Downloaded 2,904 times








![General 4: Crush Syndrome[traumatic rhabdomyolitis]Serious medical condition characterized by major shock & renal failure following a crushing injury to skeletal muscles or tourniquet left too longBywaters’ Syndrome](https://image.slidesharecdn.com/complicationoffracture-110112042527-phpapp01/75/Complication-of-fracture-107-2048.jpg)
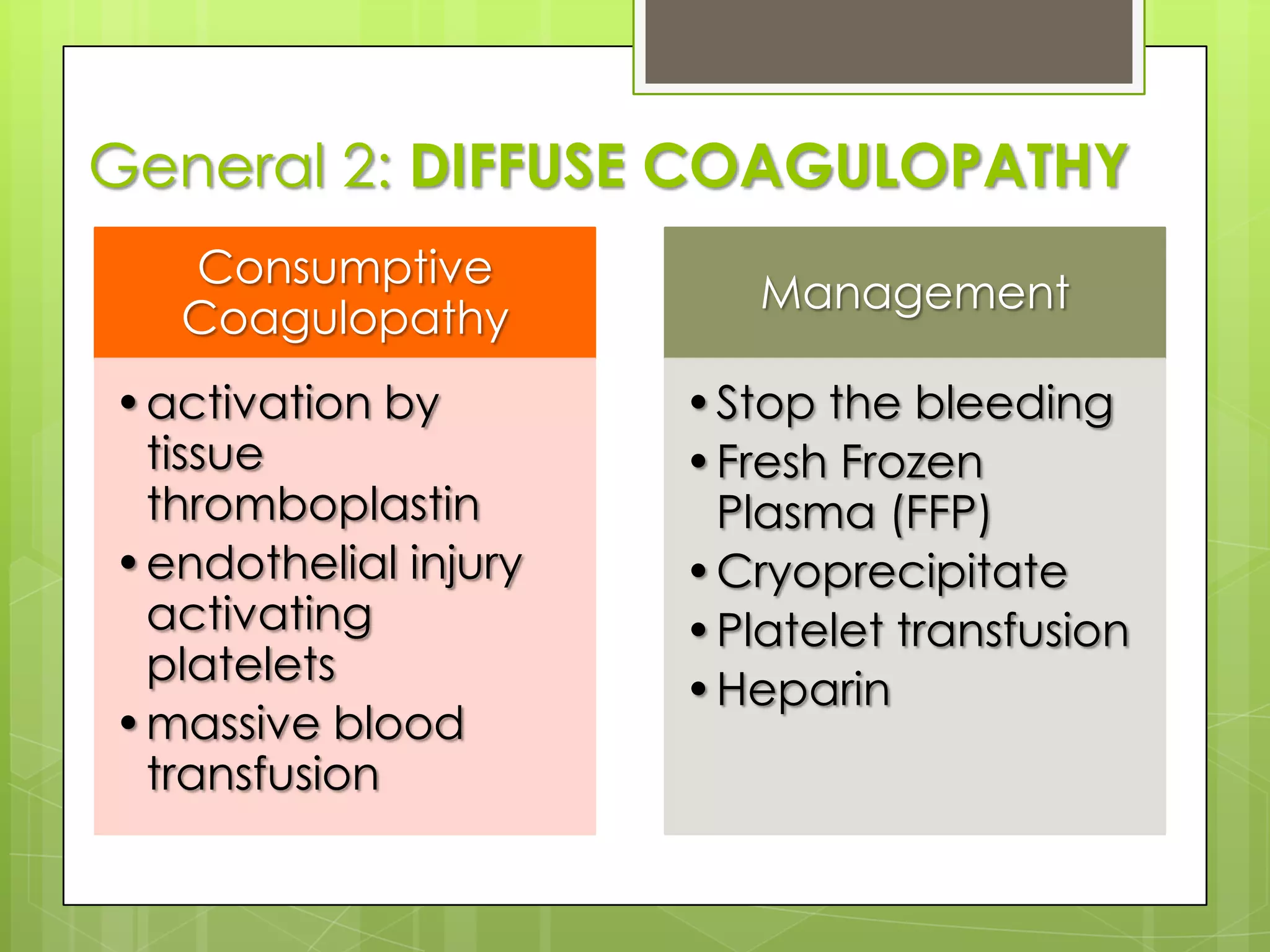
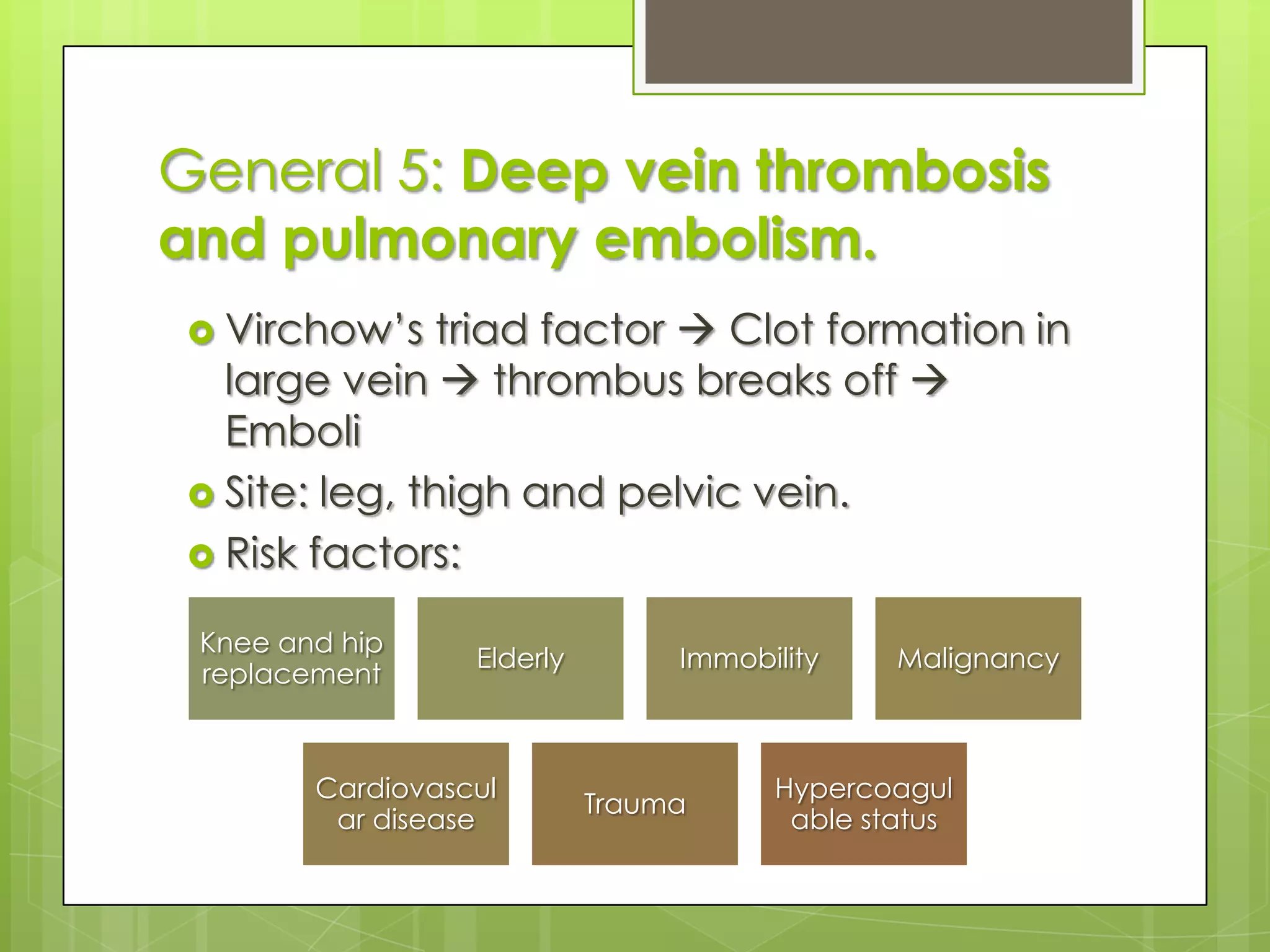
![General 6: Fat EmbolismSKIN: Fat droplets obstruct alveolar capillaries thromboplastin release consumption of coagulation fx & platelets DIVC/Skin necrosis PetechiaLUNG: Fat droplets obstruct alveolar capillaries thromboplastin release alter membrane permeability / lung surfactant oedema respiratiory failure [V/Q Mismatch]BRAIN: Fat droplets obstruct capillaries confusion coma/fits death](https://image.slidesharecdn.com/complicationoffracture-110112042527-phpapp01/75/Complication-of-fracture-113-2048.jpg)
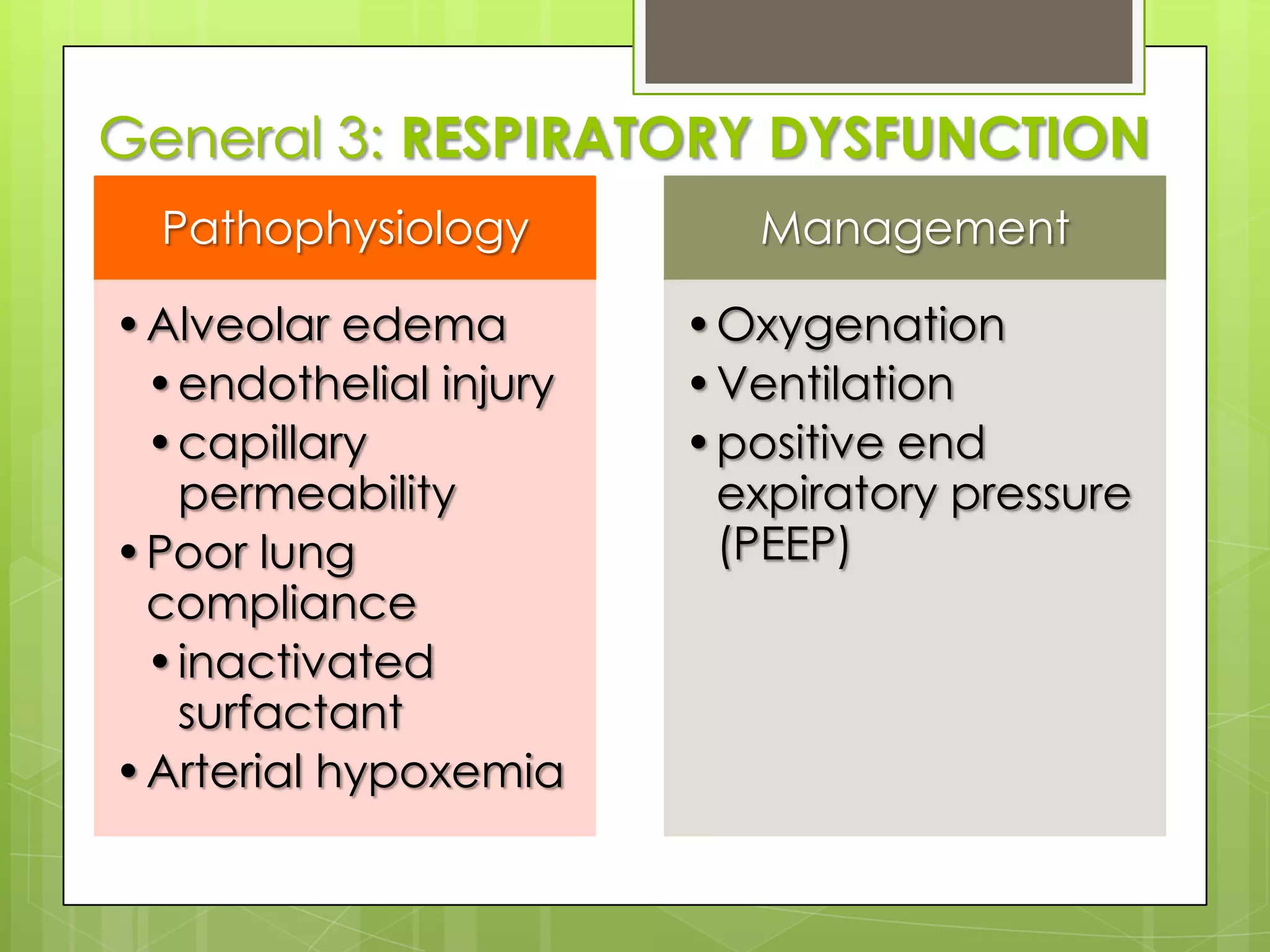
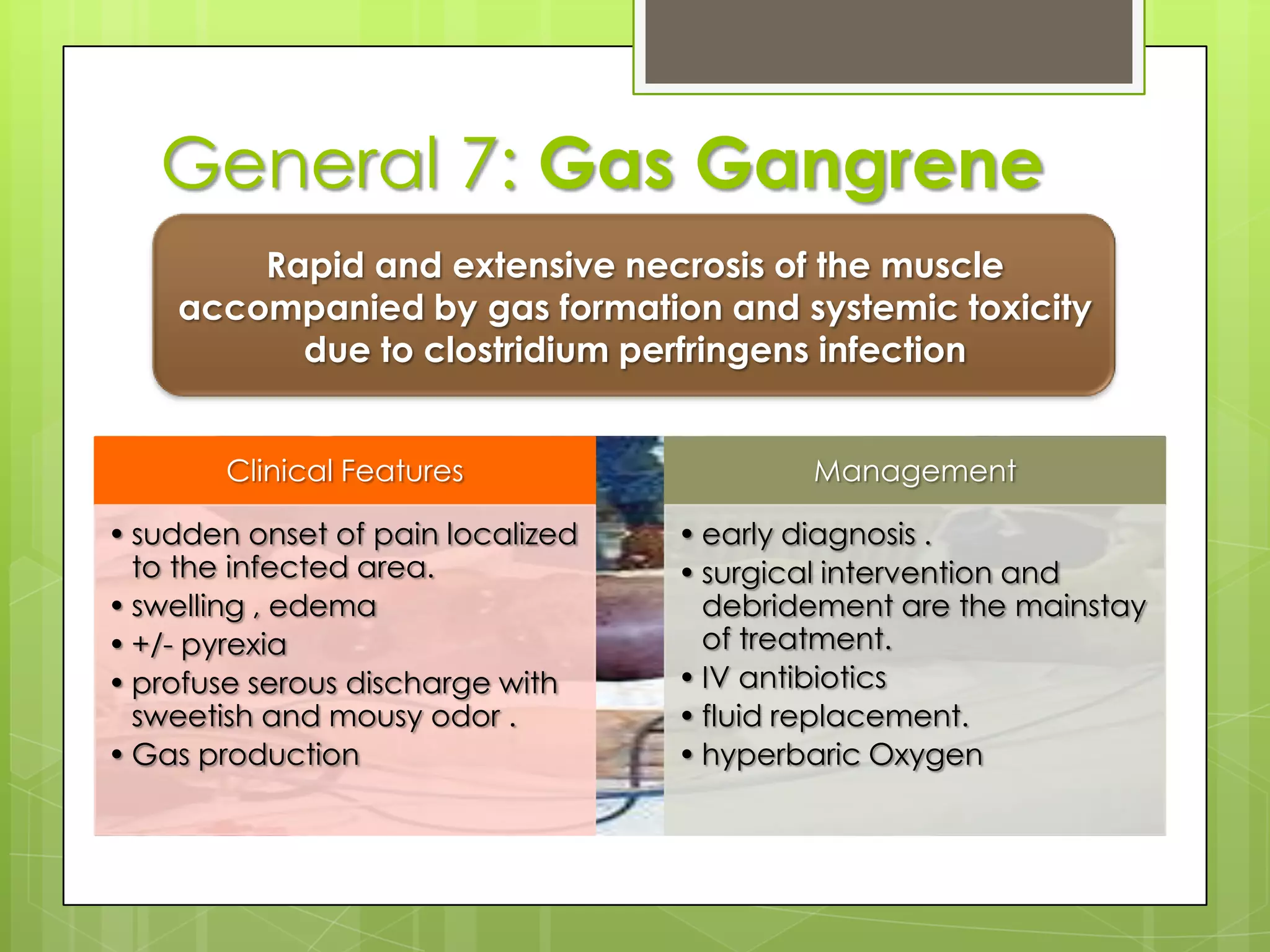
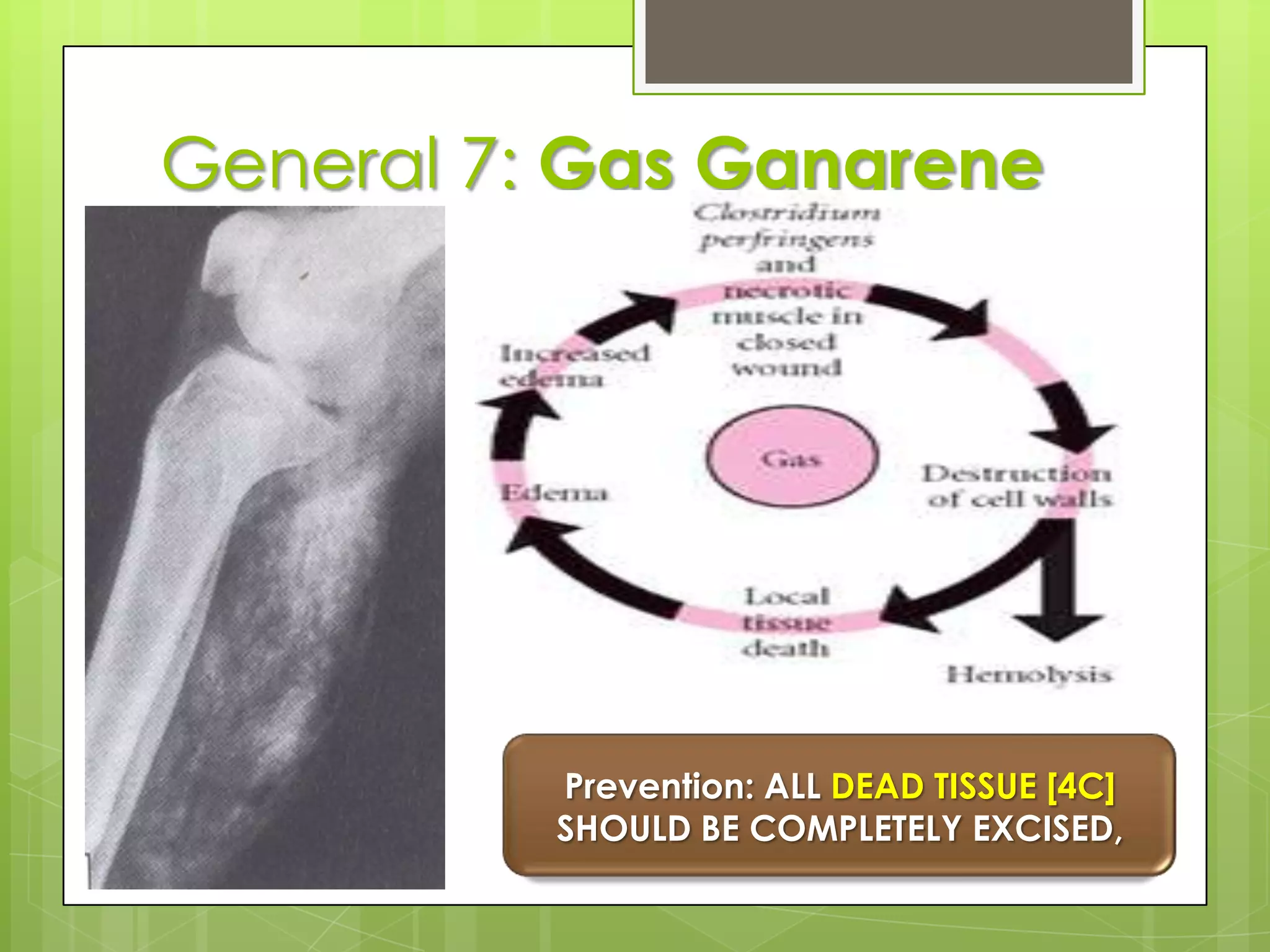
