Breast cancer
•Download as PPTX, PDF•
5 likes•4,964 views

1) Breast cancer is the second most common cancer in the US and the leading cause of cancer death in women over 65 years old. Risk factors include family history, genetic factors, age of first birth, and hormone use. 2) Breast cancer is divided into in situ carcinoma and invasive carcinoma. Invasive ductal carcinoma makes up 70-80% of cases. Staging involves the TNM system and considers tumor size, lymph node involvement, and presence of metastases. 3) Treatment involves surgery such as lumpectomy or mastectomy, radiation, chemotherapy, hormonal therapy, and targeted therapy. The type of treatment depends on cancer stage and biological markers. Neoadjuvant therapy is often used

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (19)
Similar to Breast cancer
Similar to Breast cancer (20)
More from ministry of health
More from ministry of health (20)
Recently uploaded
Recently uploaded (20)
Breast cancer
- 1. BREAST CANCER Dr/Omar Hashim
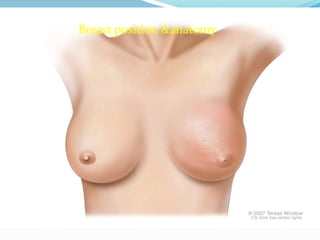
- 3. Breast anatomy The breasts are specialized accessory glands Of the skin that capable of secreting milk nipple small and surrounded by areola. The breast tissues consists of ducts embedded in connective tissue. The breast extended from2nd intercostals up word to the 6th intercostals down ward & from lateral margin ofsternum to the midaxillary line the majar part of the breast lies in the superficial fascia. Small part called called axillary tail extended to the deep fascia
- 5. each breast consists of 15-20 lobs which radiated out from The nipple .the main duct from each lobes open separately On the nipple .these is fibrous tissue in between for sport And take the breast it is normal feature Lymphdrainage ;- for lymph drainage the breast is divided Into quadrants , the lateral ones drainage to the axillary the medial ones drainage internal thoracic groups Then to the SCV . The axillary lymph nodes divided into three Levels by relation to pectorals minor muscle ;- Level one ;-(low axillary)= nodes inferior and lateral to the -Pectoralis mi Level tow ;- (mid axillary) =nodes directly beneath the Pectoralis minor muscle. Rotter’s ;-interpectoral nodes consider level tow and are
- 6. Between pectoralis major & minor . Level three ;-nodes superior/medial to the pectoralis minor
- 7. BET OF MATTED AXILLARY LYMPH NODS
- 9. Epidemiology &Etiology The second common cancer in USA representing 26% of all cancer . And 15% of all cancer deaths . Is the 1st leading cause of. *caner death in women over 65 yrs . Breast cancer is more common in whites women but black women are more likely to die from their disease . Risk factors;- past history---BRCA1&BRCA2 --↑age ---early menarche – late menopause – nilliparty – first birth after the age 30 yrs – Atypical lobular hyperplasia – Atypical ductal hyperplasia – long term postmenopausal estrogen replacement –early exposure to ionizing radiation
- 10. Pathology of ca breast The breast cancer is divided into two major group 1)insitu carcinoma 2) invasive carcinoma . The insitu subtypes inculed ;- ductal carcinoma insitu DCIS 15-20% -- lobular carcinoma insitu LCIS the invasive carcinoma subtypes include ;- 70-80% infiltrating duct cell carcinoma . 10% infiltrating lobular . The remaining of the invasive subtypes are mucinous, tubular, .papillary, & medullary Paget’s disease is nipple involvement with disease
- 15. Baget’disease
- 17. (in mammography) only10% ca breast can not be detected
- 18. Clinical breast exam every 1-3 yrs & periodic self exam recommended in young adulthood
- 19. Annual clinical exam & screening mammog-
- 20. Raphy to 40-50 yrs in USA
- 21. Screening mammography ±MRI in high risk pts
