
Downloaded 11 times


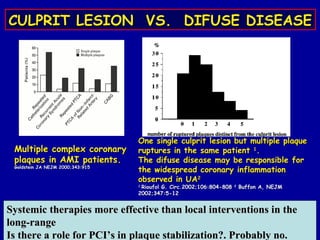
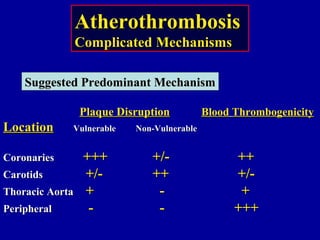
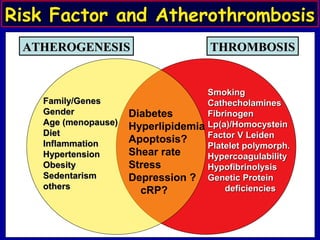
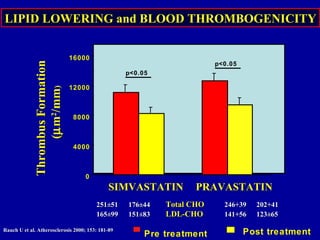
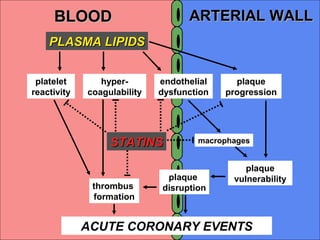
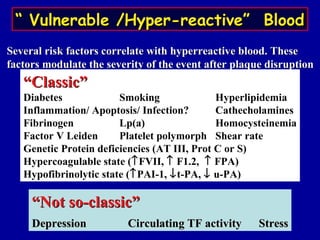
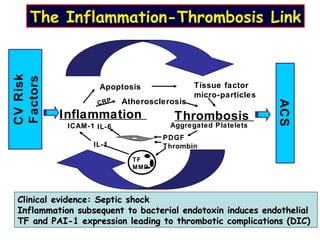
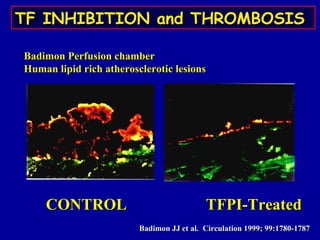
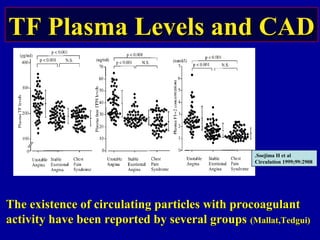
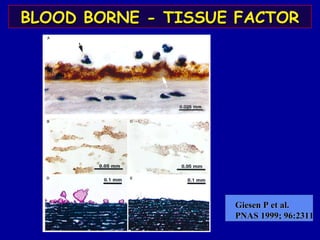
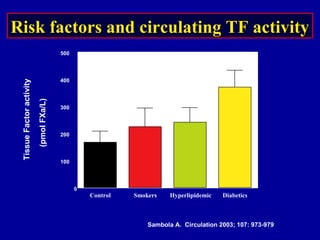
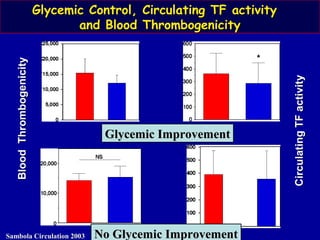
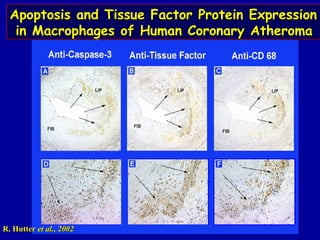
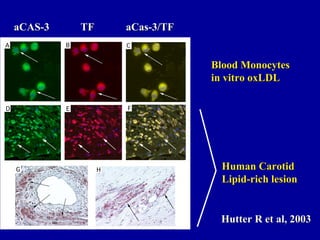
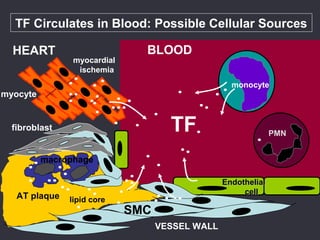

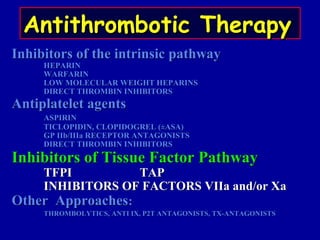
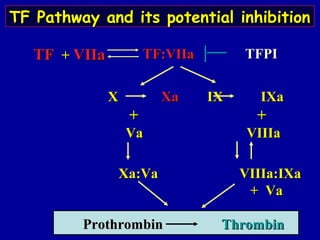
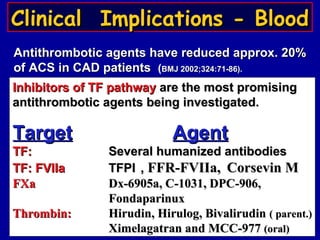
This document summarizes presentations from symposia on vulnerable plaque and discusses the relationship between plaque, blood, and patients in atherothrombosis. It notes that multiple factors like diabetes, smoking, and hyperlipidemia can make blood more thrombogenic and moderate the severity of acute events after plaque rupture. Statins, aspirin, and other drugs that target tissue factor or thrombin pathways may be promising antithrombotic agents by inhibiting thrombosis initiation and propagation.























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