![General 7: Gas GangrenePrevention: ALL DEAD TISSUE [4C] SHOULD BE COMPLETELY EXCISED,](https://image.slidesharecdn.com/complicationoffracture-110112042527-phpapp01/75/Complication-of-fracture-115-2048.jpg)
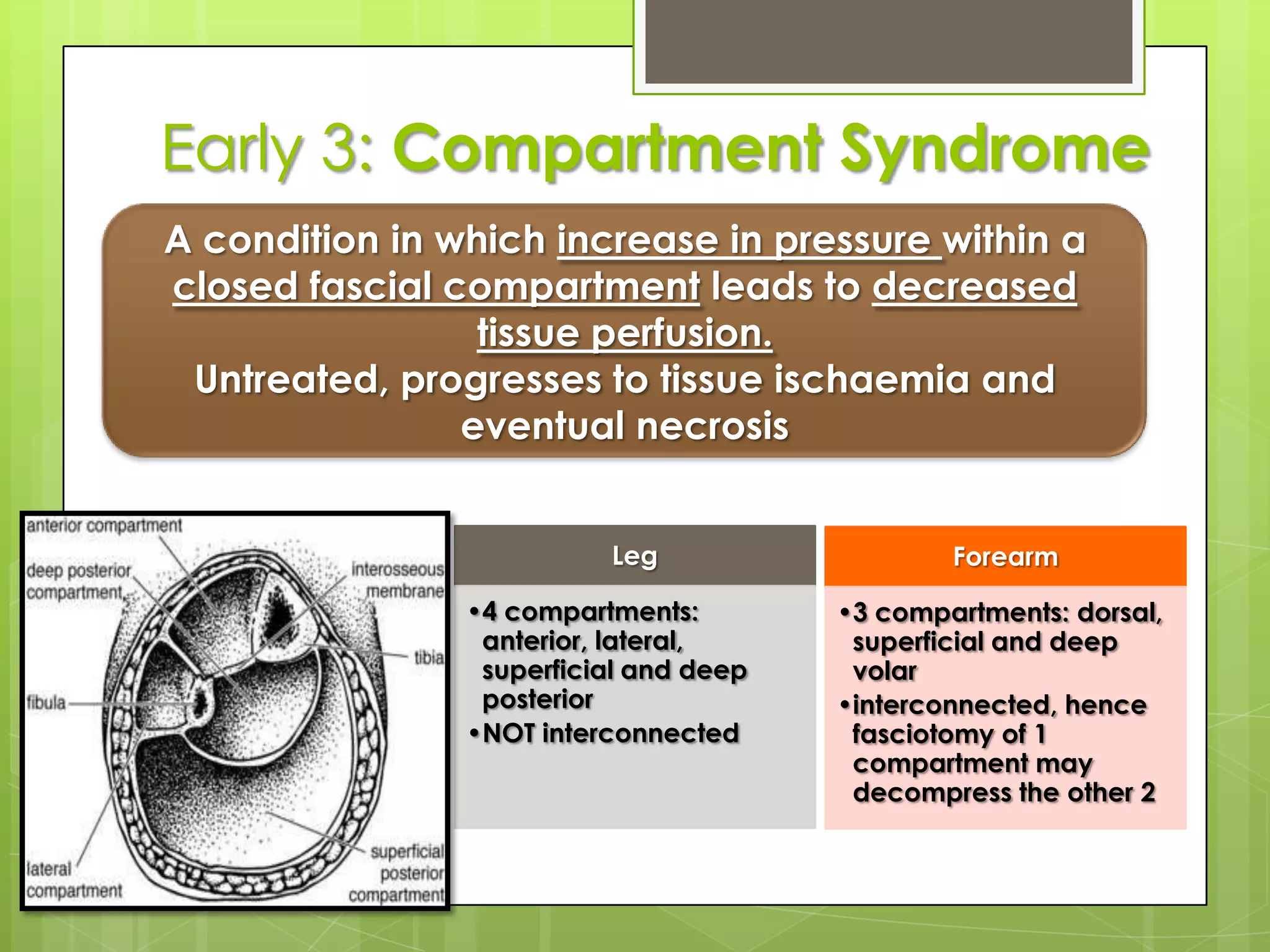
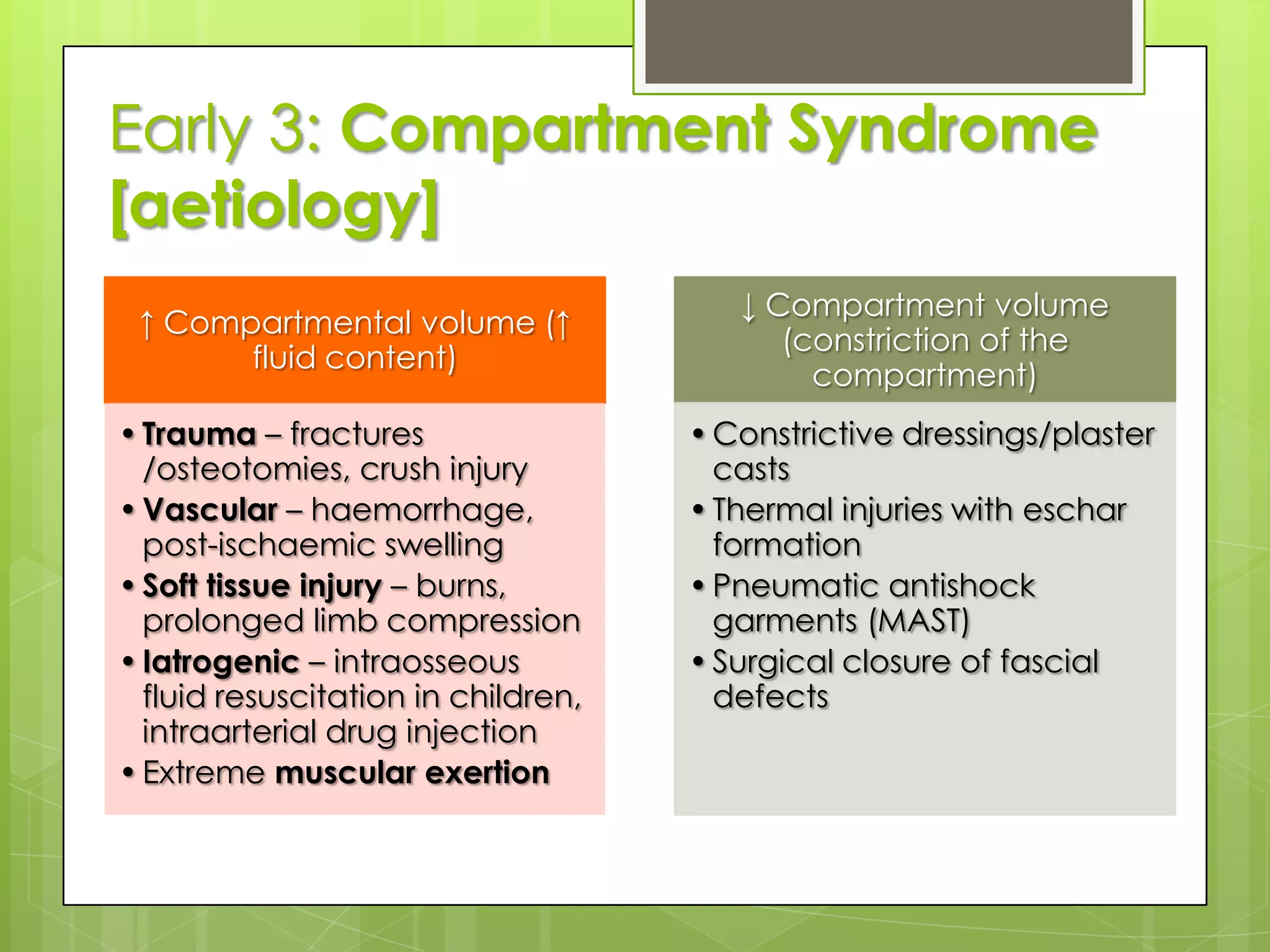
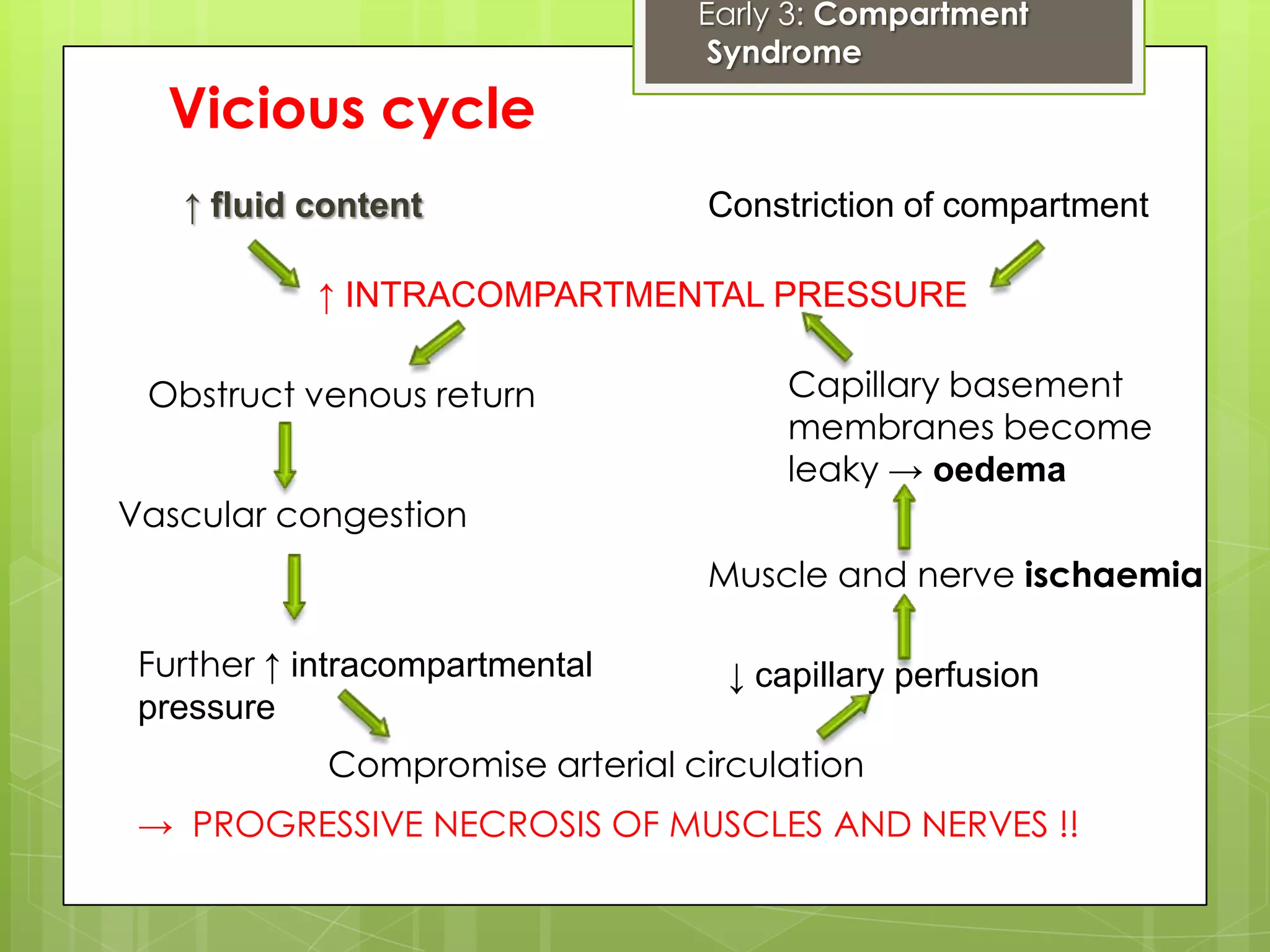
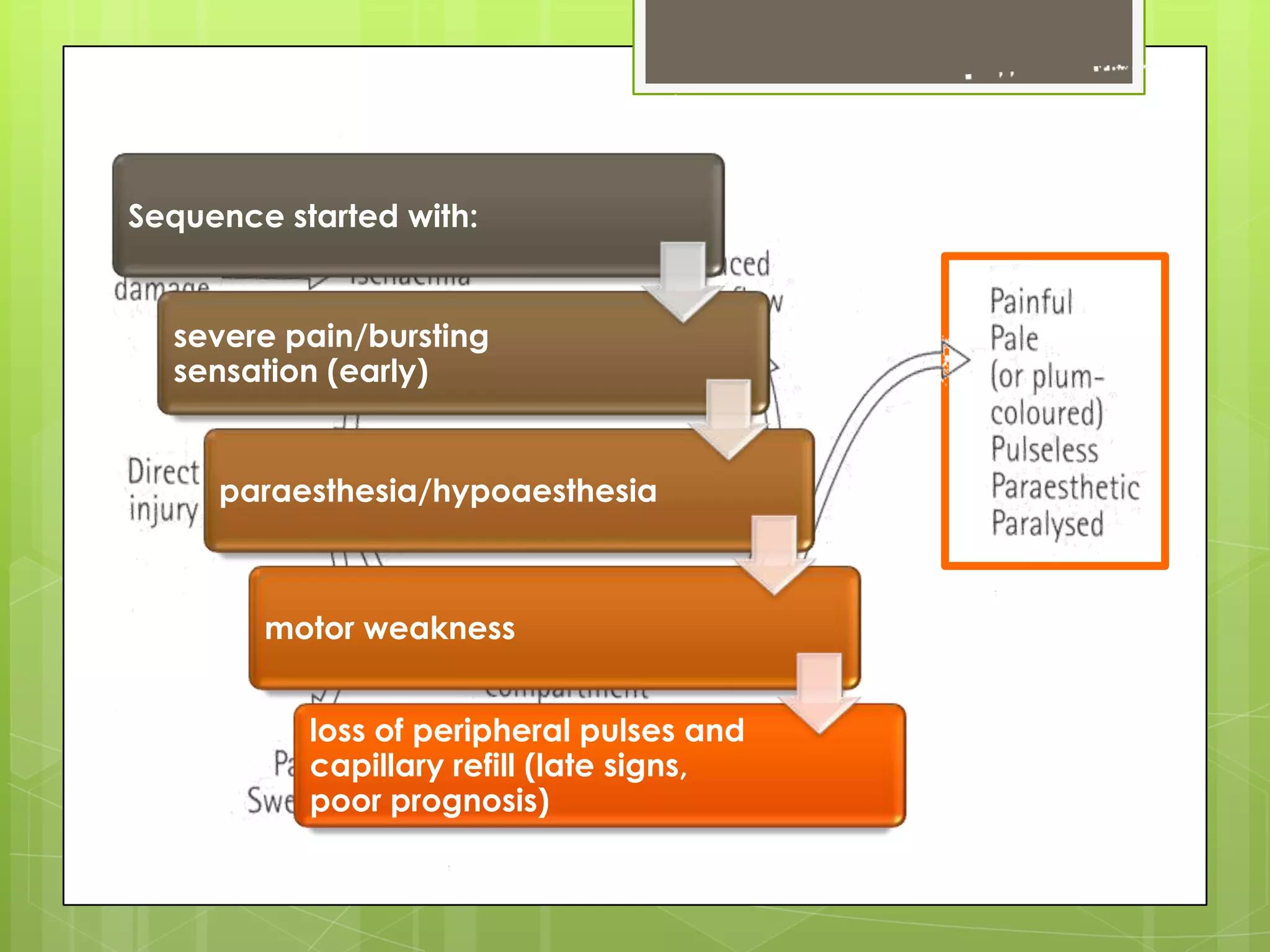
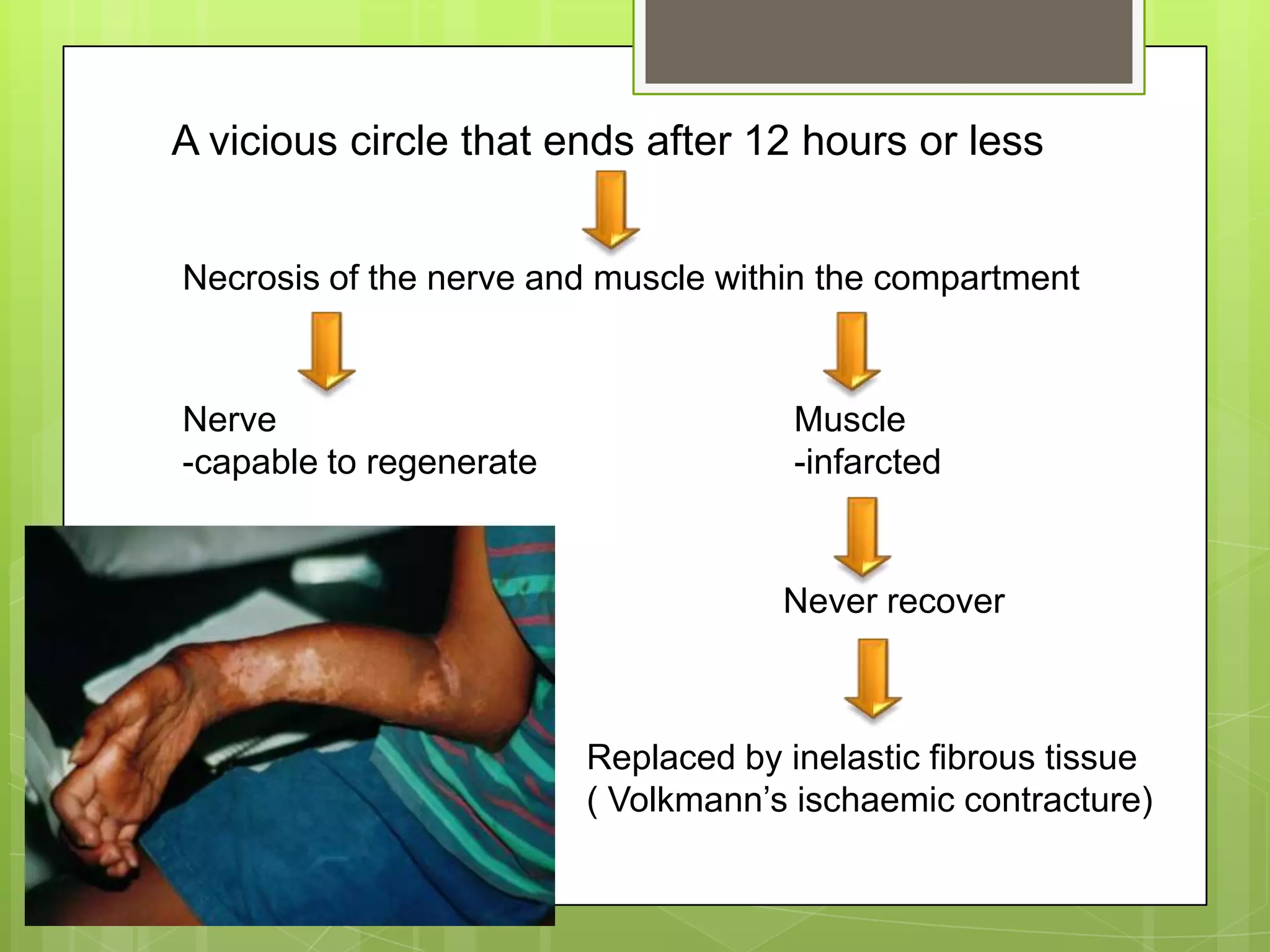
![Early 3: Compartment Syndrome [aetiology]](https://image.slidesharecdn.com/complicationoffracture-110112042527-phpapp01/75/Complication-of-fracture-124-2048.jpg)

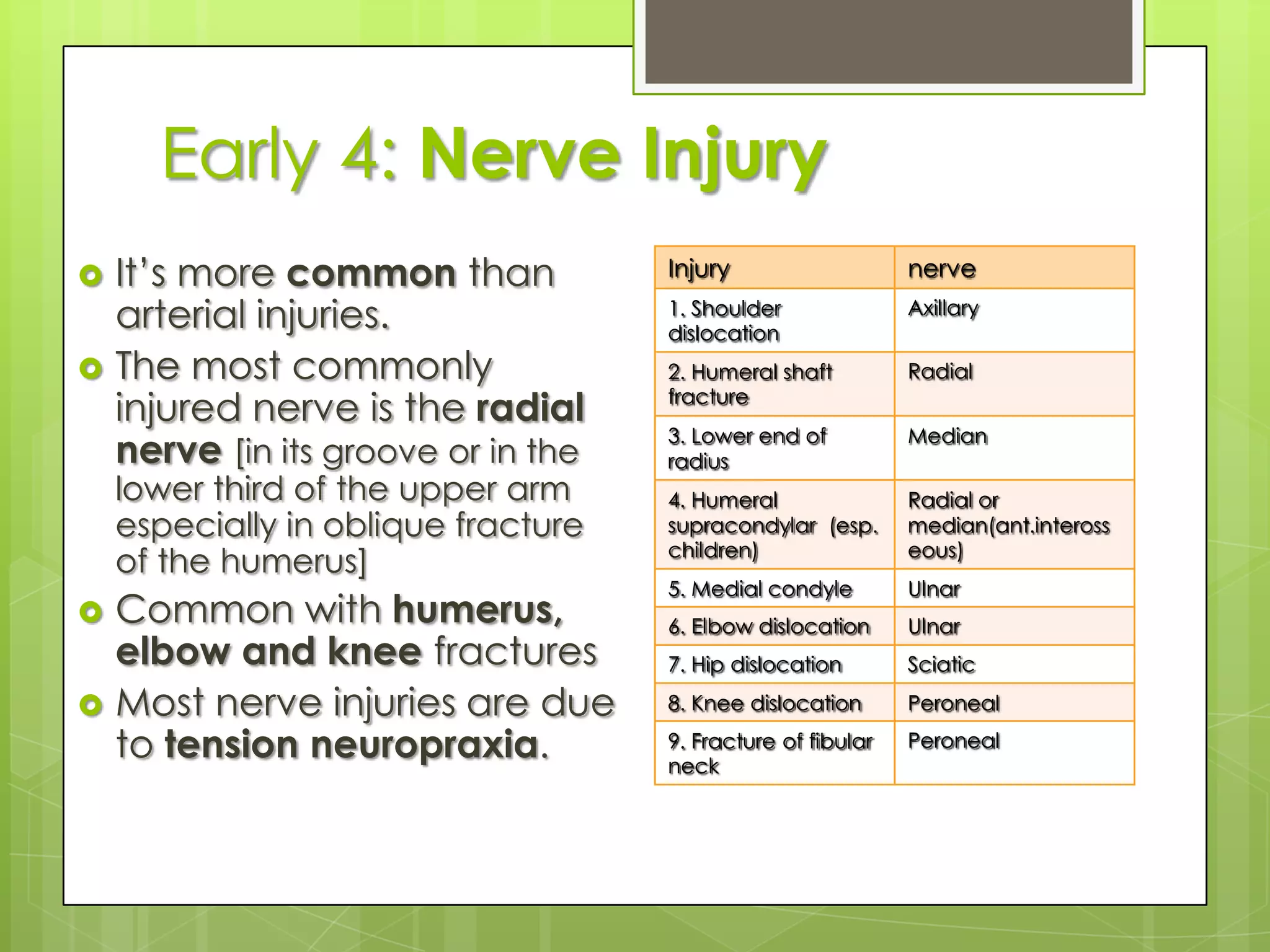
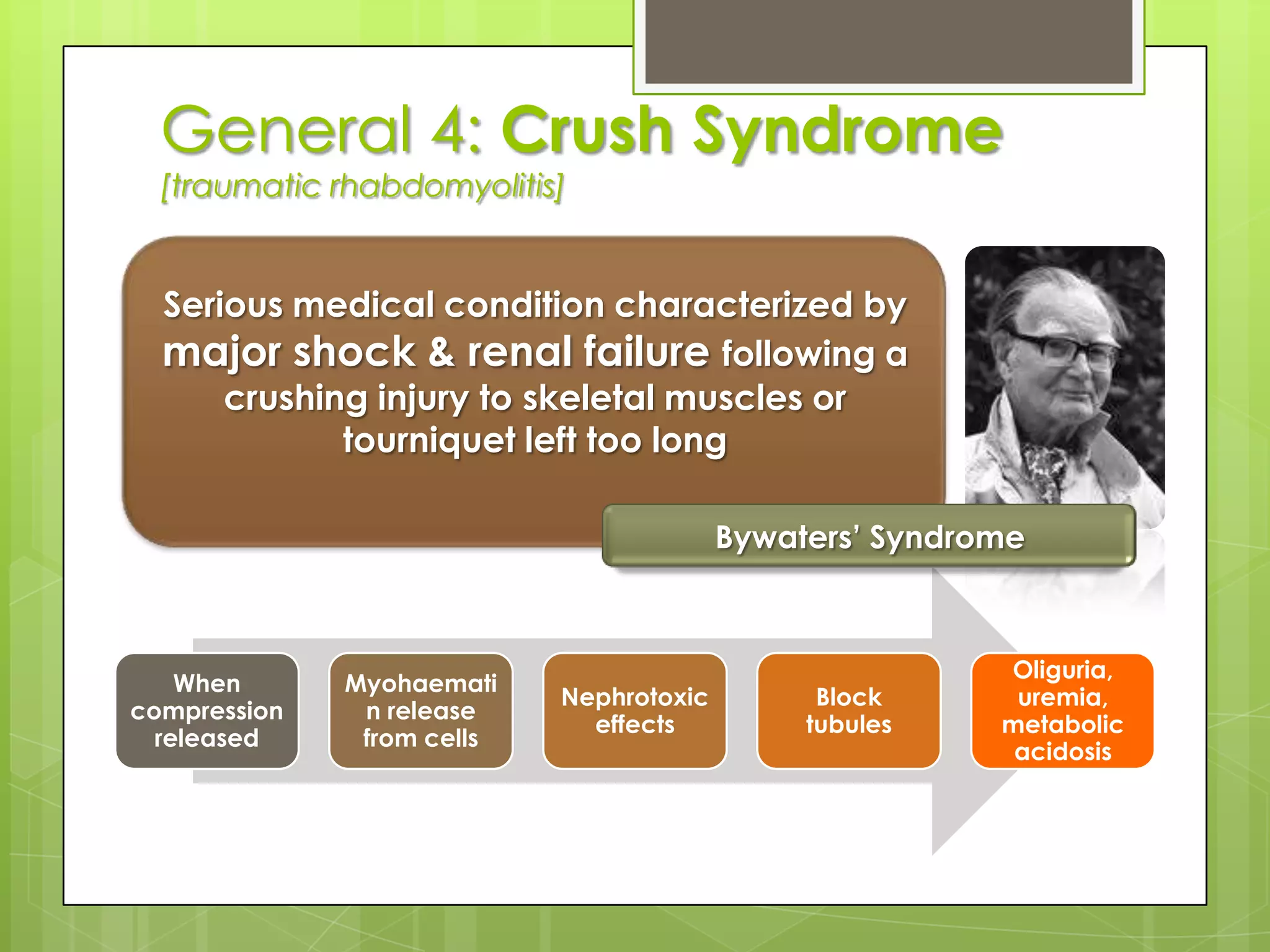
![Early 4: Nerve InjuryIt’s more common than arterial injuries.The most commonly injured nerve is the radial nerve [in its groove or in the lower third of the upper arm especially in oblique fracture of the humerus]Common with humerus, elbow and knee fracturesMost nerve injuries are due to tension neuropraxia.](https://image.slidesharecdn.com/complicationoffracture-110112042527-phpapp01/75/Complication-of-fracture-135-2048.jpg)