- 23. BIRADS ->
- 25. Work up Be side hx /exam / breast xam/lymph nods exam Bx with estrogen &progsteron receptor Studs –her-2-neu status ki-67 CBC-----Blood chemistries ---LFS Cxray-----breast imags Bone scan –head images when indicated
- 26. BIRADS=Breast Imaging Reporting and Data system American College of Radiology
- 28. *
- 30. TNM Stagin;- Tx;-tumor not assessd. T0;-no evidance T1;-tumor ≥20 mm in greater dimension;- T1a;-tumor > 1mm but ≤ 5mm in greater dimension T1b;-tumor> 5mm but ≤ 1omm in greater dimension T1c;- tumor > 10mm but ≤ 20mm in greater dimension
- 31. T NM contuation p;- T3;- tumor > 50mm in greater dimension T4a;-extension to chest wall not pectoralis muscle invasion T4b;- ulceration,ipsilat satellite noduls, edema,peau orange of not inflamm-carc- T4c;- both T4a & T4b T4d;- inflammtory carcinoma
- 32. Regional lymph nodes (N);- Nx;-LNs not assessted N0;-no L Ns mets N1;- mets to ipsilat- level 1,11 axillary LNs N2a ;- met to ipsilat- level 1,11 fixed to one another N2b;- mets- to clinical detected internal mammary LNs with out axillary LNs .
- 33. TNM Contus;- N3a;- mets- ipsital- infraclavicular level 111 LNs N3b;-mets- to ipsilat- internal mammary LNs + axillary LN N3c;- mets- to ipsilat- supraclavicular LNs Distant mets-.M0;-no distant met….CM0;- only microscopic mets M1;-mts- detcted clinically &radiographic
- 34. Staging group of ca breast;-
- 35. Staging 5- yrs survival 1V 16%
- 36. prognosis Prognosis of the breast cancer depents on number of factors ;- The most important factor is axillary LNs Then tumor size . Histological grade . Age of Pt Biological sub type as defined by molecular markers Pts- with ER and pR negative slightly worse Prognosis than pts- with either ER or PR +ve or both
- 37. Biological subtype based onER,PR &HER2;-
- 39. Surgery ;-BCS ;- quadratectomy, wide excision & Lumpectomy (local excision) qض quadratectomy lumpectomy
- 41. Variation of mastectomy Radical mastectomy ;-remove of the breast,pctoralisminor, pctoralis major ,axillary LN(ALND) ;-
- 42. Modified Radical Mastectomy ;- Remove of the breast level of the pectoralis minor ALND level 1,11
- 43. Total mastectomy (simple);- removal of the breast to level of pectorali minor with out LNs dissection
- 44. Skin sparing mastectomy ;- preserves of skin and nipple/areola complex for enhance reconstructive outcome
- 45. chemotherapy Recommended for > 1cm tumor or nodes +ve . Adjuvant chemotherapy reduces LR .Anthracycline based rgimens and taxans for high risk disease .recent evidence suggest ↑DFS and OS with taxans base therapy as compared to anthracycline.FAC;regim consist of 5flurouracil+doxorubicin+cyclophosphamide usually 4 to6 cycle every 3weeks usually start immedially after surgery other regim CMF P-cyclophosphamide+methotrexate+ 5fluorouracil
- 47. Neoadjuvant chemotherapy ;- Consider stander care in high risk patients such as advanced stage, Young patient Also evaluated in stage 11,111 in randomized trials The advantage of neo-adjuvant CH;-Assessment of di- Sease response & ↑rate of BCT Complete clinical (cCR)and pathological response rate (PCR) In advanced stage disease 20%-40% achieve cCR after Neo-CH-and 10%-20% achieve CR 1/3 OF PCR have pathological disease
- 48. Neoadvuant chemotherapy ;- If the initially clinical LNs +ve full axillary LNs dessetion Regared less of the Reponses to neoadvuant chemother- Apy . Trastuzumb (hercptin);- human monoclonal anti- Body for HER2 neu over experation , IV administration Concurrent anthracycline chemo- for 1 yrs in other Study 2yrs . Studies show that use of chemo + trastuzu- Mub ↑3yrs DFS 87% while in chemo- only 75% .but Associated with ↑risk of heart failure or cardiac death
