Downloaded 514 times

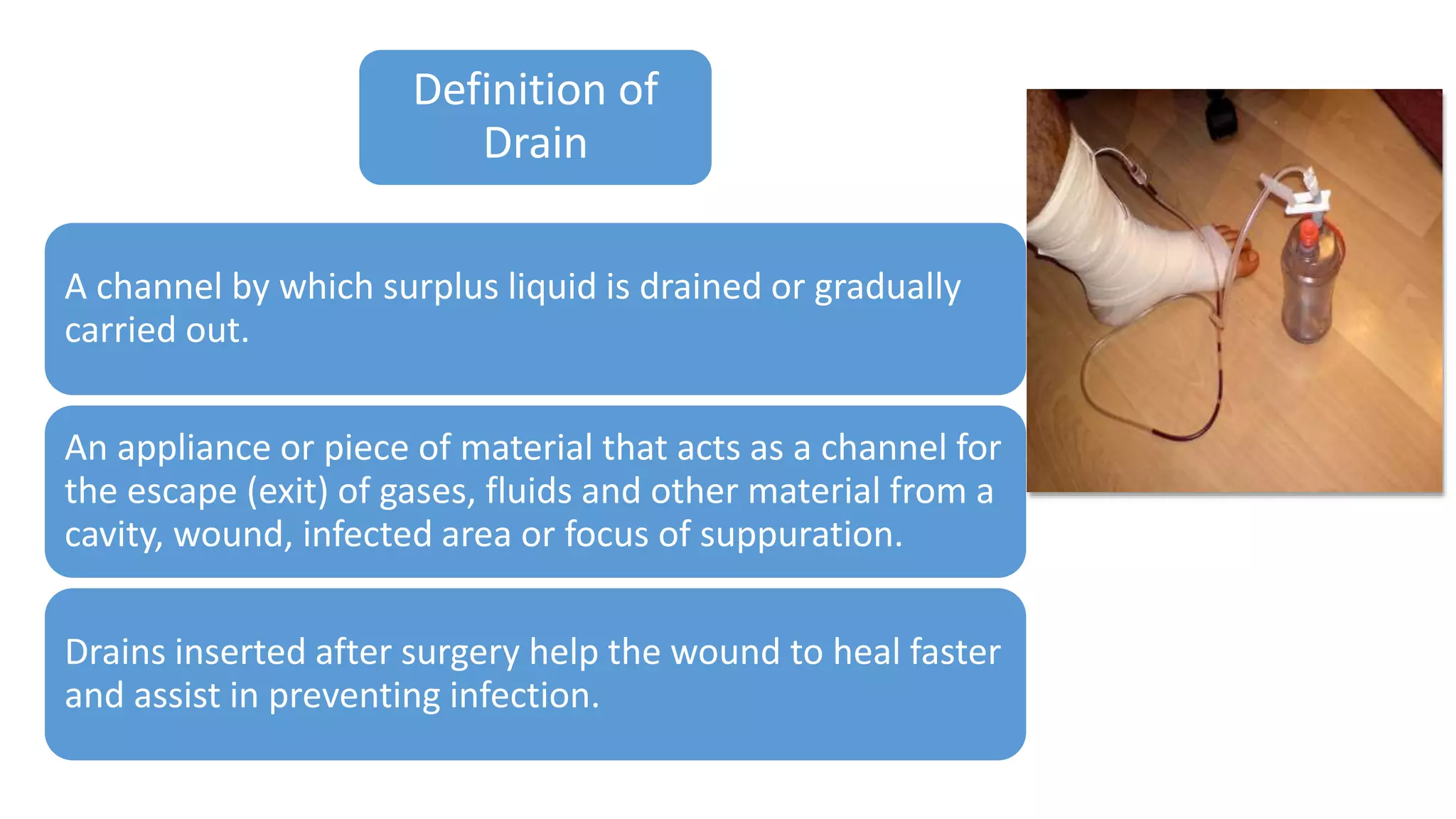








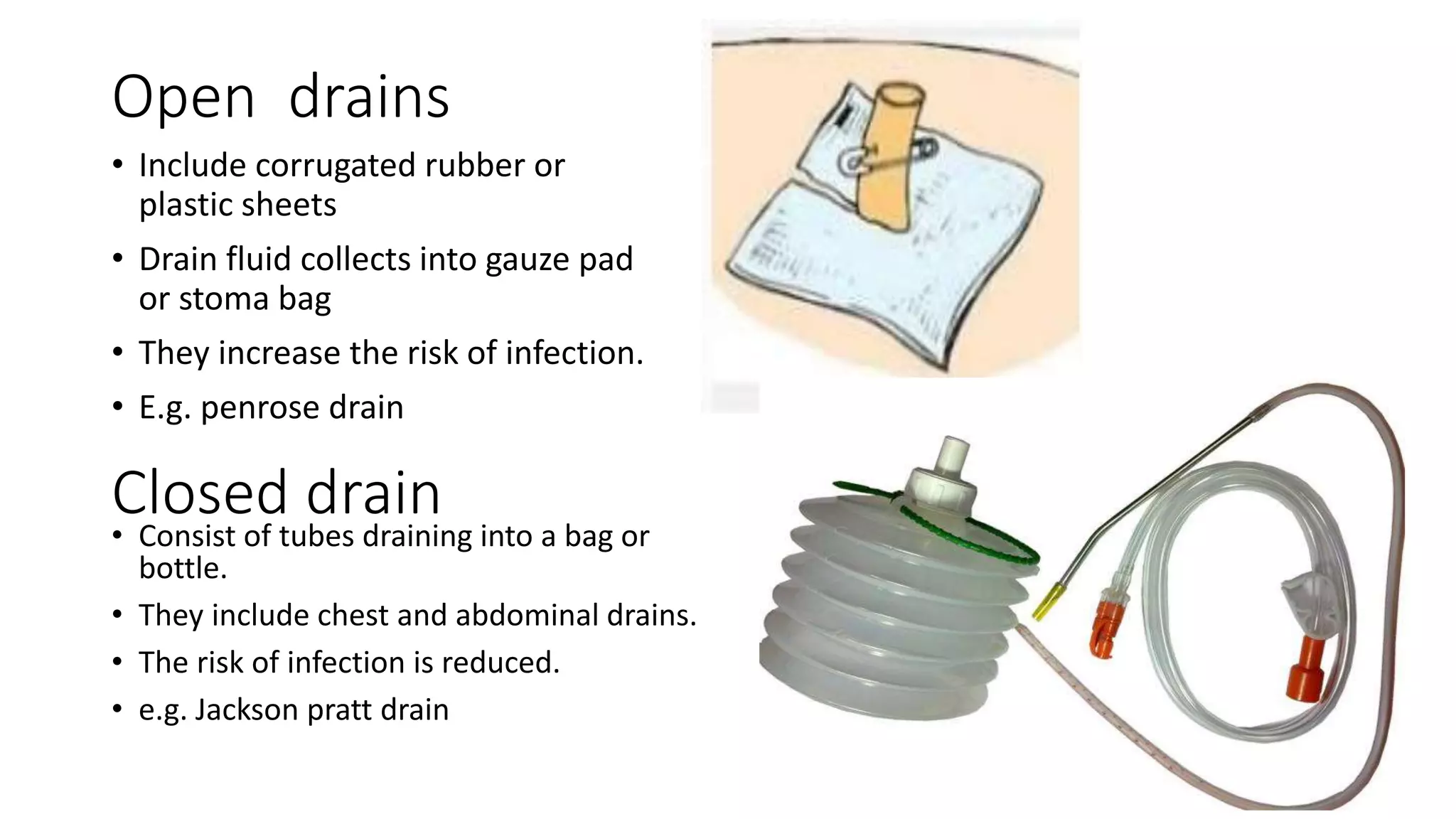