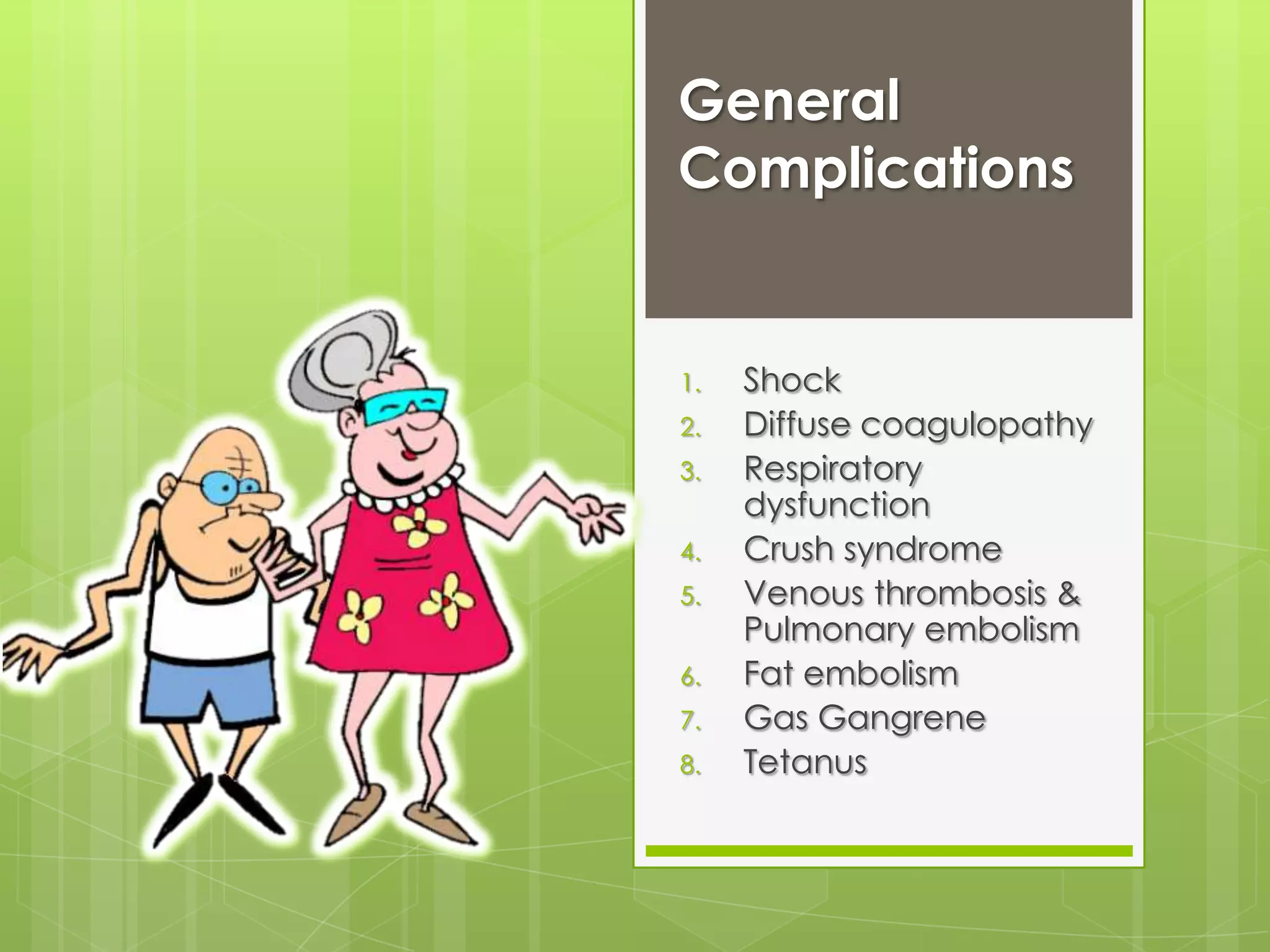
The document discusses fractures, including their definition, causes, types, healing processes, and complications. It provides details on the principle management of fractures, including reduction, immobilization, and internal or external fixation. Key complications discussed are shock, diffuse coagulopathy, respiratory dysfunction, crush syndrome, deep vein thrombosis, fat embolism, gas gangrene, and tetanus.
Overview of fractures, definitions, management principles, and complications involved.
Definitions, causes, including trauma types and conditions leading to fractures.
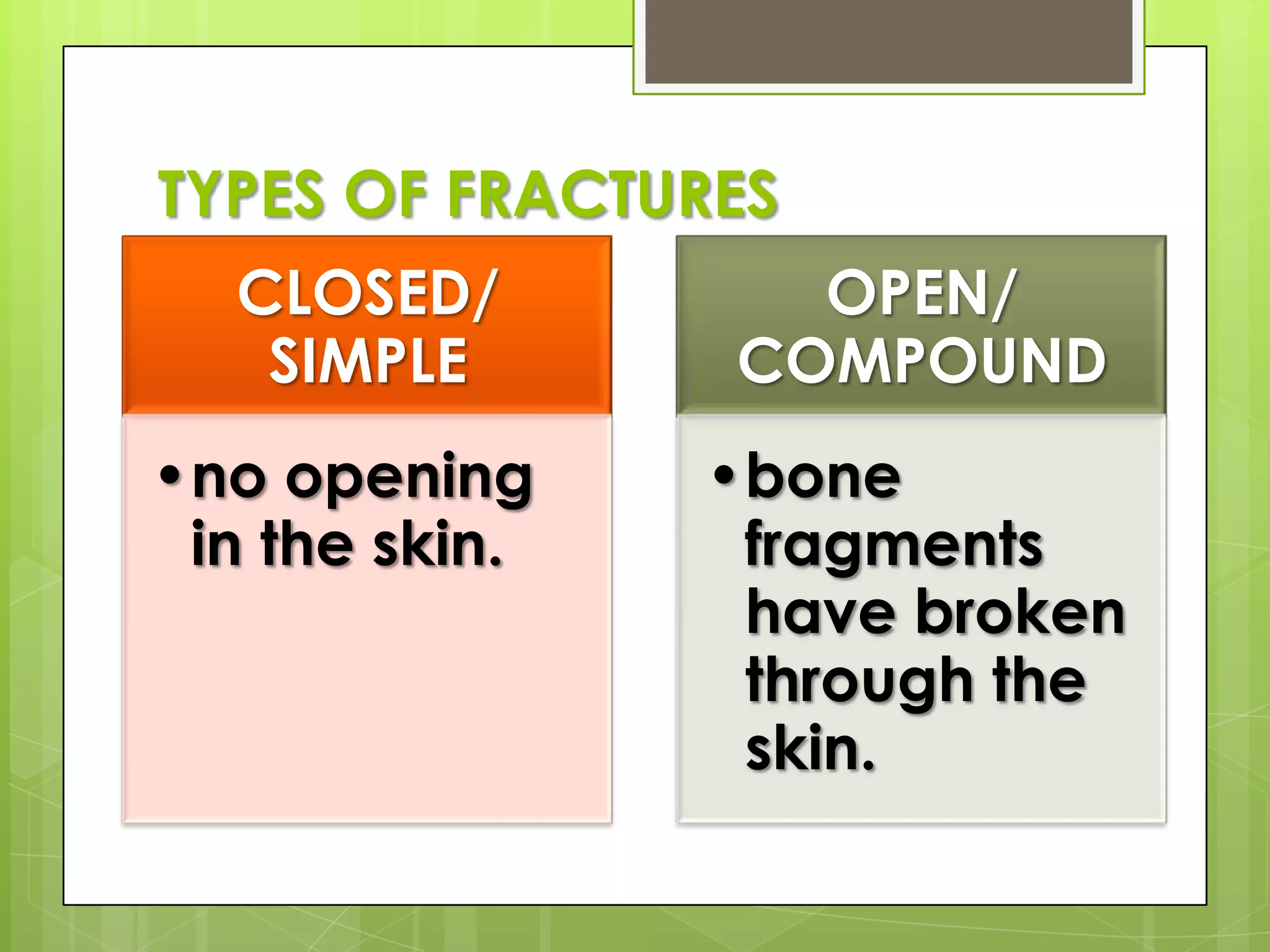
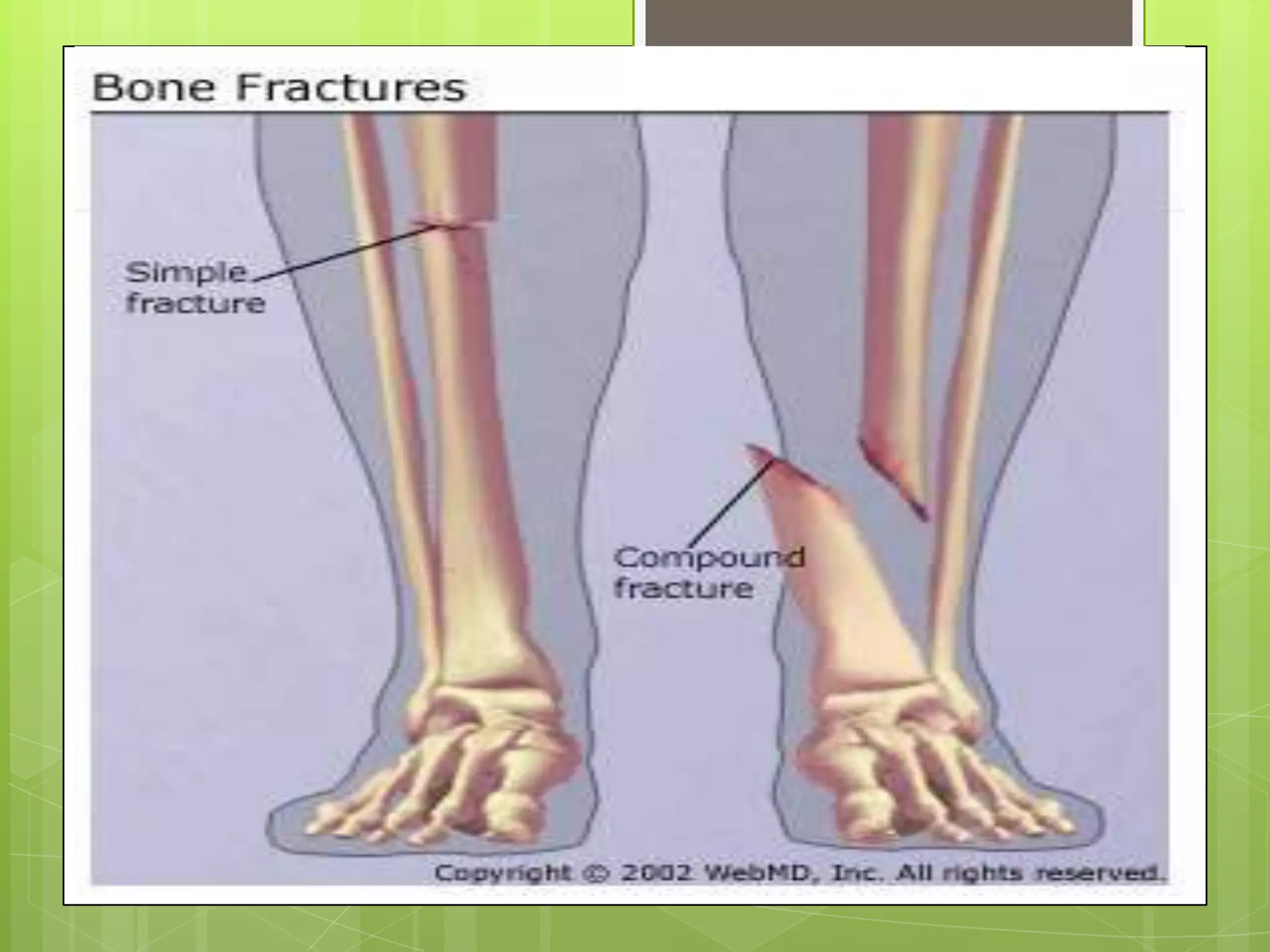
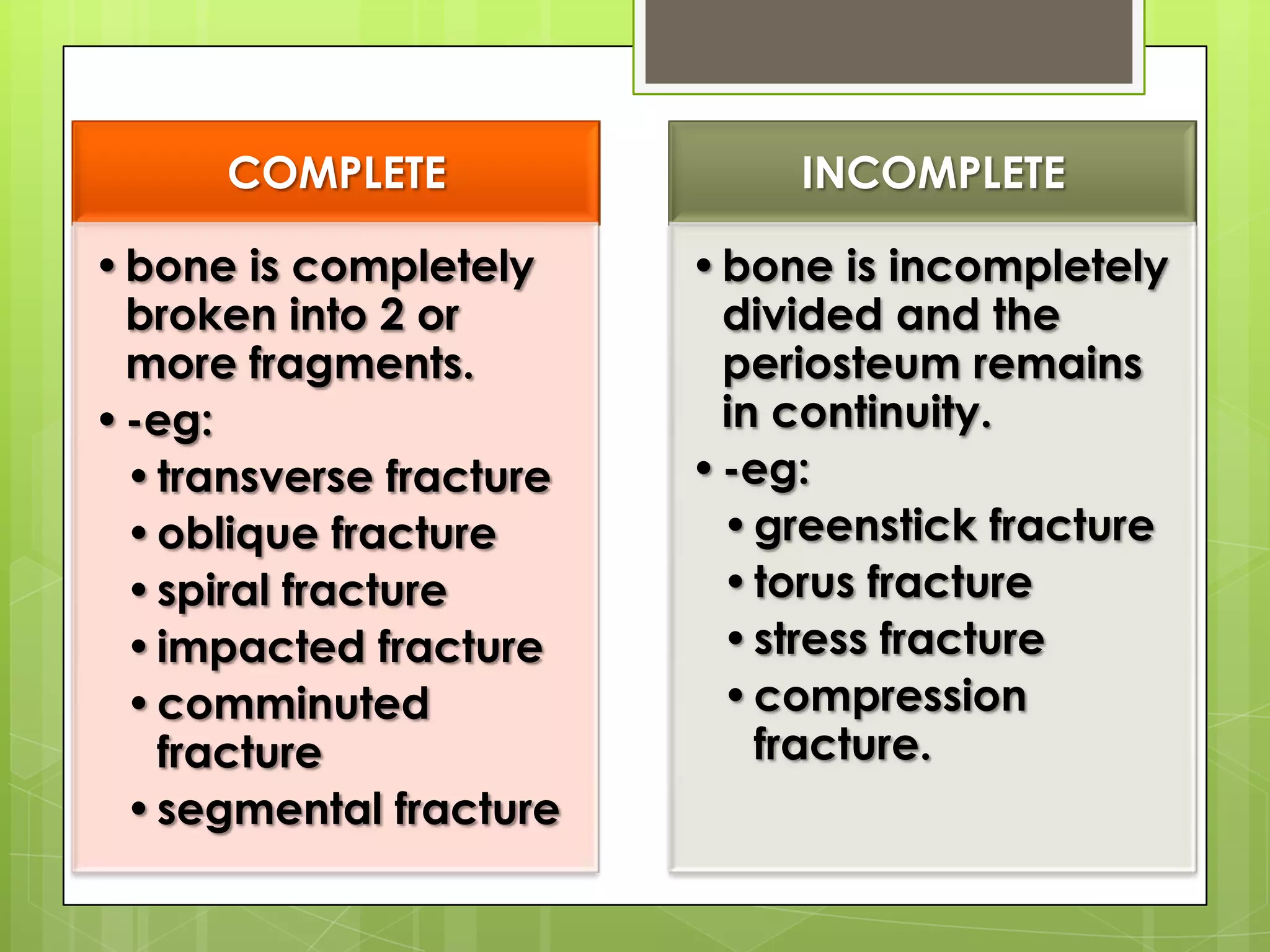
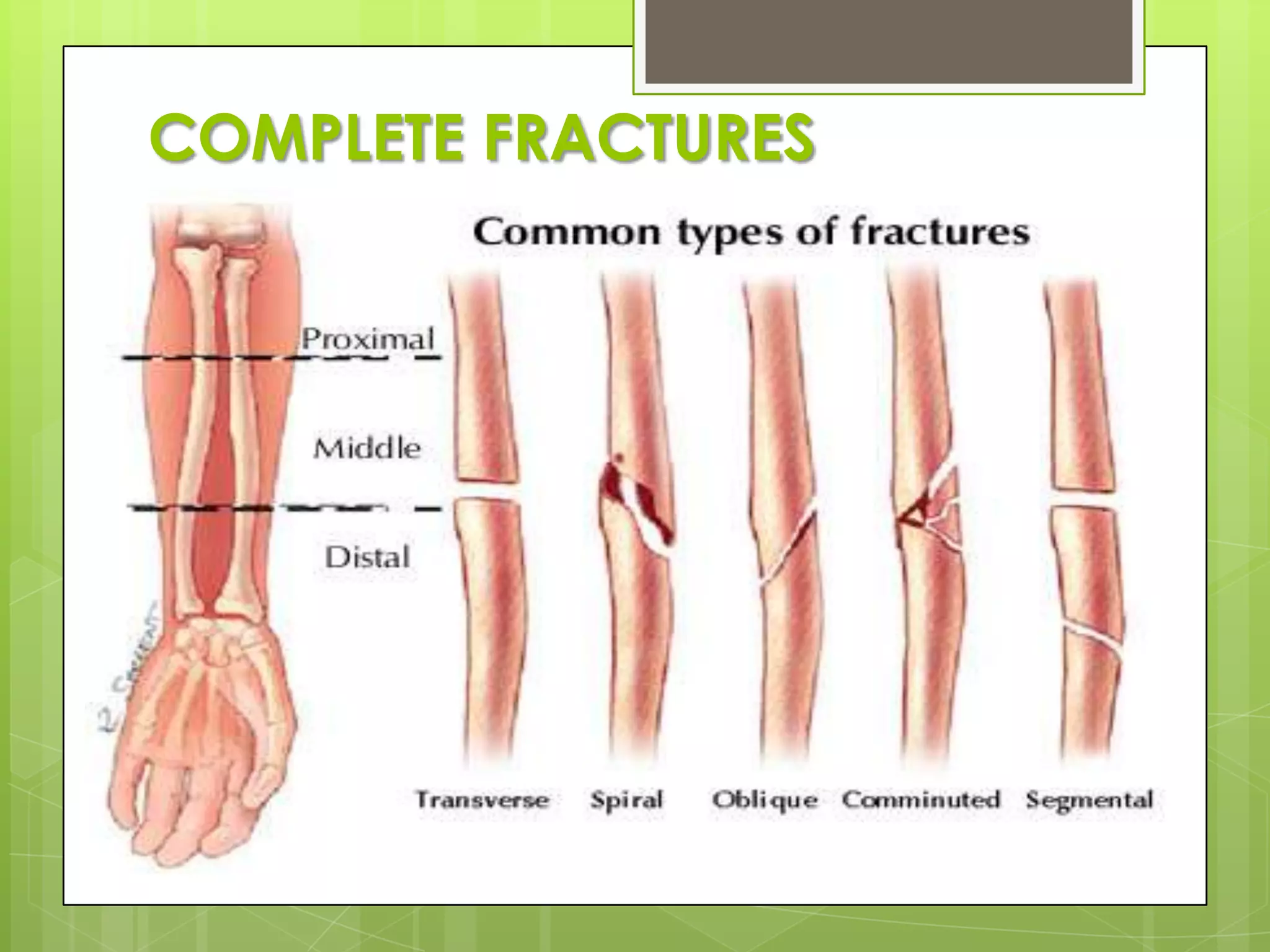
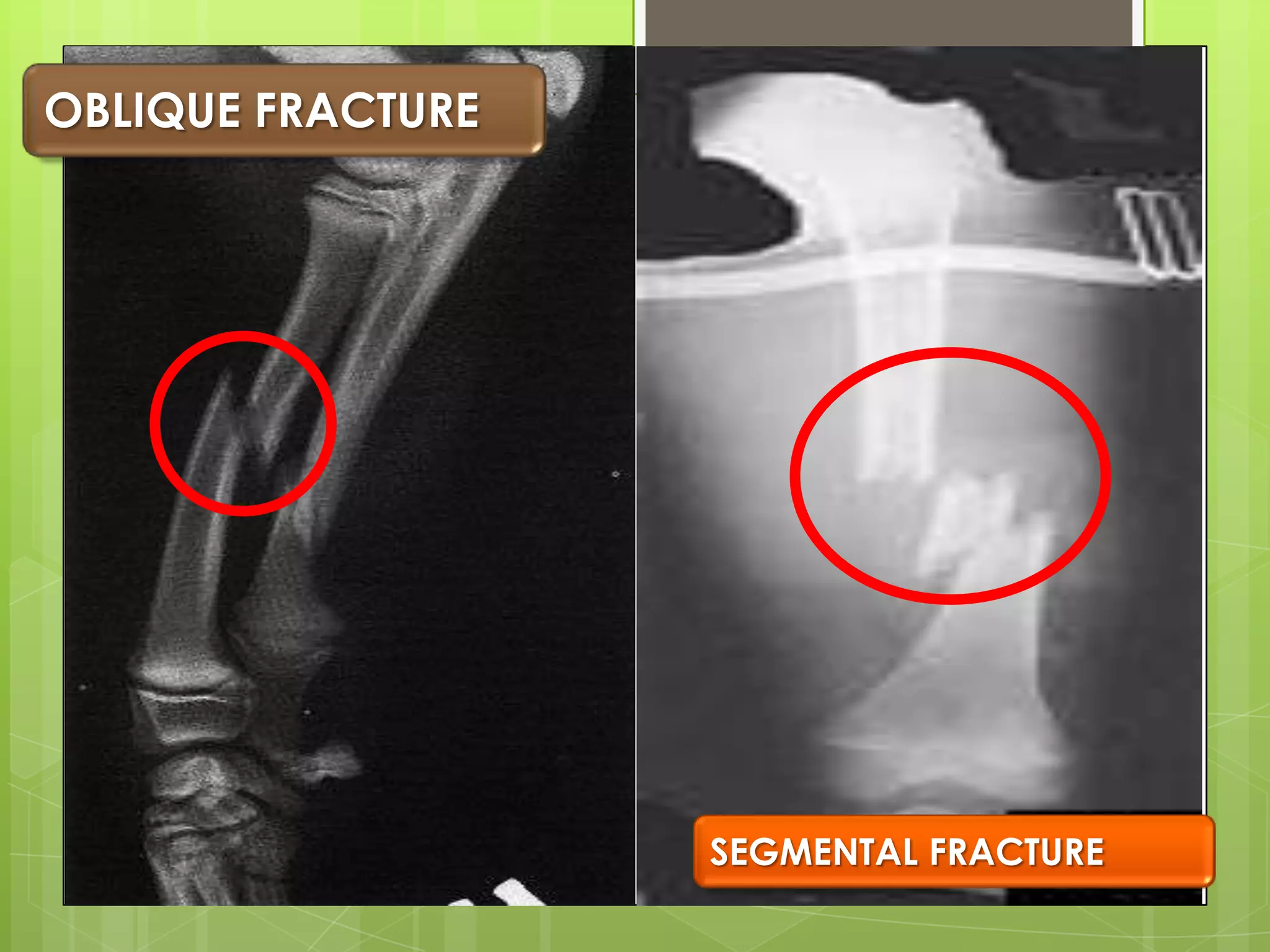
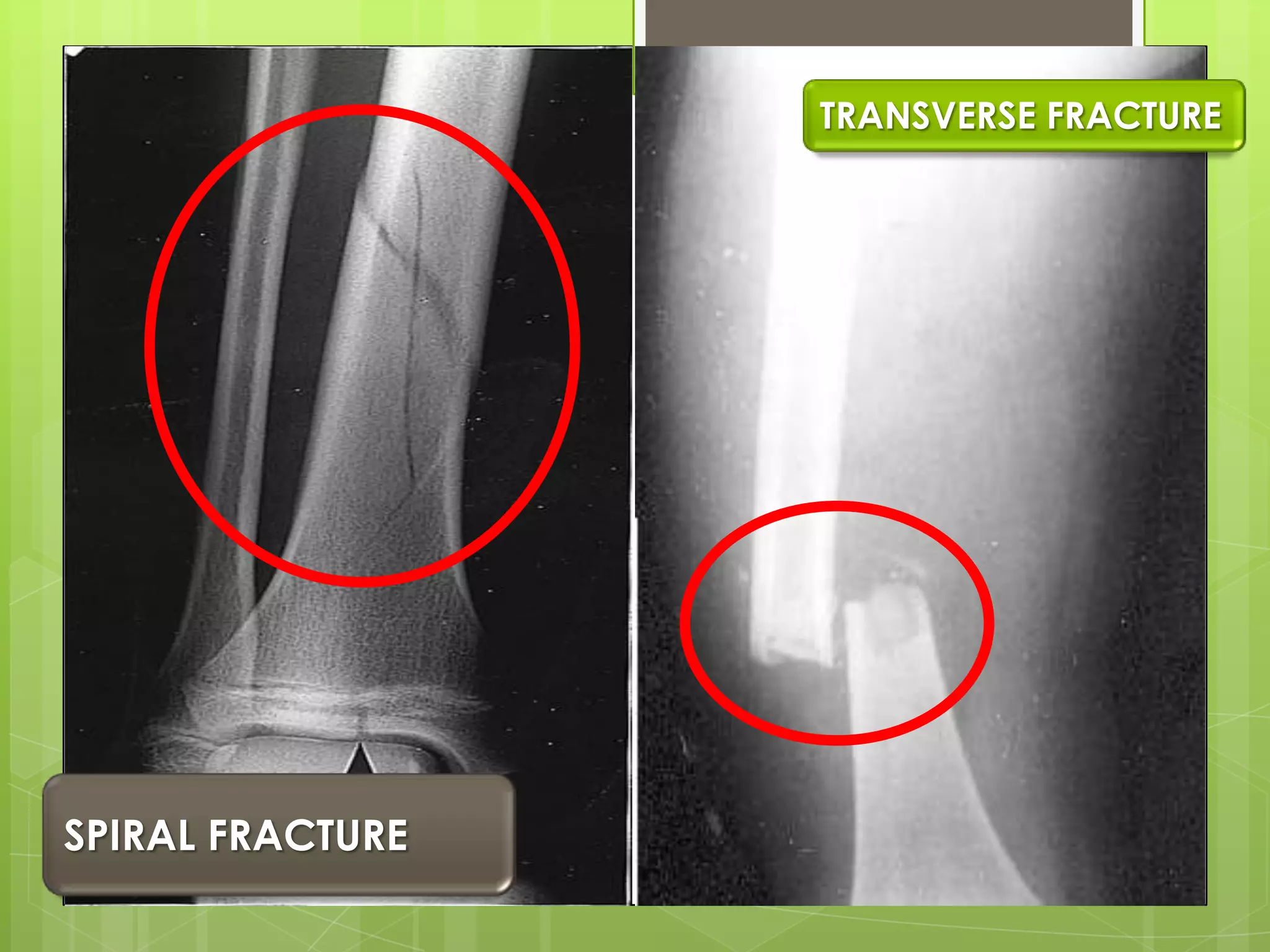
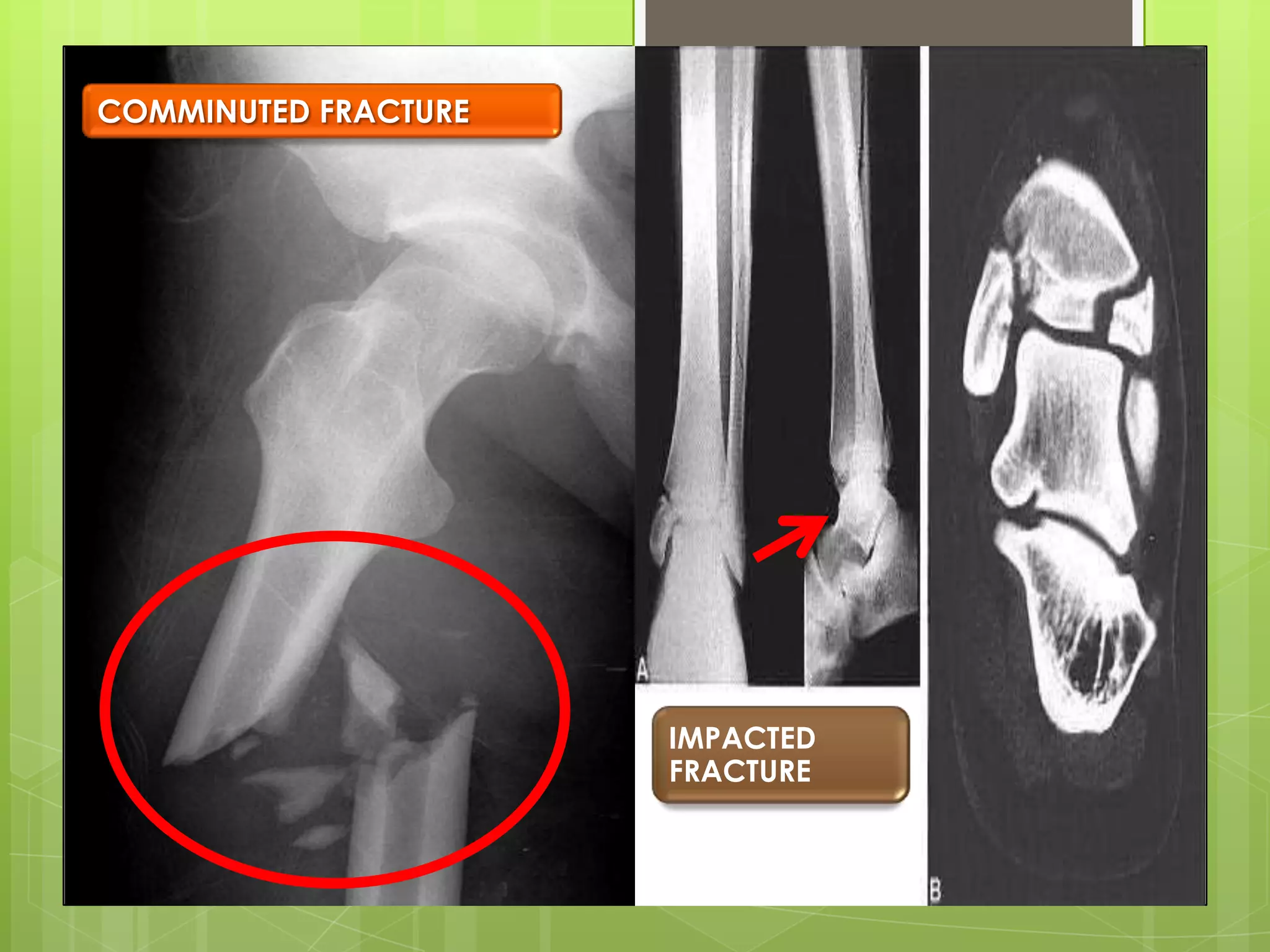
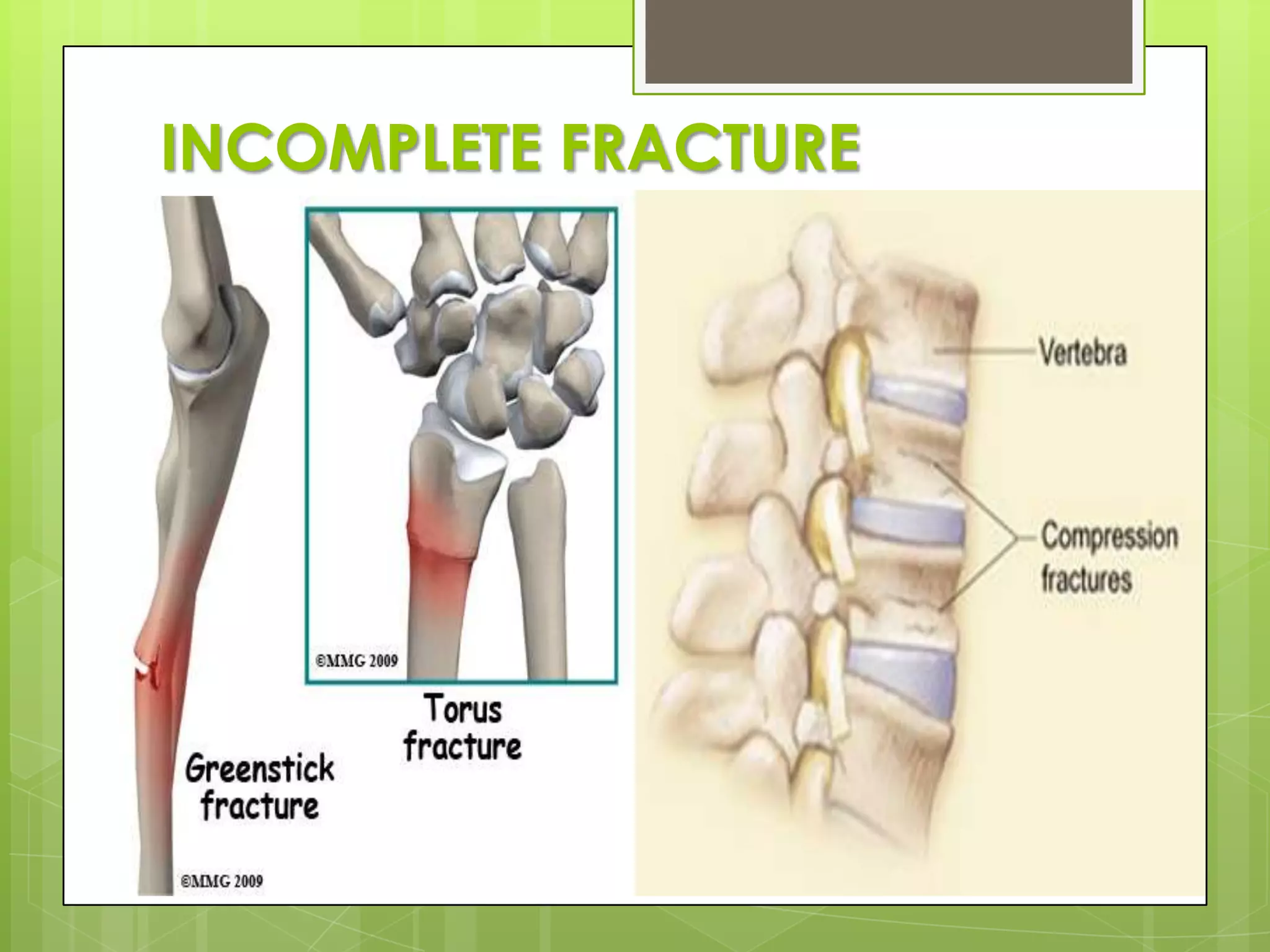
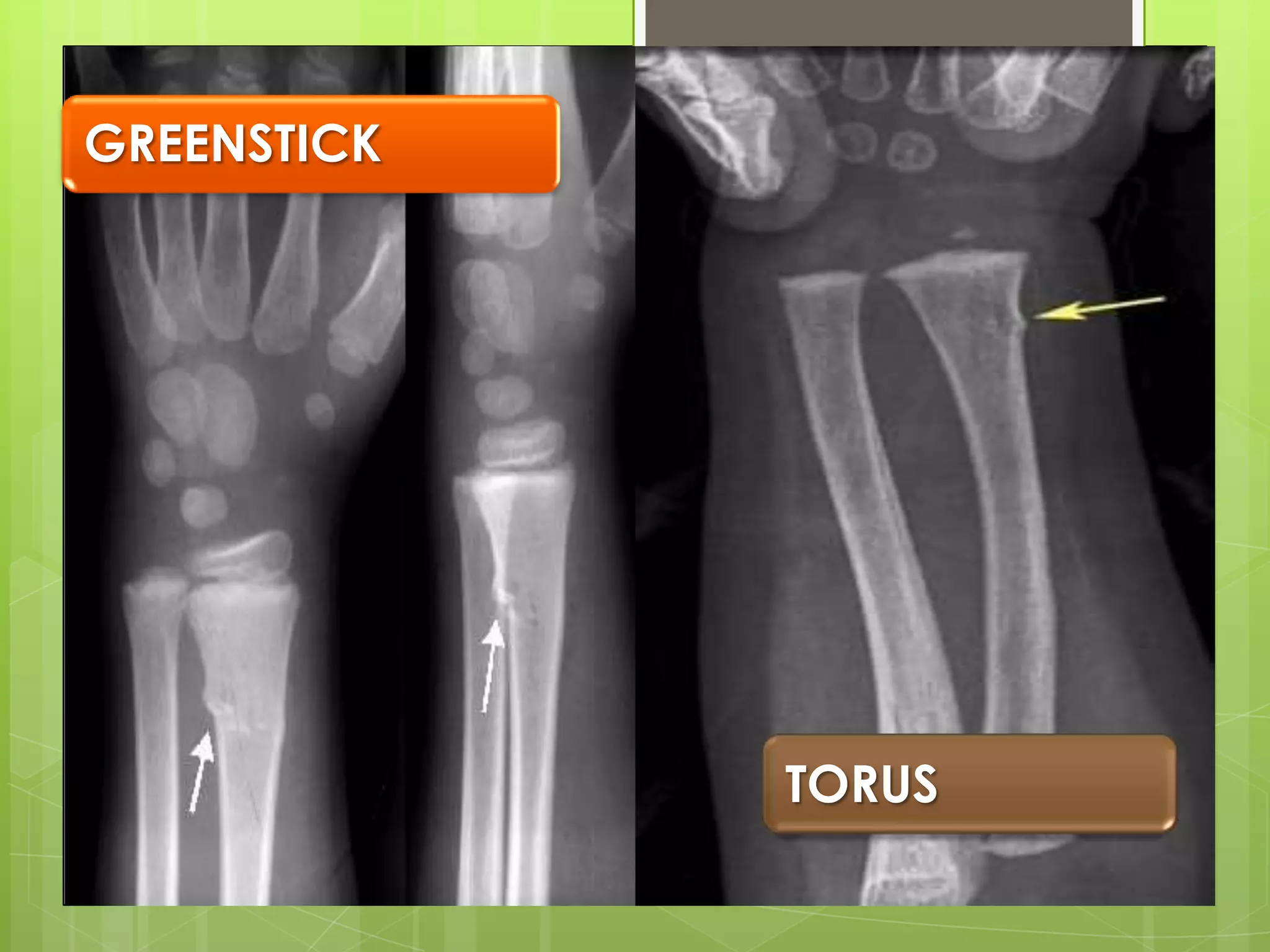
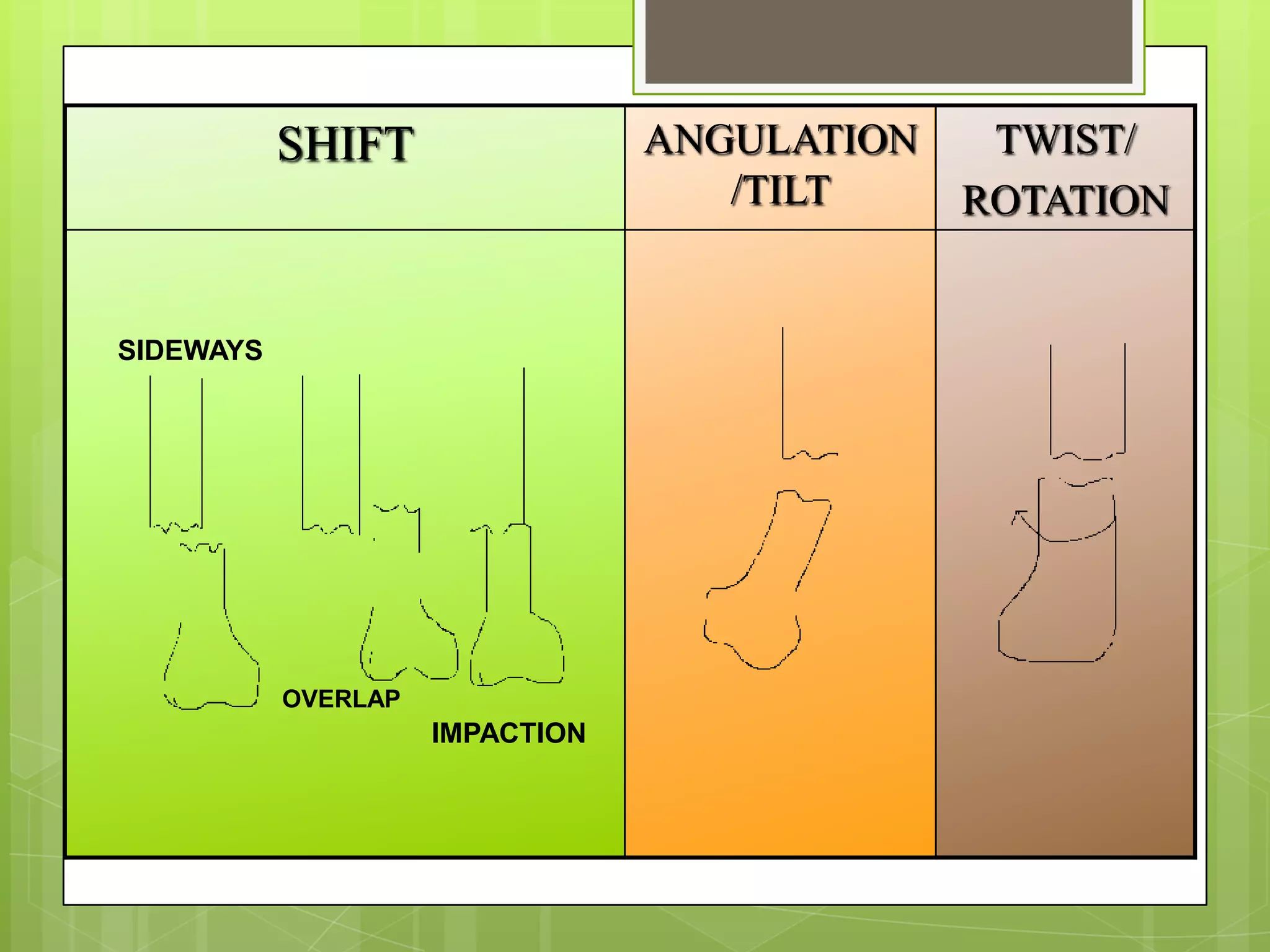
Different fracture types, complete versus incomplete, and displacement characteristics.
