

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Aminiotic Fluid and Human Milk
Similar to Aminiotic Fluid and Human Milk (20)
More from Amany Elsayed
More from Amany Elsayed (20)
Recently uploaded
Recently uploaded (20)
Aminiotic Fluid and Human Milk
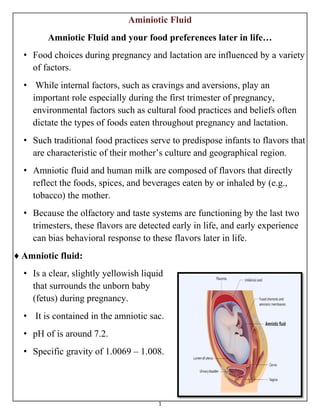
- 1. 1 Aminiotic Fluid Amniotic Fluid and your food preferences later in life… • Food choices during pregnancy and lactation are influenced by a variety of factors. • While internal factors, such as cravings and aversions, play an important role especially during the first trimester of pregnancy, environmental factors such as cultural food practices and beliefs often dictate the types of foods eaten throughout pregnancy and lactation. • Such traditional food practices serve to predispose infants to flavors that are characteristic of their mother’s culture and geographical region. • Amniotic fluid and human milk are composed of flavors that directly reflect the foods, spices, and beverages eaten by or inhaled by (e.g., tobacco) the mother. • Because the olfactory and taste systems are functioning by the last two trimesters, these flavors are detected early in life, and early experience can bias behavioral response to these flavors later in life. ♦ Amniotic fluid: • Is a clear, slightly yellowish liquid that surrounds the unborn baby (fetus) during pregnancy. • It is contained in the amniotic sac. • pH of is around 7.2. • Specific gravity of 1.0069 – 1.008.
- 2. 2 ◘ Origin and Production • The fluid is produced by the mother’s placenta during the first trimester and the early part of the second trimester, until the baby’s kidneys are mature enough to take over the task. • The baby swallows the fluid as they “breathe” and then excretes it again as urine, thus maintaining the constant circulation of the fluid. • However, the urine making up the fluid is not pure waste material as the majority of the fetal waste is passed through the placenta to be filtered by the mother’s kidneys. ♦ Function The primary functions of the fluid are: • To provide a protective cushion for the fetus. • Allow fetal movement. • Stabilize the temperature to protect the fetus from extreme temperature changes. • To permit proper lung development. • Exchanges of water and chemicals, also take place between the fluid, the fetus, and the maternal circulation. • Helps with the uniform growth of the body parts and organs of the baby. • Assists with the proper bone and muscle development.
- 3. 3 • The fluid is released when the amnion ruptures, commonly known as when a woman's "water breaks". • When this occurs during labour at term, it is known as "spontaneous rupture of membranes" (SROM). • If the rupture precedes labour at term, however, it is referred to as "premature rupture of membranes" (PROM). ♦ Amniotic Fluid: Circulation • The water content of the amniotic fluid changes every three hours • Large volume moves in both directions between the fetal & maternal circulations mainly through the placental membrane. • It is swallowed by the fetus, is absorbed by respiratory & GIT and enters fetal circulation.
- 4. 4 • It then passes to maternal circulation through placental membrane. During final stages of pregnancy fetus swallows about 400ml of amniotic fluid per day. • Excess water in the fetal blood is excreted by the fetal kidneys and returned to the amniotic sac through the fetal urinary tract. ♦ Volume By Age – 10 weeks = 30 ml – 20 weeks = 350 ml – 38 weeks = 1000 ml – Term (40 weeks) = 500 ml – Post term (more than 40 weeks) = <500 ml ♣ Volume • The amount of amniotic fluid increases throughout pregnancy, reaching a peak of approximately 1 L during the third trimester, and then gradually decreases prior to delivery. • The volume of amniotic fluid is positively correlated with the growth of fetus. • From the 10th to the 20th week it increases from 25ml to 400ml approximately. • From the 8th week, when the fetal kidneys begin to function, fetal urine is also present in the AF. • Then the relationship between AF and fetal growth stops. • It reaches the high peak of 800ml at the 28 week.
