0% IV, random, 95% CI
- 66. 2.03 [0.64, 6.44] 1.12 [0.85, 1.48] 1.16 [0.88, 1.52] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 1.06 (� = 0.29) Heterogeneity: �2 = 0.00; �2 = 0.96, df = 1 (� = 0.33); �2 = 0% Oh et al. (2005) Samanic et al. (2006) (a) Study or subgroup Total (95% CI) Log (risk ratio) 0.47 0.22314 SE 0.20687 0.086
- 67. Weight 21.0% 79.0% 100.0% IV, random, 95% CI 1.60 [1.07, 2.40] 1.25 [1.06, 1.48] 1.32 [1.08, 1.60] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 2.74 (� = 0.006) Heterogeneity: �2 = 0.01; �2 = 1.21, df = 1 (� = 0.27); �2 = 18% Bostwik et al. (1994) Reeves et al. (2007, 2011) (b) Figure 6: (a) Obesity and leukemia in men. (b) Obesity and leukemia in women. −0.5276 Study or subgroup Total (95% CI)
- 68. 0.3365 0.2397 0.3001 SE 0.54821 0.057 0.407 0.127 Weight 2.1% 65.4% 3.8% 28.7% 100.0% IV, random, 95% CI 1.40 [0.48, 4.10] 1.27 [1.14, 1.42] 0.59 [0.27, 1.31] 1.35 [1.05, 1.73] 1.26 [1.07, 1.48] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10
- 69. Log (risk ratio) Test for overall effect: � = 2.83 (� = 0.005) Heterogeneity: �2 = 0.01; �2 = 3.81, df = 3 (� = 0.28); �2 = 21% Freedman et al. (2003) Odenbro et al. (2007) Rapp et al. (2005) Samanic et al. (2006) (a) Study or subgroup Total (95% CI) Log (risk ratio) 0.049 SE 0.225 0.185 0.066 Weight 7.1% 10.5% 82.4% 100.0%
- 70. IV, random, 95% CI 0.90 [0.58, 1.40] 1.05 [0.73, 1.51] 0.94 [0.83, 1.07] 0.95 [0.84, 1.07] Risk ratio Risk Ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 −0.10536 −0.061875 Test for overall effect: � = 0.89 (� = 0.37) Heterogeneity: �2 = 0.00; �2 = 0.38, df = 2 (� = 0.83); �2 = 0% Freedman et al. (2003) Huang et al. (1997) Reeves et al. (2007, 2011) (b) Figure 7: (a) Obesity and malignant melanoma in men. (b) Obesity and malignant melanoma in women. ISRN Preventive Medicine 9
- 71. Study or subgroup Samanic et al. (2006) Total (95% CI) Log (risk ratio) SE 0.241 Weight 100.0% 100.0% 0.58 [0.36, 0.93] 0.58 [0.36, 0.93] Risk ratio Risk ratio IV, fixed, 95% CI 0.1 0.2 0.5 1 2 5 10 IV, fixed, 95% CI −0.54473 Heterogeneity: not applicable Test for overall effect: � = 2.26 (� = 0.02) (a) Study or subgroup
- 72. Bostwik et al. (1994) Reeves et al. (2007, 2011) Total (95% CI) Log (risk ratio) 0.4054 0.14842 SE 0.2806 0.104 Weight 12.1% 87.9% 100.0% IV, random, 95% CI 1.50 [0.87, 2.60] 1.16 [0.95, 1.42] 1.20 [0.99, 1.45] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 1.84 (� = 0.07)
- 73. Heterogeneity: �2 = 0.00; �2 = 0.74, df = 1 (� = 0.39); �2 = 0% (b) Figure 8: (a) Obesity and multiple myeloma in men. (b) Obesity and multiple myeloma in women. Table 1: Summary of results of meta-analysis of associations bet- ween obesity and cancer risk in 57 studies from 18 countries, 1985– 2011. Cancer Males Females RR and 95% CI RR and 95% CI Colon 1.57 (1.48, 1.65)∗ 1.19 (1.04, 1.36)∗ Endometrial NA 1.85 (1.30, 2.65)∗ Esophageal 1.23 (0.58, 2.60) 2.04 (1.18, 3.55)∗ Gallbladder 1.47 (1.17, 1.85)∗ 1.82 (1.32, 2.50)∗ Leukemia 1.16 (0.88, 1.52) 1.32 (1.08, 1.60)∗ Malignant melanoma 1.26 (1.07, 1.48)∗ 0.95 (0.84, 1.07) Multiple myeloma 0.58 (0.36, 0.93)∗ 1.20 (0.99, 1.45) Non-Hodgkins lymphoma 1.09 (0.98, 1.21) 0.91 (0.86, 0.97)∗ Pancreatic 1.36 (1.07, 1.73)∗ 1.34 (1.22, 1.46)∗ Postmenopausal breast NA 1.25 (1.07, 1.46)∗ Rectal 1.22 (0.91, 1.64) 1.03 (0.74, 1.44)