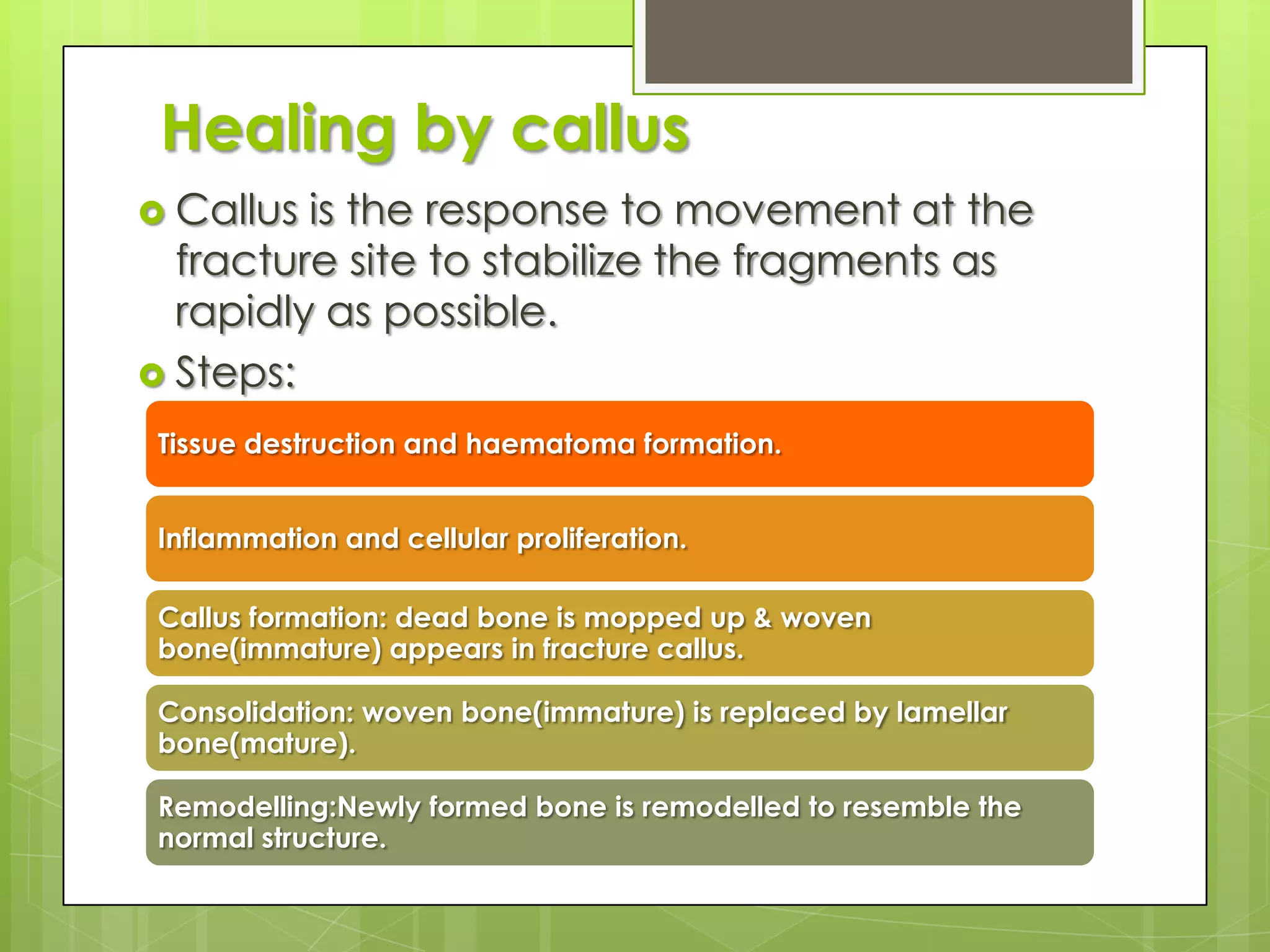
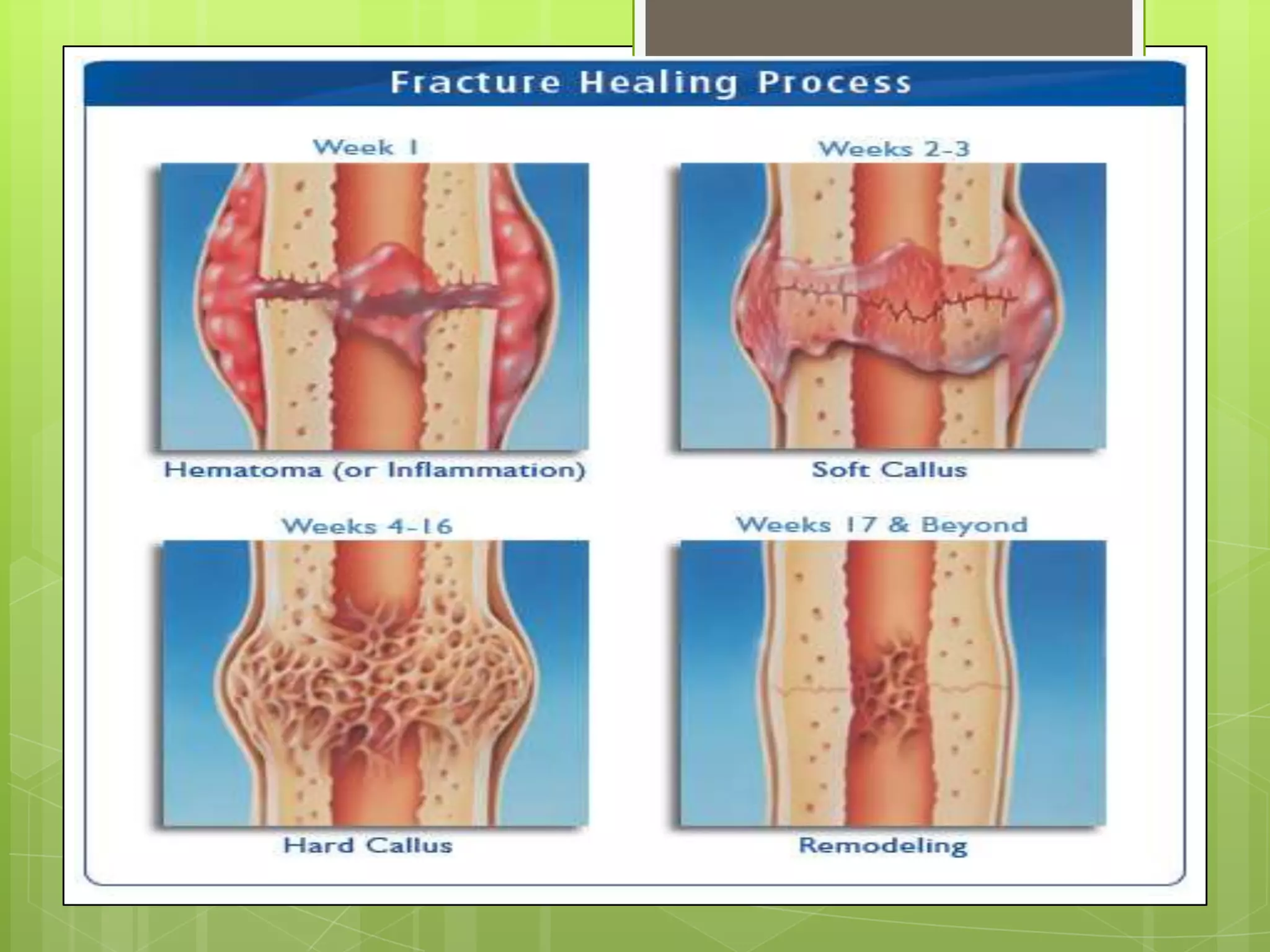
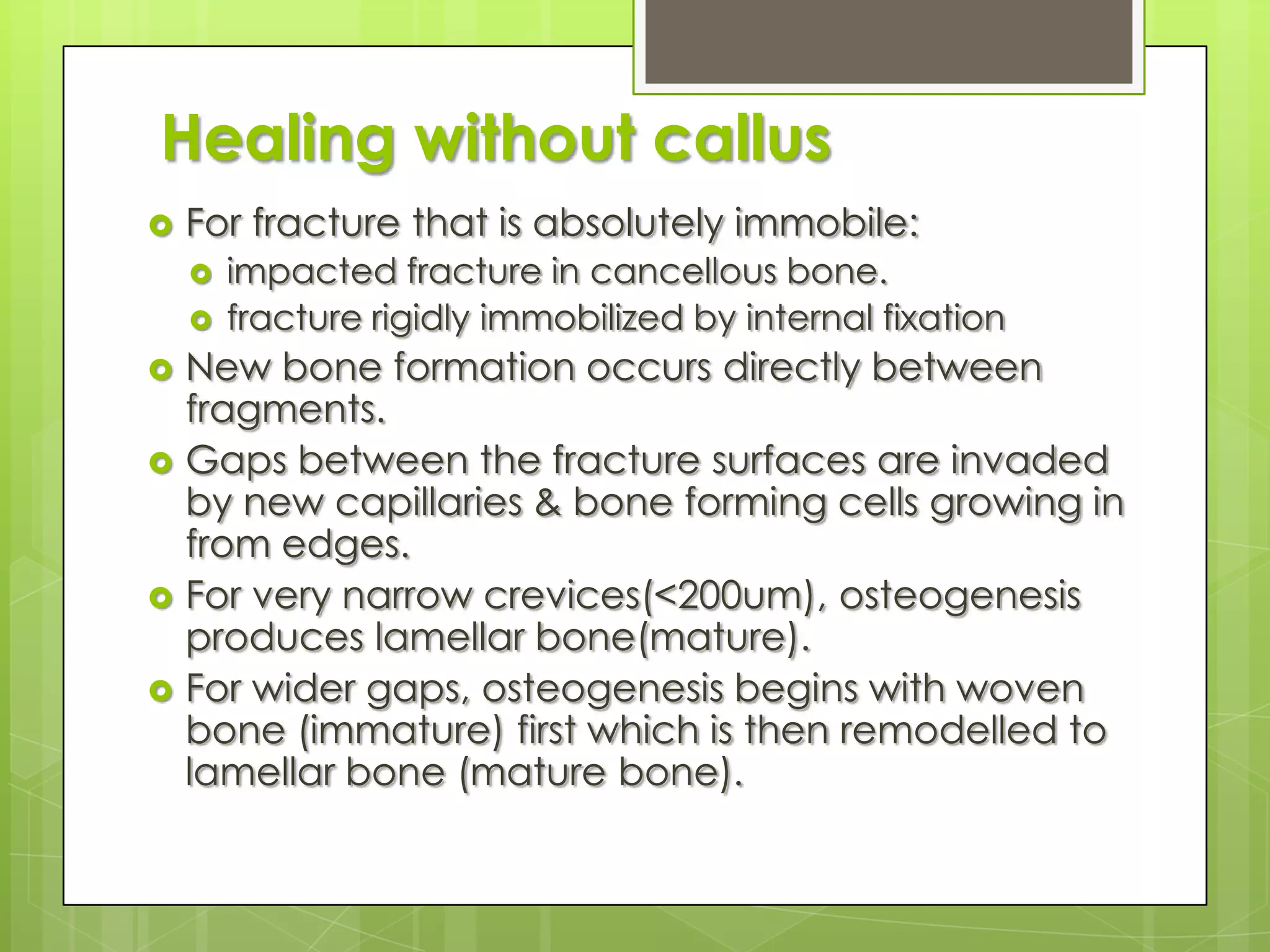
Processes of fracture healing, including callus formation and conditions for healing.
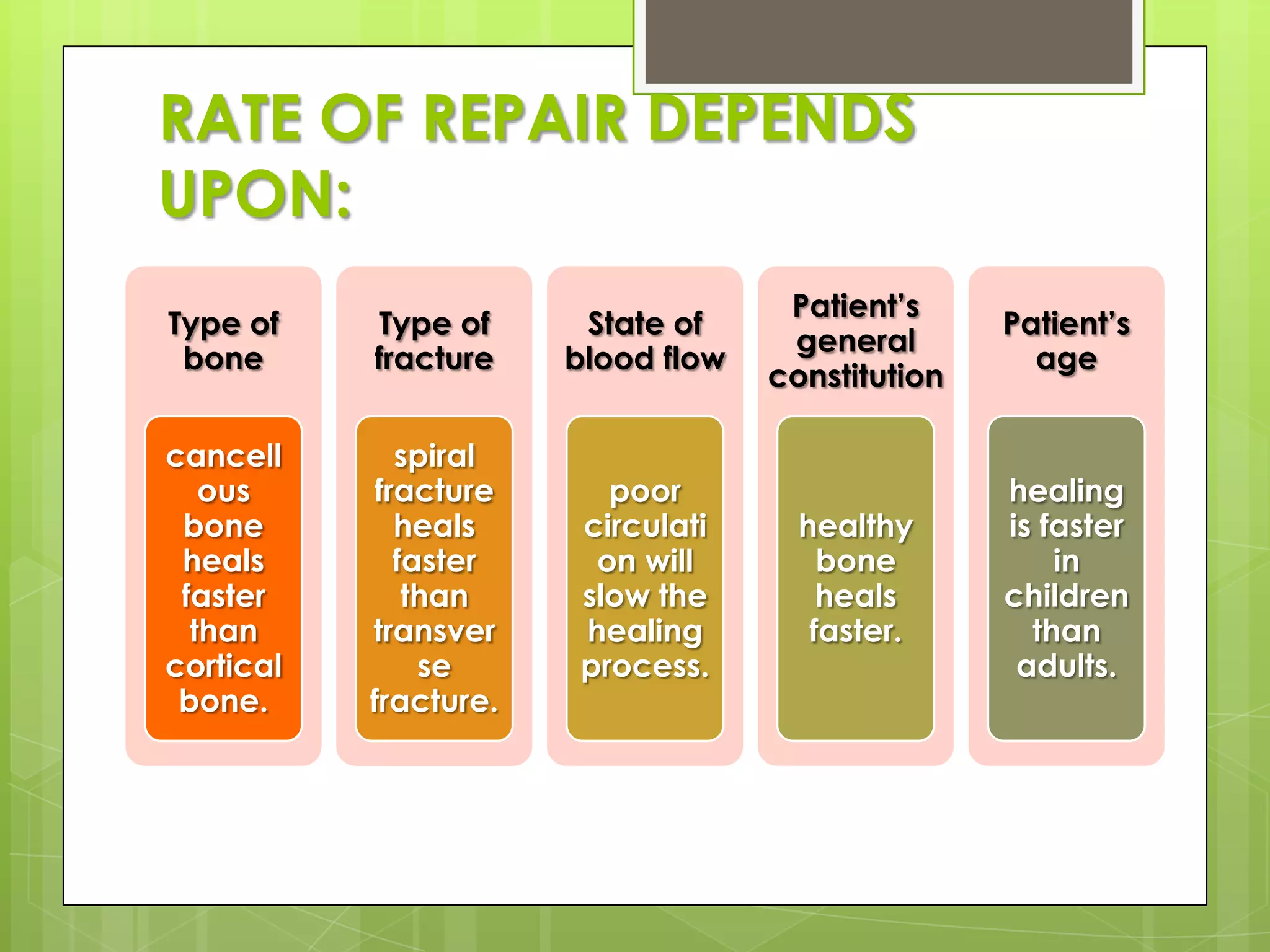
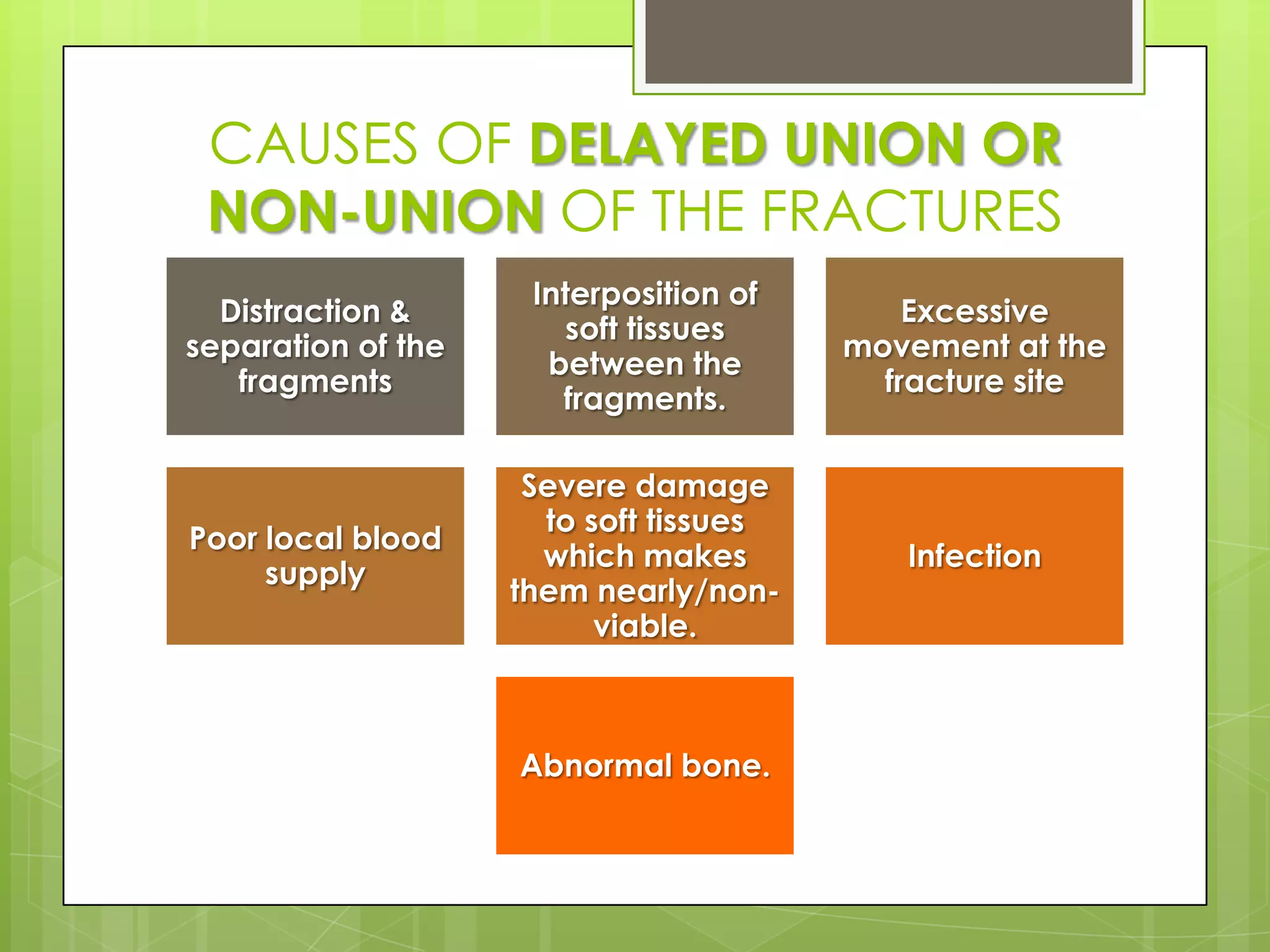
Factors influencing the rate of fracture repair and reasons for delayed union.
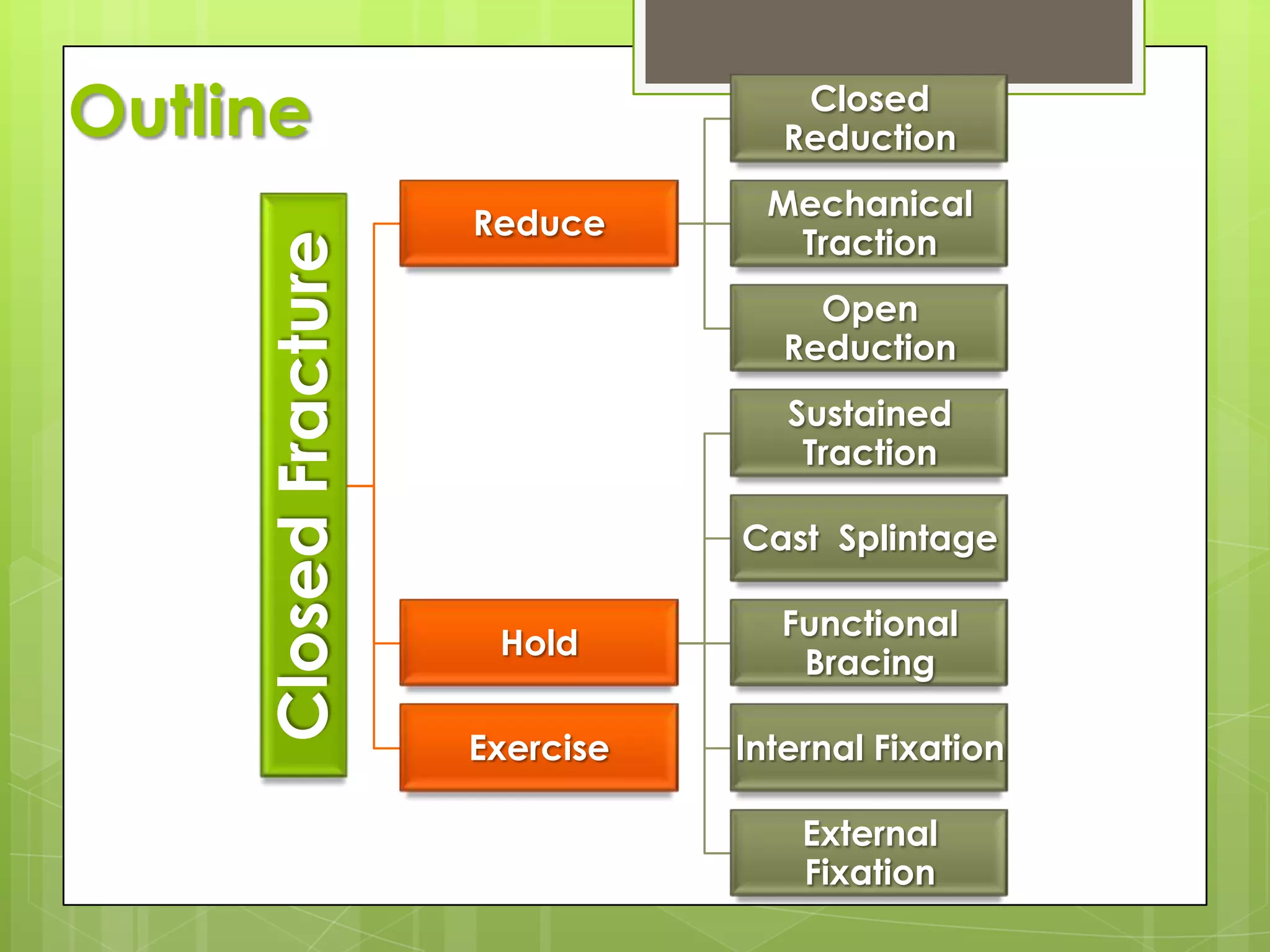
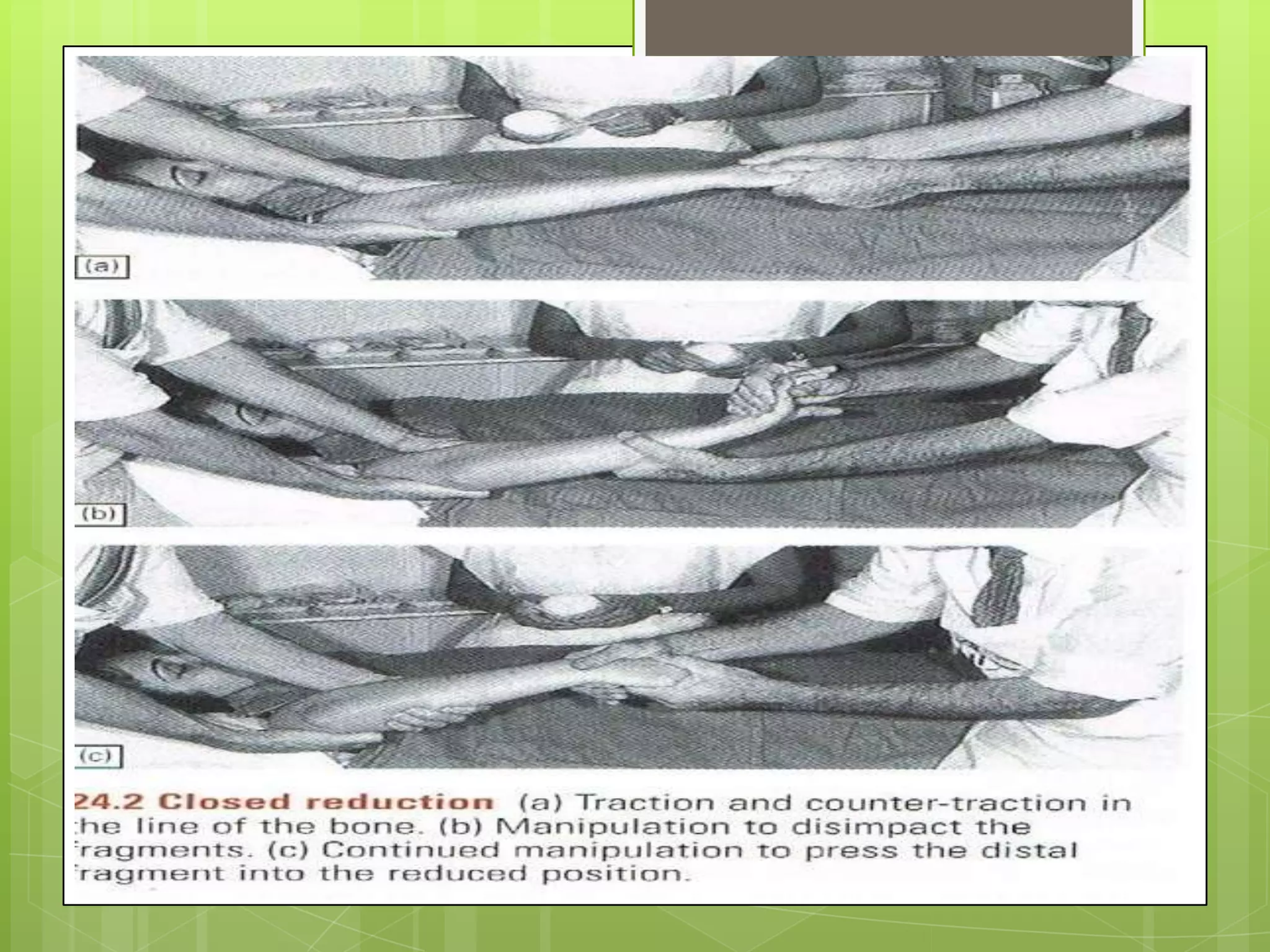
Principles and steps in treating fractures, with a focus on reduction techniques.
