Meningococcal infection
•Download as PPTX, PDF•
4 likes•2,456 views

Meningococcal infection

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Meningococcal infection
Similar to Meningococcal infection (20)
More from Rivindu Wickramanayake
More from Rivindu Wickramanayake (20)
Recently uploaded
Recently uploaded (20)
Meningococcal infection
- 1. W. P. Rivindu H. Wickramanayake Group no. 04a 6th Year 2nd Semester – 2020 September Tbilisi State Medical University, Georgia Meningococcal Infection
- 2. Introduction ● One of the most serious and life-threatening infectious diseases during childhood is bacteremia, a consequence of which is septic shock, where inadequate perfusion of tissues occurs due to endotoxemia. ● Neisseria meningitidis (Meningococcus) is an important bacterial infection manifesting as meningitis or septicemia, or more often a combination of both. ● Asymptomatic pharyngeal colonization is the initial step of infection, with humans being the natural reservoirs. ● From the nasopharynx, the coccus reaches the meninges translocating across the nasopharyngeal mucosa and along the perineural sheath of the olfactory nerve, through the cribriform plate of the ethmoid. ● Bloodstream spread to the meninges will cause meningitis. ● In some children, the predominant feature is cardiovascular collapse leading to septic shock. ● Transmission occurs by respiratory droplets and requires close direct contact. ● Children younger than 5 years do not have adequate immunity against the polysaccharide antigens of N. meningitidis. ● The risk factors for infectious disease in child care facilities include immunologic susceptibility, lack of awareness, and practice of good hygiene, a natural tendency to intimacy, frequent oral contact with objects in the environment. ● The invasive meningococcal disease is seen in 2 age groups: infants who are vulnerable due to disappearance in the early life of the maternal antibodies & adolescents with a high rate of colonization of nasopharynx.
- 3. Etiology ● N. meningitidis is a gram-negative coccus in pairs with adjacent sides flattened. It is non-motile, aerobic, and facultatively anaerobic. It produces catalase and is oxidase positive. It produces acid from glucose and maltose. Fresh isolates require enriched media like blood or chocolate agar. Incubation in a humidified 10% carbon dioxide (CO2) environment enhances growth. Virulence factors include the polysaccharide capsule, which enhances invasiveness by inhibiting phagocytosis and enhancing organism survival during the bloodstream and central nervous system (CNS) invasion. Pili mediate attachment, colonization, and invasion of the organisms to the mucosal cells of the nasopharynx. The antigenic variation of pili by a cassette mechanism allows the bacterium to escape the host's immune system. Outer Membrane Proteins Porin proteins can insert themselves into membranes of target cells, and phagolysosomes can induce apoptosis. OPC protein functions in mucosal adherence and invasion of endothelial cells. IgA1 protease hydrolyzes IgA1 molecules in the hinge regions. The enzyme inactivates IgA1 at mucosal surfaces, enabling initial attachment and subsequent invasion. Pathogenic Neisseria survives and multiplies by their ability to extract iron from high-affinity iron-binding proteins. N. meningitidis can acquire penicillin resistance from commensal Neisseria species in the nasopharynx through DNA fragments by the transformation. Meningococcus also exhibits a phase variation of surface antigens, thus evading the host immune response. The capsular polysaccharides are antigenic and form the basis of serogroups. Twelve serogroups are A, B, C, H, I, K, L, X, Y, Z, W-135, and 29F. Serogroups A, B, C, W-135, X, and Y are the most common causes of invasive disease worldwide.
- 4. Epidemiology ● In developing countries, the incidence rate is 10 to 25 per 100,000 inhabitants per year. ● The highest rate of 10 to 1000 per 100,000 per year is seen in a belt across sub-Saharan Africa, termed the meningitis belt, with recurrent epidemics of group A. ● Death occurs in 6% to 10% of cases and complications in 4.3 to 11.2% of cases. ● Group A was predominant from 2007 through 2009, while serogroup W135 predominated in 2010 through 2011. ● In 2013 and 2014, 2 outbreaks of meningococcal serogroup C, a strain relatively rare in Africa, occurred in Nigeria and Kebbi. ● International outbreaks of N. meningitidis infections occurred in 1987 and 2000 associated with the Hajj pilgrimage to Mecca. ● 1987 outbreak was due to serogroup A and the 2000 outbreak due to serogroup W-135. Serogroup W has emerged in other regions, including South America and England. ● In European countries, invasive serogroup C disease has declined, and serogroup B is causing 60% to 72% of cases of invasive disease. ● In Asia, large epidemics caused by serogroup A occurred historically in China, India, Nepal, and Russia. More recently, serogroup B and C emerged as the cause in this area. ● An increase in the serogroup Y has been reported in the Nordic European countries.