- 74. Renal 1.57 (1.38, 1.77)∗ 1.72 (1.58, 1.88)∗ Thyroid 1.12 (0.72, 1,72) 1.03 (0.87, 1.23) ∗ Statistically significant at � < 0.05. obese women the pooled risk ratio illustrated an increased risk of renal cancer compared to women of normal weight (RR 1.72; 95% confidence interval 1.58 to 1.88). There was no significant heterogeneity across studies (heterogeneity � = 0.22). 3.4.13. Thyroid Cancer. There were 6 studies included in the meta-analysis assessing the association between obesity and thyroid cancer among men (Figure 14(a)) and 4 studies among women (Figure 14(b)). The pooled risk ratio illus- trated that obese men had no increased risk of thyroid cancer compared to men of normal weight (RR 1.12; 95% confidence interval 0.72 to 1.72). There was significant heterogeneity across studies (� < 0.00001). Likewise, among obese women the pooled risk ratio demonstrated no increased risk of thy- roid cancer compared to women of normal weight (RR 1.03; 95% confidence interval 0.87 to 1.23). There was significant heterogeneity across studies (� < 0.004). 3.4.14. Results Summary. Table 1 summarizes the results of the observed associations between obesity and the 13 cancers included in this meta-analysis. Among men a statistically significant increased risk of cancer was observed for the following 5 cancers: colon, gallbladder, malignantmelanoma, pancreatic, and renal cancer. In addition, obese men had significantly lower risk of multiple myeloma in comparison to men of normal weight. Among women a statistically signi- ficant increased risk of cancer was observed for the follow- ing 8 cancers: colon, endometrial, esophageal, gallbladder, leukemia, pancreatic, postmenopausal breast, and renal.
- 75. Obese women also had significantly lower risk of non-Hodg- kin lymphoma compared to women of normal weight. 3.4.15. Population-Attributable Risk. As an example to illus- trate the use of meta-analysis results reported in this study, the PAR% for men and women in Canada was calculated on cancers for which a statistically significant association 10 ISRN Preventive Medicine Study or subgroup Engeland et al. (2004) Fernberg et al. (2007) Rapp et al. (2005) Samanic et al. (2006) Log (risk ratio) 0.1484 0.0198 SE 0.066 0.1234 0.4
- 76. 0.128 Weight 63.3% 18.1% 1.7% 16.8% IV, fixed, 95% CI 1.16 [1.02, 1.32] 0.95 [0.75, 1.21] 0.91 [0.42, 1.99] 1.02 [0.79, 1.31] Risk ratio Risk ratio IV, fixed, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 1.64 (� = 0.10) −0.0513 −0.0943 Total (95% CI) 100.0% 1.09 [0.98, 1.21] Heterogeneity: �2 = 2.60, df = 3 (� = 0.46); �2 = 0%
- 77. (a) Study or subgroup Bostwik et al. (1994) Engeland et al. (2004) Fernberg et al. (2007) Lu (2009) Reeves et al. (2007, 2011) Wu et al. (2007) Log (risk ratio) 0 0.06766 0.4574 0.174 0.17395 SE 0.171 0.0499 0.449 0.125 0.061 0.065 Weight 3.4% 39.8% 0.5% 6.3%
- 78. 26.6% 23.4% IV, fixed, 95% CI 1.00 [0.72, 1.40] 1.07 [0.97, 1.18] 1.58 [0.66, 3.81] 1.19 [0.93, 1.52] 1.19 [1.06, 1.34] 0.47 [0.41, 0.53] Risk ratio Risk ratio IV, fixed, 95% CI 0.1 0.2 0.5 1 2 5 10 Favours experimental Favours control Test for overall effect: � = 2.86 (� = 0.004) −0.75311 Total (95% CI) 100.0% 0.91 [0.86, 0.97] Heterogeneity: �2 = 139.00, df = 5 (� < 0.00001); �2 = 96% (b) Figure 9: (a) Obesity and non-Hodgkin lymphoma in men. (b) Obesity and non-Hodgkin lymphoma in women. between obesity and cancer incidencewas observed (Table 2). The population prevalence of obesity in Canada in 2002 was 22.9% in men and 23.2% in women. Among men PAR% ranged from a low of 5.6% to a high of 11.5%. The PAR% for obesity among men was greatest for colon and renal cancer (11.5%), gallbladder cancer (9.7%), pancreatic (7.6%), and
