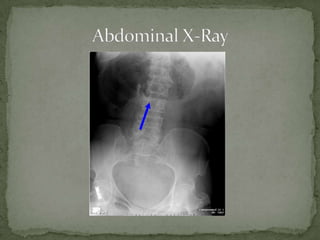
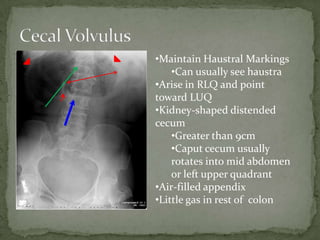
A 56-year-old female presented with acute severe abdominal pain and nausea with a distended right abdomen. Imaging showed cecal volvulus, identified by a dilated cecum greater than 9cm that had rotated into the mid or left upper abdomen. She was started on IV fluids, made NPO, and required surgical consultation for definitive management due to the high risk of perforation or ischemia with cecal volvulus.