This document provides information on inspecting and palpating the respiratory system during a physical examination. Key points include:
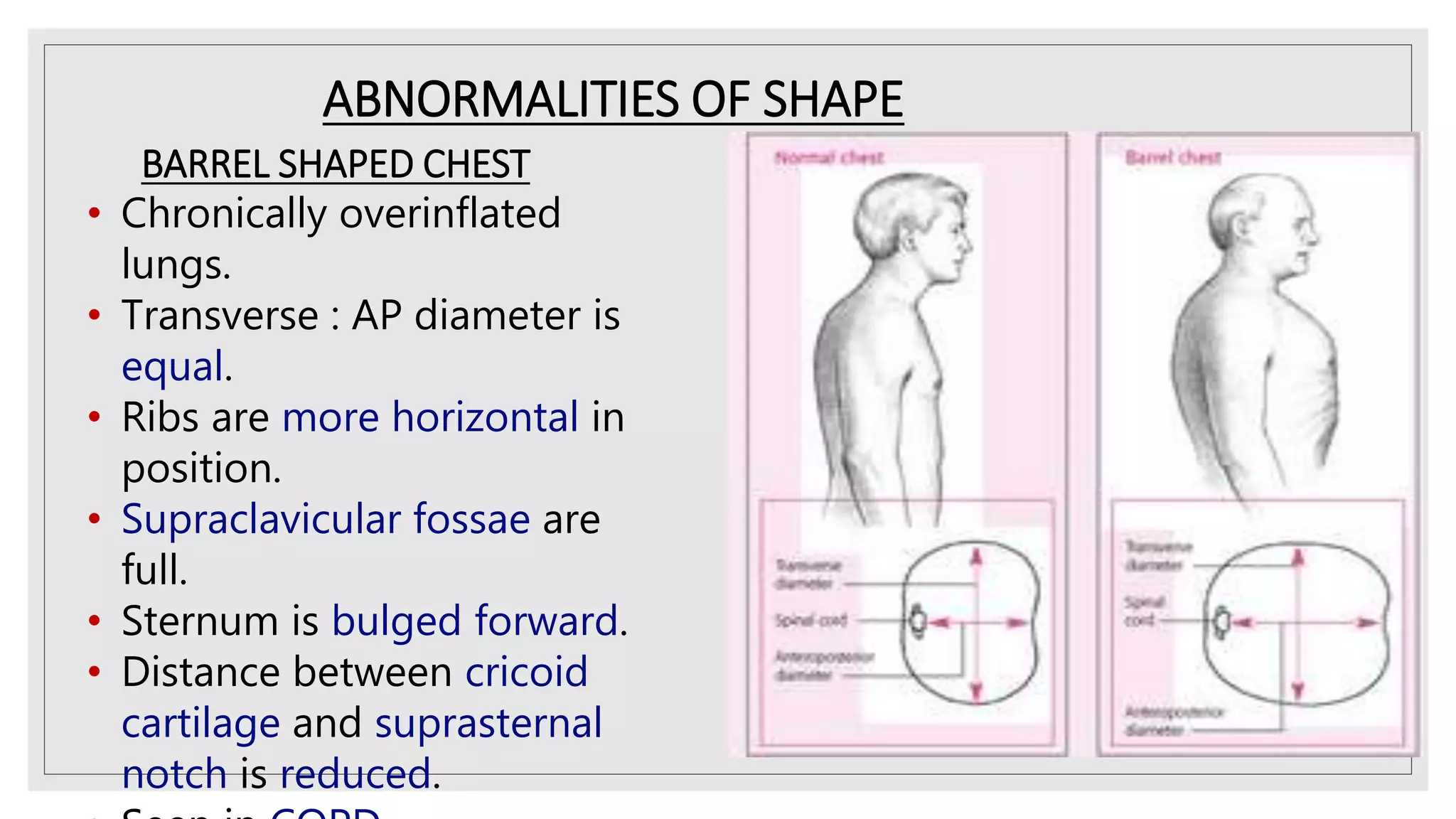
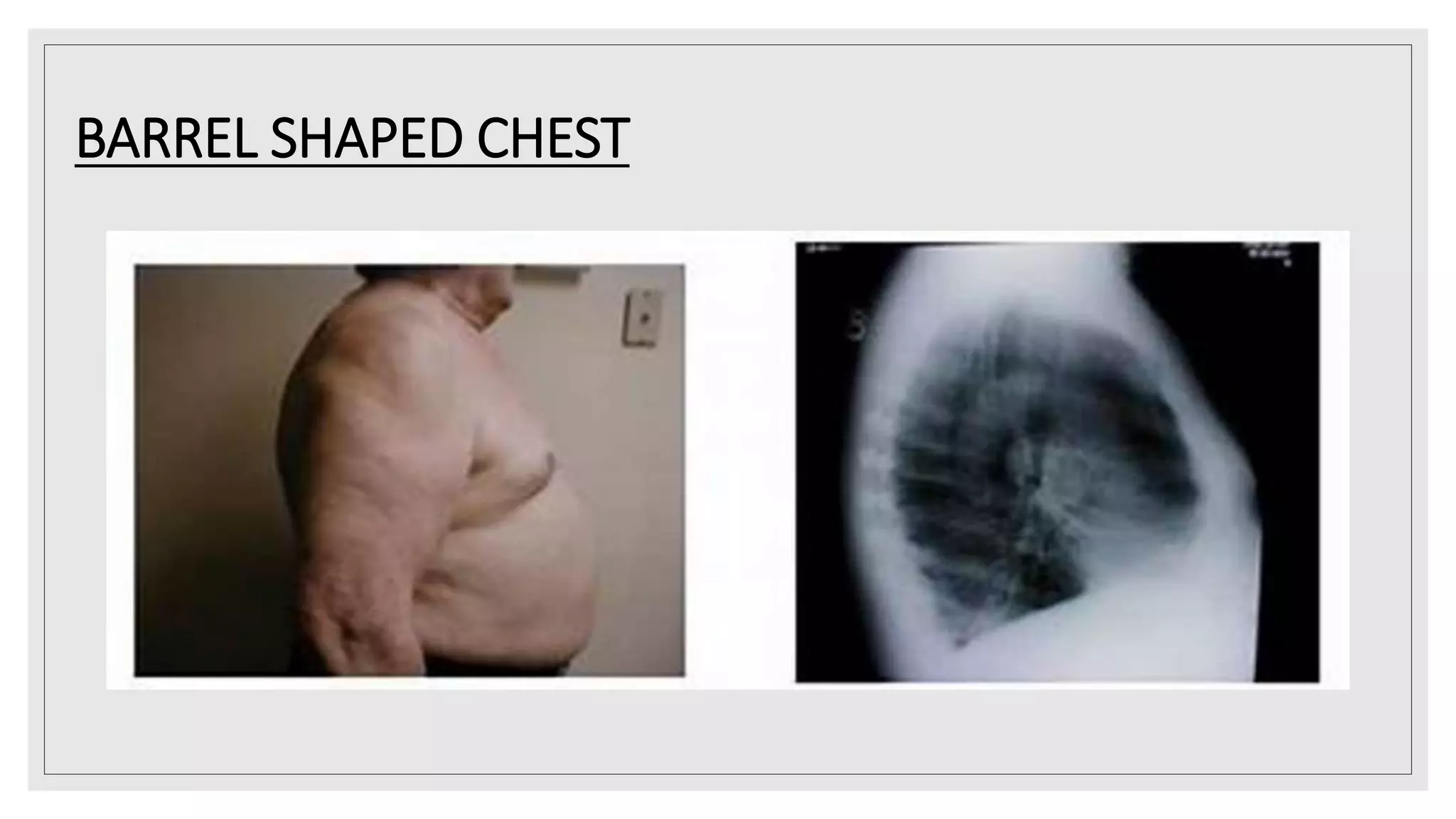
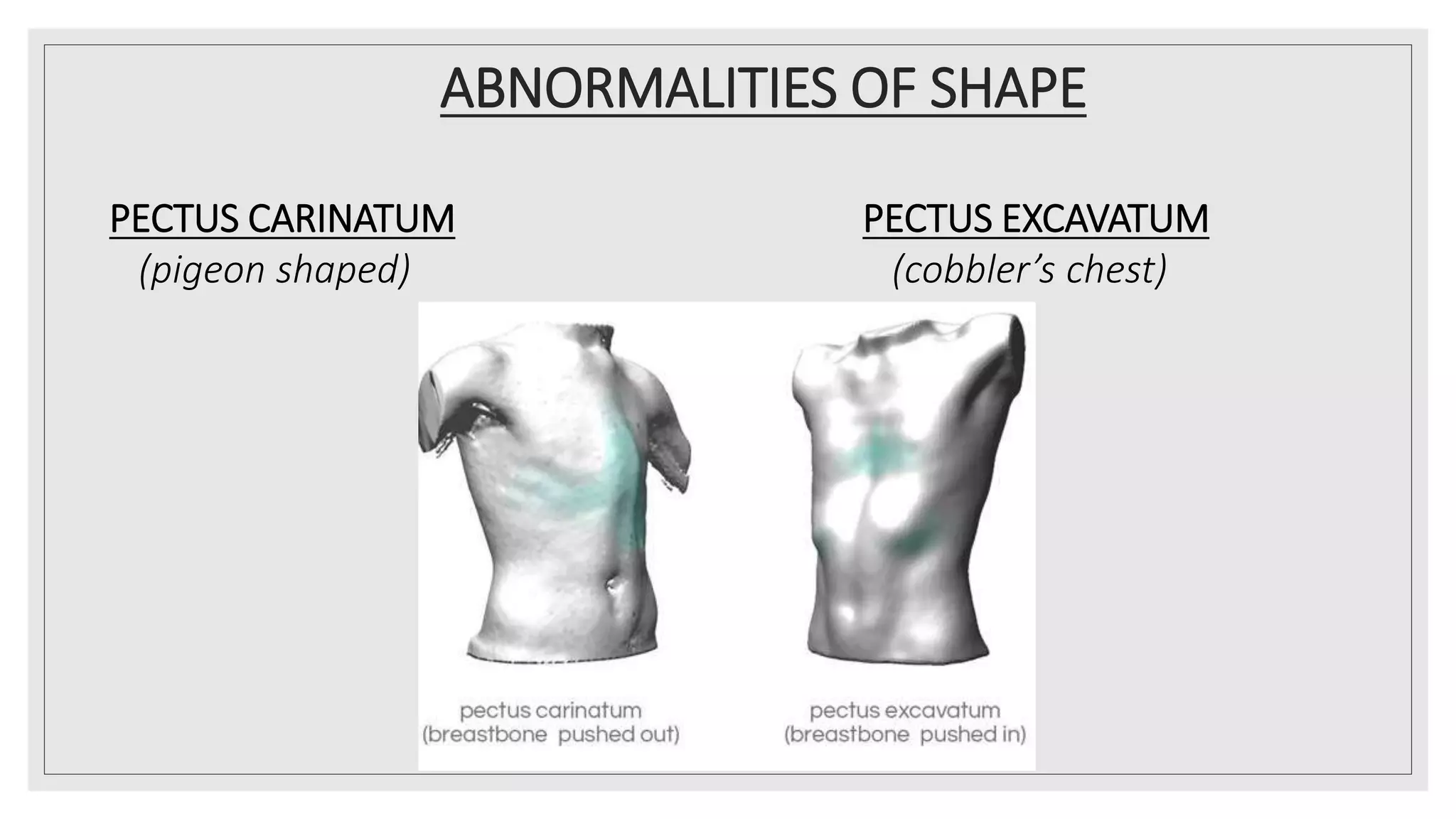
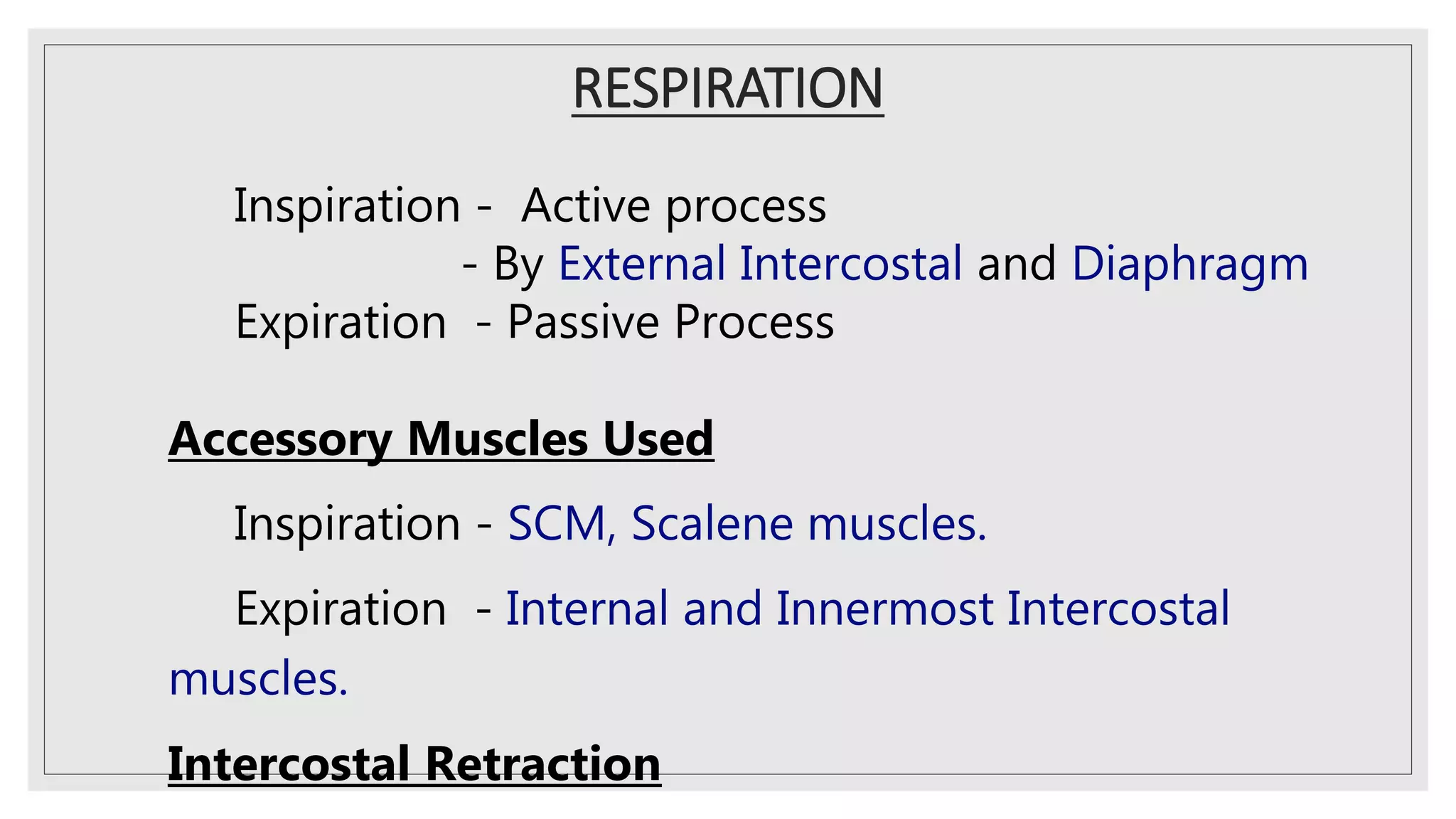