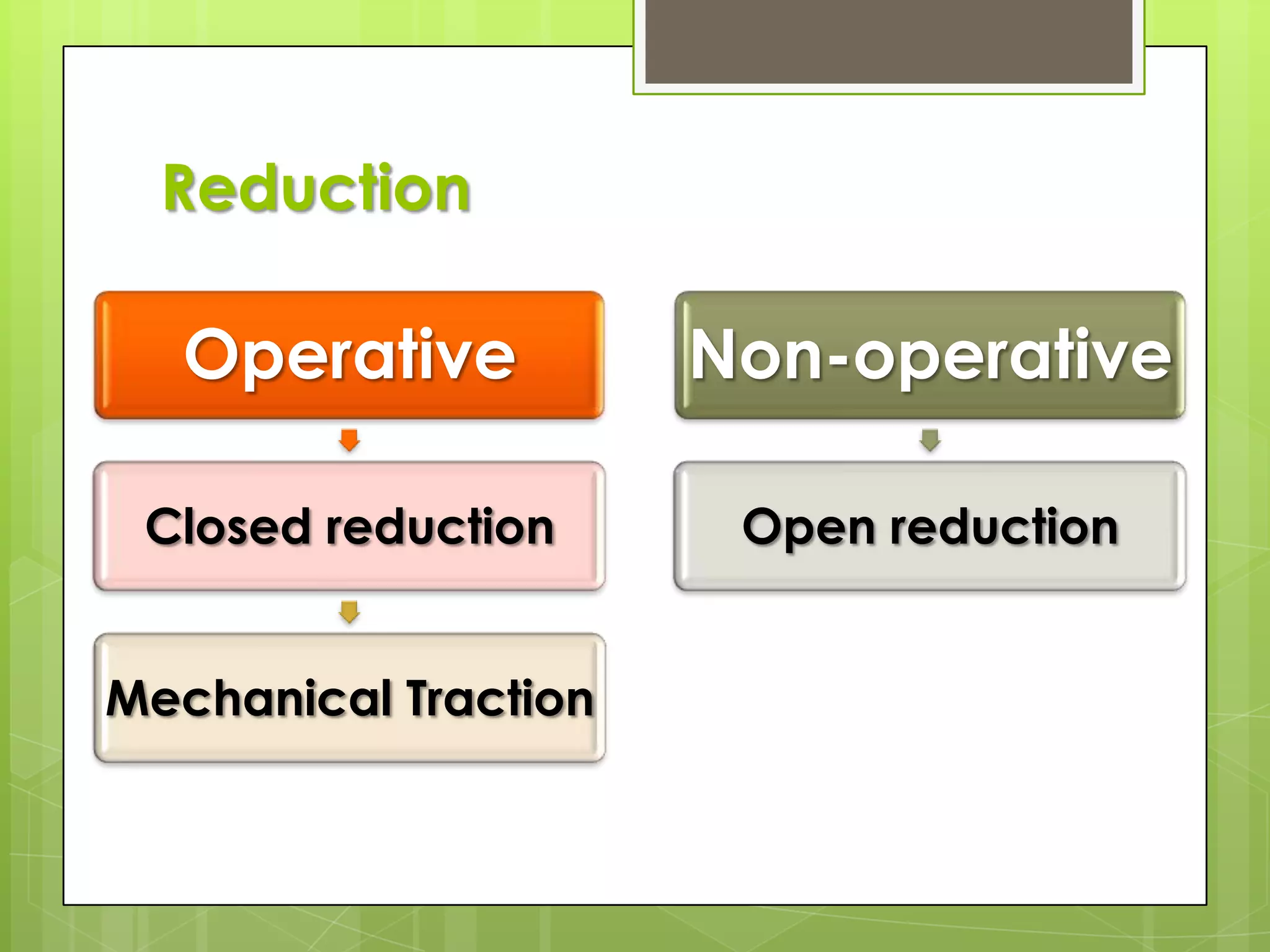
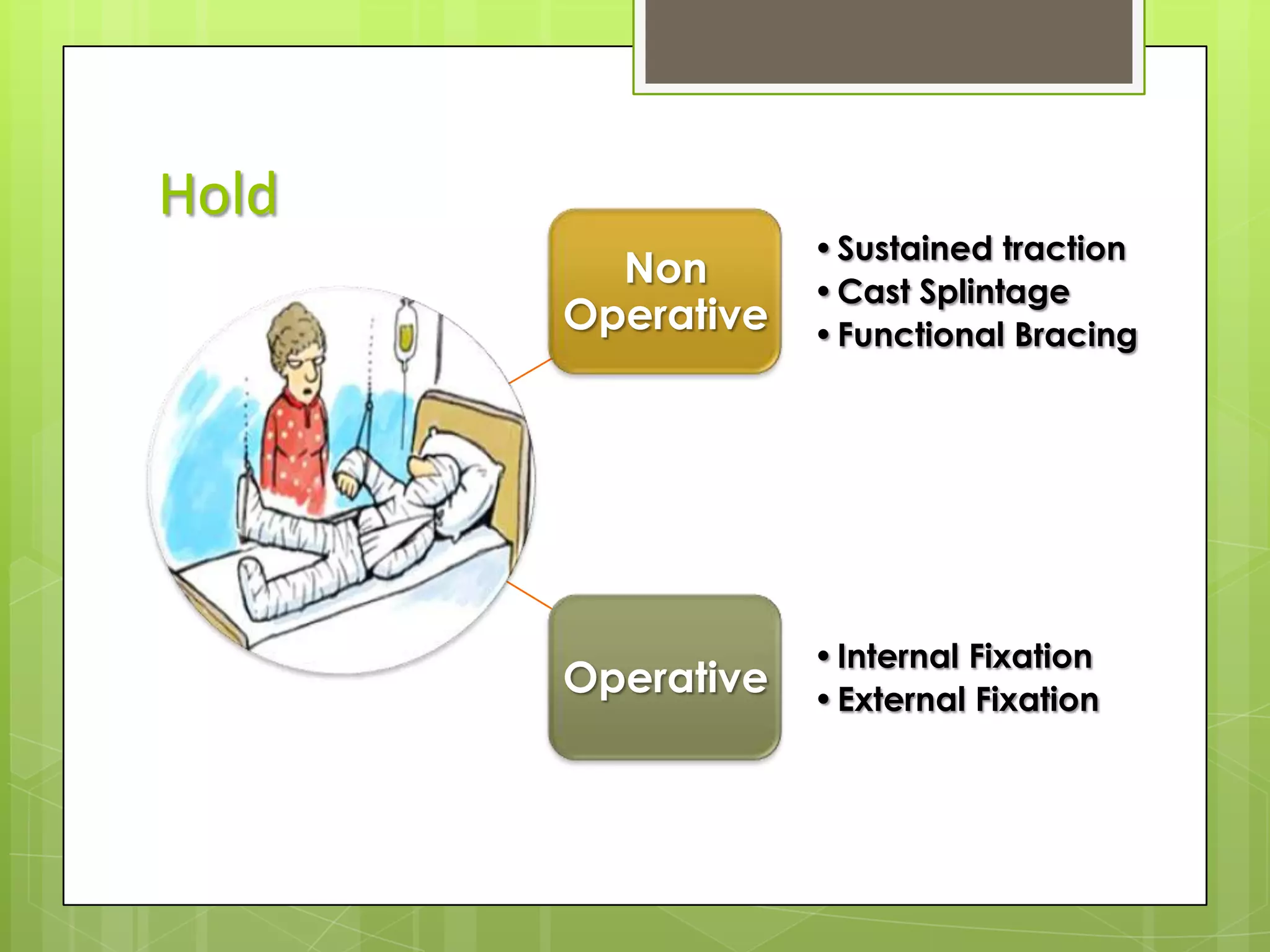
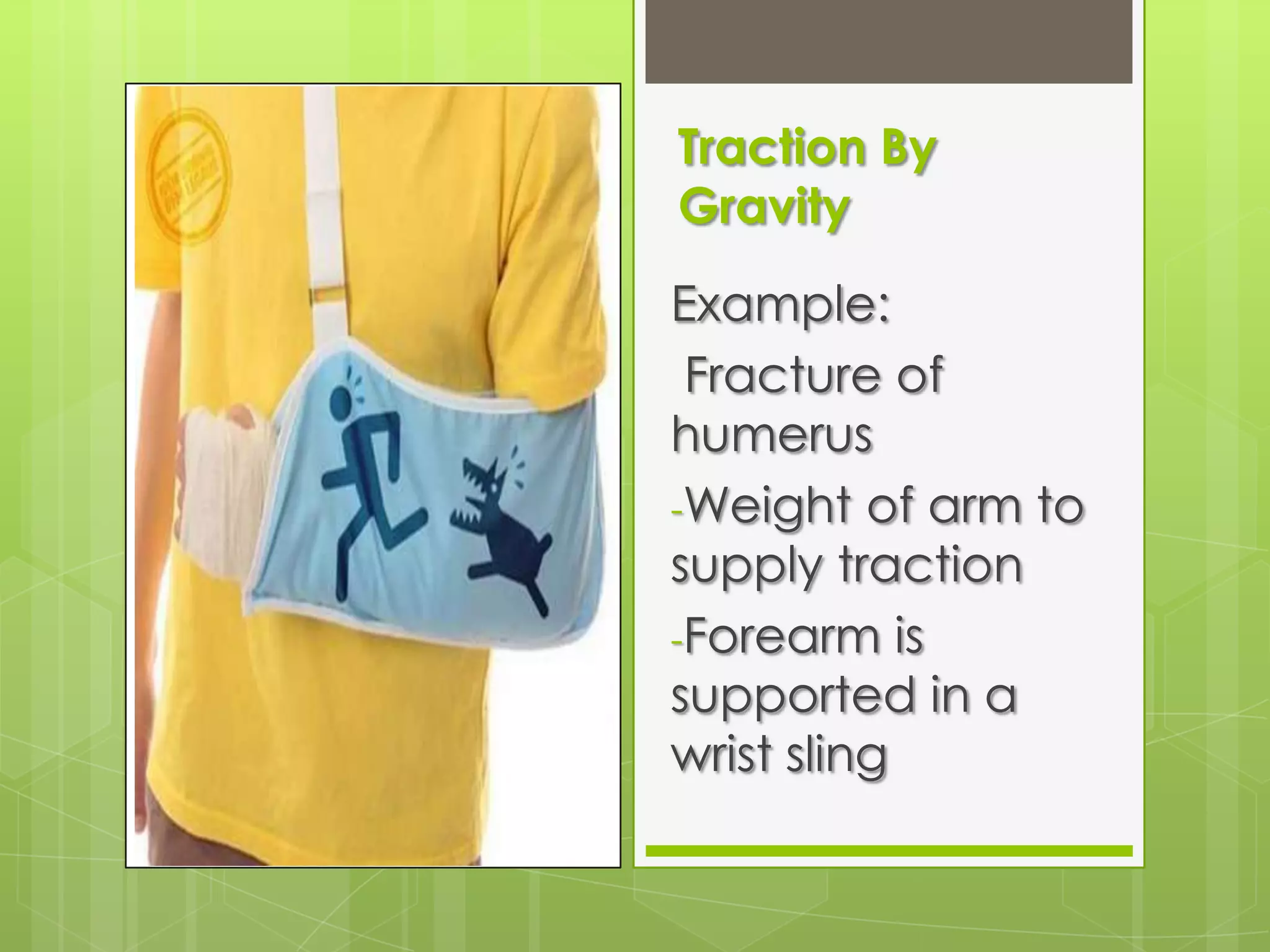
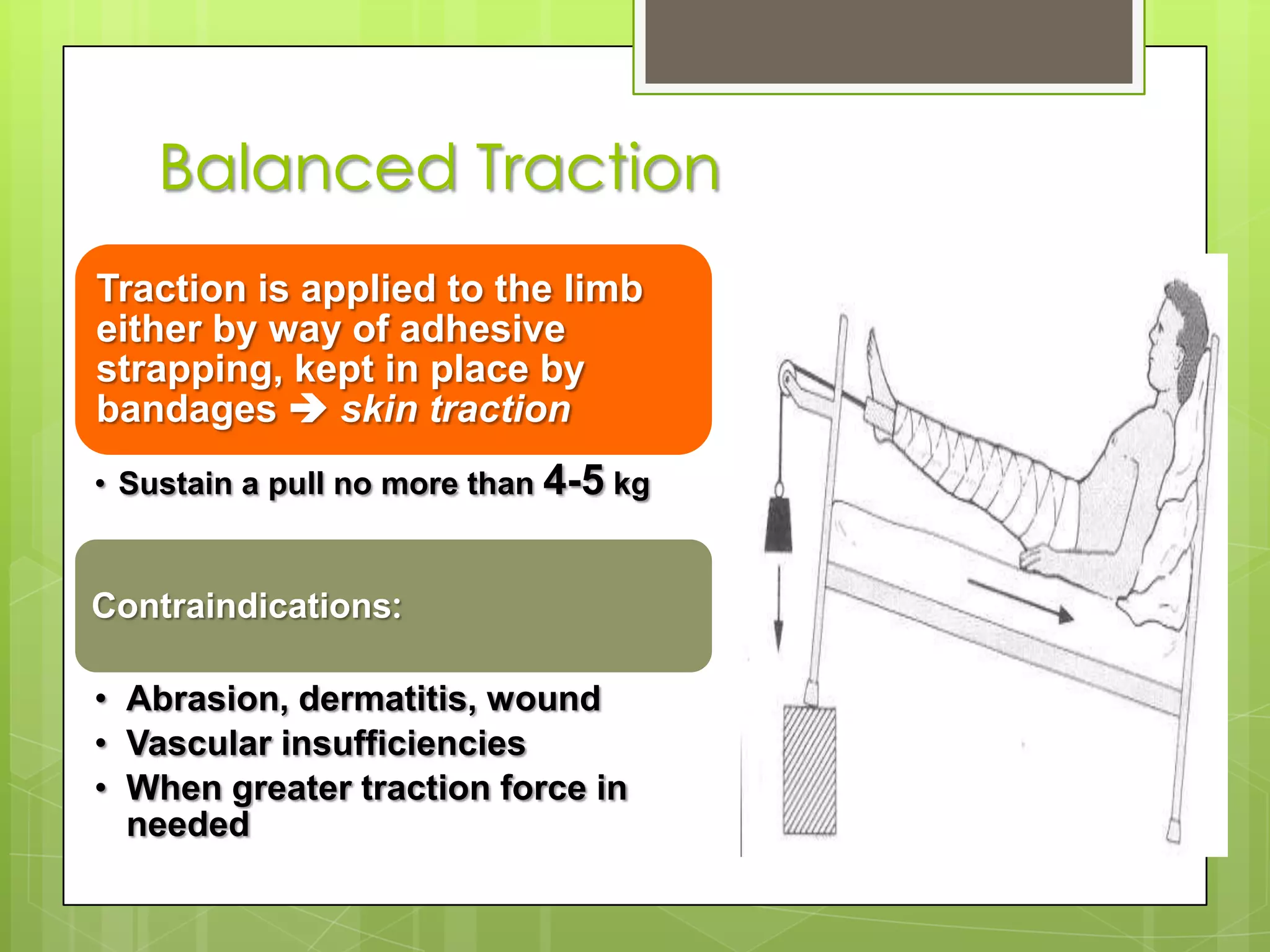
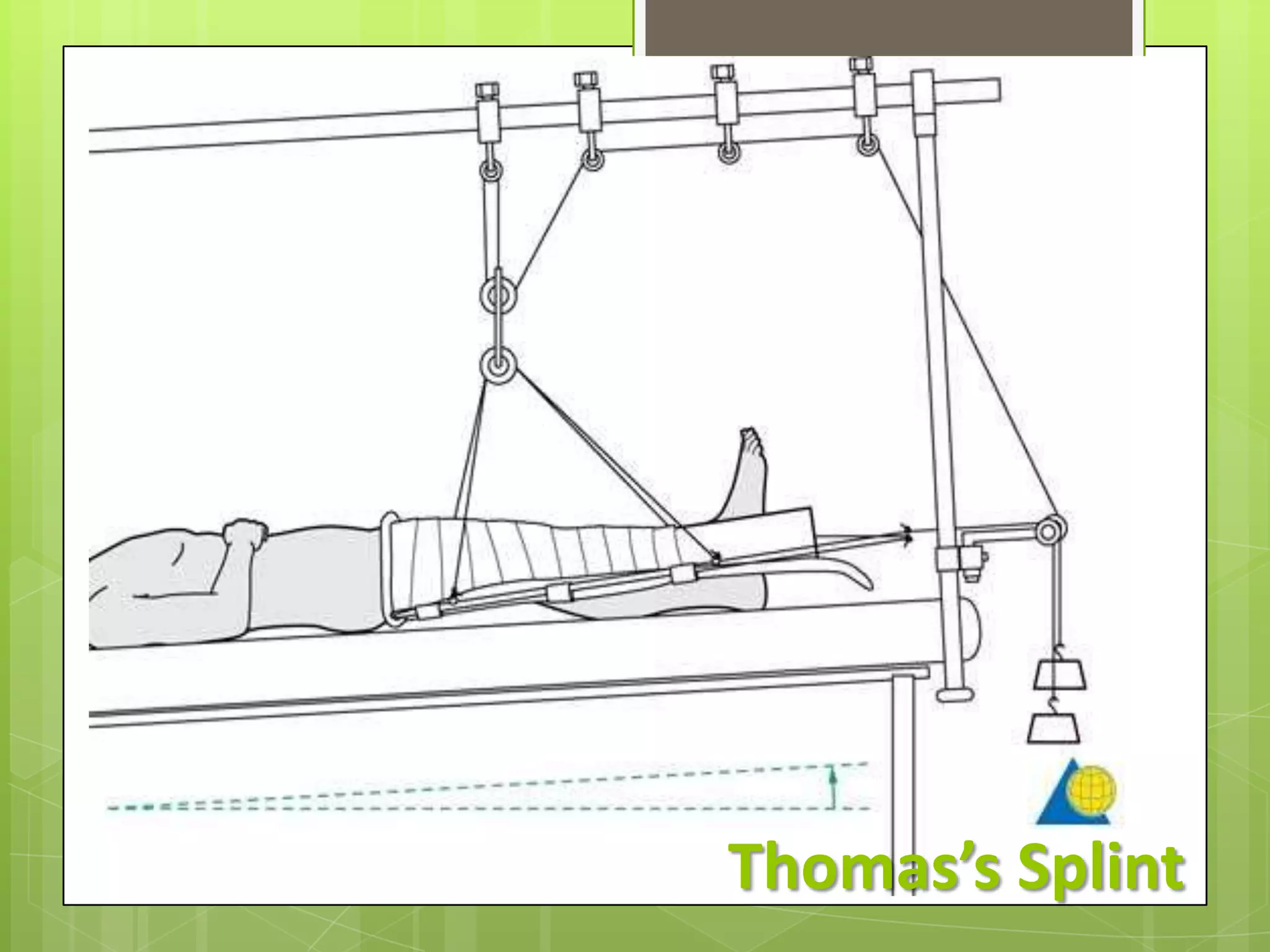
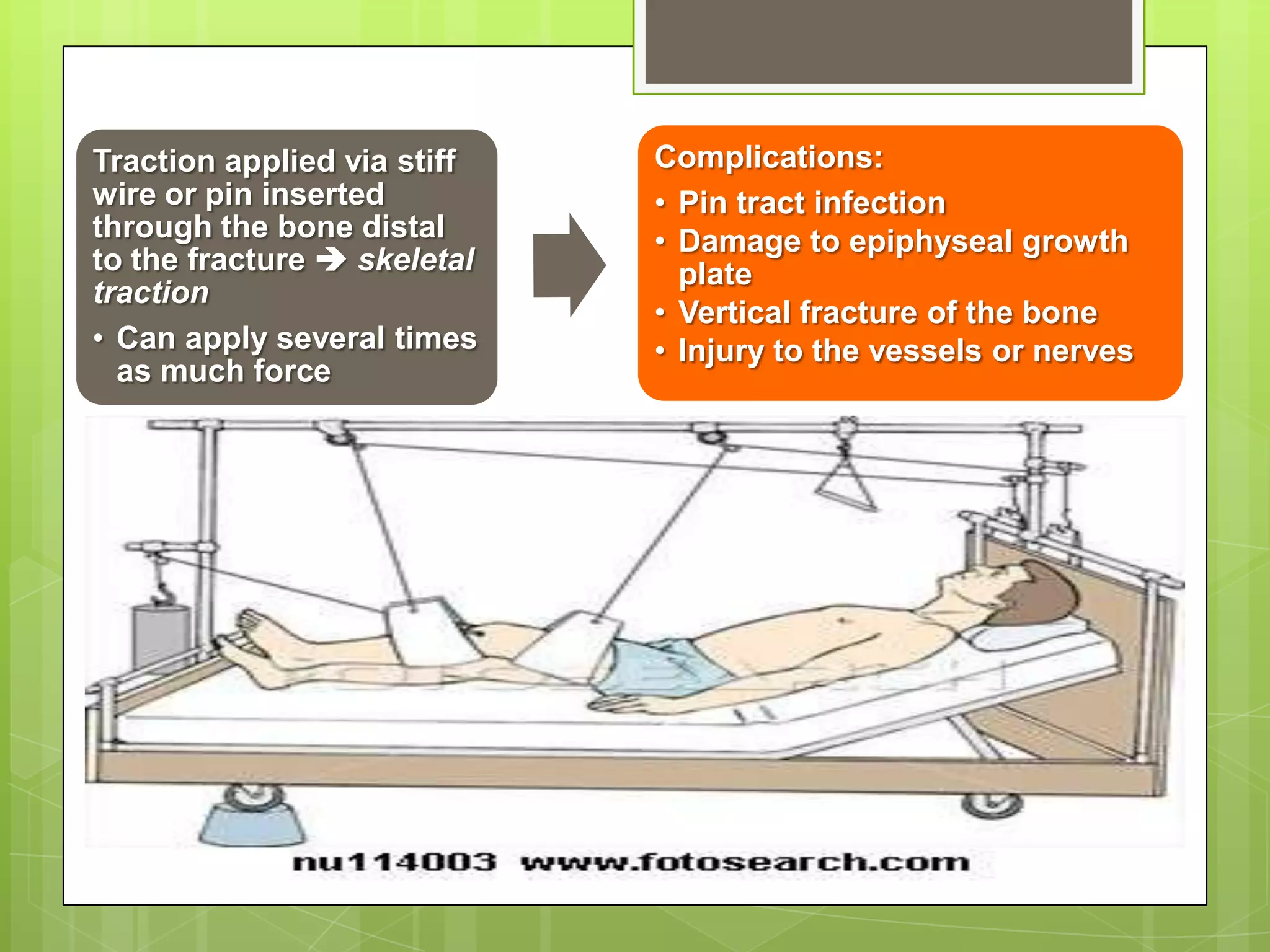
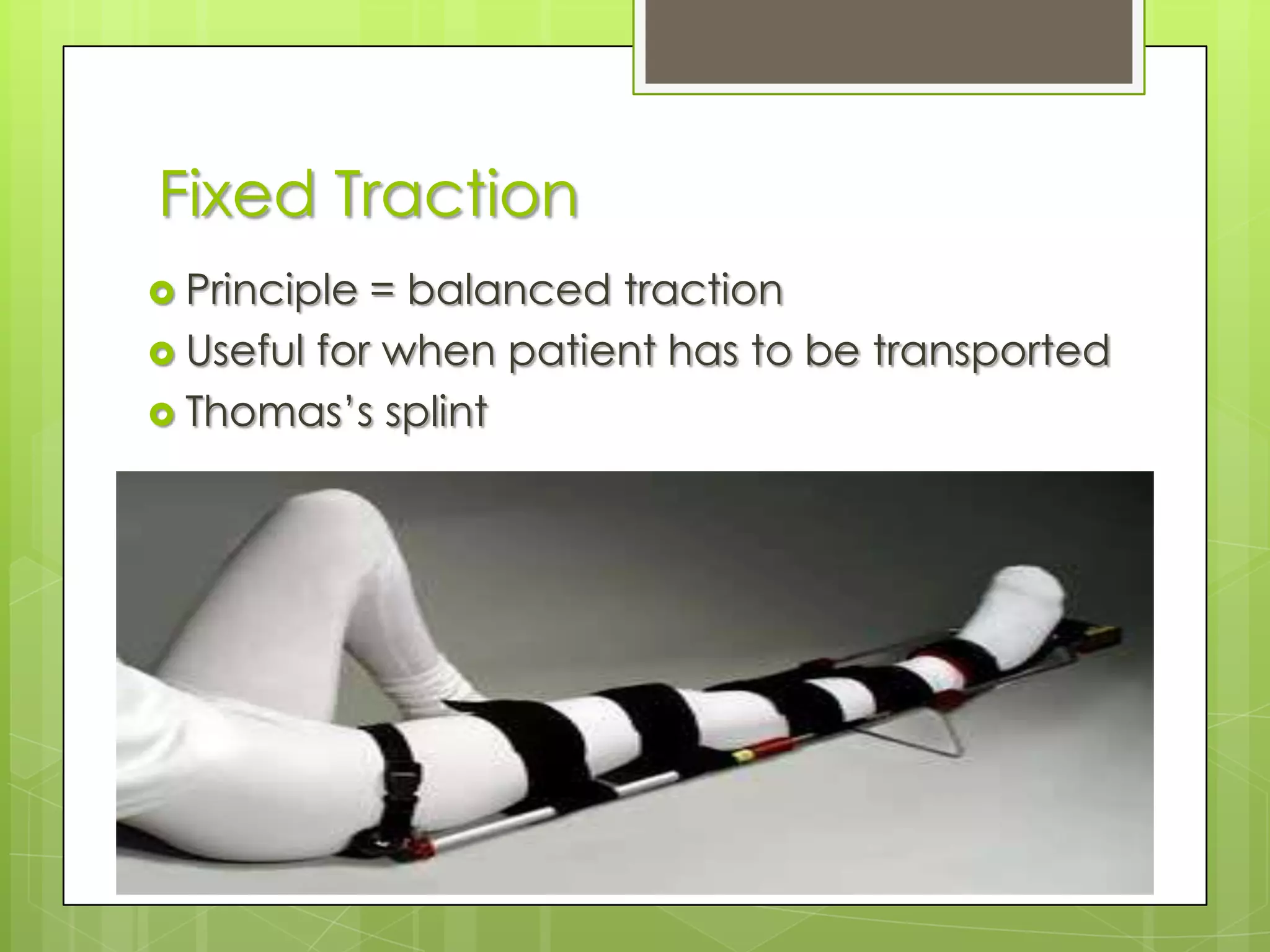
Closed and open reduction methods, indications, advantages, and mechanical traction.
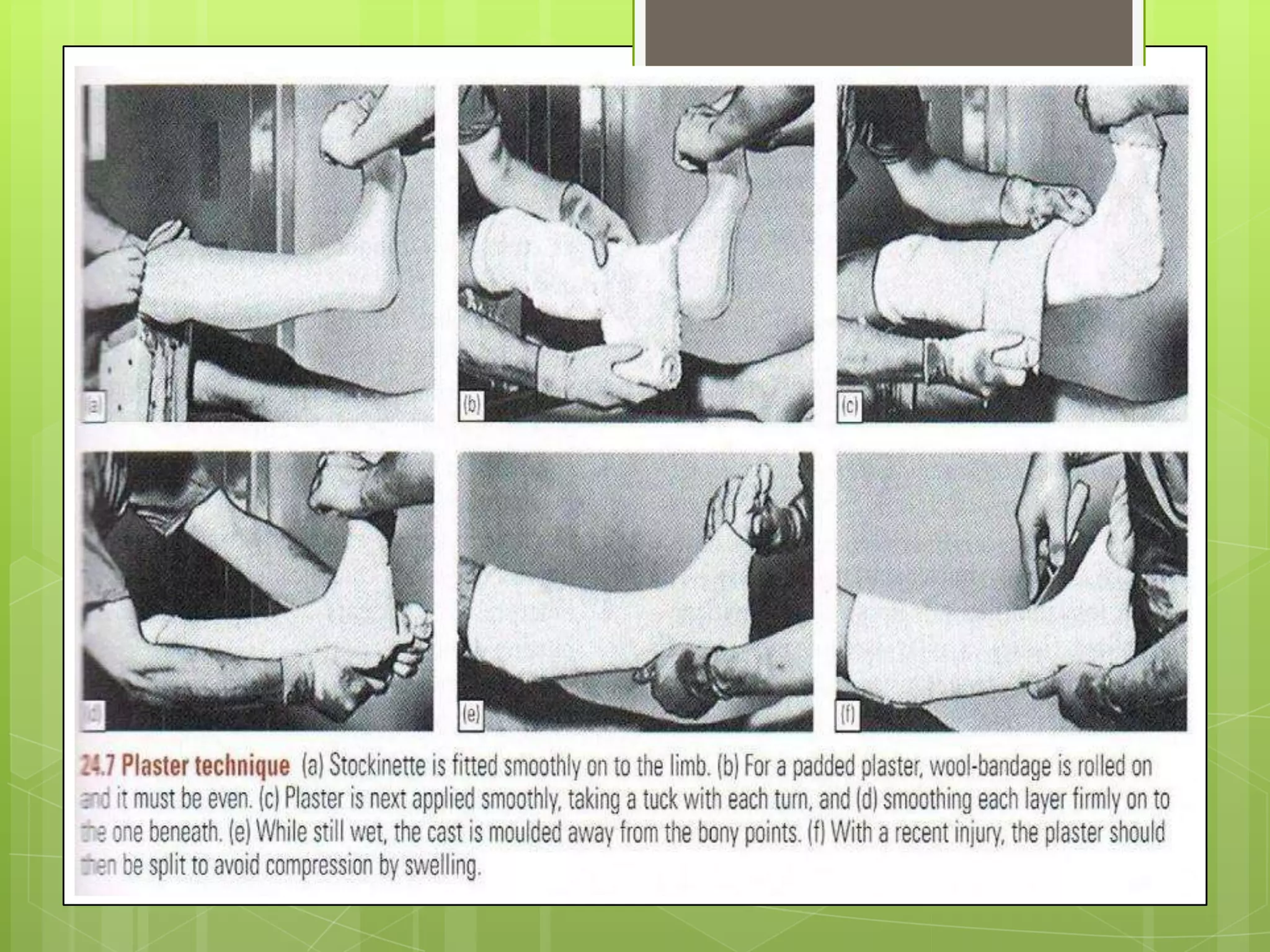
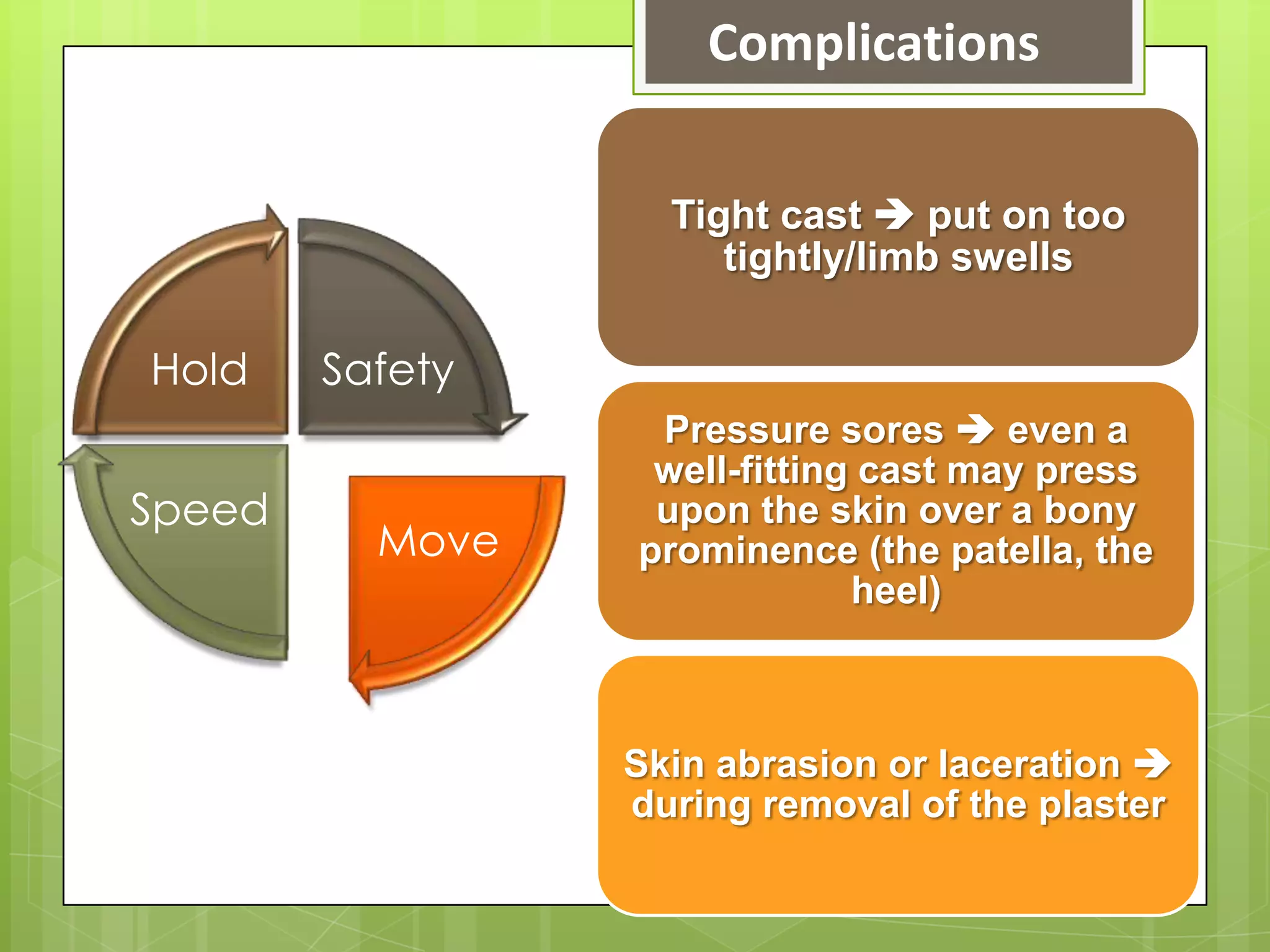
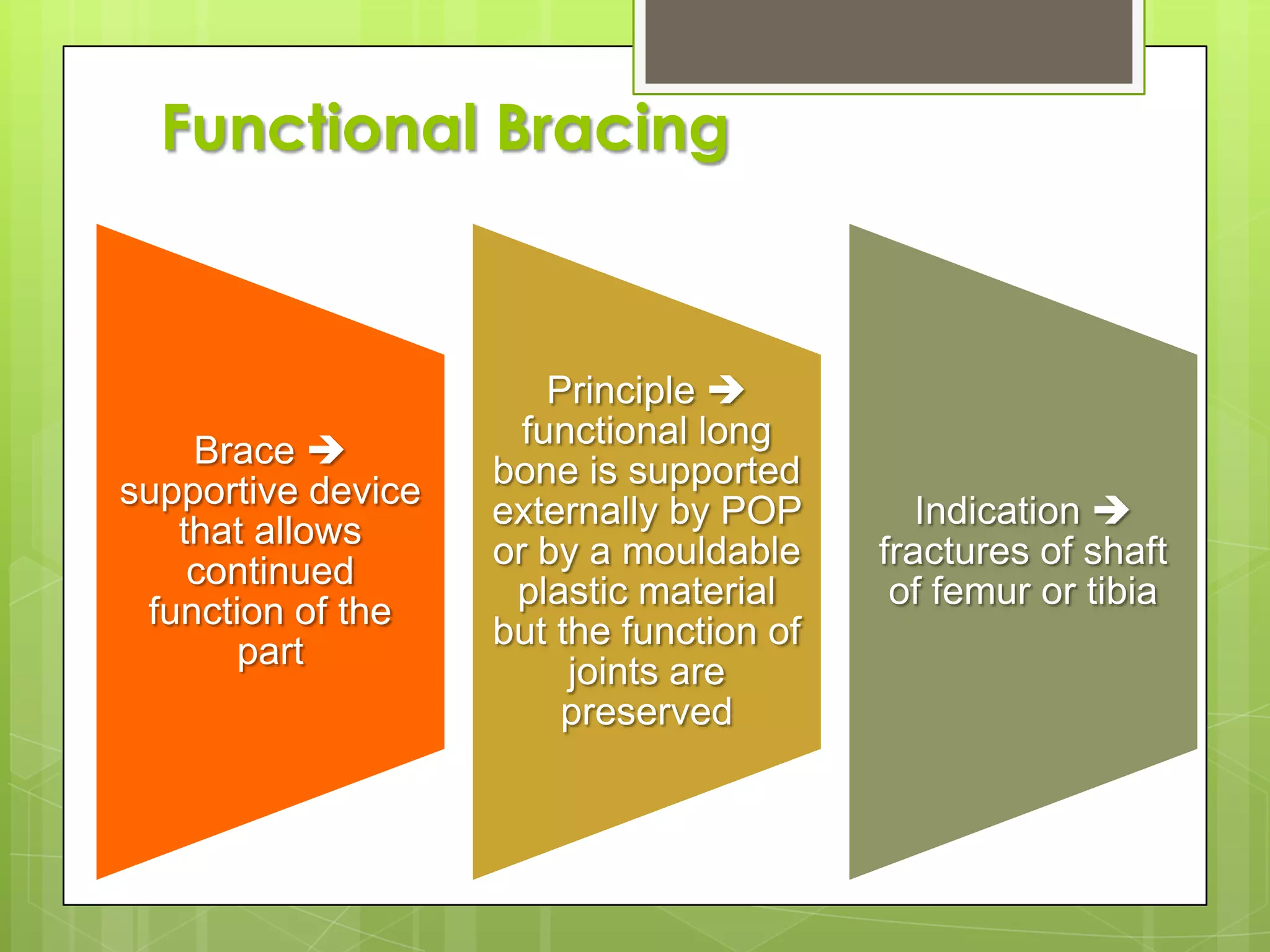
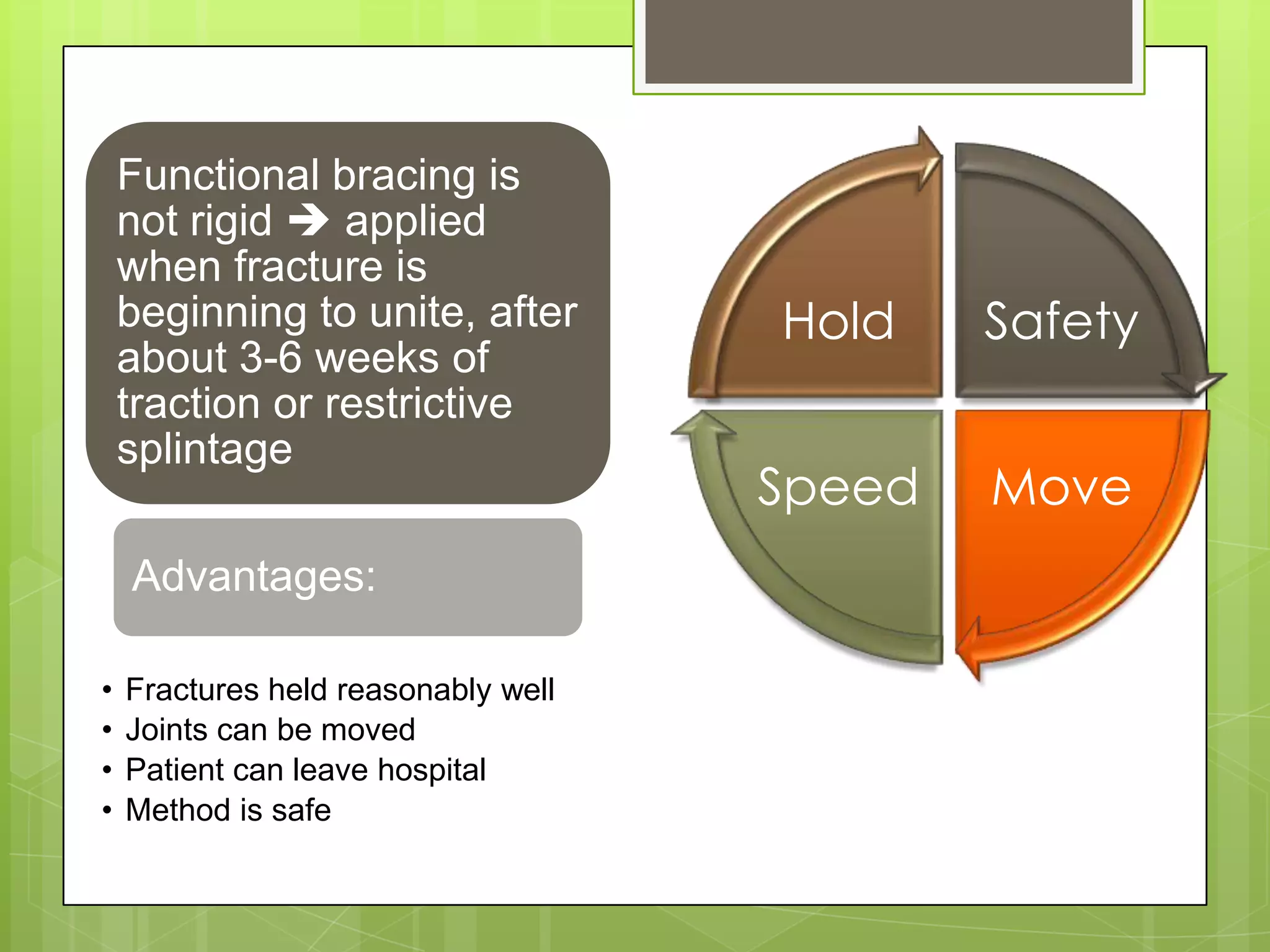
Cast splintage methods for fracture treatment, including advantages and disadvantages.
