Downloaded 2,823 times
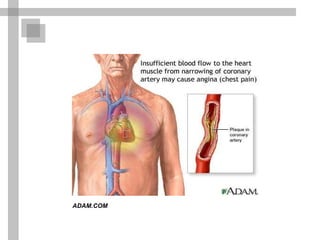
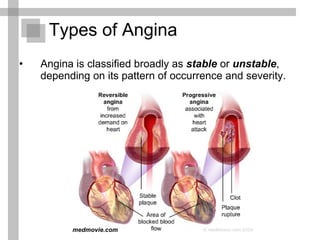

This document provides a summary of angina pectoris (chest pain). It begins with an example case history and treatment. It then defines angina and describes the main types (stable and unstable). It discusses the pathophysiology and clinical presentation. It outlines the diagnostic tests and procedures used to diagnose angina. The goals and approaches to treatment are summarized, including drug therapies like nitrates, beta blockers, and calcium channel blockers. Other measures for managing coronary artery disease are mentioned like lifestyle changes and procedures.






































![Angina pectoris and management[Stable Angina]](https://cdn.slidesharecdn.com/ss_thumbnails/cjjehgfq5k8jyciroa3w-5-6079959866040916905-251204152943-57f808a0-thumbnail.jpg?width=640&height=640&fit=bounds)