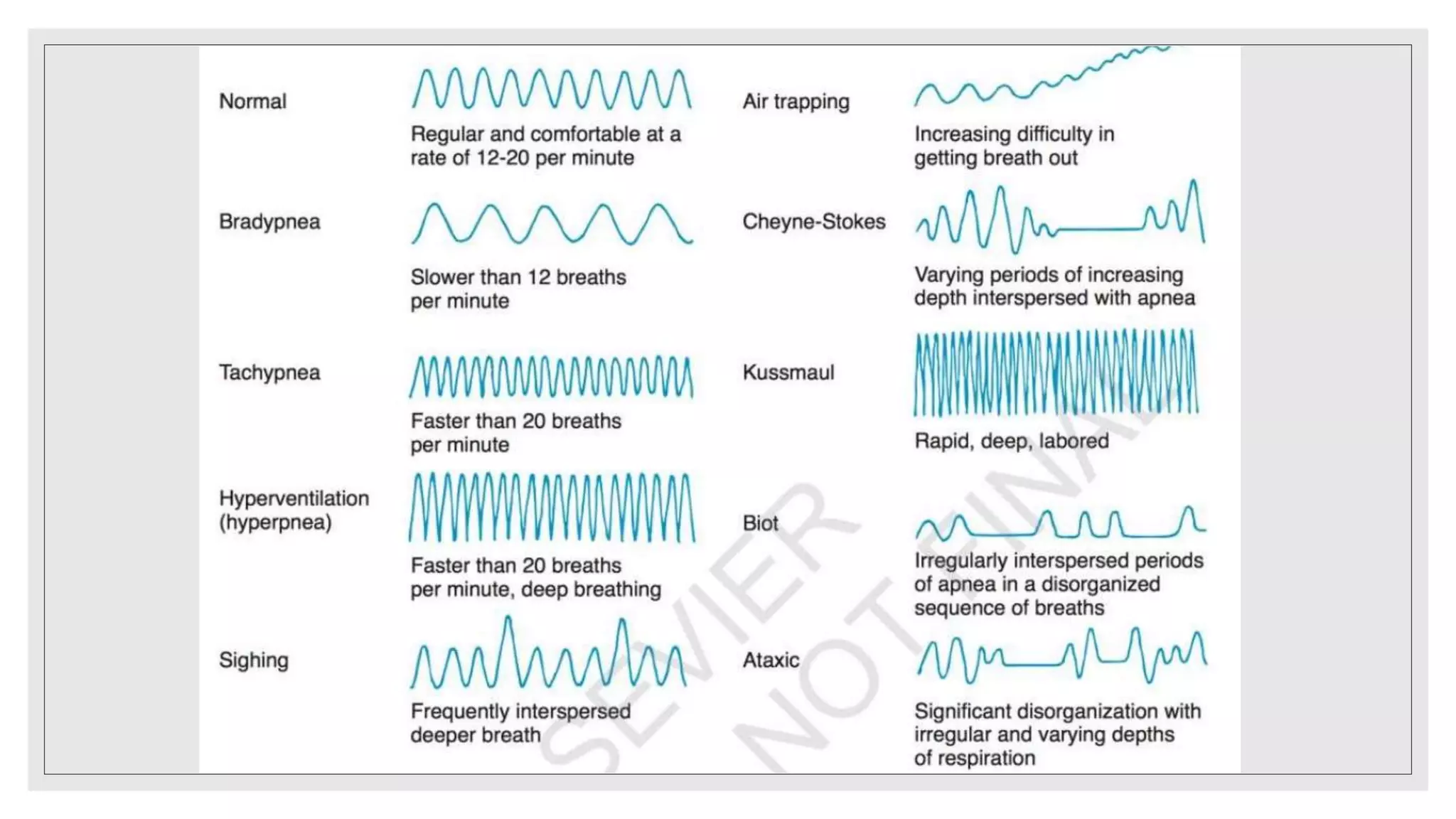
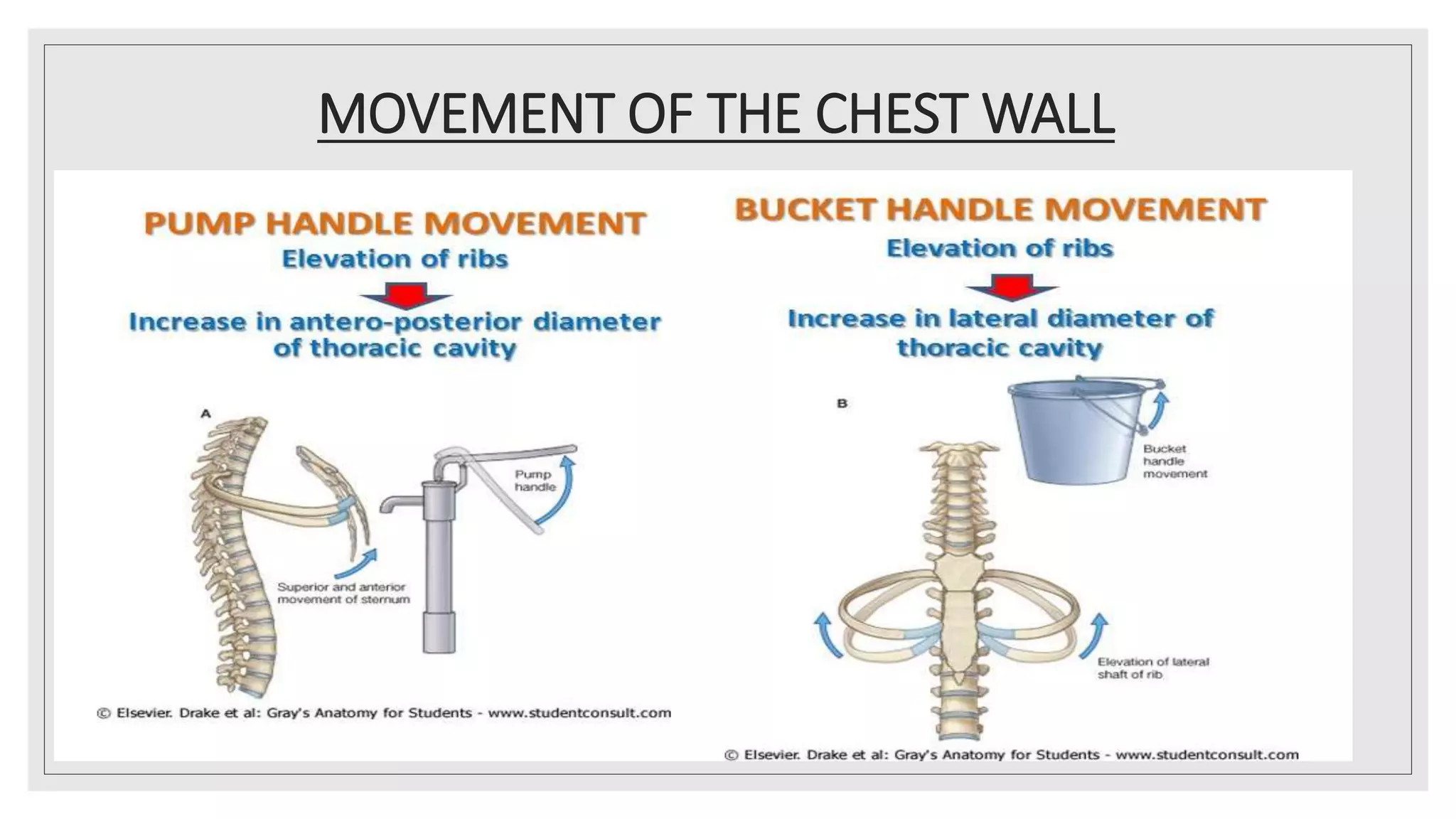
- Inspection involves observing symmetry, shape, size of chest wall, tracheal position, and respiration. Abnormal chest shapes include barrel-shaped, pectus carinatum, and pectus excavatum.