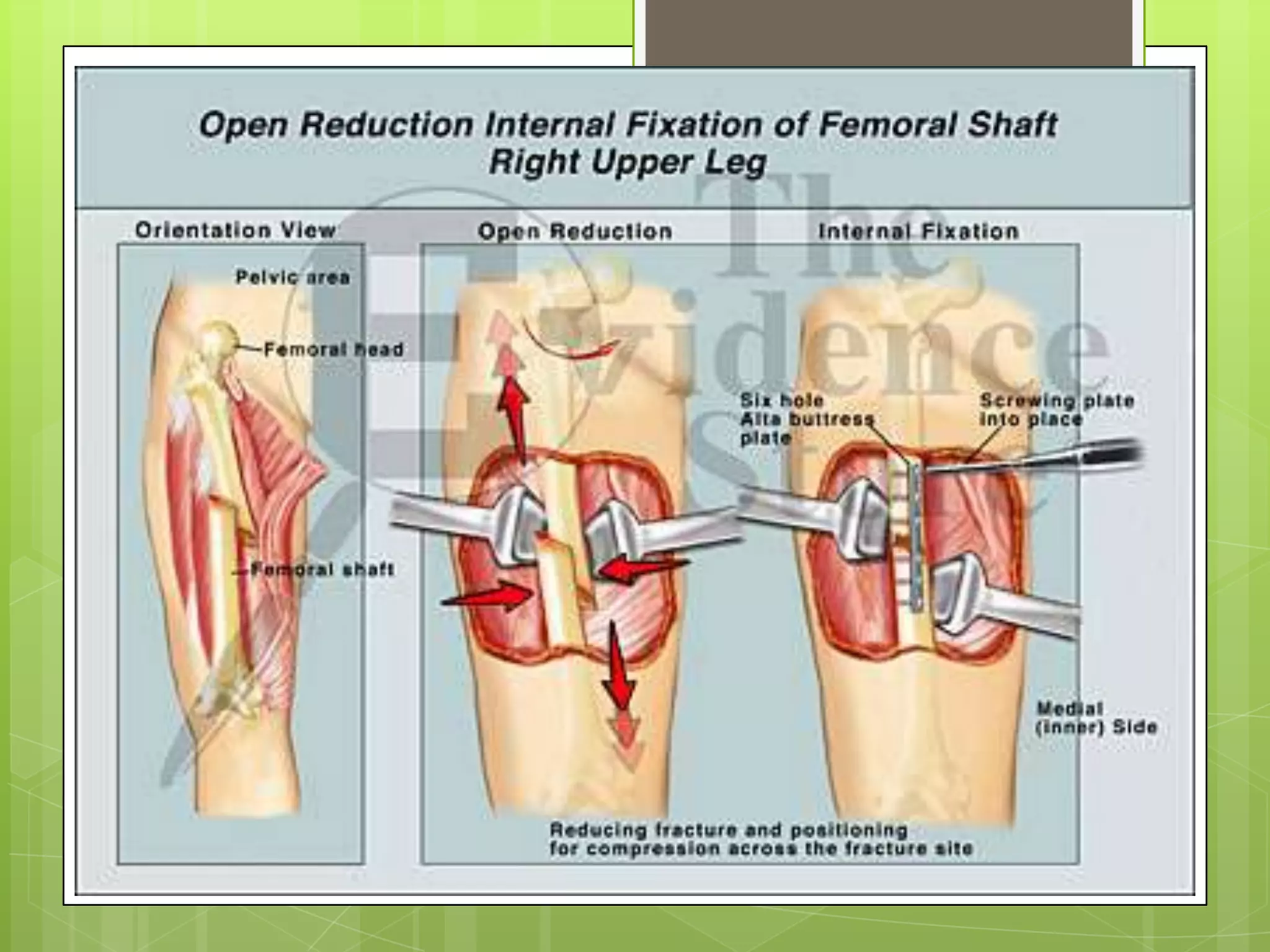
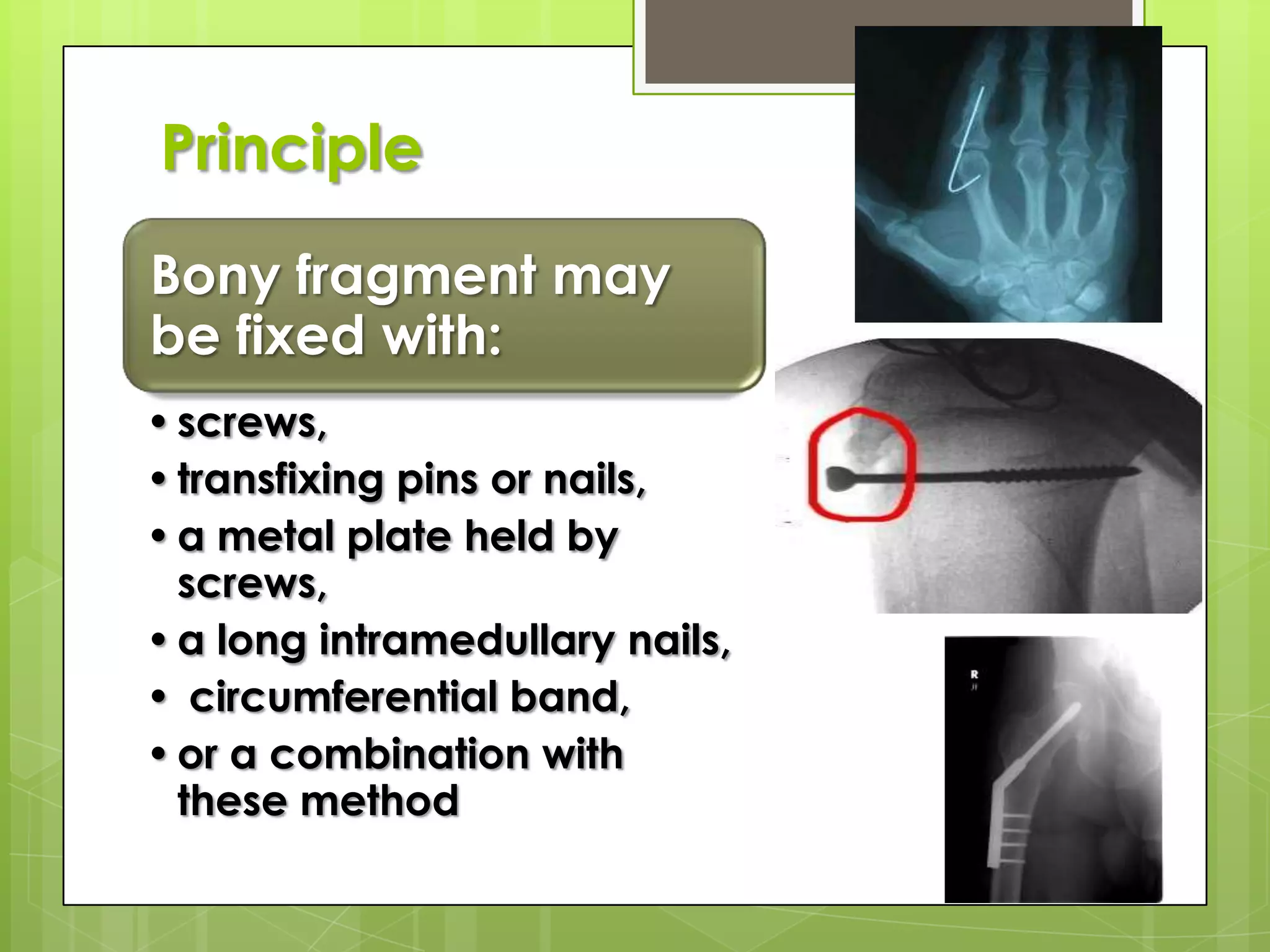
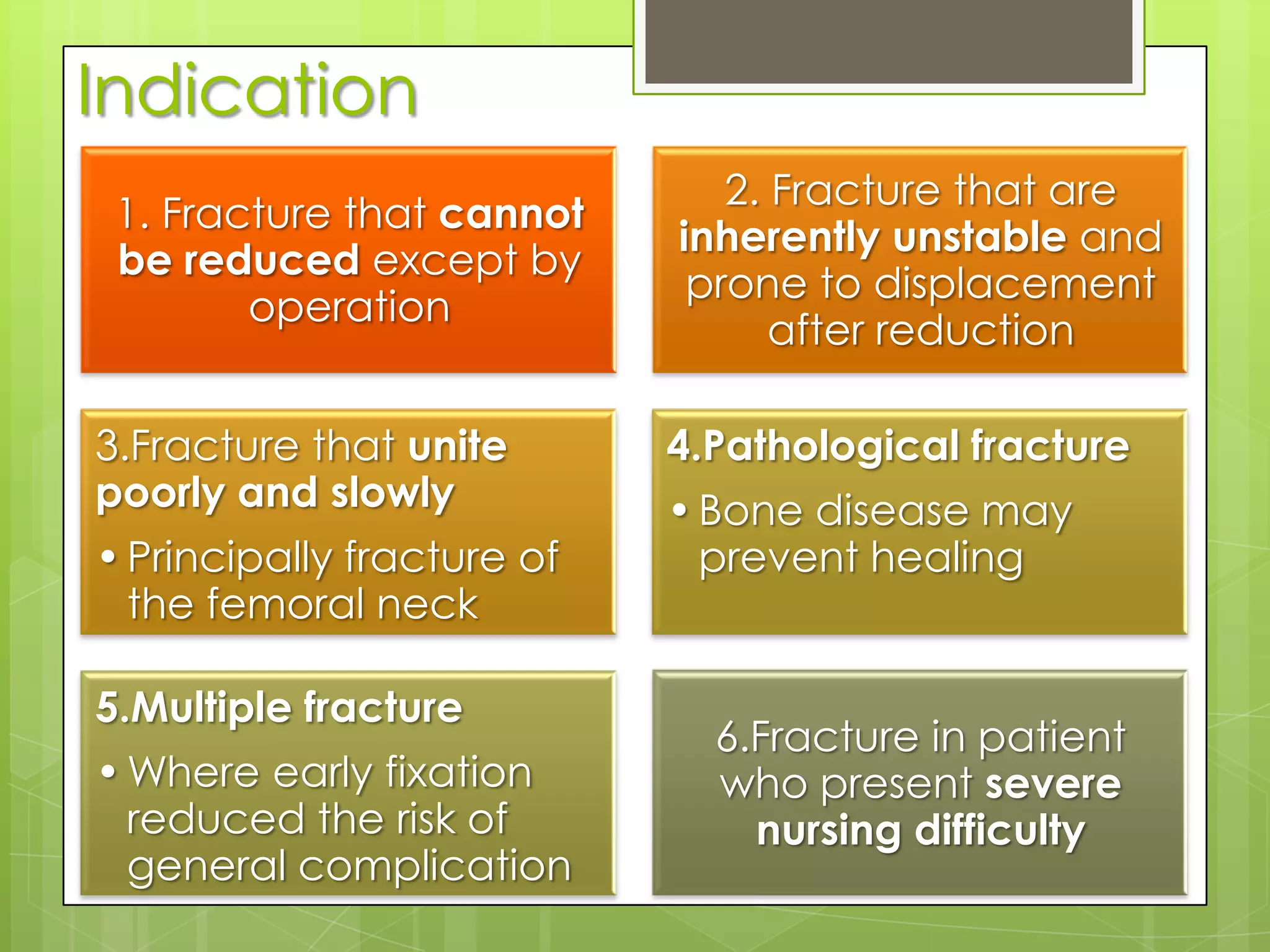
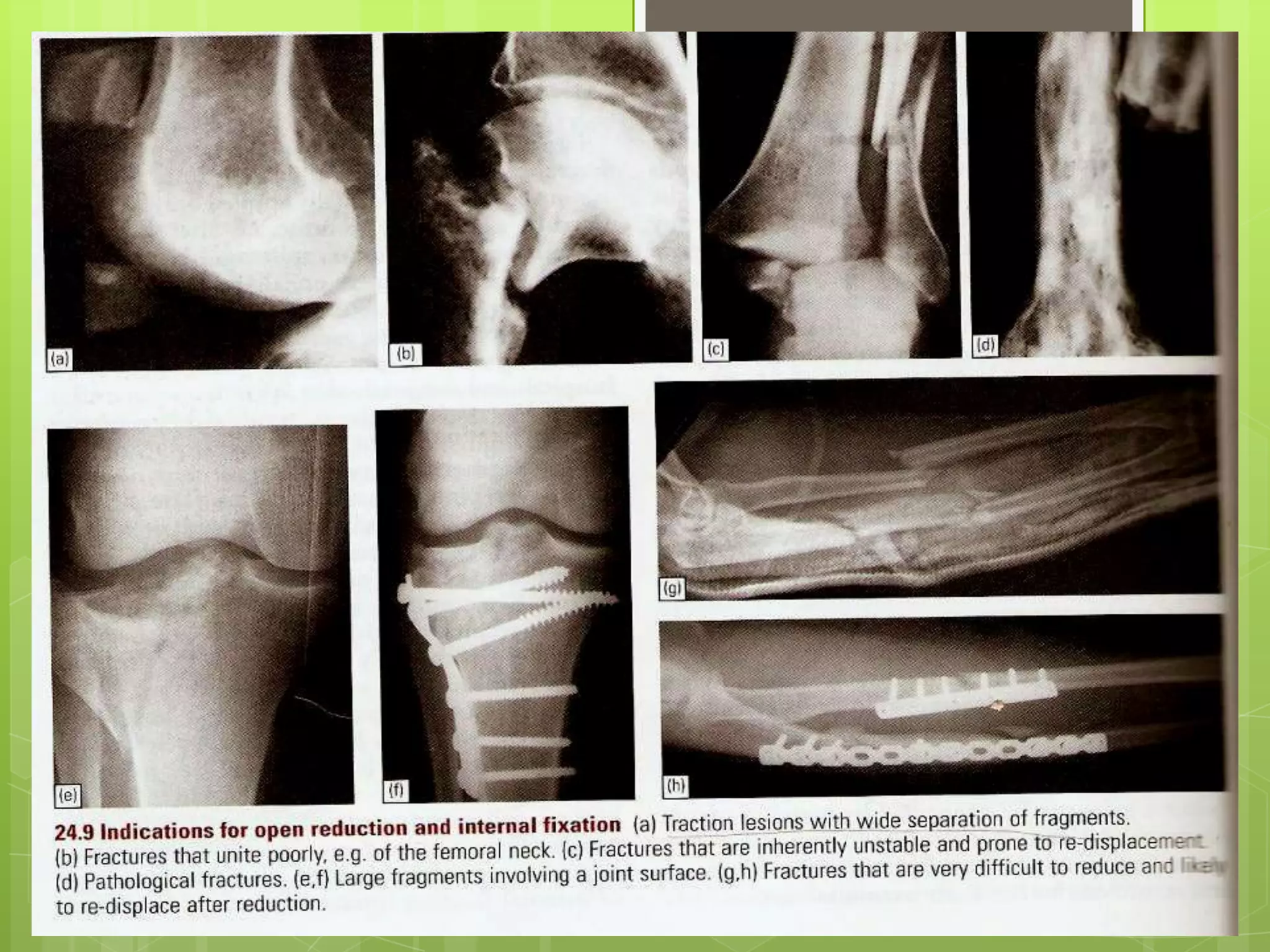
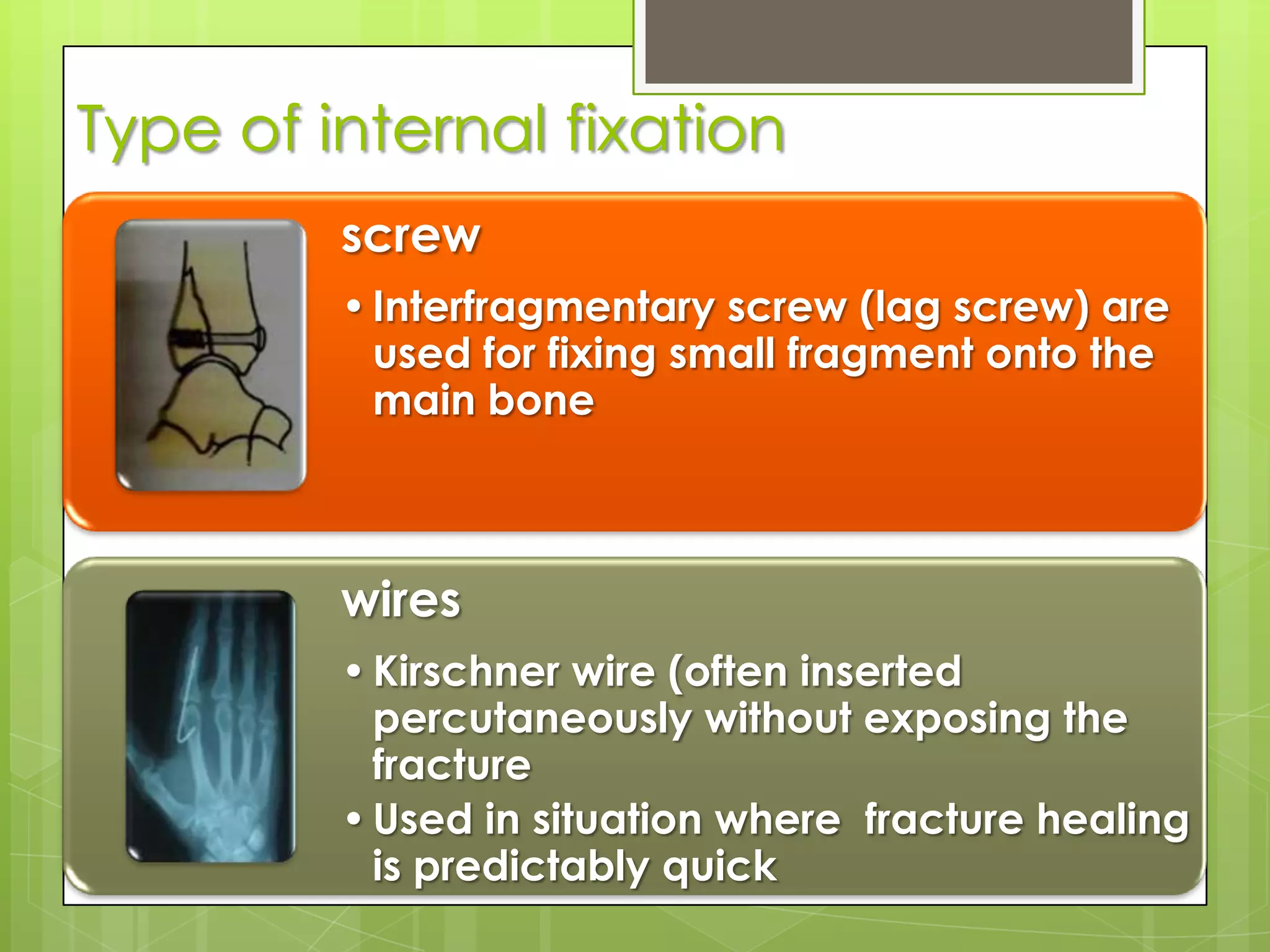
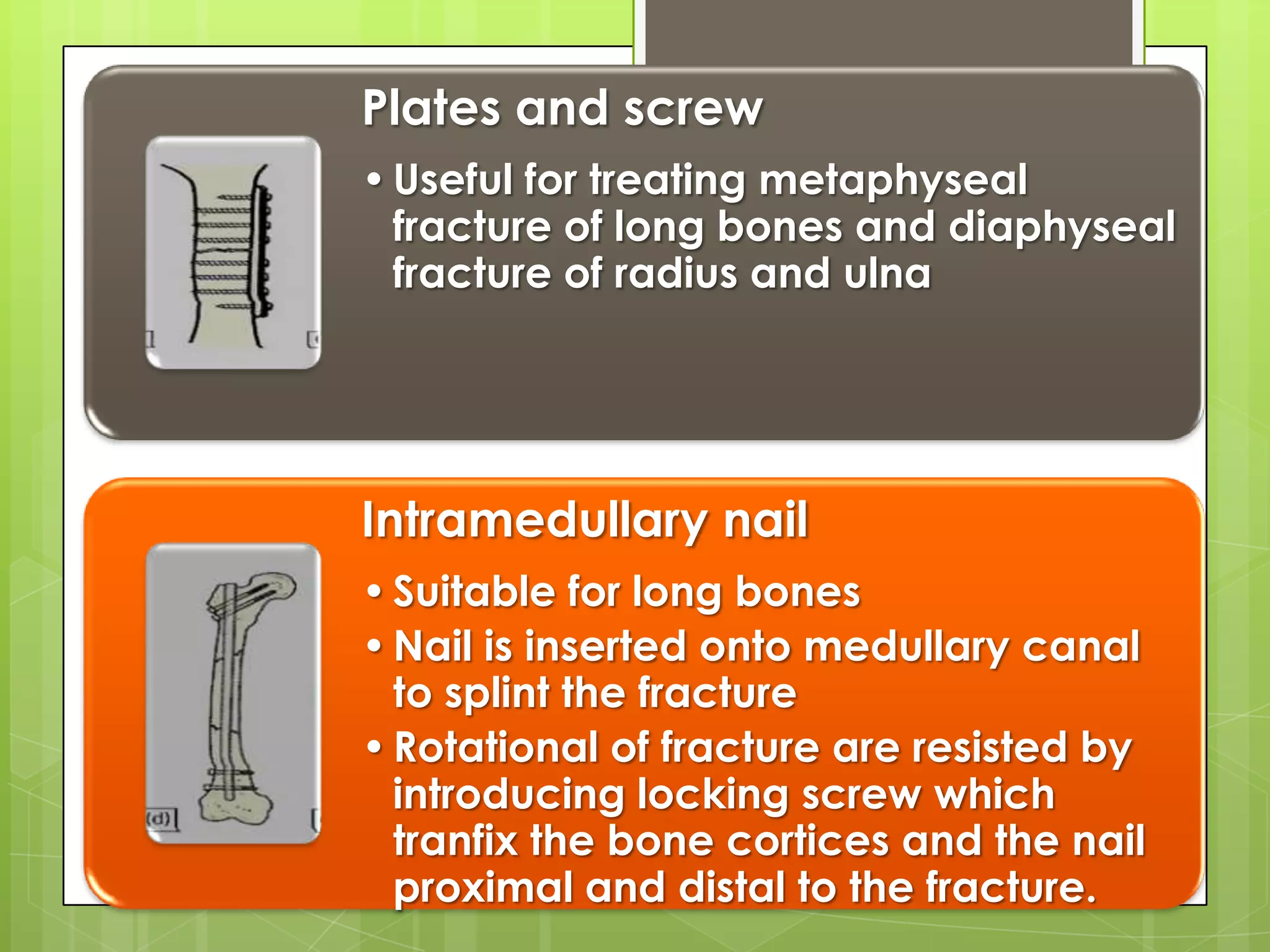
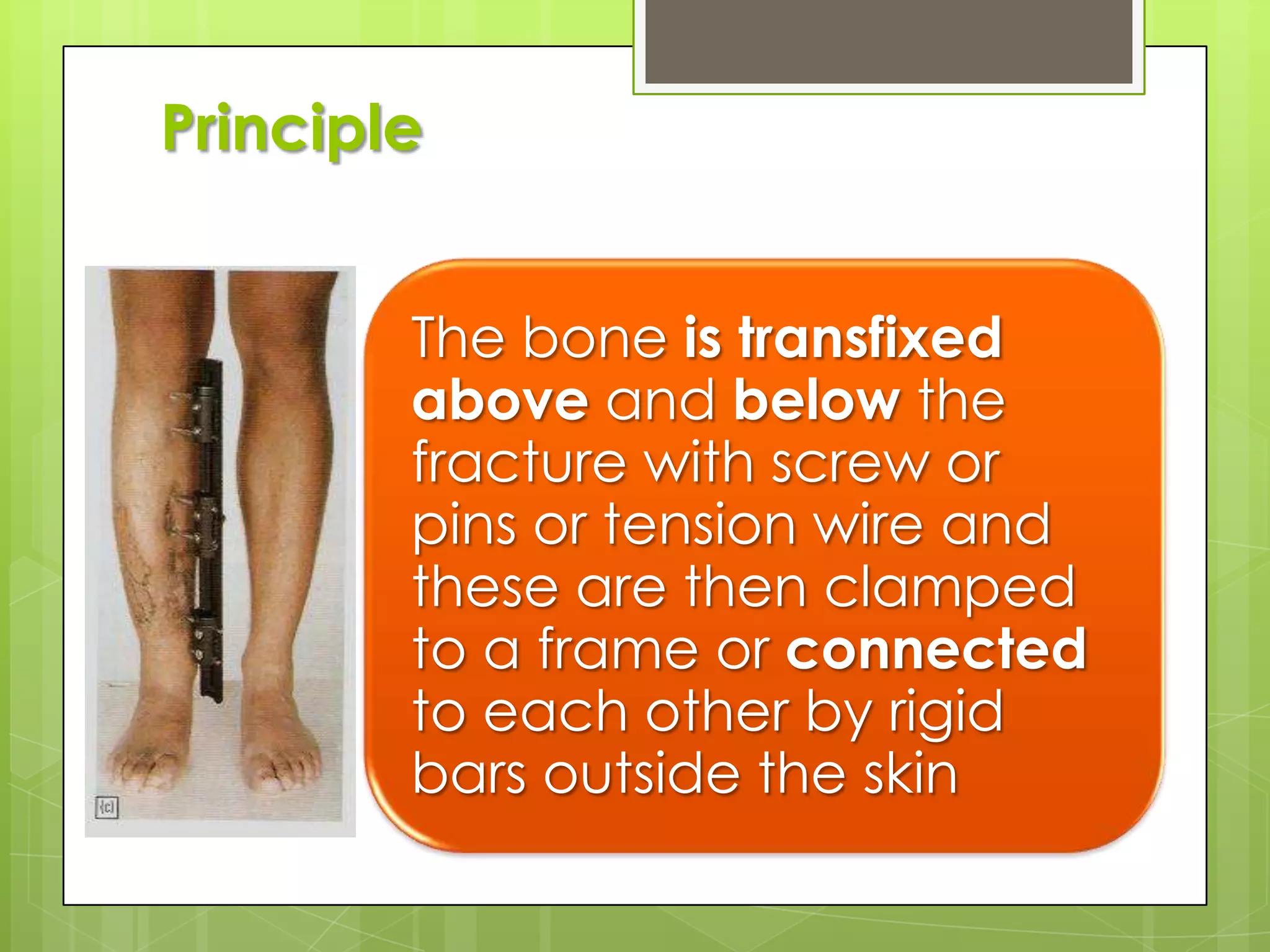
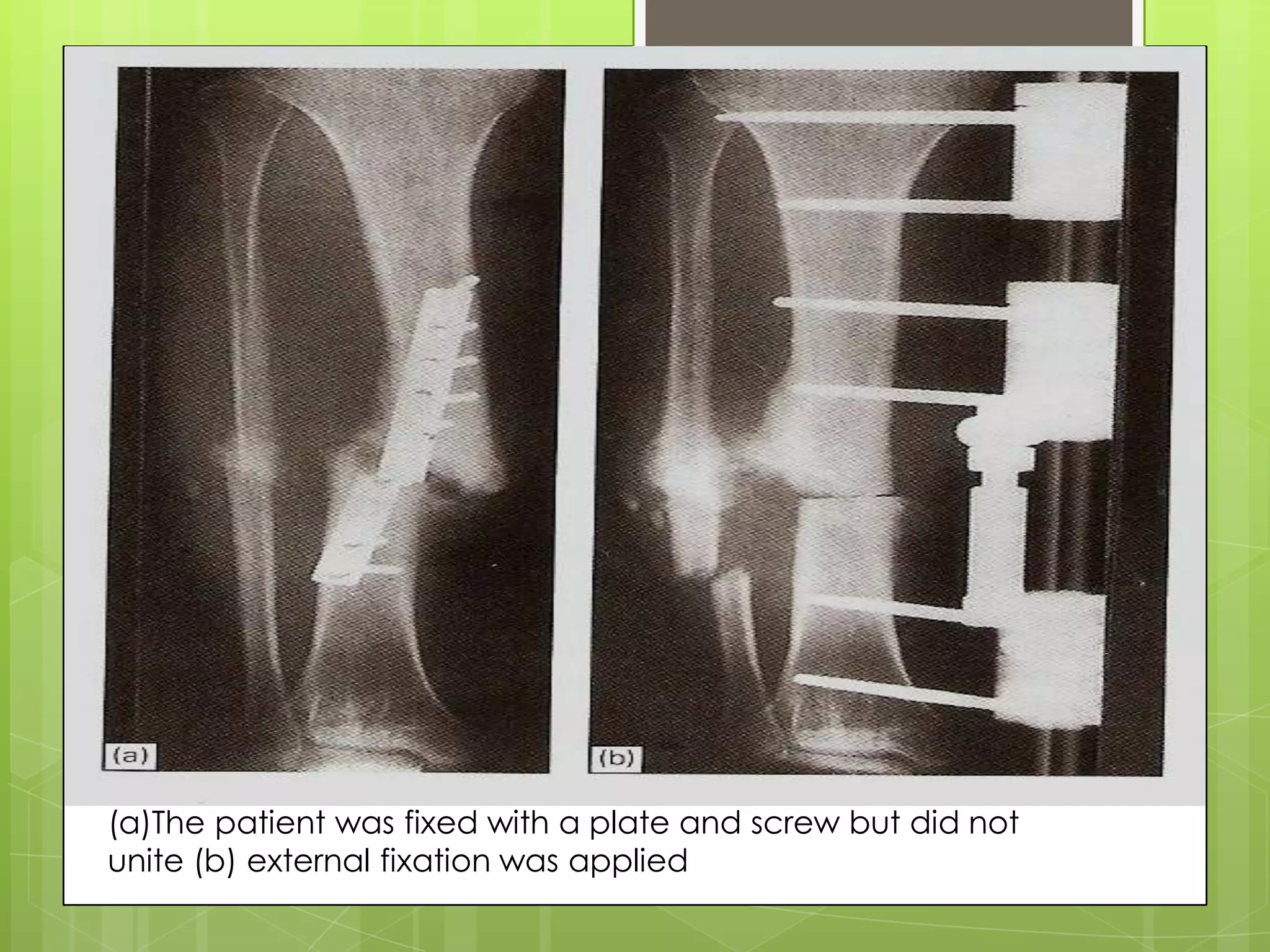
Overview of internal and external fixation principles, indications, and advantages.