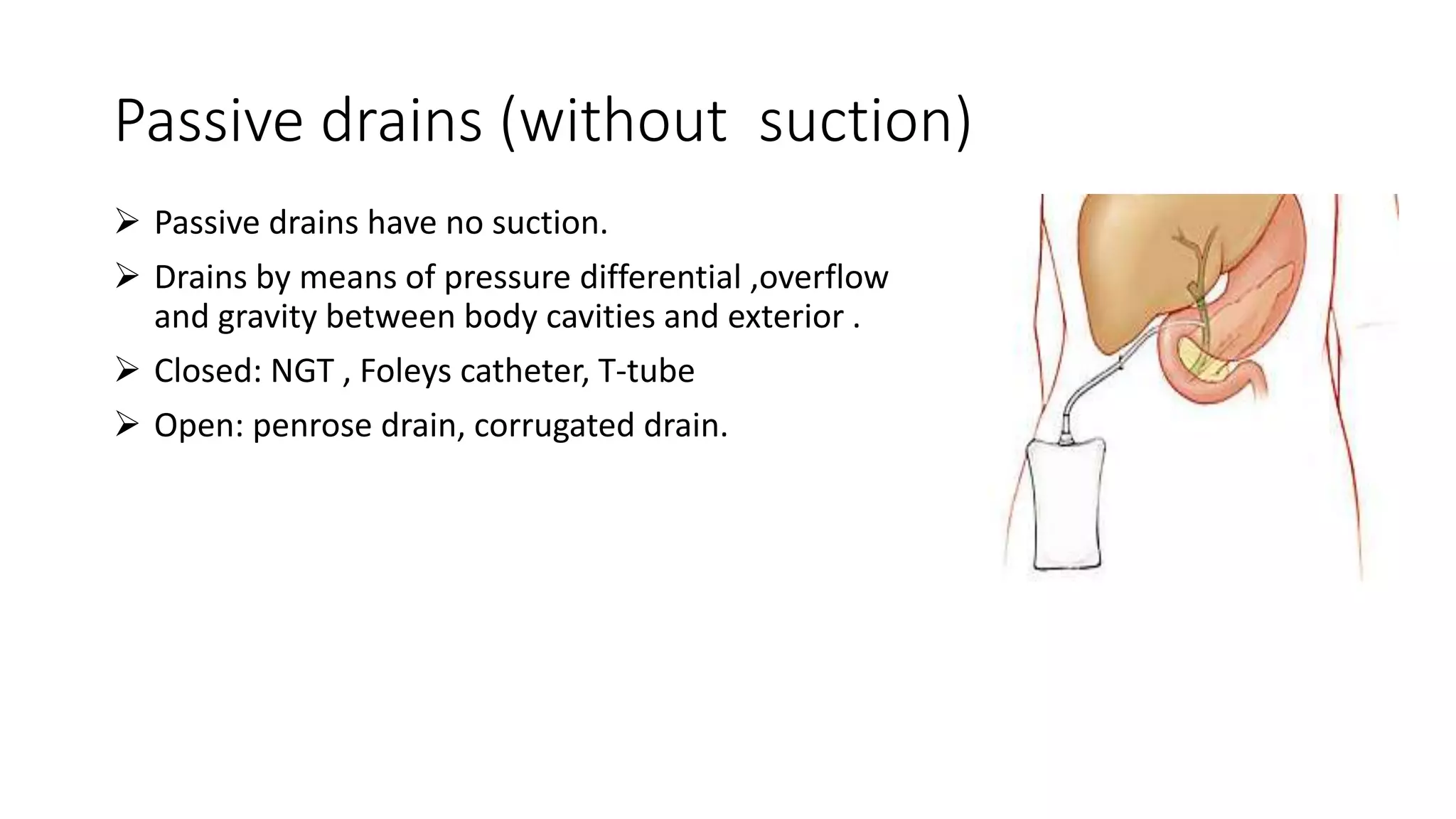
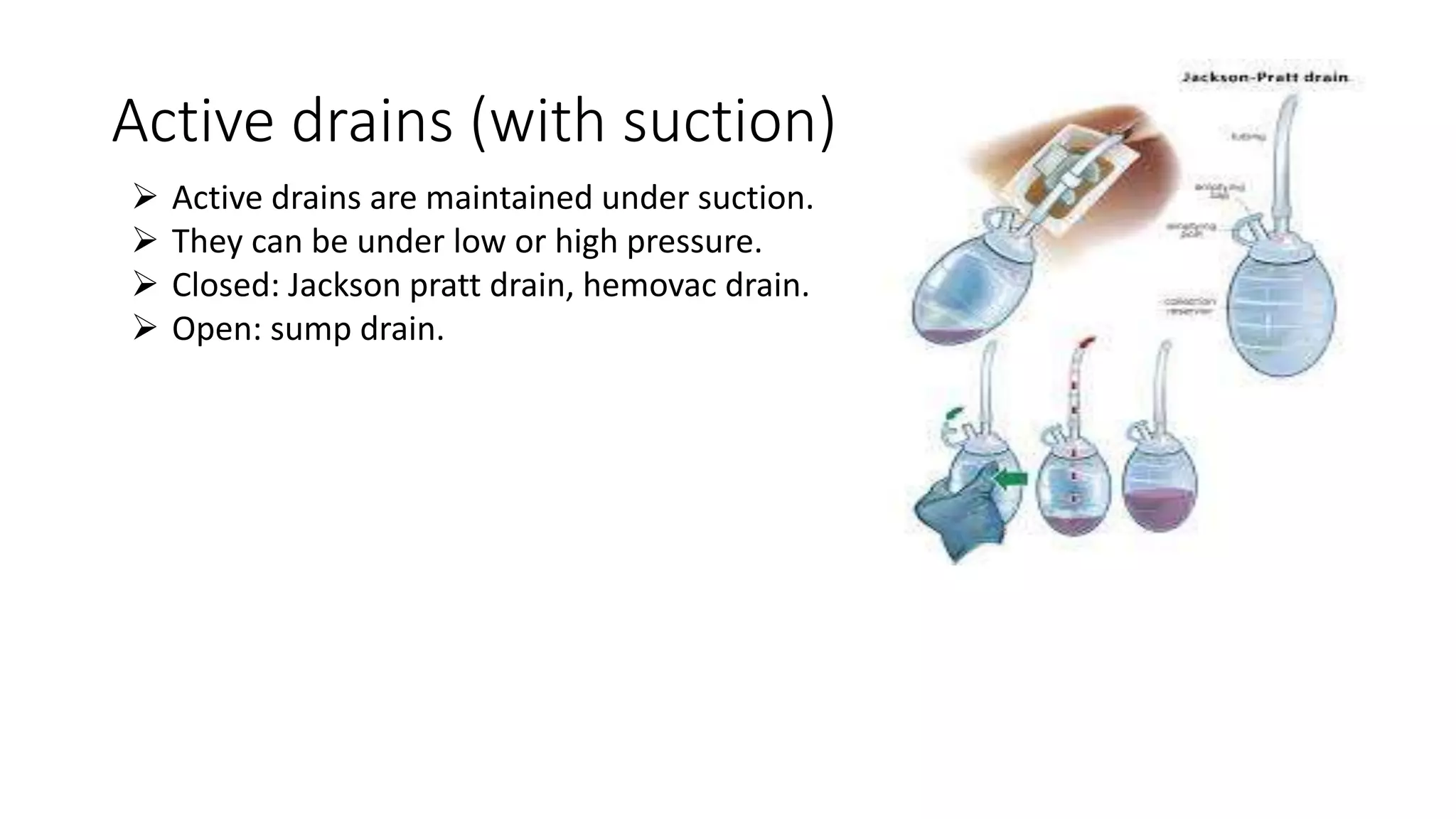







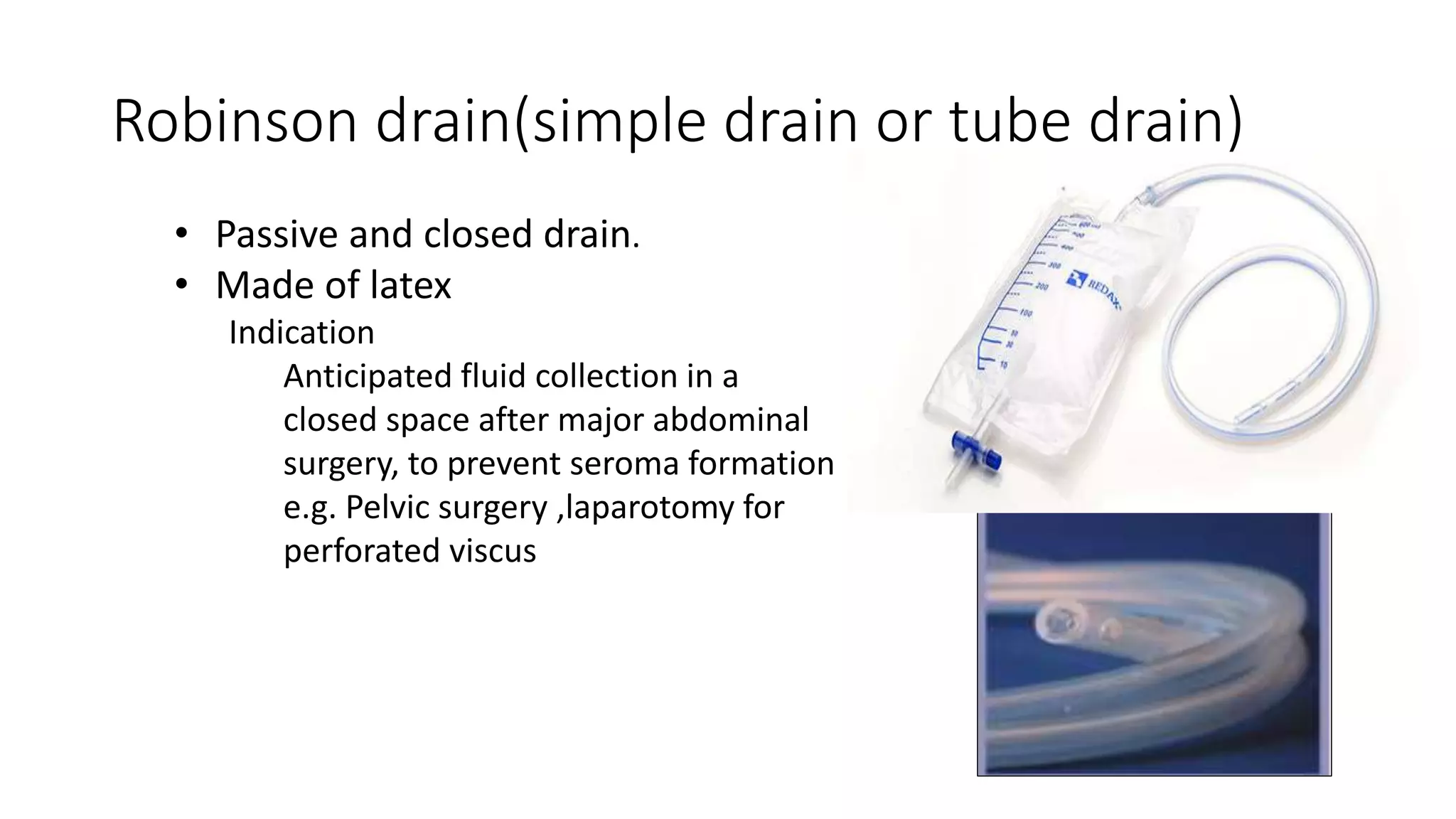