- 5. Pathophysiology ● Primary cause of cardiovascular collapse from sepsis is a peripheral circulatory failure. ● Cardiac dysfunction due to myocardial failure plays a prominent role. ● Higher endotoxin (LOS) concentrations were associated with shock, renal failure, and respiratory distress. ● High concentrations of IL-6 and IL-8 are seen in those with meningococcal shock. ● TNF and IL-1 activate endothelial cells by increasing their permeability and adhesiveness for white cells. ● Overproduction of nitric oxide lowers arterial pressure due to vasodilation. It also impairs cardiac contractility. ● Endothelial cell retraction on interaction with bacterial endothelial cells leads to a loss of integrity, causing capillary hemorrhages and the formation of thrombi in purpuric lesions. ● When a large number of bacteria colonize the blood vessels and leads to the corresponding signaling, this is responsible for the extensive purpuric lesions and severity of shock in Purpura fulminans.
- 6. ● Histology of skin lesions shows endothelial necrosis of capillaries and small veins in the dermis and subcutaneous tissue. ● Neutrophil infiltration and occlusion of vessels with WBCs, platelets, fibrin thrombi, and hemorrhage are seen. ● Meningococci are seen within the endothelium and thrombi. Histopathology
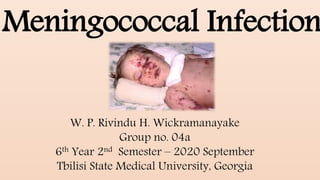
- 7. ● The disease spectrum caused by N. meningitidis ranges from asymptomatic carriage to death due to fulminant meningococcemia. ● Meningococcal meningitis and septicemia are the common syndromes reported, although both clinical pictures present in some cases. ● The signs and symptoms of meningococcemia include an early upper respiratory tract infection with coryza, pharyngitis, tonsillitis, and laryngitis. ● Patients are febrile with a headache, vomiting, and lethargy. ● Typically, patients with meningococcemia have a fever and hemorrhagic rash, followed by signs of severe circulatory collapse. ● Purpura and shock often develop within hours. ● Diffuse mottling to extensive purpuric lesions are the skin manifestations. ● Petechiae or purpura are seen in 50% to 60% of patients. ● Twenty percent to 30% of children may not have a rash on presentation. History and Physical
- 8. ● Chronic meningococcemia is defined as meningococcal septicemia with fever for at least a week before antibiotic therapy and with no meningeal symptoms. ● In chronic meningococcemia, bacteria are never found by biopsy or culture of skin lesions. ● Researchers postulate that the skin changes and arthritis may result from antigen-antibody complexes. ● The diagnosis is established by identifying the organism in blood cultures. ● Recovery is prompt following antibiotic therapy. ● Myocardial manifestations associated with meningococcal meningitis, including heart failure with pulmonary edema and high central venous pressures accompanying signs of poor peripheral perfusion. ● Treatment of myocardial failure can ameliorate the situation. ● Increased levels of interleukin 6 may be a mediator of myocardial depression in septic shock due to meningococcal infection. Continued;
- 9. ● Diagnosis should be clinically made, and broad-spectrum antibiotic therapy started with pending organism identification. Microbiological Diagnosis - Public health control - Antibiotic sensitivity - To exclude other organisms Gram Stain - Cerebrospinal fluid (CSF) in meningitis shows gram-negative intracellular and extracellular diplococci. - Skin lesions in meningococcemia: Needle aspiration and scrapings are Gram-stained Buffy coat of blood Gram stain Culture - CSF is inoculated onto chocolate agar and incubated in 3% to 5% CO2 - Specimens from mucosa are inoculated into selective medium- Thayer-Martin chocolate agar to which vancomycin, colistin, and nystatin are added to inhibit commensals. - Blood culture: 40% to 75% positive before starting treatment. CSF cultures are positive in 90% of untreated patients with meningitis - Combining the results of blood & CSF cultures with CSF Gram stain identifies 94% of meningitis antigen. Evaluation