- 5. 5 ○ The amount of fluid declines to roughly 400 ml at 42 weeks age. • An excessive amount of amniotic fluid is called polyhydramnios. • This condition can occur with multiple pregnancy (twins or triplets), congenital anomalies, or gestational diabetes. • An abnormally small amount of amniotic fluid is known as oligohydramnios. • This condition may occur with late pregnancies, ruptured membranes, placental dysfunction, or fetal abnormalities. • Abnormal amounts of amniotic fluid may cause the health care provider to watch the pregnancy more carefully. • Removal of a sample of the fluid, through amniocentesis, can provide information about the sex, health, and development of the fetus. ♦ Chemical Composition • The placenta is the ultimate source of amniotic fluid water and solutes. • Amniotic fluid has a composition similar to that of the maternal plasma and contains a small amount of sloughed fetal cells from the skin, digestive system, and urinary tract. • The fluid also contains biochemical substances that are produced by the fetus, such as bilirubin, lipids, enzymes, electrolytes, nitrogenous compounds, and proteins that can be tested to determine the health or maturity of the fetus. • A portion of the fluid arises from the fetal respiratory tract, fetal urine, the amniotic membrane, and the umbilical cord. • As would be expected, the chemical composition of the amniotic fluid changes when fetal urine production begins.
- 6. 6 • The concentrations of creatinine, urea, and uric acid increase, whereas glucose and protein concentrations decrease. • The concentrations of electrolytes, enzymes, hormones, and metabolic end products also vary (change) but are of little clinical significance. • Measurement of amniotic fluid creatinine has been used to determine fetal age. • Prior to 36 weeks’ gestation, the amniotic fluid creatinine level ranges between 1.5 and 2.0 mg/dL. • It then rises above 2.0 mg/dL, thereby providing a means of determining fetal age as greater than 36 weeks. ♦ Specimen Collection • Amniocentesis is recommended when screening blood tests such as the maternal serum alpha feto protein test [AFP], human chorionic gonadotropin [hCG], and unconjugated estriol [UE3]), yield results that are abnormal. • Fetal epithelial cells in amniotic fluid indicate the genetic material of the fetus and the biochemical substances that the fetus has produced. • These cells can be separated from the fluid, cultured, and examined for chromosome abnormalities by karyotyping, Fluorescence in situ hybridization (FISH) , and DNA testing. ♦ Ultrasonography • Fetal body measurements taken with ultrasonography accurately estimate the gestational age of the fetus and provide an assessment of the size and growth of the fetus throughout pregnancy. • Finding an abnormality on the ultrasound could indicate potential fetal development problems and indicate the need for an amniocentesis and laboratory measurements of fetal lung maturity.
- 7. 7 ♦ Amniotic Fluid Index • Amniotic Fluid Index (AFI) is a measure of the amount of amniotic fluid and is an index for the fetal wellbeing. • It is a part of the Biophysical profile. • AFI is the score given to the amount of amniotic fluid (by adding up centimeters of depth of four pockets of fluid) seen on pregnant uterus by ultrasound. • An AFI < 5-6 is considered as Oligohydramnios and an AFI > 18-22 is considered as Polyhydramnios. • Storage Instructions: Freeze within 4 hours to transport to laboratory; stable refrigerated up to 1 week. • Protect from light. • Avoid repeated freezing and thawing of the specimen, which may cause the sample to precipitate, resulting in a lower than expected value. • If cell culture is requested the specimen should be kept at 37o C. ◘ Indications For Performing Amniocentesis Mother’s age of 35 or more at delivery. Family history of chromosome abnormalities, such as trisomy 21 (Down syndrome). Parents carry an abnormal chromosome rearrangement. Parent is a carrier of a metabolic disorder. Three or more miscarriages. Fetal lung maturity.