Importance of exercise and rehabilitation in preventing complications after fractures.
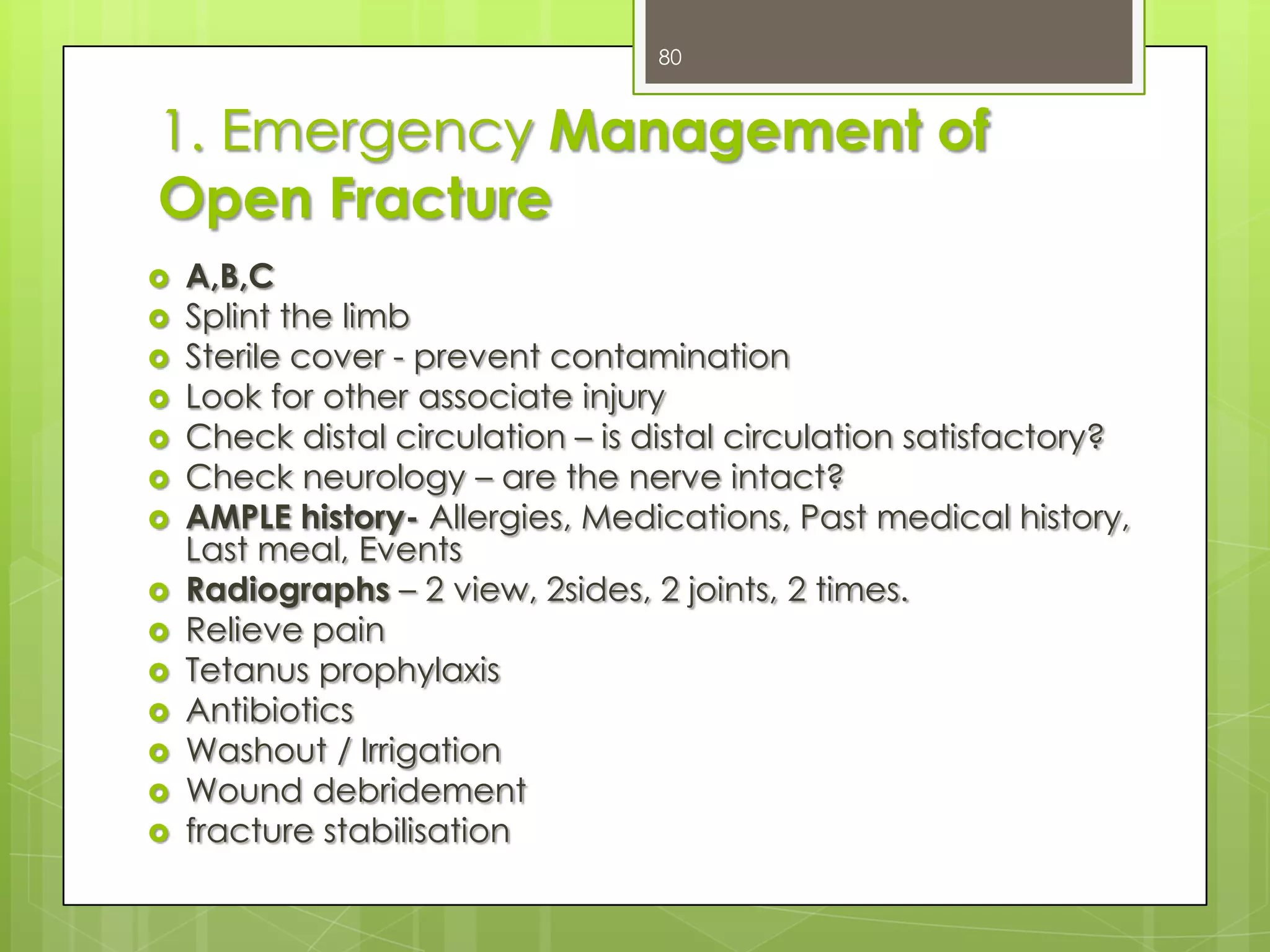
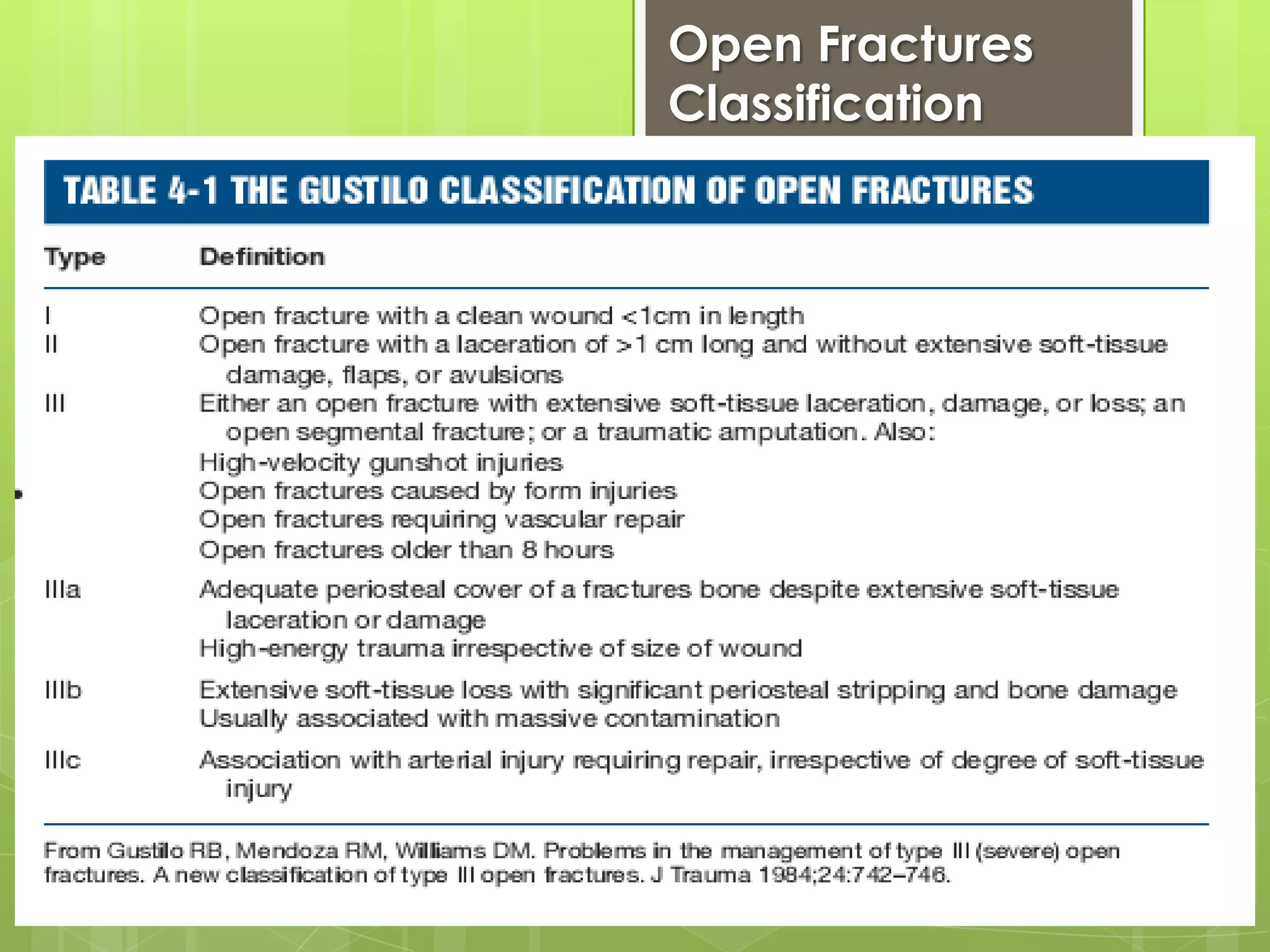
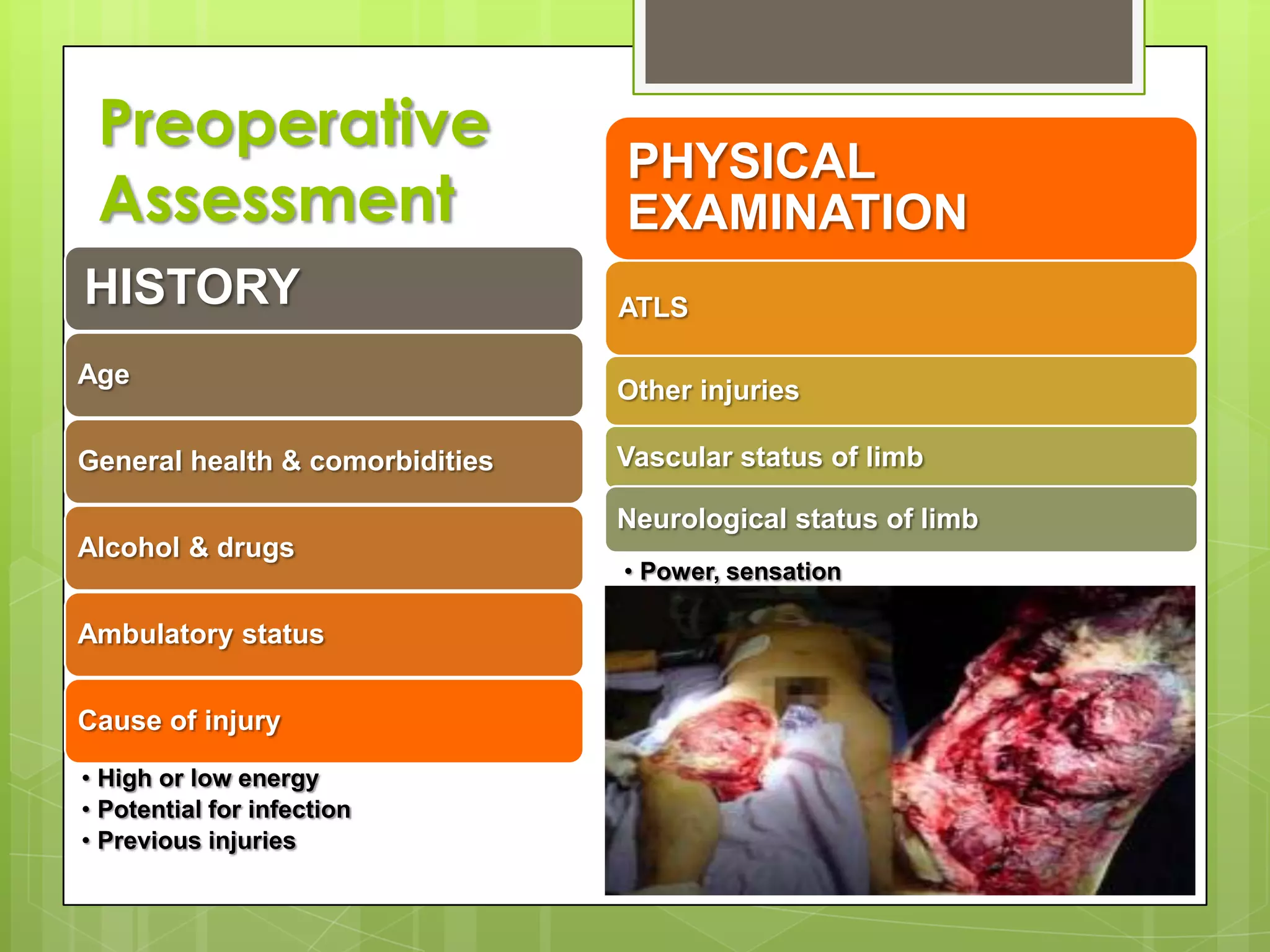
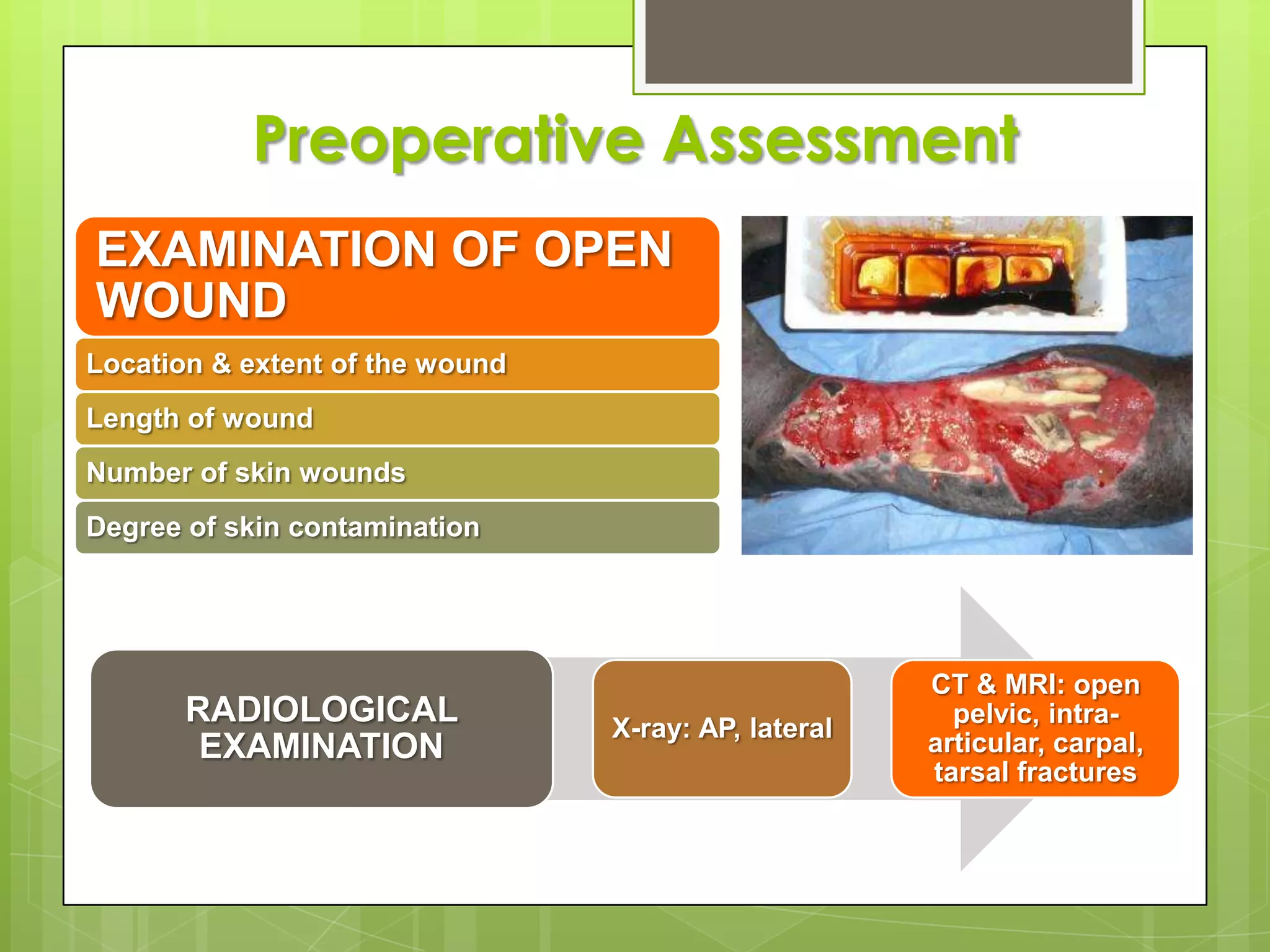
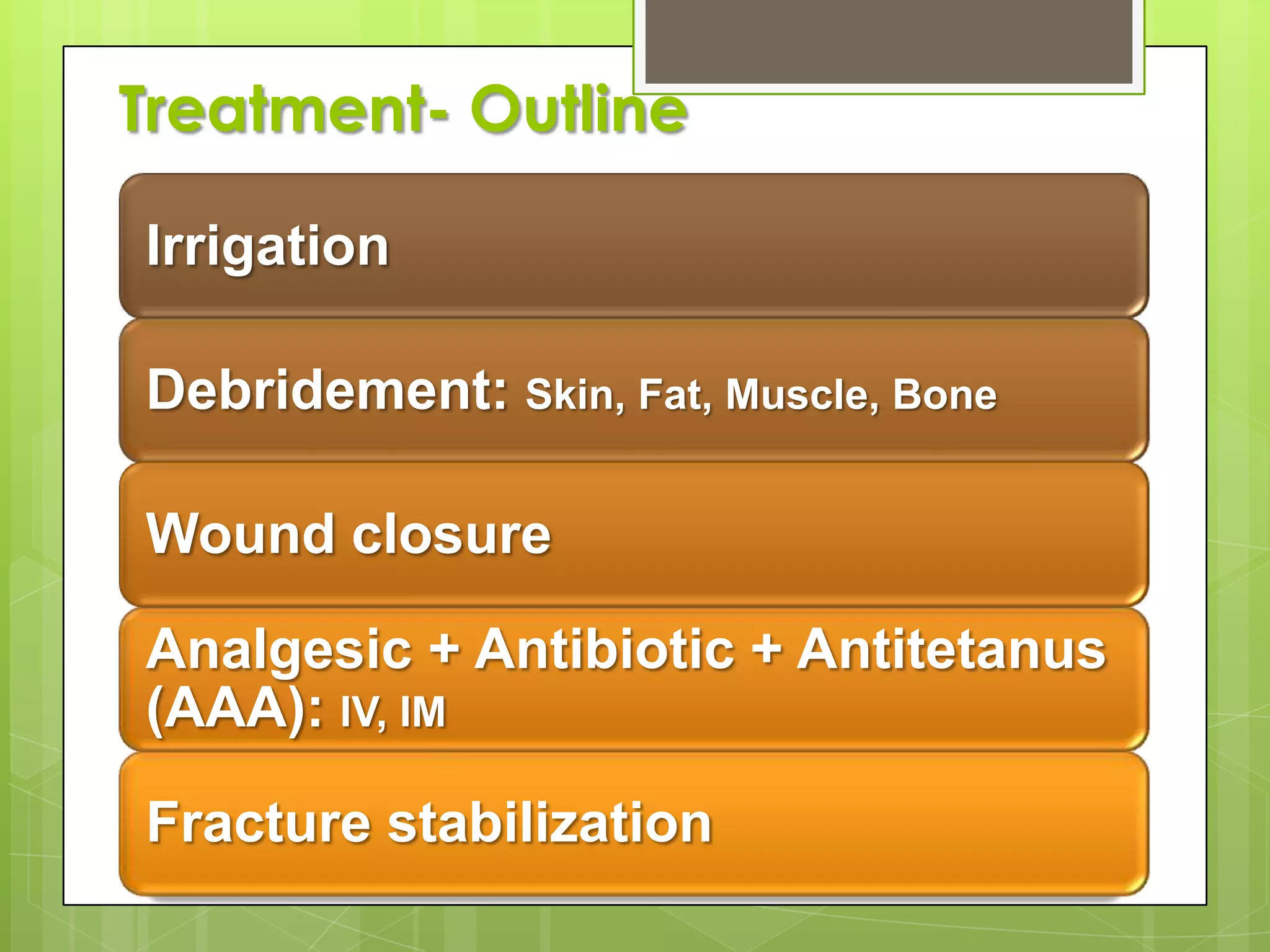
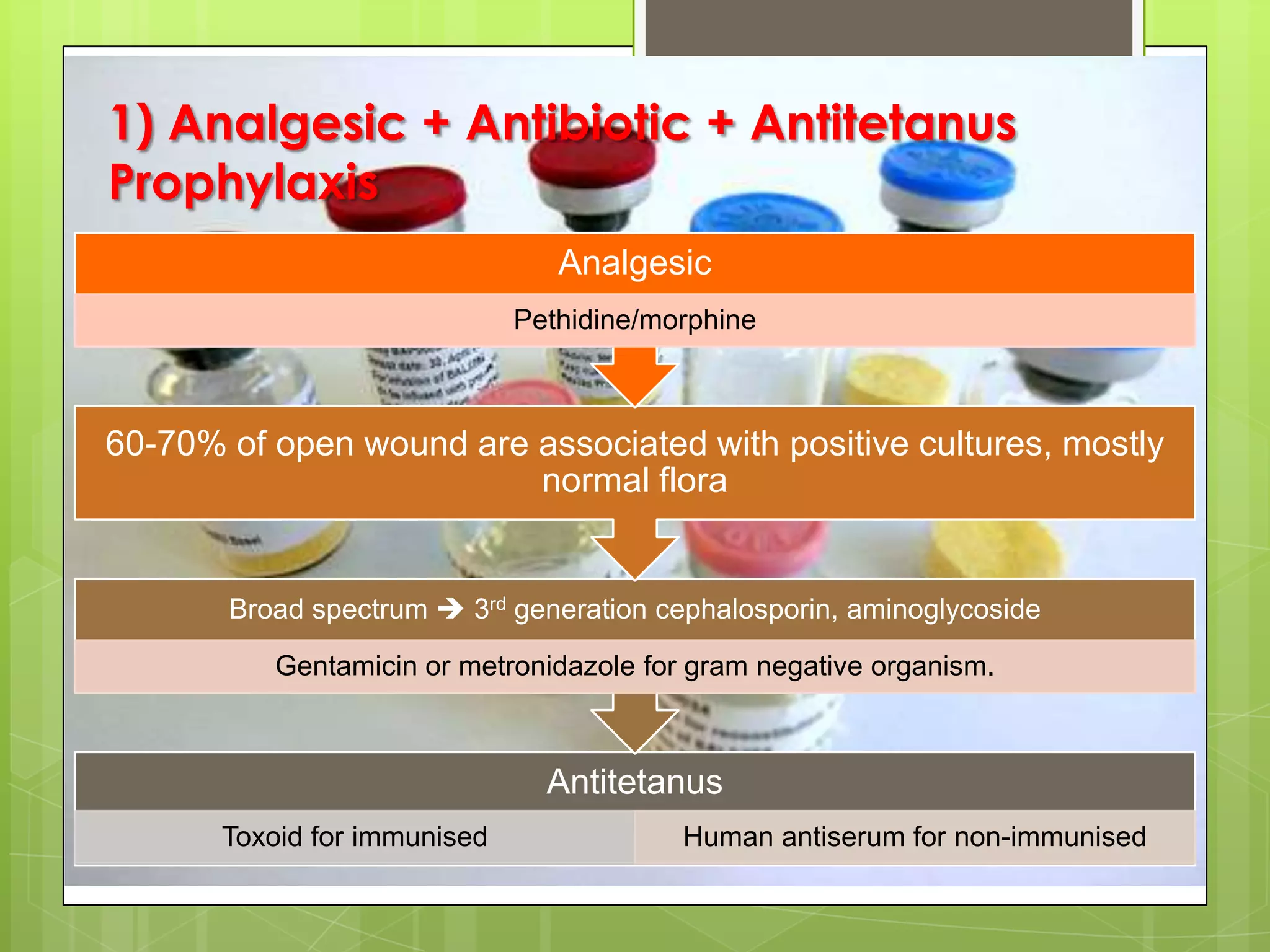
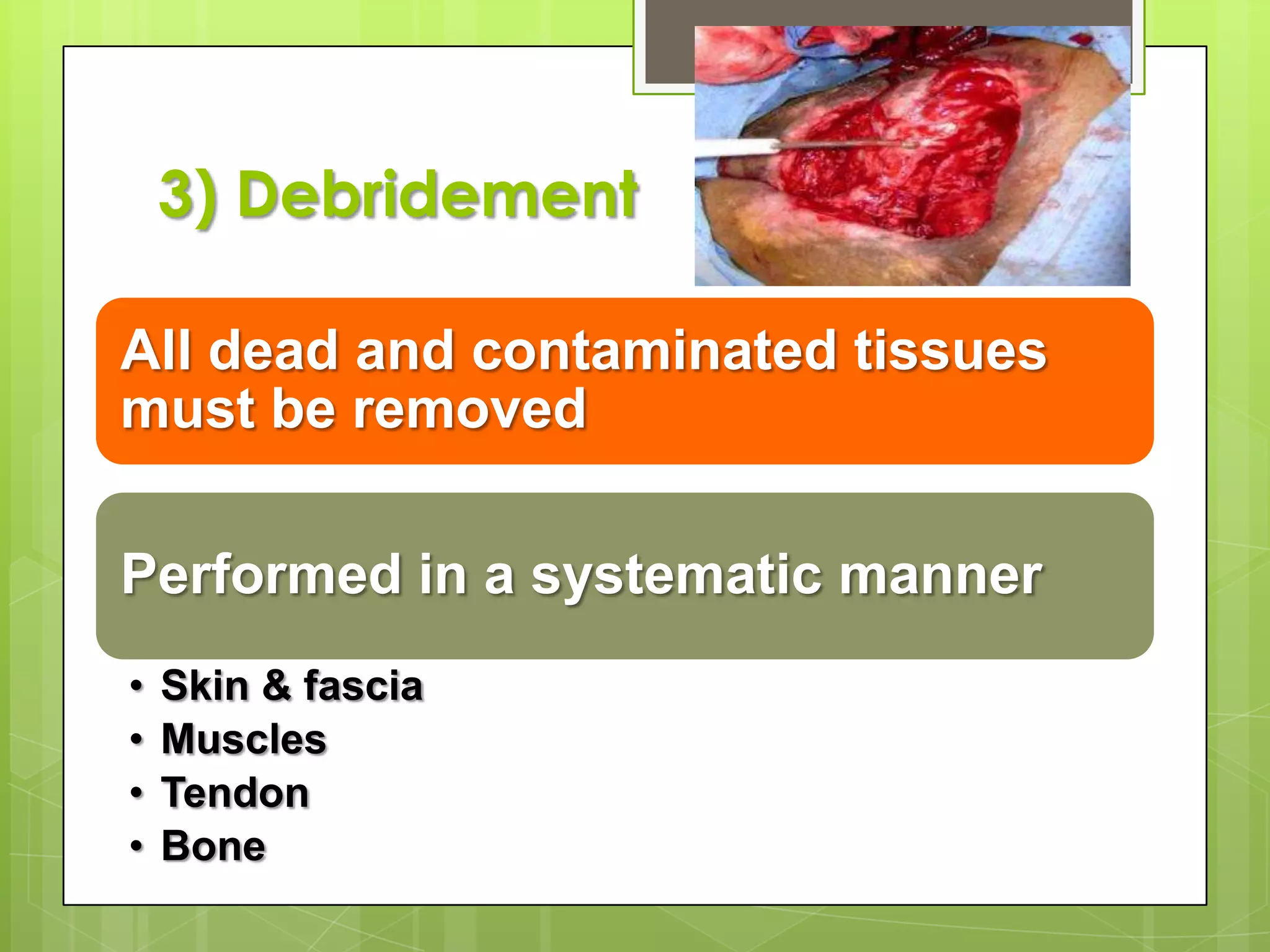
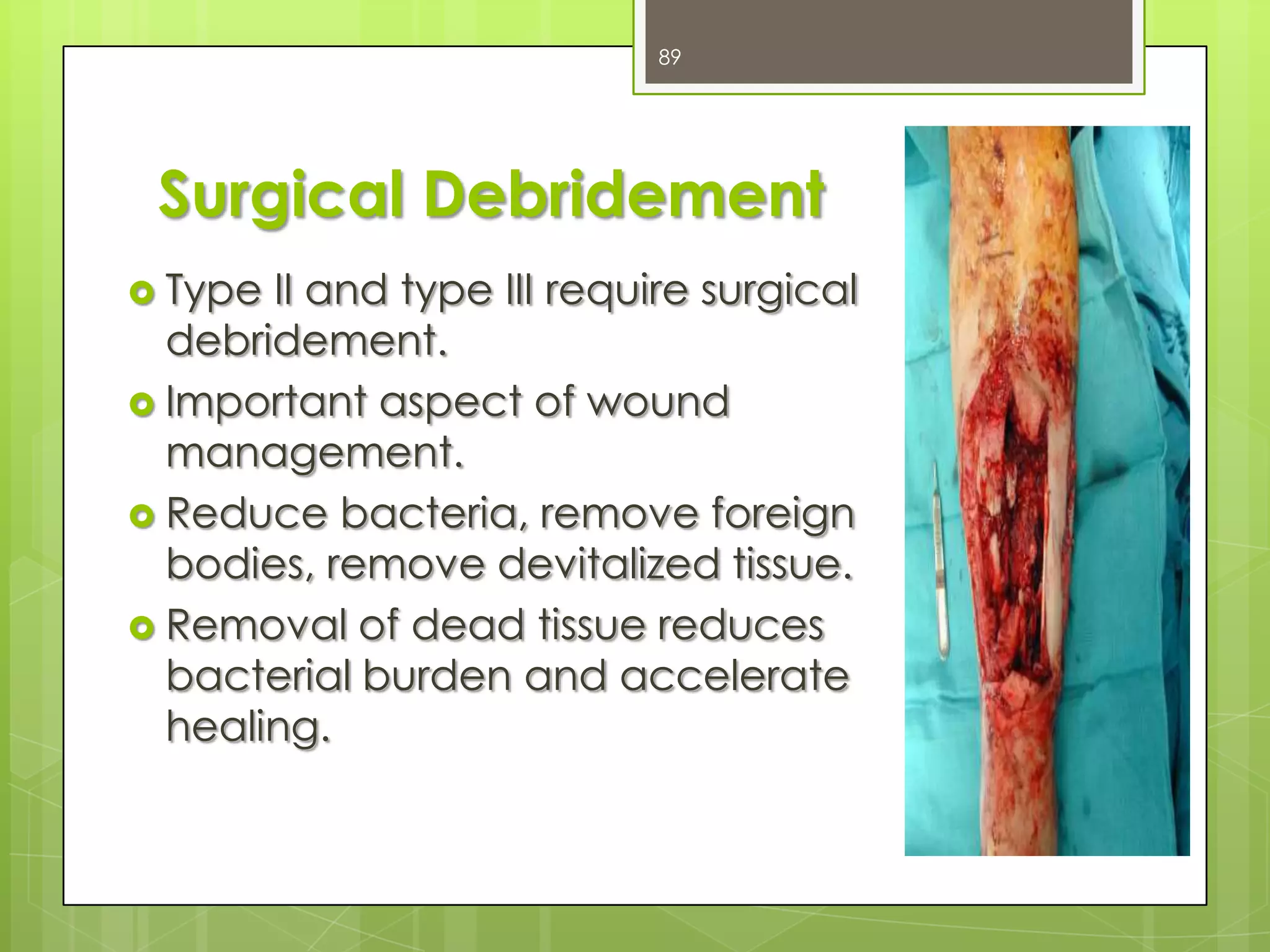
Management strategies for open fractures, including first aid and treatment protocols.