- 79. malignant melanoma (5.6%). When the 95% confidence intervals for PAR% for men are considered the results are particularly noteworthy. For example for colon cancer PAR% is as low as 9.9% but at the upper limit of the confidence inter- val PAR% is 13.1%. Likewise, for renal cancer the 95% con- fidence interval for PAR% ranged from 8.0% to 15%, while for pancreatic cancer, it ranged from 1.6% to 17.5%, and 1.6% to 9.9% for malignant melanoma. Among women PAR% ranged from a low of 4.2% to a high of 19.4%. The PAR% for obesity among women was greatest for esophageal adenocarcinoma (19.4%), endometrial (16.5%), gallbladder (16%), and renal cancer (14.3). When the 95%confidence intervals for PAR% forwomen are considered the results are also noteworthy. For example, at the upper limit of the confidence interval, PAR%was as high as 37.2% for esophageal adenocarcinoma, 27.7% for endometrial cancer, and 25.8% for gallbladder cancer. However, at the lower limit the PAR% was as low as 0.9% for colon cancer, 1.6% for postmenopausal breast cancer, and 1.8% for malignant melanoma. 4. Discussion The results of this meta-analysis demonstrate a significant association between obesity and some of the 13 cancers for men and many of the 13 cancers for women. Obesity was significantly and positively associated with 5 of the possible 11 cancers relevant to men including, colon, gall- bladder, malignant melanoma, pancreatic, and renal. A sig- nificant association was not observed among obese men for esophageal adenocarcinoma, leukemia, multiple myeloma, non-Hodgkin lymphoma, rectal, and thyroid cancer. Among women obesity was significantly and positively associated with 8 of the 13 cancers including, colon, endometrial,
- 80. esophageal adenocarcinoma, gallbladder, leukemia, pancre- atic, postmenopausal breast, and renal cancer. A significant association was not observed among women for malignant melanoma,multiplemyeloma, non-Hodgkin lymphoma, rec- tal cancer, and thyroid cancer. ISRN Preventive Medicine 11 Study or subgroup Batty et al. (2009) Chang et al. (2006, 2007) Feigelson et al. (2004) Larsson et al. (2005) Oh et al. (2005) Otani et al. (2005) Rapp et al. (2005) Samanic et al. (2006) Sun et al. (2008) Suzuki et al. (2006) Total (95% CI) Log (risk ratio) 0.1655 0.039 0.8671 0.73237 0.03922 0.85015 0.14842
- 81. 0.29267 0.73237 SE 0.201 0.159 0.236 0.365 0.507 0.275 0.351 0.141 0.293 0.365 Weight 12.8% 14.8% 11.4% 7.2% 4.5% 9.9% 7.5% 15.6% 9.2% 7.2% 100.0% IV, random, 95% CI 1.18 [0.80, 1.75] 1.04 [0.76, 1.42]
- 82. 2.38 [1.50, 3.78] 2.08 [1.02, 4.25] 1.04 [0.39, 2.81] 0.70 [0.41, 1.20] 2.34 [1.18, 4.66] 1.16 [0.88, 1.53] 1.34 [0.75, 2.38] 2.08 [1.02, 4.25] 1.36 [1.07, 1.73] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 2.54 (� = 0.01) −0.35667 Heterogeneity: �2 = 0.08; �2 = 20.77, df = 9 (� = 0.01); �2 = 57% (a) Study or subgroup Bostwik et al. (1994) Chang et al. (2006, 2007) Feigelson et al. (2004) Larsson et al. (2005) Morimoto et al. (2002) Otani et al. (2005) Reeves et al. (2007, 2011) Stevens et al. (2009) Sun et al. (2008) Suzuki et al. (2006)