- 49. Adjuvant Hormonal therapy ;- Gnerally recommended for all ER +ve pts. We need to Do complete ovarian suppression /ablation in pre- Menopausal women.SERMS (tamoxifen) is indicted For both pre- and postmenopausal pt-s .associated With side effect ;- ↑bone mineral density, hot flashes, ↑risk of thromoembolic disease, endometrial proliferation & uterine cancer. Aromatase inhibitors indicated for postmenopausal pts
- 50. NSABP B-14 ;- in which randomization between Tamoxifen 5yrs and placebo. Adjvant tamoxifen Improved 15 yrs DFS (HR=0.58) and OS (HR=0.80) and Other study compare between anastrozole Tamoxifen or both
- 51. Radiation therapy ;- For radiation ;-indication Adjuvant treatment after lumpectomy for Dcis &early invasive ca breast Adjuvant treatment after mastectomy for↑risk pts locally advanced disease (iflammatory breast disease) Palliative treatment for mets-
- 52. ;- Techniques for breast irradiation Whole breast EBRT is delivered using 3D-CRT for Dcis And early stage invasive breast cancer Selected nodal irradiation to the supraclavicular,axilla ,and internal mammary nodes when pathologically +ve Partial breast irradiation using brachytherapy or EBRT in special case In local advanced disease irradiation of the breast or chest wall ,supraclavicular ,axilla ,with or with out internal mammary is planned
- 53. Radiation tech- ;- Usually radiation began in 2-4 w after surgery . For receiving cth- radiation began after last cycle . Pt- treated in supine position with customized immobilization . Bilateral arms abducted and externally rotated . Ware surgical scar . Target volume is entire breast using tangential fields &SCV
- 54. Mark estimated medial, lateral, cranial, and caudal Field borders ;- 1) Medial border at midsternum 2)Lateral border placed 2cm beyond all palpable breast Tissue (midaxillary line). 3)Inferior border is 2 cm from inframammary fold . 4) Superior border is at head of clavicle or second Intercostal space . 5) Deep intrathoracic field border must be non diver- Gent and edges made coplanar
- 55. Whole breast irradiation by tangenial field ;-
- 56. Tech-con Use half beam block tchniques, or rotate gantry to make Symmetric and align posterior edge of each tangent . (gantry rotation angle= arctan ({0.5 field with }SAD ) ~3 For 10 cm field. Isocenter is typically placed in the center of the treatment, lunge is acceptablegeneral 1-2cm of underlying in
- 57. For left sided lesion we have to ↓the radiation to the Heart in the tangential field . CT planning is required for more accurate dose distri- Bution. Rarely we need to treat completely dissected axilla Although axillary failure is un common . Rt tangential usually cover large percentage of level1,11 Of the axillary nodes . High tangent of technique can be used to treat great Percentage of the axilla if no axillary dissection perfor- med
- 58. When using 3rd (SCV) attention to geometric match Helf beam block for -- With tangential field Caudal edage of supraclavicular field to eliminate Divergenve . Divergence of tangential fields superiorly can be Eliminated with various tech;- Couch kick away from tangent field ; arctan {(0.5X Tangetial field length })
- 59. Supraclavicular LNs irradiation field
- 61. Partial breast irradiation by brachytherapy
- 62. Insitu carcinoma Representing 20%-22% of diagnosis ca breast usually by mammography. Dcis ;-BCT with lumpectomy ±RT.RT is indicated to reduce LR,Total mastectomy (TM)is indicated to for diffuse malignant,microcalification,multicentric disease,persistant +margin. Lcis;-lifelong close observation±tamoxifen for risk ↓ (↓ invasive cancer rate by 56% ). Mastectomy if strong FH ,diffuse disease, genetic predisposition as prophylacisis bilateral