- 8. 8 ♦ Collection • Amniotic fluid is obtained by needle aspiration into the amniotic sac, a procedure called amniocentesis. • The procedure most frequently performed is a transabdominal amniocentesis. • Using continuous ultrasound for guidance, the physician locates the fetus and placenta to safely perform the procedure. • A maximum of 30 mL of amniotic fluid is collected in sterile syringes. The first 2 or 3 mL collected can be contaminated by maternal blood, tissue fluid, and cells and are discarded. • Fluid for bilirubin analysis in cases of hemolytic disease of the newborn (HDN) must be protected from light at all times. ♣ What About Normal Activities After An Amniocentesis? • After an amniocentesis, it is best to go home and relax for the remainder of the day. • No exercise or strenuous activity should be performed, don’t lift anything over 20 pounds (including children), and sexual relations should be avoided. • To relieve discomfort two Tylenol (acetaminophen) every 4 hours, may be taken. • The day after the procedure, normal activities may be resumed unless otherwise directed by the doctor. • Call your doctor if you develop a fever or have bleeding, vaginal discharge, or abdominal pain that is more severe than cramps.
- 9. 9 ♦ Color and Appearance • Normal amniotic fluid is colorless and may exhibit slight to moderate turbidity from cellular debris, particularly in later stages of fetal development. • Blood-streaked fluid may be present as the result of a traumatic tap, abdominal trauma, or intra-amniotic hemorrhage. • The presence of bilirubin gives the fluid a yellow color and is indicative of red blood cell destruction resulting from HDN. ◘ Differentiating Maternal Urine From Amniotic Fluid • Differentiation between amniotic fluid and maternal urine may be necessary to determine possible premature membrane rupture or accidental puncture of the maternal bladder during specimen collection. • Chemical analysis of creatinine, urea, glucose, and protein aids in the differentiation. • Levels of creatinine and urea are much lower in amniotic fluid than in urine. • Creatinine does not exceed 3.5 mg/dL and urea does not exceed 30 mg/dL in amniotic fluid. • Whereas values as high as 10 mg/dL for creatinine and 300 mg/dL for urea may be found in urine. • Measurement of glucose and protein by a reagent strip is a less reliable indicator, because glucose and protein are not uncommon urine constituents during pregnancy.
- 10. 10 ♦ Fetal Distress • Clinical analysis of amniotic fluid assesses both fetal well being and maturation. • Because amniotic fluid is a product of fetal metabolism, the constituents that are present in the fluid provide information about the metabolic processes taking place and the progress of fetal maturation. • The oldest routinely performed laboratory test on amniotic fluid evaluates the severity of the fetal anemia produced by hemolytic disease of the newborn. • Those infants are referred to as (Rh babies). • The incidence of this disease has been decreasing rapidly since the development of methods to prevent anti-Rh antibody production. • The destruction of fetal red blood cells by antibodies that are present in the maternal circulation results in the appearance of the red blood cell degradation product, bilirubin, in the amniotic fluid. • By measuring the amount of bilirubin present in the fluid, it is possible to determine the degree of hemolysis taking place and to assess the danger of this anemia presents to the fetus. • In cases of premature or prolonged rupture of the amniotic membranes there is concern over possible infection of the mother and fetus.
- 11. 11 ♦ Can Amniotic Fluid Be Tested To Look For Infections? • Yes, there are a few tests that can be performed on amniotic fluid to detect infections that are passed from mother to baby during pregnancy (congenital infections). • Some of these infections may have serious consequences for the developing fetus. • A few examples include tests for cytomegalovirus (CMV), toxoplasmosis, and bacterial infections.
- 12. 12 Human Milk • Characteristic of the class Mammalia is the ability to produce milk. • It is the most appropriate source of nutrition for the infant up to the age of 6 months.
- 13. 13 • It contains: bioactive components such as the maternal antibodies, chemical mediator, vitamins, enzymes and some types of white blood cells. ◘ Types of breast milk: • Colostrum or early milk • Transitional milk • Fore milk • Hind milk 1- Colostrum (Also called “the first milk”) (2-3 days after birth). It has a yellowish to cream colored thick appearance. Contains antibodies, immune-system cells and Lactobacillus bifidus factor (bacteria that inhibits negative bacteria and parasites in the infant). It is high in protein especially antibodies, vitamins, minerals, but very low in fat and carbohydrate compared to mature breast milk. 2- Transitional milk It occurs after colostrum stage and lasts for approximately two weeks until it is replaced by mature milk. it contains high levels of fat, lactose, and vitamins to help the baby regain any weight lost after birth.