- 10. Antigen Detection - The meningococcal antigen in CSF (serum and urine have cross-reactions): Latex agglutination; Poor sensitivity and specificity for capsular B type - PCR assays can detect meningococcal DNA in CSF, plasma, and serum. Sensitivity and specificity are above 90%. It is more sensitive than blood culture. Diagnosis can be made in 4 to 8 hours. PCR assays are less affected by previous antibiotic therapy. Imaging - If the patient is in a coma, computed tomography (CT) brain imaging is helpful to exclude intracranial hemorrhage. Hematologic and Metabolic Abnormalities - In meningococcal meningitis, CSF, WBC count, peripheral blood leukocyte count and C-reactive protein, procalcitonin, and ESR are elevated. CSF has raised protein, low glucose, and gram-negative Diplococcus. - In meningococcal septicemia, metabolic derangements like hypoglycemia, hypokalemia, hypocalcemia, hypomagnesemia, hypophosphatemia, and metabolic acidosis are seen in severe cases. Anemia, coagulopathy, decreased protein C, fibrinogen, prothrombin, and coagulation factors (V, VII, and X) are also seen. Continued;
- 11. Antimicrobial Agents - Third-generation cephalosporin-ceftriaxone or cefotaxime are used for initial therapy. Continued disease: • Ceftriaxone (80 mg/kg per day in 1 to 2 divided doses intravenously [IV]) • Cefotaxime (200 mg/kg per day in 3 to4 divided doses IV) • Penicillin G (50 mg/kg every 4 to 6 hours IV) • Chloramphenicol (100 mg/kg/day in 4 divided doses, orally or IV) • Meropenem for those with severe allergies - The recommended duration of therapy is 7 days for both meningitis and meningococcemia. Treatment / Management
- 12. Adjunctive and Experimental Therapies - Corticosteroid therapy: Replacement doses (25 mg/m3 hydrocortisone 4 times) daily is useful in children with refractory shock associated with impaired adrenal gland response. • Recombinant bactericidal permeability-increasing protein (rBPI) binds to endotoxin and blocks the inflammatory cascade. Children receiving rBPI had fewer amputation and blood product transfusions and improved functional outcomes. • Other adjunctive therapies in the management of septicemia are plasmapheresis, extracorporeal membrane oxygenation (ECMO), fibrinolysis, and anti-mediator therapy. Continued;
- 13. Emergency Management • After securing the airway, priorities in children with meningococcal disease are:Correction of cardiovascular shock and • Control of raised intracranial pressure • Aggressive fluid resuscitation with 0.9% NaCl solution in a volume of 20 ml/kg over 5 to 10 minutes is of importance and repeated until shock improves. Inotropic support is needed to maintain tissue perfusion. • Human albumin solution can be used as an alternative. • Anemia, coagulopathy is monitored and corrected. • In cases of raised intracranial pressure, adequate cerebral perfusion should be ensured by correcting shock and providing neurointensive care. Continued;
- 14. Infectious 1. Rocky Mountain spotted fever 2. Ehrlichiosis 3. Streptococcal pneumoniae 4. Hemophilus influenza type B 5. Group A streptococcus 6. Staphylococcus aureus 7. Gram-negative bacterial sepsis with DIC 8. Infective endocarditis 9. Gonococcemia 10. Rat-bite fever 11. Typhus 12. Secondary syphilis Non-Infectious 1. Henoch-Schonlein purpura 2. Acute hemorrhagic edema of infancy 3. Platelet disorders (Idiopathic thrombocytopenic purpura) 4. Collagen vascular disease 5. Neoplastic processes Differential Diagnosis
- 15. ● Scoring systems are devised to predict prognosis with meningococcal disease. Most prognostic scoring systems agree that purpura fulminans and shock are poor prognostic signs. ● The Glasgow meningococcal septicemia prognostic score (GMSPS) evaluates 7 key items: hypotension, the difference in skin-core temperature, coma, acute deterioration, the absence of meningismus, progressive purpura, and base deficit. ● At Los Angeles Children's Hospital, 5 features were correlated with a poor prognosis: Shock or seizures, hypothermia, total WBC count less than 5000/mm, platelet count less than 100,000/mm, and development of Purpura fulminans. ● The overall mortality of invasive meningococcal disease is 7% to 19%. Prognosis