- 83. Total (95% CI) Log (risk ratio) 0.13103 0.285 0.54812 0.39204 0.0953 0.18232 0.3148 0.293 0.5878 0.39204 SE 0.179 0.201 0.267 0.456 0.15825 0.234 0.079 0.081 0.236 0.456 Weight 6.7%
- 84. 5.3% 3.0% 1.0% 8.5% 3.9% 34.2% 32.5% 3.8% 1.0% 100.0% IV, random, 95% CI 1.14 [0.80, 1.62] 1.33 [0.90, 1.97] 1.73 [1.03, 2.92] 1.48 [0.61, 3.62] 1.10 [0.81, 1.50] 1.20 [0.76, 1.90] 1.37 [1.17, 1.60] 1.34 [1.14, 1.57] 1.80 [1.13, 2.86] 1.48 [0.61, 3.62] 1.34 [1.22, 1.46] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 6.26 (� < 0.00001) Heterogeneity: �2 = 0.00; �2 = 5.24, df = 9 (� = 0.81); �2 = 0%
- 85. (b) Figure 10: (a) Obesity and pancreatic cancer in men. (b) Obesity and pancreatic cancer in women. The magnitude of the associations between obesity and cancer incidence in men and women, including the 95% confidence intervals, is particularly noteworthy. For example, obese men have an increased risk of developing colon and renal (RR both 1.57), gallbladder (1.47), pancreatic cancer (1.36), and malignant melanoma (1.26) in comparison to nonobese men. When the 95% confidence intervals are considered the results become even more compelling. For example the risk ratio is as high as 1.77 for renal cancer, 1.73 for pancreatic cancer and 1.65 for colon cancer. Even at the low end of the 95% confidence interval, cancer risk is still noteworthy at 1.48 for colon cancer, and 1.38 for renal cancer. The results for obese women are equally concerning. Obese women are not only at higher risk for developing cancer at more sites than men, the risk associated with some of the cancers is significantly higher. For example, obese women have an increased risk for developing esophageal adenocarcinoma (RR 2.04), endometrial (1.85), gallbladder (1.82), and renal cancer (1.72). Where statistically significant associations are observed only one risk ratio is less than 20% (colon 1.19), while the remaining risk ratios range between 1.25 (postmenopausal breast), 1.32 (leukemia), and 1.34 (pan- creatic). The 95% confidence intervals are also alarming. For example, at the upper limit of the confidence interval the risk ratio is as high as 3.55 for esophageal adenocarcinoma, 2.65 for endometrial, and 2.50 for gallbladder cancer. The results also clearly demonstrate that a significant
- 86. proportion of cancer incidence could be avoided, in Canada, by reducing the percentage of obese adults. The population- attributable risk percent for obesity in Canada was highest 12 ISRN Preventive Medicine Study or subgroup Chang et al. (2006, 2007) Huang et al. (1997) Kuriyama et al. (2005) Lin et al. (2004) Lundqvist et al. (2007) MacInnis et al. (2004, 2006) Montazeri et al. (2008) Otani et al. (2005) Reeves et al. (2007, 2011) Tehard and Clavel-Chapelon (2006) Terry et al. (2001, 2002) Total (95% CI) Log (risk ratio) 0.095 0.1222 0.98208 0.68813 0.26236 0.33647 0.824175
- 88. 100.0% IV, random, 95% CI 1.10 [0.96, 1.26] 1.13 [0.87, 1.46] 2.67 [1.03, 6.92] 1.99 [1.23, 3.21] 1.30 [0.99, 1.70] 1.40 [1.03, 1.91] 0.76 [0.65, 0.89] 2.28 [0.94, 5.53] 1.29 [1.22, 1.36] 1.44 [1.04, 1.99] 1.26 [0.95, 1.67] 1.25 [1.07, 1.46] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Favours experimental Favours control −0.27119 Test for overall effect: � = 2.89 (� = 0.004) Heterogeneity: �2 = 0.04; �2 = 50.72, df = 10 (� < 0.00001); �2 = 80% Figure 11: Obesity and postmenopausal breast cancer. Table 2: Population-attributable risk percent in Canada for obesity and cancer.