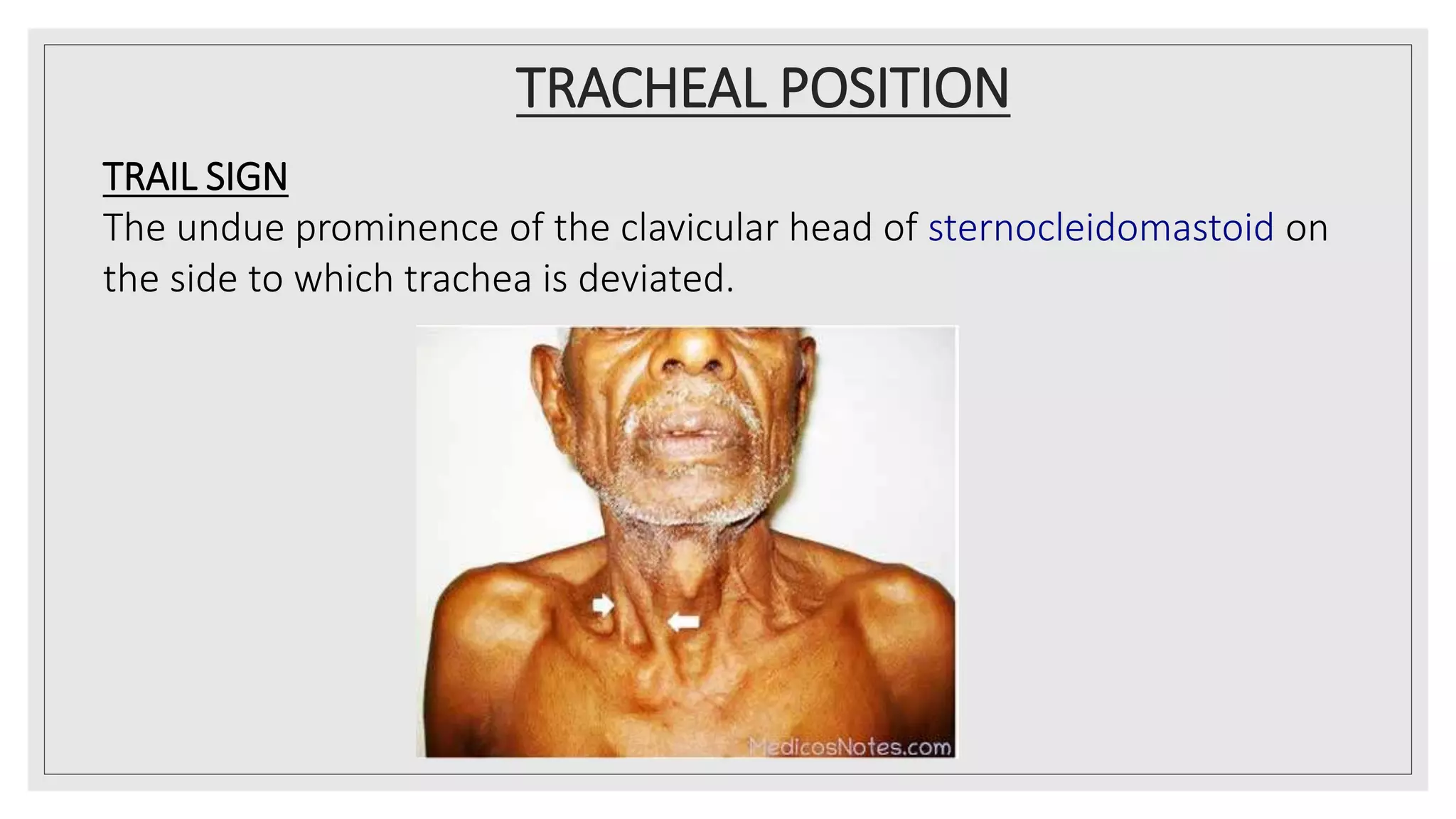
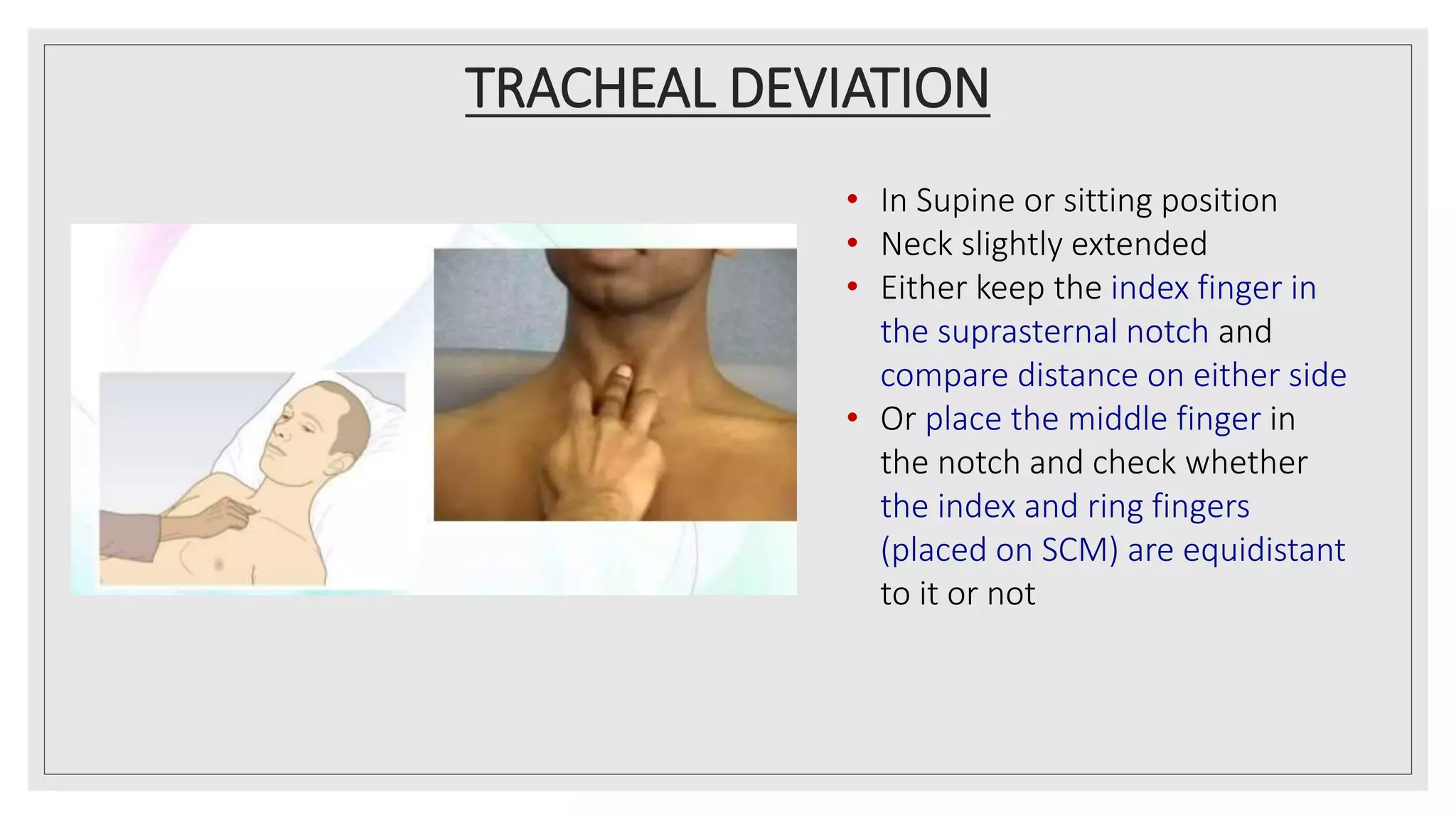
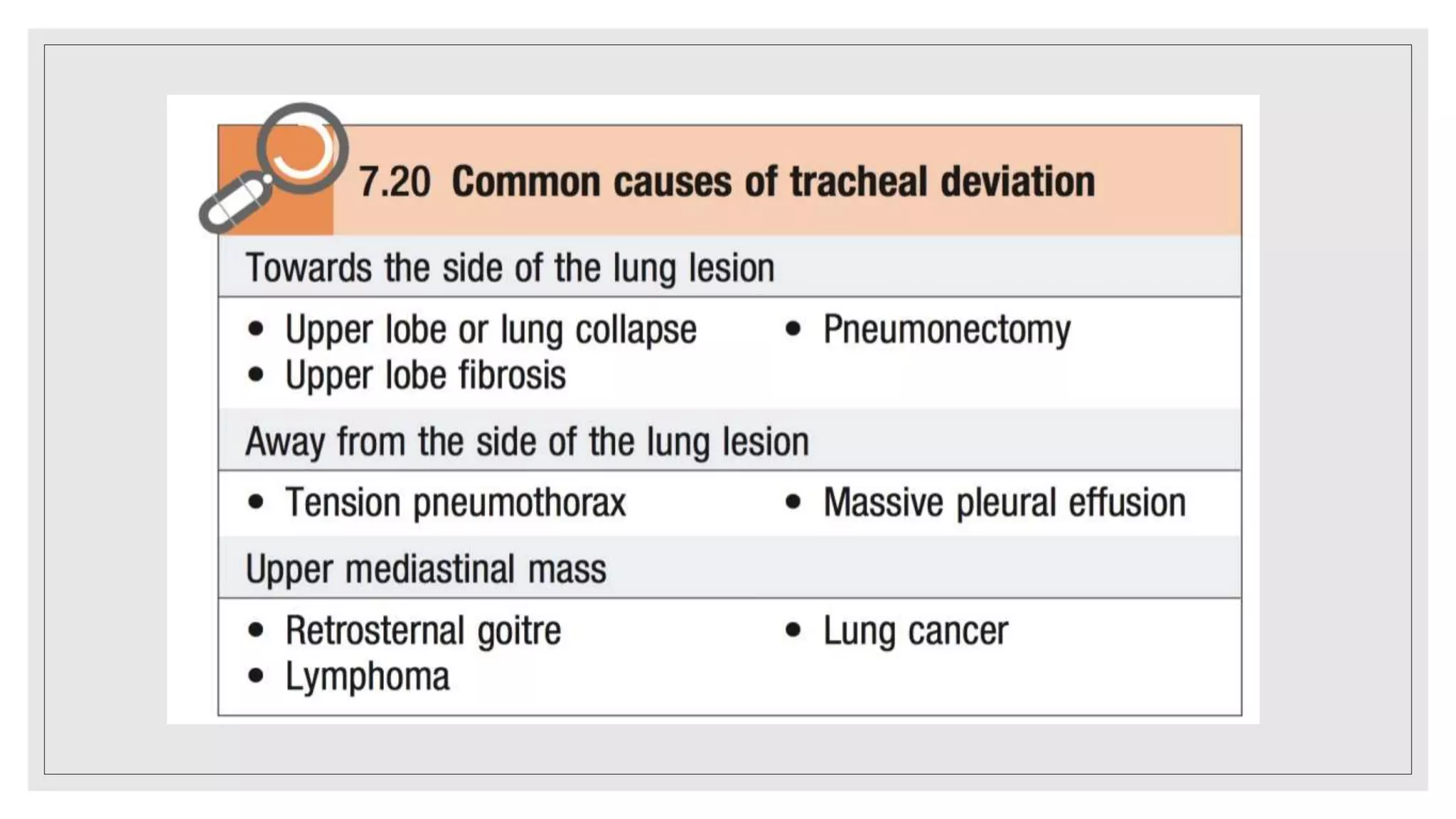
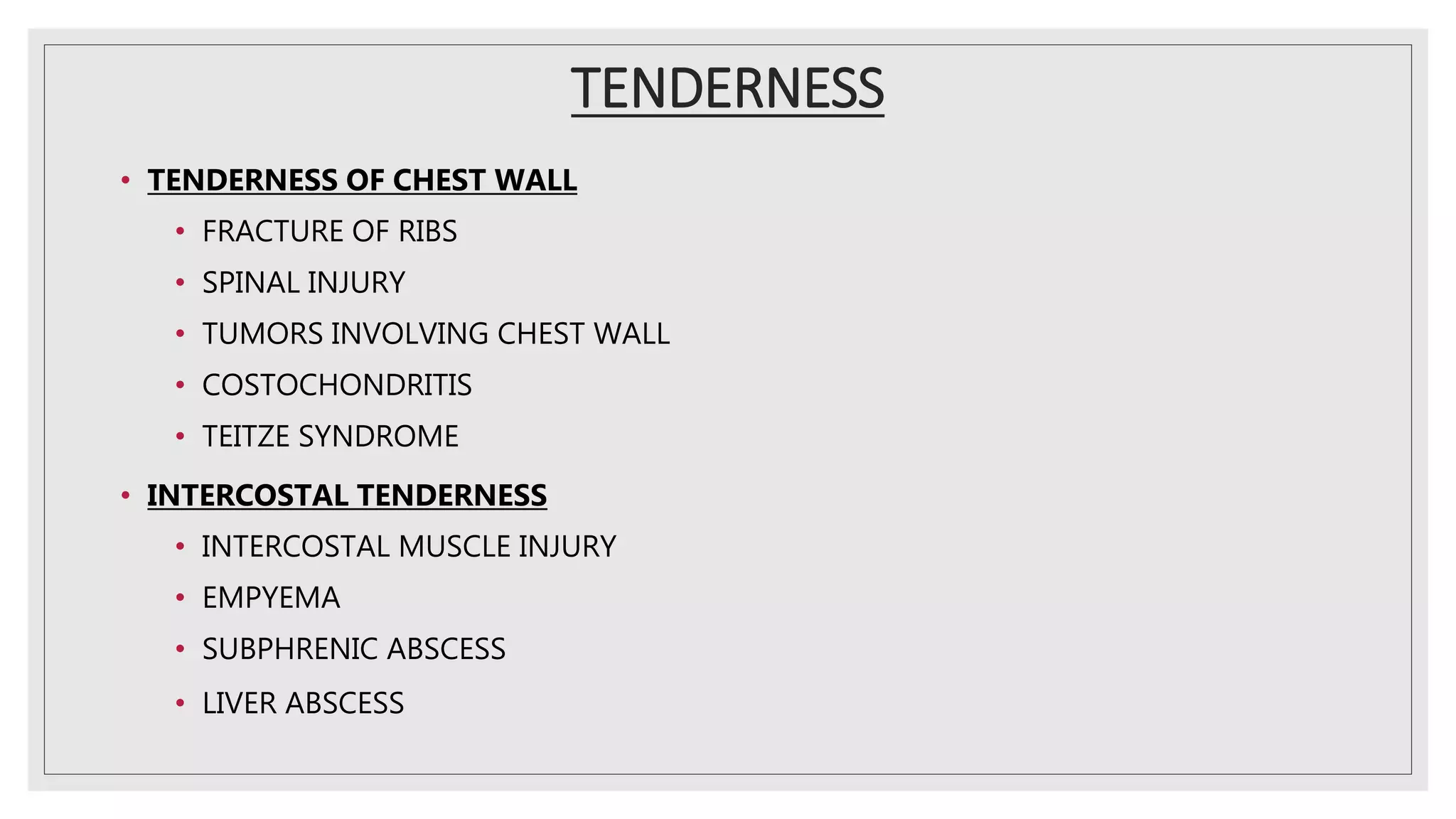
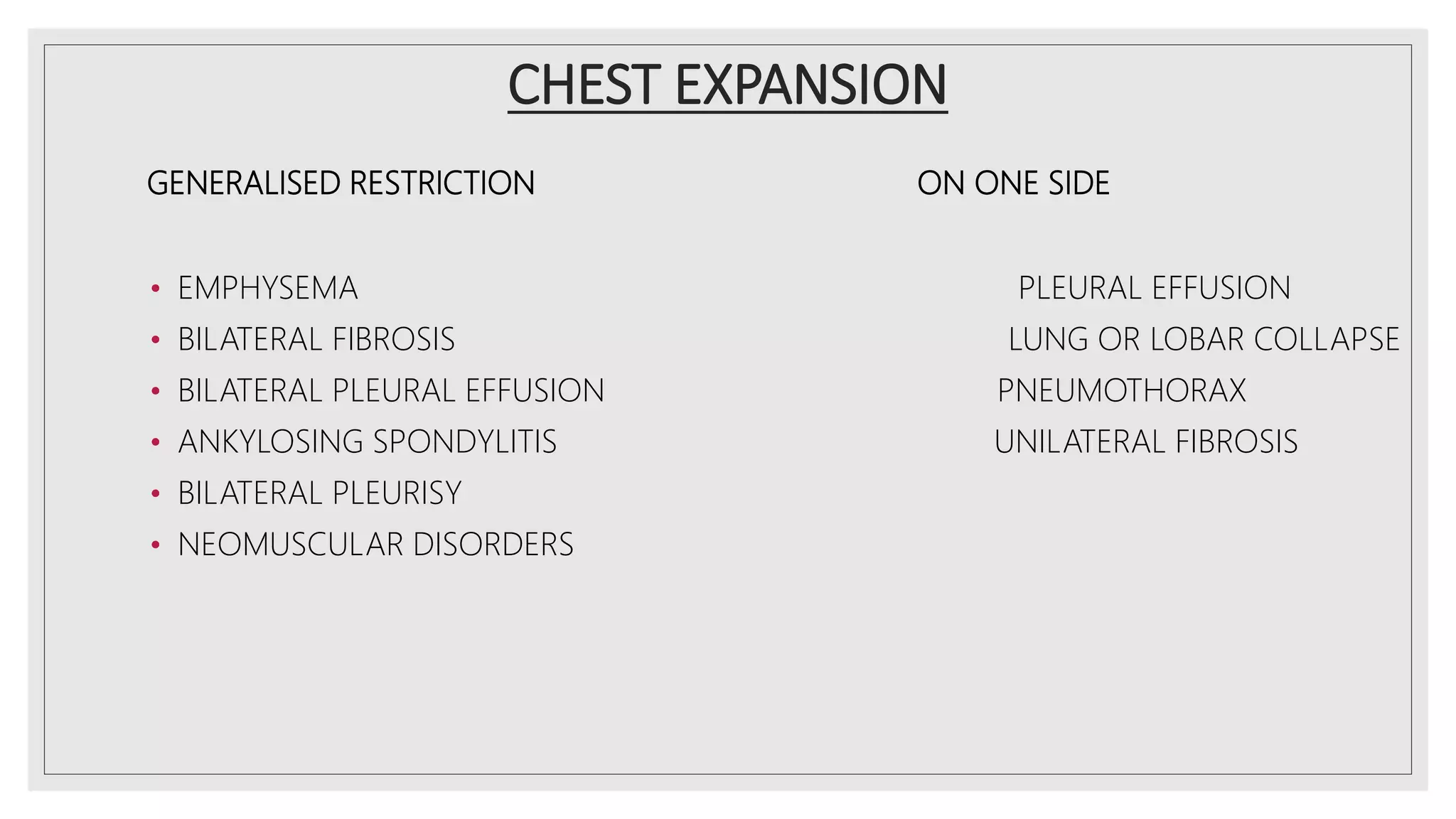
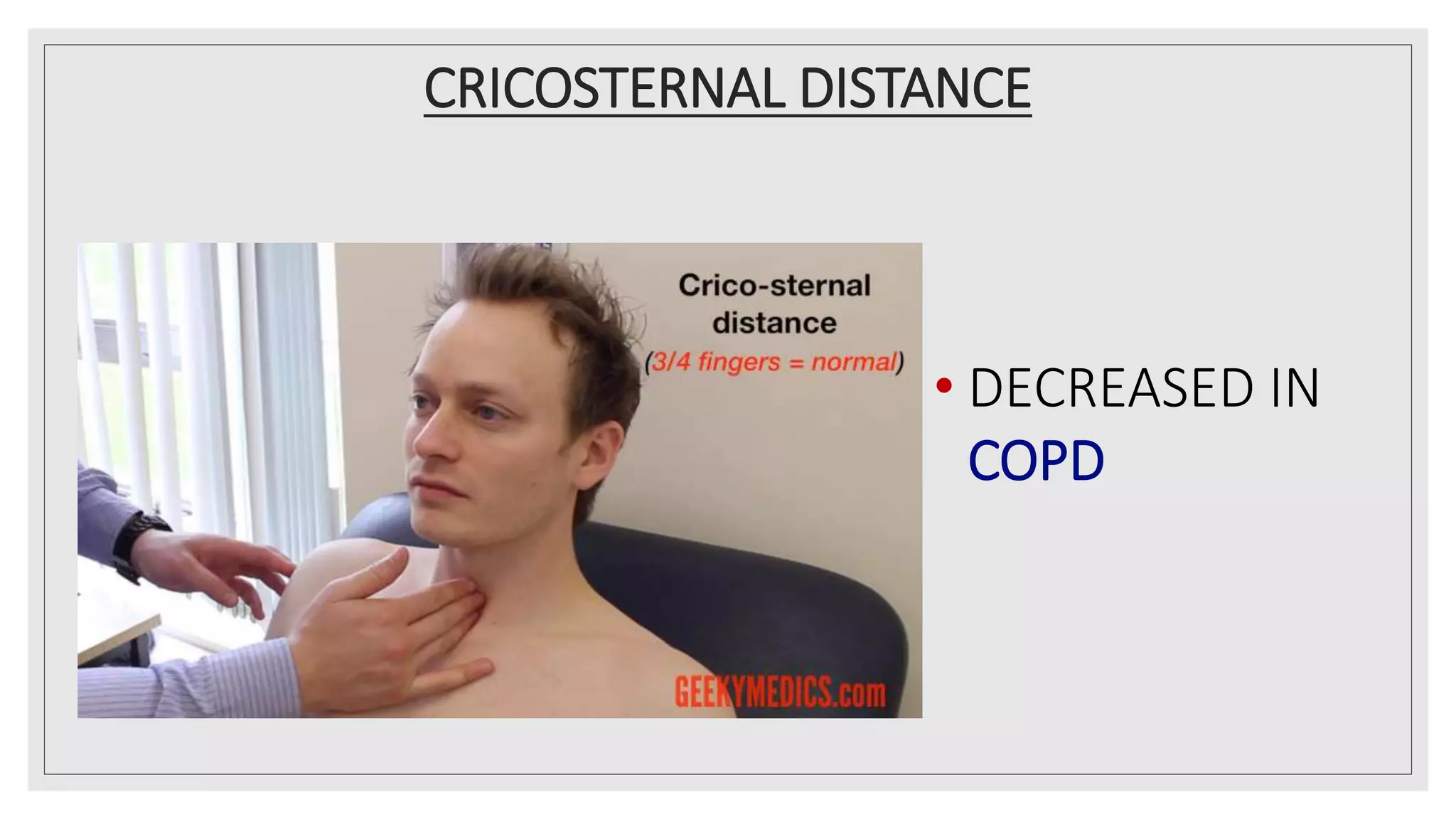
- Palpation is used to confirm inspection findings and check for tracheal deviation, tenderness, crepitus, chest expansion, apex beat, cricosternal distance, and vocal fremitus.
- Signs found on inspection and palpation can provide clues about underlying respiratory conditions such as COPD, pneumonia, pleural effusion, and lung



























































![chapter 4 Physical diagnosis [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/physicaldiagnosisautosaved-250416123318-d2df54aa-thumbnail.jpg?width=640&height=640&fit=bounds)


![Respiratory and Cardiovascular Exams.pptx [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/respiratoryandcardiovascularexams-230308035939-d7e720d1-thumbnail.jpg?width=640&height=640&fit=bounds)


