- 14. 14 3- Mature milk It is the final milk that is produced and lasts throughout lactation. 90% is water, which is necessary to maintain hydration of the infant. The other 10% is carbohydrates, protein, and fats, which are necessary for both growth and energy. There are two types of mature milk: Foremilk and hindmilk. It contains Docosahexaenoic acids (DHA), long chain omega- 3 fatty acids. Used for synthesis of brain tissues, central nervous system and eyes. DHA and cholesterol not found in human milk substitutes. ◘ Proteins In Breast Milk 1-Casein: It is the main protein. It complexes with calcium thus promoting its absorption. These are present in breast milk in much lower concentration than in cow's milk. Mature Human Milk- CHO ♦ Lactose – Disaccharide of galactose and glucose. – Dominant carbohydrate in human milk. – Enhances calcium absorption.
- 15. 15 ♦ Other carbohydrates – Monosaccharides, glucose. – Polysaccharides • Contribute calories. • Stimulate the growth of bifidus bacteria in the gut. • Inhibit the growth of E. coli and other bacteria. • Which prevents infection & diarrhea. The Immunologic Components of Mature Milk ♣ Immunoglobulins • Mature milk contains all of the different antibodies (M,A, D, G, E), but secretory immunoglobulin A (sIgA) is the most abundant. ♣ Lactoferrin It has antimicrobial activity (bacteriocide, fungicide). Human colostrum has the highest concentration, followed by human milk, then cow milk ♣ Lysozyme Enhances sIgA bactericidal activity against gram-negative organisms. ♣ Mucins Adhere to bacteria and viruses and help eliminate them from the body. ♣ Leukocytes With the transition from colostrum to mature milk, the percentage of macrophages increases from 40-60% of the cells to 80-90%.
- 16. 16 ◘ Physical Properties of Milk White appearance due to the presence of: the calcium salt of casein. the emulsified lipids. The pH of milk is 6.6-6.8. The Volume of milk at the high level of lactation is 1.5 liters of milk. ◘ Milk Formation The formation and secretion of milk depend on: • Prolactin • Growth hormones • Cotrisol • Parathyroid hormone
- 17. 17 1. During Pregnancy: 2. After Birth: Milk ejection is promoted by: 1- Neurogenic stimulant (stimulated by suckling) 2- Hormonal reflex (oxytocin & prolactin) Alcohol Nicotine Caffeine Marijuana and other drugs Environmental Exposures Genes
- 18. 18 ♦ Alcohol The alcohol transfers to the breast milk and affect directly on the baby. It slows let down reflex (oxytocin hormone). ♦ Nicotine The nicotine in the milk is 1.5- 3 times higher than in the blood. Over time the infant could metabolize it in liver and emit nicotine into kidneys. ♦ Caffeine ♦ Marijuana and other drug abuse Marijuana, cocaine, and heroin. Very harmful for mother and affect the infant directly and negatively. Each drug may include bacteria, heavy metals, pesticides. ♦ Environmental Exposures Avoid eating swordfish, king mackerel, and shark from freshwaters that are contaminated. Avoid exposure to paints, glues, furniture strippers, nail polish and gas fumes.
- 19. 19 ♦ Genes •Different variations of Apolipoproteins affect on the amount of fat absorbed into the bloodstream and fat metabolism, then affect the breast milk composition. Cows milk vs. human milk Human milk Cow’s milk • Higher content of water and lactose. • Lower content of protein than cows milk. • Contain vitamins and minerals that are necessary for human growth. • It lacks some of the immunological components that are required by the human infant. • It contains foreign proteins that may trigger allergic reactions in some babies.
- 20. 20 ◘ Benefits of Mother’s Milk 1. It is high in nutritional value. 2. It is rich in immunological components . 3. It is sterile and cheap. ♣ It has positive effects on mother health: It reduces the risk of developing breast cancer. Causes weight loss. Delays menstruation. Causes low iron loss.