- 89. Cancer Males Males Females Females RR and 95% CI Population-attributable risk Percent RR and 95% CI Population-attributable risk Percent Colon 1.57 (1.48, 1.65)∗ 11.5% (9.9, 13.1)∗ 1.19 (1.04, 1.36)∗ 4.2% (0.9, 7.7) Endometrial NA NA 1.85 (1.3, 2.65)∗ 16.5% (6.5, 27.7)∗ Esophageal 1.23 (0.58, 2.60) — 2.04 (1.18, 3.55)∗ 19.4% (4.0, 37.2)∗ Gallbladder 1.47 (1.17, 1.85)∗ 9.7% (3.7, 16.3)∗ 1.82 (1.32, 2.50)∗ 16% (6.9, 25.8)∗ Leukemia 1.16 (0.88, 1.52) — 1.32 (1.08, 1.60)∗ 6.9% (1.8, 12.2)∗ Malignant melanoma 1.26 (1.07, 1.48)∗ 5.6% (1.6, 9.9)∗ 0.95 (0.84, 1.07) — Multiple myeloma 0.58 (0.36, 0.93)∗ — 1.20 (0.99, 1.45) — Non-Hodgkin lymphoma 1.09 (0.98, 1.21) — 0.91 (0.86, 0.97)∗ Pancreatic 1.36 (1.07, 1.73)∗ 7.6% (1.6, 17.5)∗ 1.34 (1.22, 1.46)∗ 7.3% (4.9, 9.6)∗ Postmenopausal breast NA NA 1.25 (1.07, 1.46)∗ 5.5% (1.6, 9.6)∗ Rectal 1.22 (0.91, 1.64) — 1.03 (0.74, 1.44) — Renal 1.57 (1.38, 1.77)∗ 11.5% (8.0, 15.0)∗ 1.72 (1.58, 1.88)∗
- 90. 14.3% (12.0, 16.9)∗ Thyroid 1.12 (0.72, 172) — 1.03 (0.87, 1.23) — ∗ Statistically significant at � < 0.05. in men for five cancers: colon, renal, gallbladder, pancreatic, and malignant melanoma. Significant reductions in obesity therefore would dramatically decrease the incidence of those cancers. For women the greatest benefits from obesity reduc- tion and prevention efforts would be observed for esophageal adenocarcinoma, endometrial, gallbladder, renal, pancreatic, leukemia, postmenopausal breast, and colon cancer. Signif- icant reductions in these cancers for men and women in Canada would result in decreased health care expenditures and improved quality of life for many men and women in Canada. When the results of this meta-analysis are compared to those of Renehan et al. [6], who reviewed similar but earlier literature on obesity and cancer, a number of important simi- larities and differences are observed. First, there were some differences in the associations found between the two meta- analyses for men. Renehan et al. reported a significant and positive association for the following five cancers that was not ISRN Preventive Medicine 13 Study or subgroup Campbell et al. (2007) Chang et al. (2006, 2007) Engeland et al. (2004) Kuriyama et al. (2005)
- 91. Larsson et al. (2005) MacInnis et al. (2004, 2006) Oh et al. (2005) Otani et al. (2005) Rapp et al. (2005) Samanic et al. (2006) Total (95% CI) Log (risk ratio) 0.239 0.8796 0.36464 0.262 0.07696 0.47 0.50682 0.30748 0.41211 SE 0.062 0.165 0.042 0.6025 0.303 0.3128 0.338 0.454
- 92. 0.253 0.102 0.213 Weight 12.2% 10.8% 12.3% 4.1% 8.2% 8.1% 7.6% 5.8% 9.2% 11.8% 9.9% 100.0% IV, random, 95% CI 0.59 [0.52, 0.66] 0.94 [0.68, 1.30] 1.27 [1.17, 1.38] 2.41 [0.74, 7.85] 1.30 [0.70, 2.40] 1.08 [0.56, 2.09] 1.60 [0.66, 3.90] 1.66 [1.01, 2.73] 1.36 [1.11, 1.66] 1.51 [0.99, 2.29] 1.22 [0.91, 1.64]
- 93. Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 1.35 (� = 0.18) −0.53604 −0.061875 1.44 [0.80,2.61] Stolzenberg-Solomon et al. (2002, 2008) Heterogeneity: �2 = 0.18; �2 = 126.87, df = 10 (� < 0.00001); �2 = 92% (a) Study or subgroup Campbell et al. (2007) Chang et al. (2006, 2007) Engeland et al. (2004) Kuriyama et al. (2005) Lin et al. (2004) MacInnis et al. (2004, 2006) Otani et al. (2005) Sun et al. (2008) Terry et al. (2001, 2002) Total (95% CI) Log (risk ratio)
- 95. 12.7% 100.0% IV, random, 95% CI 0.50 [0.43, 0.58] 1.09 [0.68, 1.75] 1.04 [0.97, 1.11] 1.21 [0.28, 5.14] 1.55 [0.64, 3.78] 1.10 [0.64, 1.90] 1.30 [0.55, 3.10] 1.14 [0.77, 1.68] 1.35 [0.88, 2.07] 1.03 [0.74, 1.44] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 0.20 (� = 0.84) −0.69315 Heterogeneity: �2 = 0.17; �2 = 82.56, df = 8 (� < 0.00001); �2 = 90% (b) Figure 12: (a) Obesity and rectal cancer in men. (b) Obesity and rectal cancer in women. reported in this meta-analysis: leukemia, multiple myeloma, non-Hodgkin lymphoma, rectal, and thyroid cancer. Further-