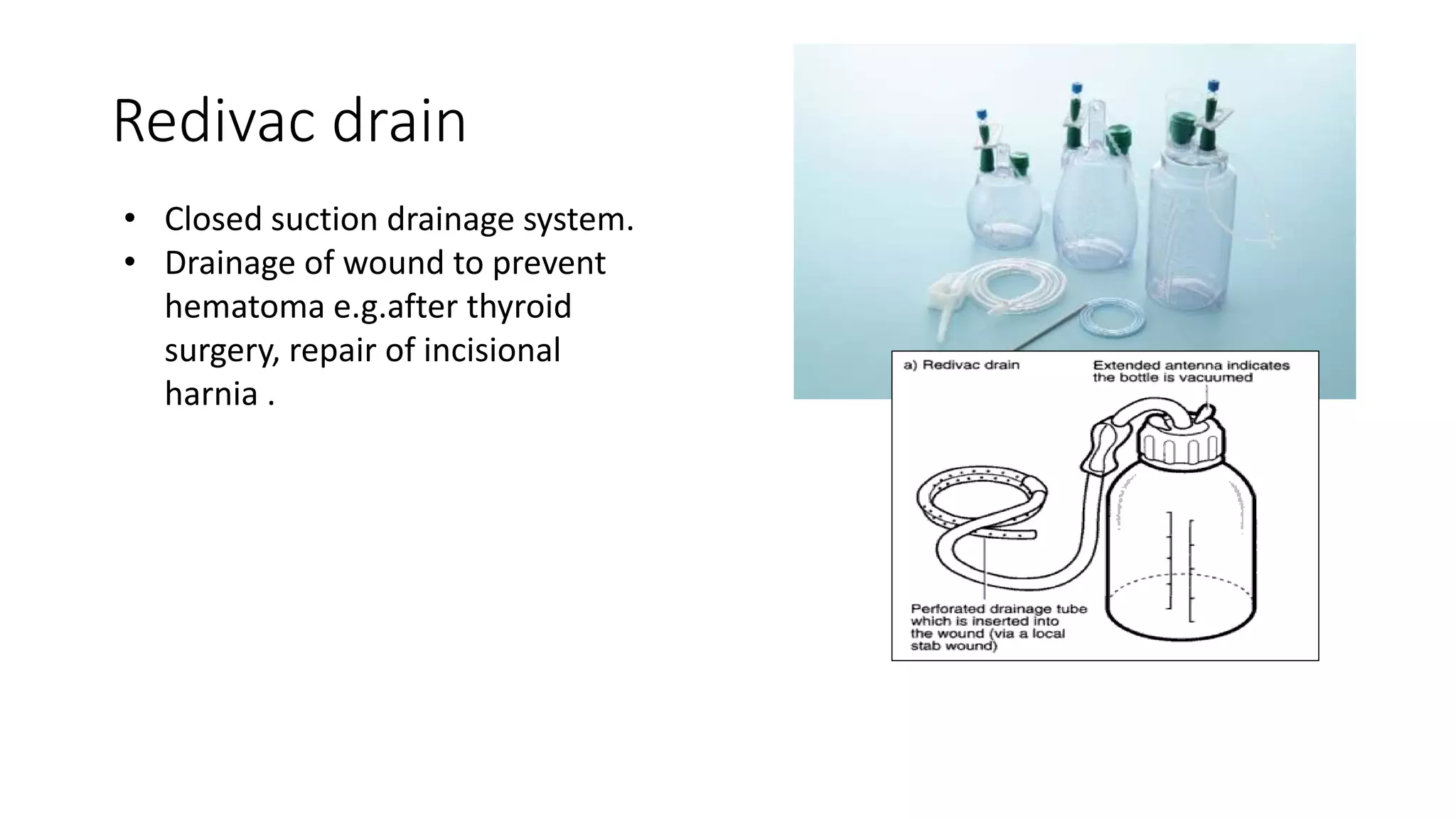








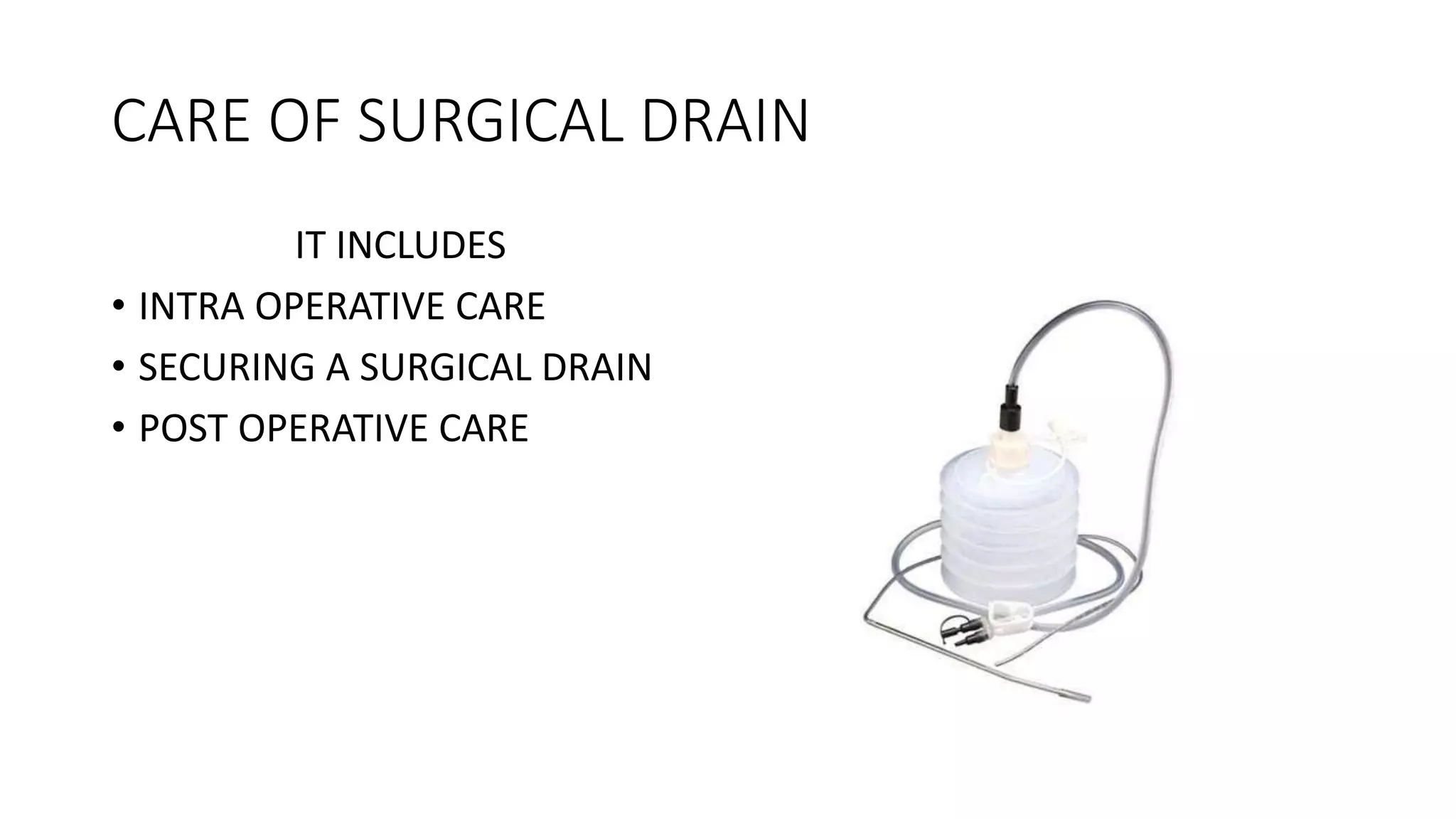








Surgical drains have several purposes and types. They help evacuate fluids from surgical sites to prevent infection and allow wounds to heal. Common types include closed suction drains like Jackson-Pratt drains and open drains like Penrose drains. Placement, securing, and care of drains is important to avoid complications like infection, displacement, or blockage. Drains are removed once drainage decreases significantly or they are no longer needed.