Downloaded 91 times


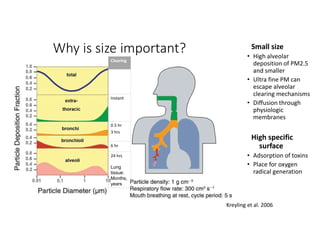
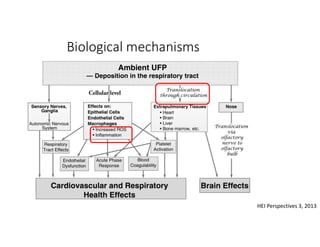

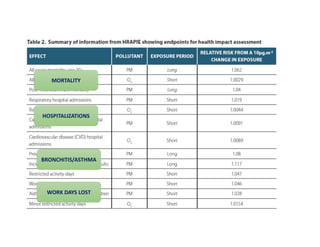
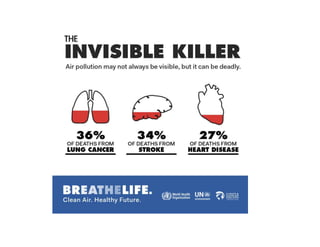
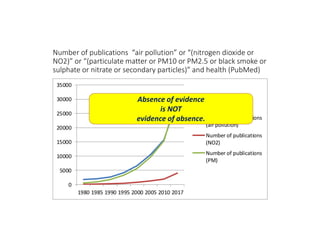


- Air pollution causes 6.5 million premature deaths per year, nearly half from outdoor sources. 80% of urban populations are exposed to unsafe air pollution levels according to WHO guidelines. - Small particulate matter can penetrate deep into lungs and cause health risks like asthma, chronic obstructive pulmonary disease, lung cancer, and cardiac issues. Biological mechanisms on the cellular level also contribute to health risks. - Numerous studies and growing evidence over decades show relationships between increased air pollution exposure and mortality, hospitalizations, and lost work days. However, absence of evidence is not evidence of absence of health impacts.























































