- 96. more, Renehan et al. did not report a significant and positive association for gallbladder and pancreatic cancer whereas a significant andpositive associationwas reported in this paper. There was greater similarity between the results of this paper and Renehan et al. for women. For example, there were only two cancers, multiple myeloma and thyroid cancer where Renehan et al. reported a positive and significant asso- ciation with obesity for women, and this paper did not.There were no differences for the remaining eleven cancers on the relationship between obesity and cancer in women. The second important difference between the two meta- analyses concerns the observed magnitude of the association and the coinciding 95% confidence intervals. Generally the results of our meta-analysis demonstrated higher magnitude of associations and confidence intervals. The most notable differences occurred for four cancers among men: renal, colon, pancreatic, and gallbladder cancer. For example, we reported a pooled risk ratio and 95% confidence interval of 1.57 (1.38, 1.77) for renal cancer, while Renehan et al. re- ported 1.24 (1.15, 1.34). Likewise, for colon cancer, we reported 1.57 (1.48, 1.65), while Renehan et al. reported 1.24 (1.20, 1.28), and for pancreatic cancer, we reported 1.36 (1.07, 1.73) and Renehan et al. reported 1.07 (0.93, 1.23). Finally, for gallblad- der cancer, we reported 1.47 (1.17, 1.85) while Renehan et al. reported 1.09 (0.99, 1.21). Similar differences existed for obese women with the greatest differences in the pooled risk ratios and 95% confidence intervals being for three cancers: endometrial, renal, and gallbladder. For these cancers the magnitude of associations we reported is larger than those reported by
- 97. Renehan et al. For endometrial cancer we reported a risk ratio of 1.85 (1.30, 2.65), while Renehan et al. reported 1.59 14 ISRN Preventive Medicine Study or subgroup Engeland et al. (2004) Kanda et al. (2010) Oh et al. (2005) Total (95% CI) Log (risk ratio) 0.43825 0.688 0.4967 SE 0.065 0.331 0.415 Weight 94.1% 3.6% 2.3% 100.0%
- 98. IV, random, 95% CI 1.55 [1.36, 1.76] 1.99 [1.04, 3.81] 1.64 [0.73, 3.71] 1.57 [1.38, 1.77] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Test for overall effect: � = 7.12 (� < 0.00001) Heterogeneity: �2 = 0.00; �2 = 0.56, df = 2 (� = 0.76); �2 = 0% (a) Test for overall effect: � = 12.49 (� < 0.00001) Study or subgroup Engeland et al. (2004) Kanda et al. (2010) Morimoto et al. (2002) Reeves et al. (2007, 2011) Total (95% CI) Log (risk ratio) 0.6152 0.438 0.47
- 99. 0.4187 SE 0.055 0.367 0.2069 0.078 Weight 62.9% 1.4% 4.4% 31.3% 100.0% IV, fixed, 95% CI 1.85 [1.66, 2.06] 1.55 [0.75, 3.18] 1.60 [1.07, 2.40] 1.52 [1.30, 1.77] 1.72 [1.58, 1.88] Risk ratio Risk ratio IV, fixed, 95% CI 0.1 0.2 0.5 1 2 5 10 Heterogeneity: �2 = 4.47, df = 3 (� = 0.22); �2 = 33% (b)
- 100. Figure 13: (a) Obesity and renal cancer in men. (b) Obesity and renal cancer in women. (1.5, 1.68). For renal cancer we reported 1.72 (1.58, 1.88) while Renehan reported 1.34 (1.25, 1.43), and for gallbladder cancer we reported 1.82 (1.32, 2.50) and Renehan, 1.59 (1.02, 2.47). There was only one cancer where Renehan et al. reported a larger risk ratio than we did, which was for non-Hodgkin lymphoma. There are some plausible explanations for these differ- ences. Likely the most significant factor contributing to the differences in the results of the two