- 63. Treatment of early- stage breast cancer (stage 1,2A);- Lumpectomy wjth radiation . Breast conservation surgery (BCS) followed by radiation Relative contraindication ;- Gross mullicantric . Pregnance . Prior irradiation . Scleroderma . Post mastectomy radiation is not indicated for early stage Disease . In BCS radiation radiation ↓ local recurrence
- 64. Study show that lumpectomy with radiation is superior To mastectomy in ↓local recurrence while no deferent in The OS , distant metastasis , contralatral breast cancer New 1ry malignance and locoregional recurrence no Significantly different
- 65. stage 11B&111 ;- Local advanced breast cancer include large espectram From simple large 1ry to aggressive inflammatory breast Cancer . Treatment usaully is multimodality surgery ,chemo-therapy which is adjuvant or neoadjvuant. The adjuvant in locorgional advanced breast cancer recently a companied with trastuzumab in HER2- +ve . Trial with the use of trastuzumab with adrimycin, Cyclophosphamide & paclitaxel show ↑of 3 yrs DFS &OS Treatment of local advanced ca breast
- 66. con- stage 11B, 111 ;--> Neoadjuvant chemotherapy ;- The Neo-ch followed by mastectomy With adequate down stage BCS can be done . In clinical trial excluding inflammatory breast cancer Using operable AC (A; adriamycin . C; cyclophoshpamide ) ->D (docetaxel) versus AC S(surgery) -> D ,PCR (pathological complete response ) Favored the 2nd one (p;0.001)
- 67. Treatment of locally advanced breast cancer (stage11B &111)
- 68. Oprable local advanced disease;-
- 69. Inoperable in local advanced disease ;- Hormonal
- 70. Treatment of the inflammatory breast cancer ;- BIC is treated with combined modality of therapy Neoadjuvant cth- , surgery , radiation. Clinical trial IBC AND LABC (local advanced breast Cancer );- using doxorubicin, vincristine, cycloph- Osphamide and 5fu- followed by local treatment which include ;-mastectomy, and radiation (pre- or post- surgery) with median follow up of 10 yrs where Median OS, and DFS were 70% and 45%
- 71. Treatment of locally recurrent Due to improvement of BCS local recurrent occur in 10-15%. Although mastectomy is the current standard These is 2nd chance of BCS with brachytherapy
- 72. Treatment algorithm for inflammatory breast cancer ;-
- 73. Operable ;- due to complete or partial response ;-
- 74. Inoperable (No response or progression) in IBC
- 75. Male breast cancer ;- Male breast oflen present with palpable mass uasully have high incidnce of lumph nodes met- At presentation . ↑of male ca breast associated with Family hitory BRCA 1, 2 & testcular dysfuction . Treatment usually is mastectomy with either axllary LNs sampling or dissection
- 76. Clinical evidence of the treatment of the breast cancer ;-
Editor's Notes
- Mi=minor
- *2nd leading cause of cancer death
- Dcis = ductal carcinoma in situ . Lcis = lobular carcinoma in situ
- * =1 in the age groub 59-60 yrs . ↓*2 =stronge family history or history of LCIS . BRCA 1 or 2 .
- * Propsed algorithm for palpable breast cancer
- FNA = Fine needle espiraton
- Luminal A =favorable prognosis , will respond to endocrine therapy , less response to chemotherapyLuminal B = prognosis worse than A.HER 2 = poor prognosis – but use of trastuzumab ↑ improvementTriple –ve =basal ,poor clinical prognosis . Although some benefit from chemotherapy
- EBRT =External beam RadioTherapy
- Tech- =techniques
- SCV =Supraclavicular lymph nodes
- BCT = breast concerveting surjeryDcis =ductal carcinoma in situLR = Local recurrence .FH= Family history
- Bx =biopsy ---- LN = lymph nodes MRM = Modified radical mastectomy
- Neoadj =Neoadjevuant ---- cth =chemotherapy ---- BCS =Breast conservative surgery
- lymph nodesLN = ---Mammo =mammography ----bx =biopsy