- 16. ● Sequelae of meningococcemia are skin necrosis (ischaemic infarction of skin and soft tissues), hearing loss, deafness, seizure, amputation, and skin scarring. ● Impaired organ perfusion due to hypovolemia, vasoconstriction, and myocardial failure result in prerenal failure manifesting as oliguria or anuria or acute tubular necrosis. ● Immunologic or reactive complications like arthritis, cutaneous vasculitis, iritis, and pericarditis are due to the deposition of immune complexes with polysaccharide antigen, IgG, and C3 resulting in acute inflammation. Complications
- 17. Vaccine Prevention ● Monovalent capsular group C meningococcal conjugate vaccines (MenC) are used in Europe, Australia, and Canada for routine immunization of infants and toddlers. They are highly effective, although a booster at adolescence is advocated. ● Quadrivalent meningococcal A, C, Y, W conjugate vaccines (Men ACYW) are used for adolescent immunization in North America. It is being used as a vaccine for high-risk groups and travelers in many countries. It is also replacing Men C as an adolescent booster outside the United States. ● Booster doses of Men ACYW are advocated in the United States for high-risk children and persons immunized at younger than 15 years of age. Capsular group B outer membrane vesicle (OMV) vaccines are used for outbreaks involving single clones. ● Two capsular group B vaccines (Men B-4C, 2 doses, and Men B-FHbp, 3 doses) are licensed for people older than 10 years of age. It is recommended for at-risk patients and outbreaks and can be given at 16 to 23 years of age at clinical discretion. Prophylaxis/Prevention
- 18. Chemoprophylaxis for Contacts of Patients of Meningococcal Disease Antibiotic Dose ● Rifampin: 10 mg/kg per dose; Orally every 12 hours for 4 doses (for infants younger than 1 month of age, 5 mg/kg per dose) ● Ceftriaxone: Single injection of 125 mg for less than 15 years and 250 mg for older than 15 years* ● Ciprofloxacin: 20 mg/kg (max 500 mg) older than 1 month of age* * From American Academy of Pediatrics Committee on Infectious Diseases. Red book 2015 Report of the Committee on Infectious Diseases, 30th edition. Elk Grove, IL, American Academy of Pediatrics 2015.
- 19. 1. https://www.ncbi.nlm.nih.gov/books/NBK534849/ 2. Batista RS, Gomes AP, Dutra Gazineo JL, Balbino Miguel PS, Santana LA, Oliveira L, Geller M. Meningococcal disease, a clinical and epidemiological review. Asian Pac J Trop Med. 2017 Nov;10(11):1019- 1029. [PubMed] 3. Harrison LH. Epidemiological profile of meningococcal disease in the United States. Clin. Infect. Dis. 2010 Mar 01;50 Suppl 2:S37-44. [PMC free article] [PubMed] 4. Dass Hazarika R, Deka NM, Khyriem AB, Lyngdoh WV, Barman H, Duwarah SG, Jain P, Borthakur D. Invasive meningococcal infection: analysis of 110 cases from a tertiary care centre in North East India. Indian J Pediatr. 2013 May;80(5):359-64. [PMC free article] [PubMed] 5. Törös B, Thulin Hedberg S, Jacobsson S, Fredlund H, Olcén P, Mölling P. Surveillance of invasive Neisseria meningitidis with a serogroup Y update, Sweden 2010 to 2012. Euro Surveill. 2014 Oct 23;19(42) [PubMed] 6. Coureuil M, Join-Lambert O, Lécuyer H, Bourdoulous S, Marullo S, Nassif X. Pathogenesis of meningococcemia. Cold Spring Harb Perspect Med. 2013 Jun 01;3(6) [PMC free article] [PubMed] 7. Dwilow R, Fanella S. Invasive meningococcal disease in the 21st century—an update for the clinician. Curr Neurol Neurosci Rep. 2015 Mar;15(3):2. [PubMed] 8. Halperin SA, Bettinger JA, Greenwood B, Harrison LH, Jelfs J, Ladhani SN, McIntyre P, Ramsay ME, Sáfadi MA. The changing and dynamic epidemiology of meningococcal disease. Vaccine. 2012 May 30;30 Suppl 2:B26-36. [PubMed] References