This document summarizes information about breast carcinoma, including:
- Pakistan has the highest rate of breast cancer in Asia, with approximately 90,000 new cases diagnosed annually.
- Common risk factors include age, family history, obesity, lack of breastfeeding, and environmental toxins.
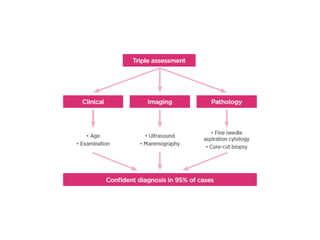
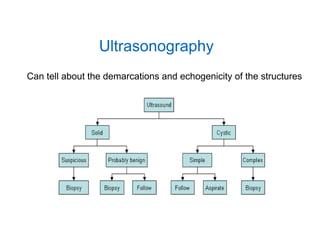
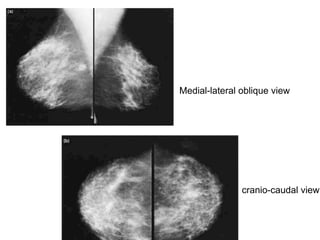
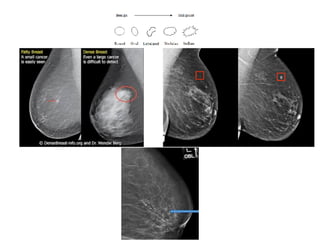
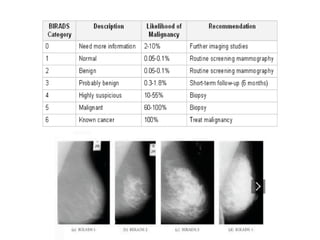
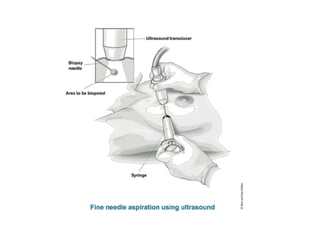
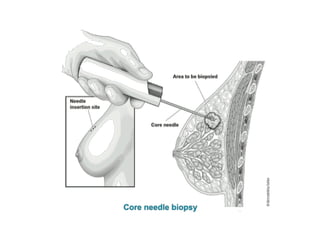
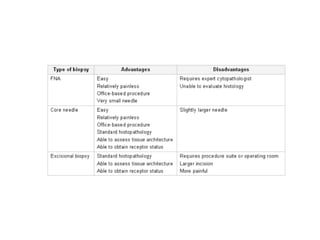
- Screening is recommended annually with mammography after age 40. Diagnosis involves biopsy of suspicious lumps.
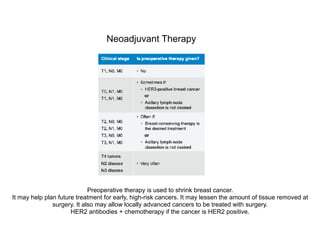
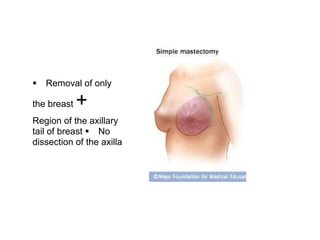
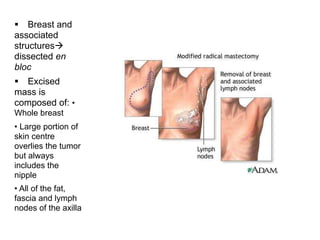
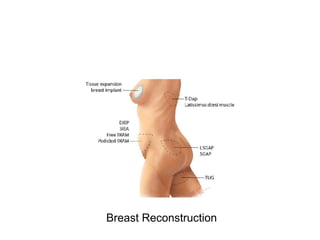
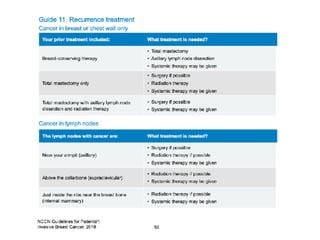
- Treatment options include surgery, chemotherapy, radiation therapy, hormone therapy, and reconstruction as needed.























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