meta-analyses are the different approaches to the statistical methods used to aggre- gate the data across studies. The approach used by Renehan assessed the risk in developing cancer as BMI increased every 5 points, from the lowest BMI category up to the highest category. This strategy incorporates the risk of those who have a BMI slightly above normal, to above normal to those identified as obese. Given the risk of developing cancer at lower BMI levels is generally less than that of obese persons which provides some explanation why Renehan et al’s results generally illustrate lower overall risk and more narrow confi- dence intervals. In this paper we compared the risk of developing cancer between those in the lowest BMI category (normal healthy weight) and those considered obese (BMI 30+) category. Our meta-analysis therefore did not incorporate into the pooled risk ratio and 95% confidence intervals, the risk associated with developing cancer among those with slightly above normal and above normal BMI. Given the primary objective of this paper was to assess the relationship between obesity and cancer incidencewe believe this was themost appropriate
- 101. statistical analysis to answer the research question. The question Renehan et al. answered was broader in that they were interested in assessing across the spectrum of BMI from normal to obese, the relationship between BMI and cancer risk. A second major difference between the two reviews was our exclusion of studies judged to be of weak methodological quality. The results of studies of weak methodological quality are less trustworthy. The exclusion of these studies likely contributed to the higher pooled risk ratios observed in this meta-analysis in comparison to Renehan et al.The combined effect of the different statistical approaches and the exclusion of studies of weak methodological quality likely explains much of the observed differences between the reviews. Finally, itmay be that studies published since theRenehan et al. meta-analysis, report higher relative risks than had been reported previously. Given several studies published since 2007 were added to this paper, this may further explain the higher pooled risk ratios and 95% confidence intervals observed in this paper. It is important to note that the results from some of the studies included in this paper may not be relevant to a Cana- dian context. For example, studies conducted in South East Asian countries may have limited applicability in Canada. However, a rigorous and systematic meta-analysis process ISRN Preventive Medicine 15 Study or subgroup
- 102. Brindel et al. (2009) Chang et al. (2006, 2007) Engeland et al. (2004) Freedman et al. (2003) Oh et al. (2005) Samanic et al. (2006) Total (95% CI) Log (risk ratio) 0.637 0.131 0.647 0.11333 SE 0.143 0.229 0.16 0.444 0.2449 0.353 Weight 19.9% 17.7% 19.5% 11.6% 17.2% 14.0%
- 103. 100.0% IV, random, 95% CI 0.54 [0.41, 0.72] 1.89 [1.21, 2.96] 1.14 [0.83, 1.56] 1.91 [0.80, 4.56] 1.12 [0.69, 1.81] 0.98 [0.49, 1.96] 1.12 [0.72, 1.72] Risk ratio Risk ratio IV, random, 95% CI 0.1 0.2 0.5 1 2 5 10 Favours experimental Favours controlTest for overall effect: � = 0.49 (� = 0.62) −0.0202 −0.607 Heterogeneity: �2 = 0.23; �2 = 28.37, df = 5 (� < 0.0001); �2 = 82% (a) Study or subgroup Brindel et al. (2009) Chang et al. (2006, 2007) Freedman et al. (2003) Tehard and Clavel-Chapelon (2006)
- 104. Total (95% CI) Log (risk ratio) 0.095 0.344 0.565 SE 0.131 0.194 0.217 0.23 Weight 46.6% 21.3% 17.0% 15.1% 100.0% IV, fixed, 95% CI 0.76 [0.58, 0.98] 1.10 [0.75, 1.61] 1.41 [0.92, 2.16] 1.76 [1.12, 2.76] 1.03 [0.87, 1.23] Risk ratio Risk ratio IV, fixed, 95% CI