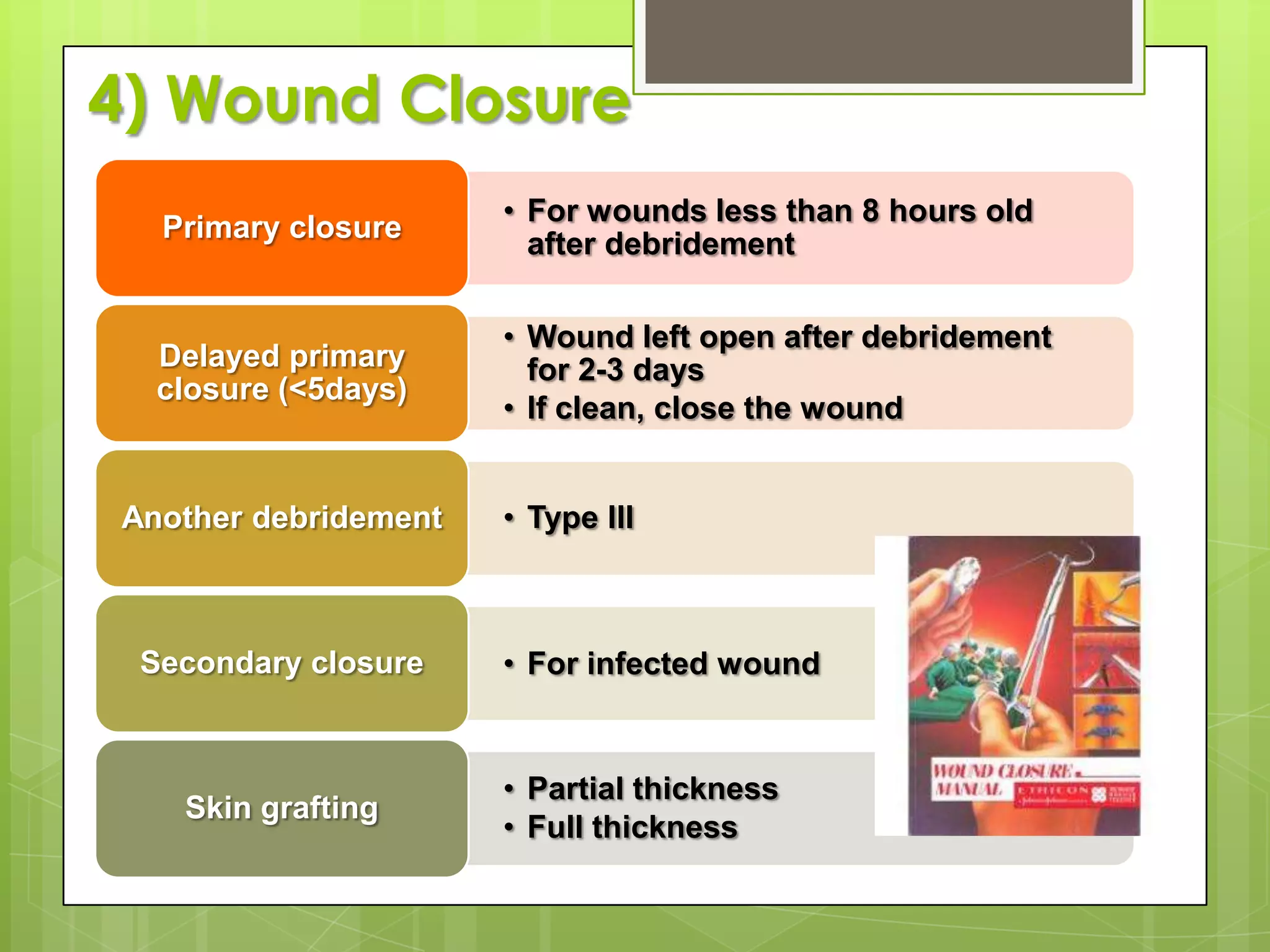
Tactics for wound closure and methods of fracture stabilization post-injury.
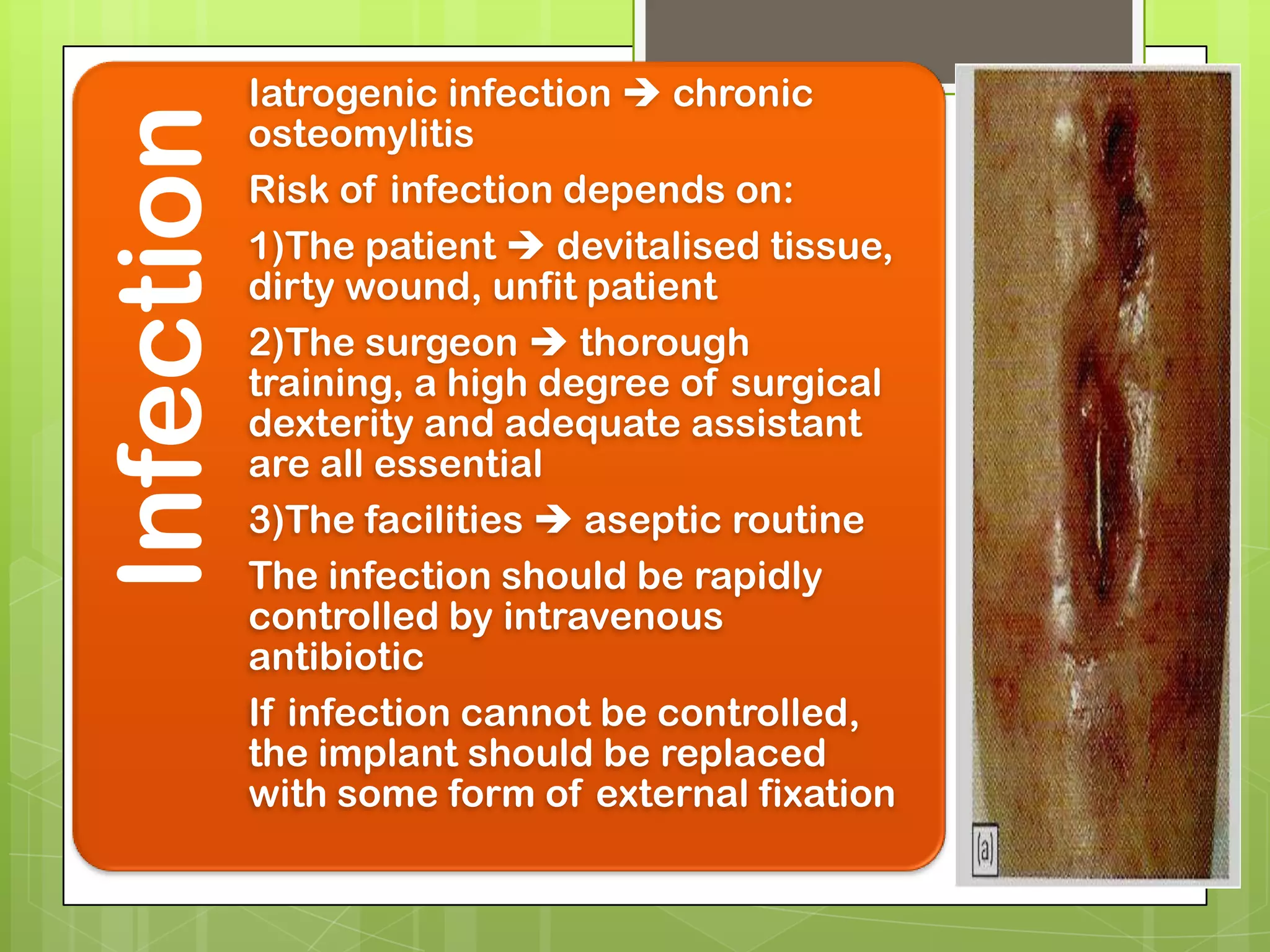
Exploration of general, bone, joint, and soft tissue complications arising from fractures.
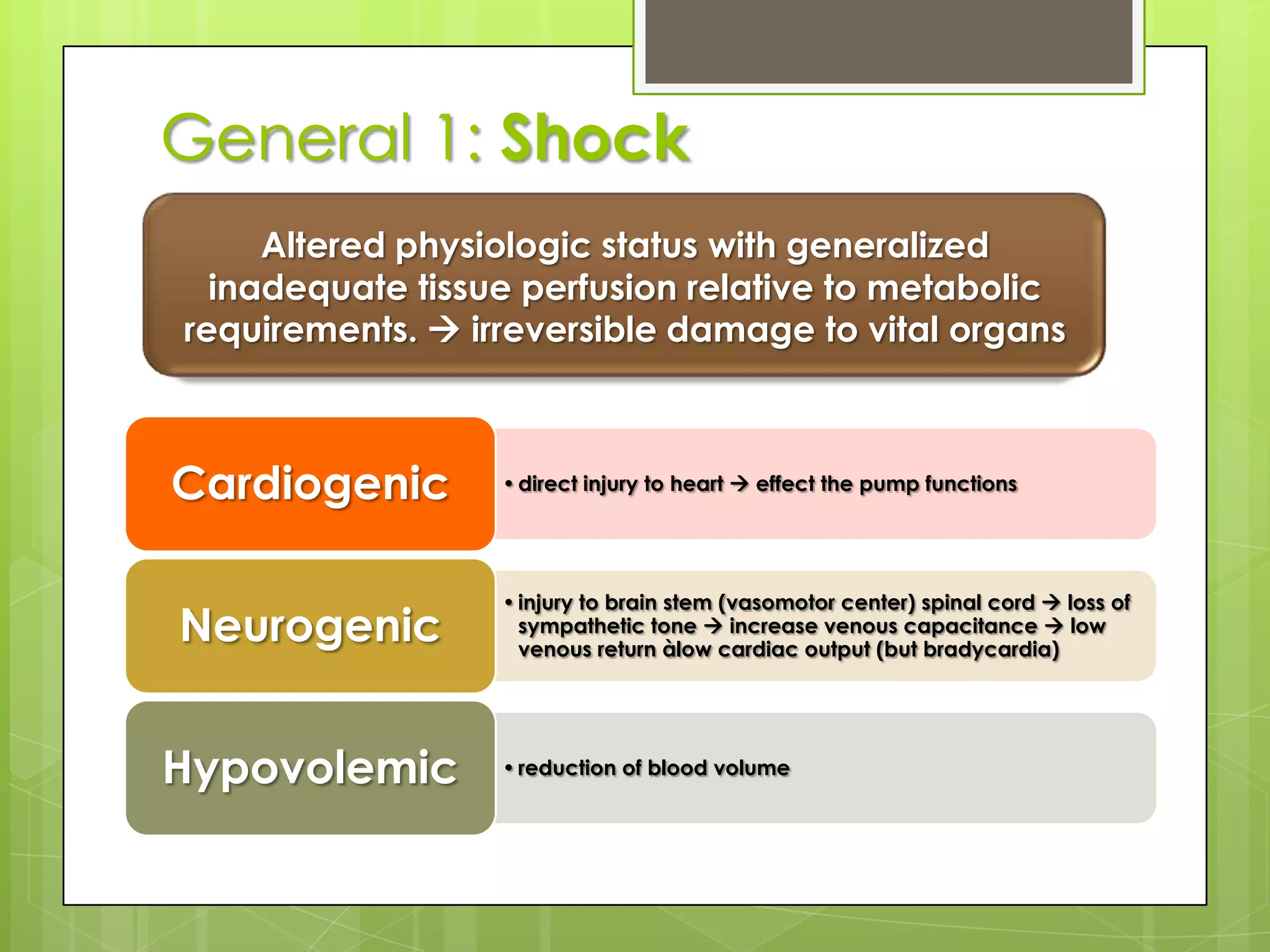
Understanding shock after fractures, including its physiological impact.
Management and prevention of DVT and pulmonary embolism related to fractures.
Information on fat embolism and gas gangrene complications from fractures.
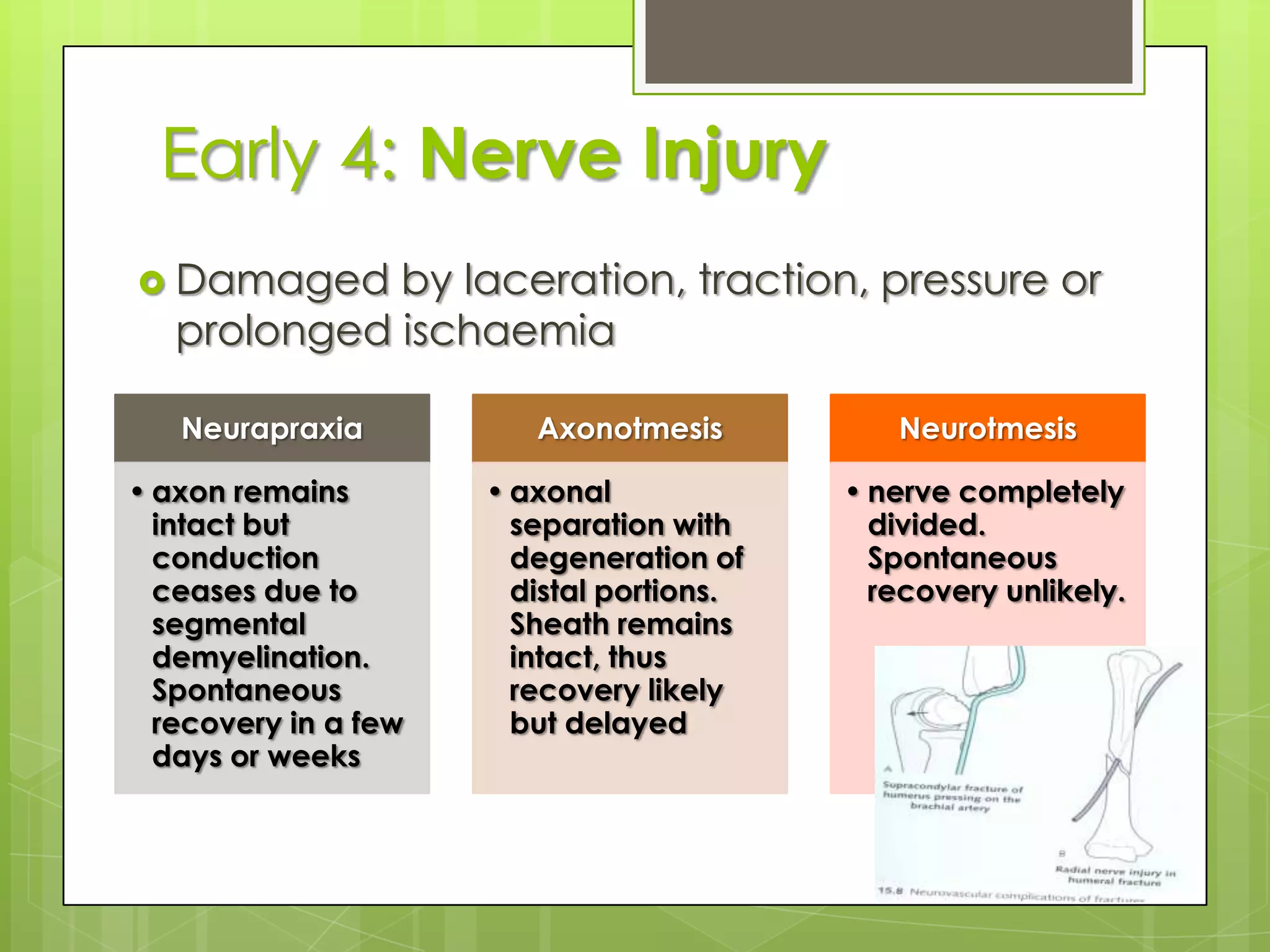
Nerve injuries associated with fractures, including assessment and treatment protocols.
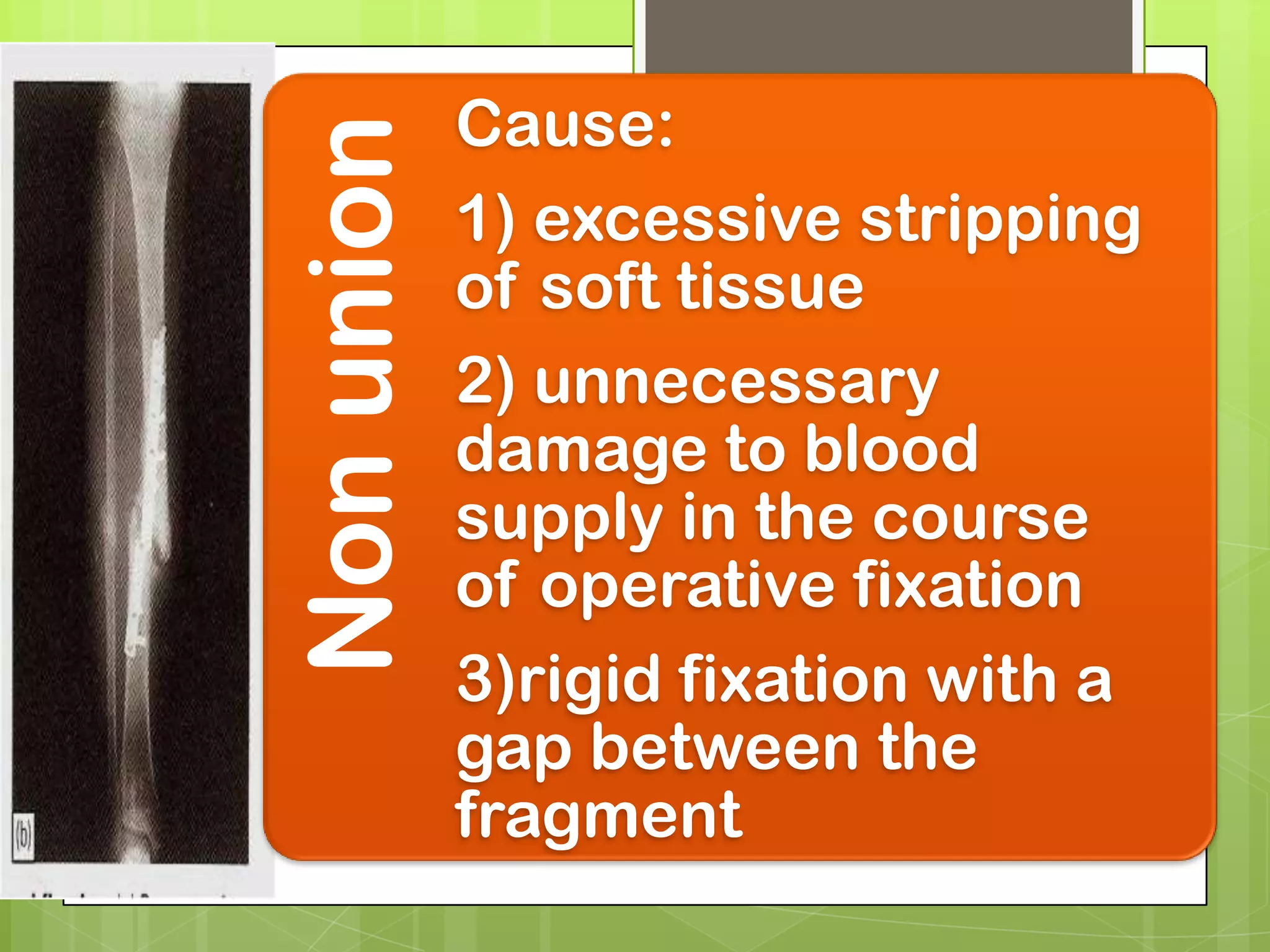
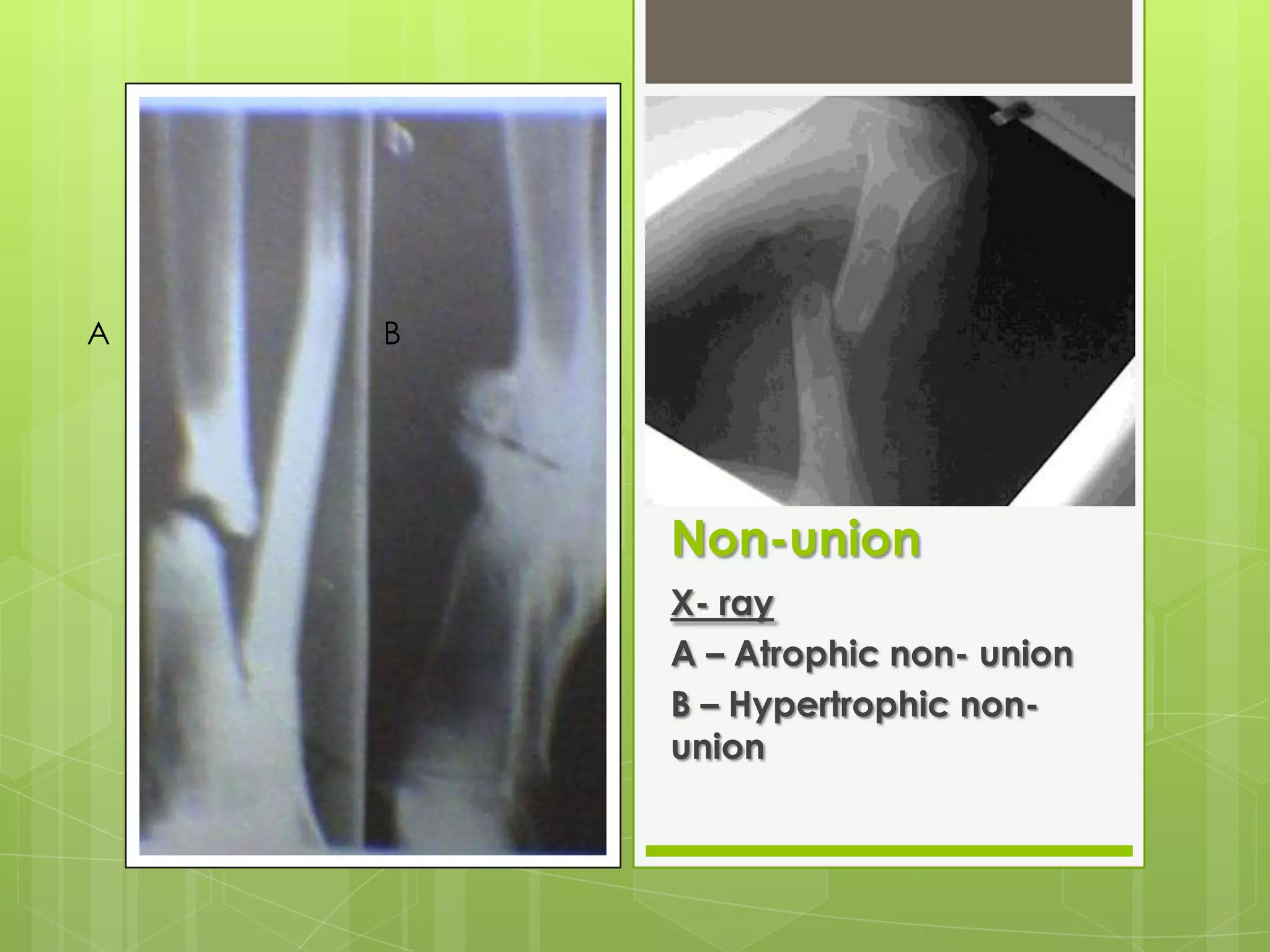
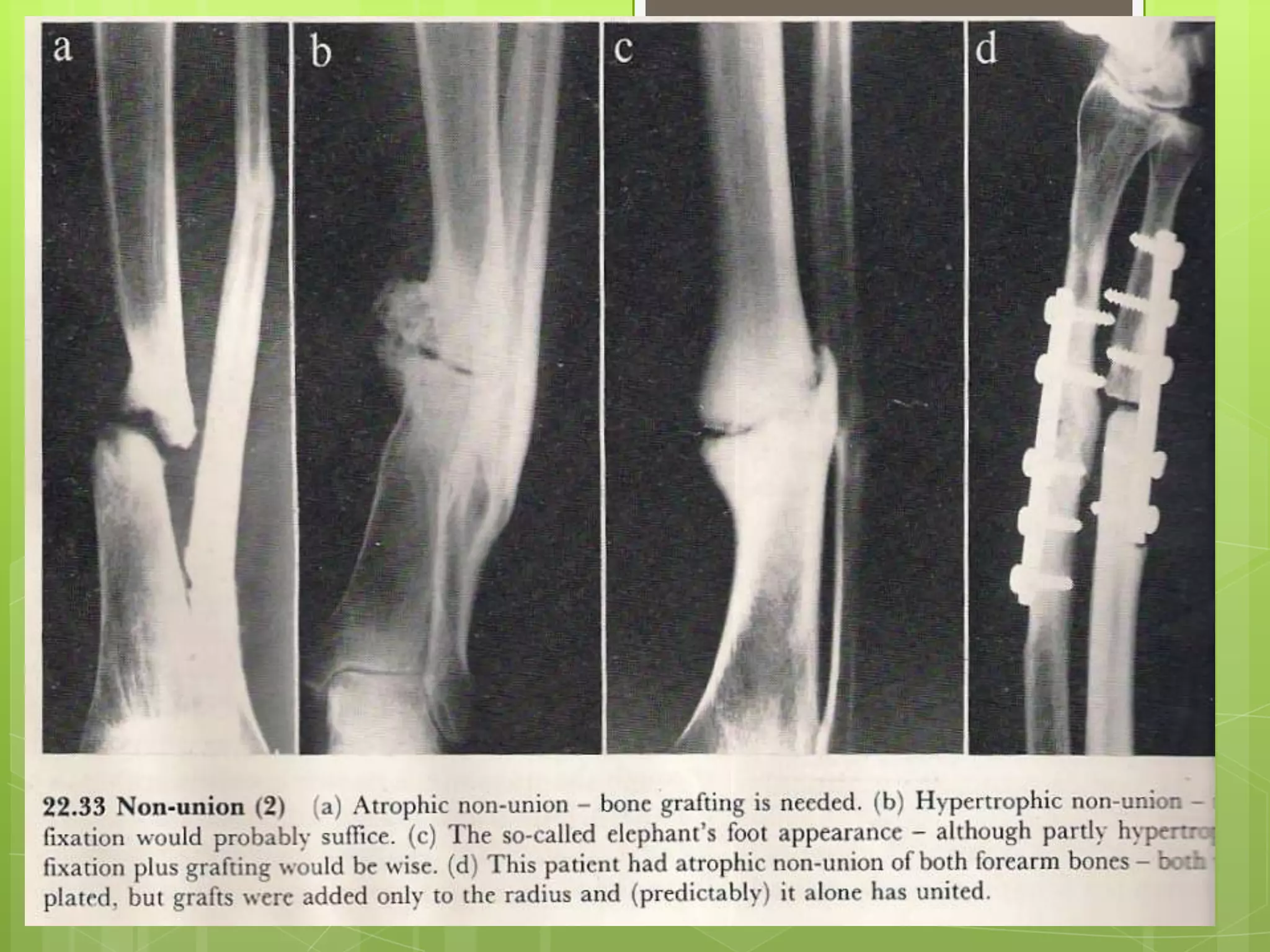
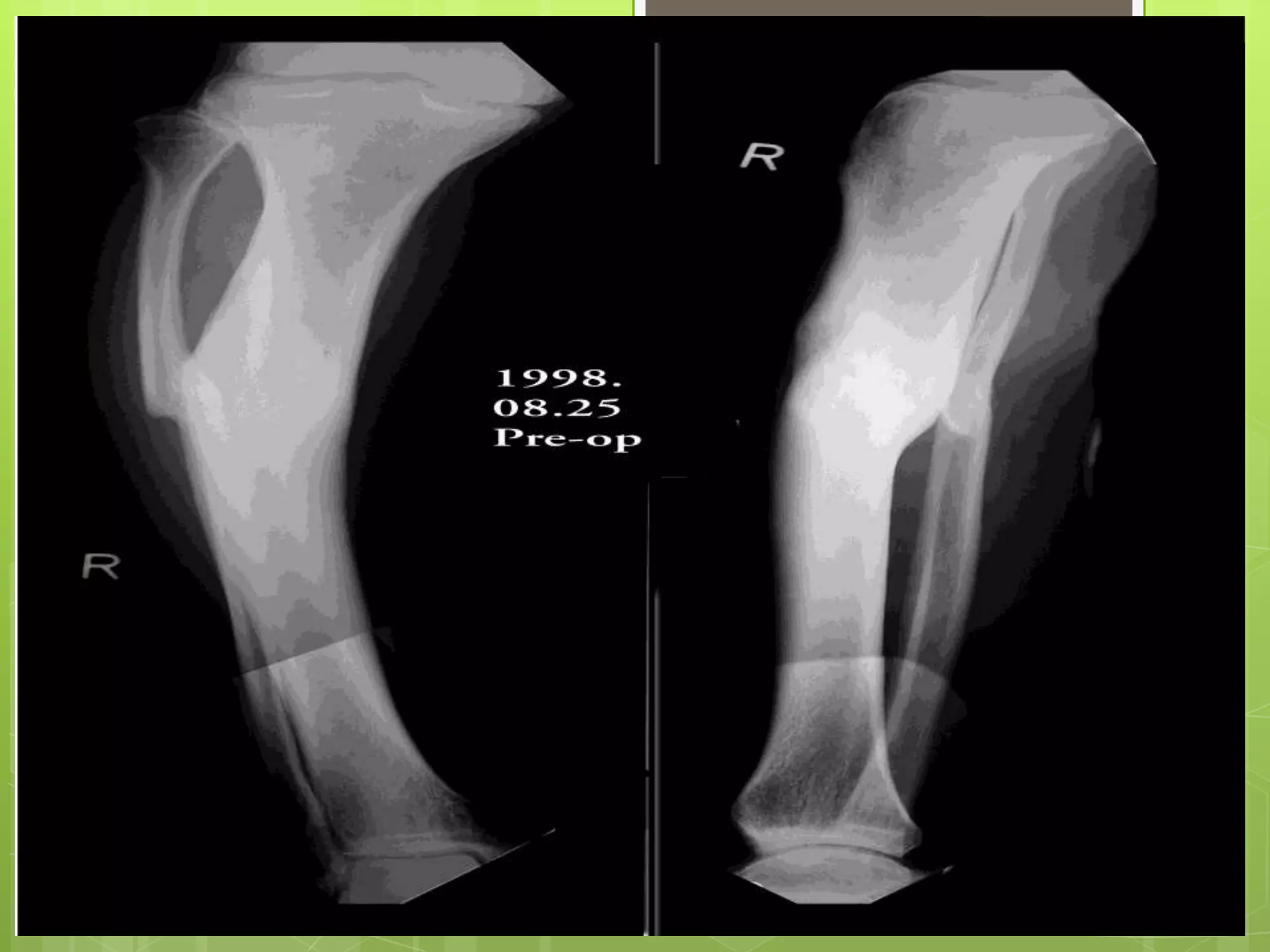
Discussion on delayed union, non-union, and mal-union in fracture healing.
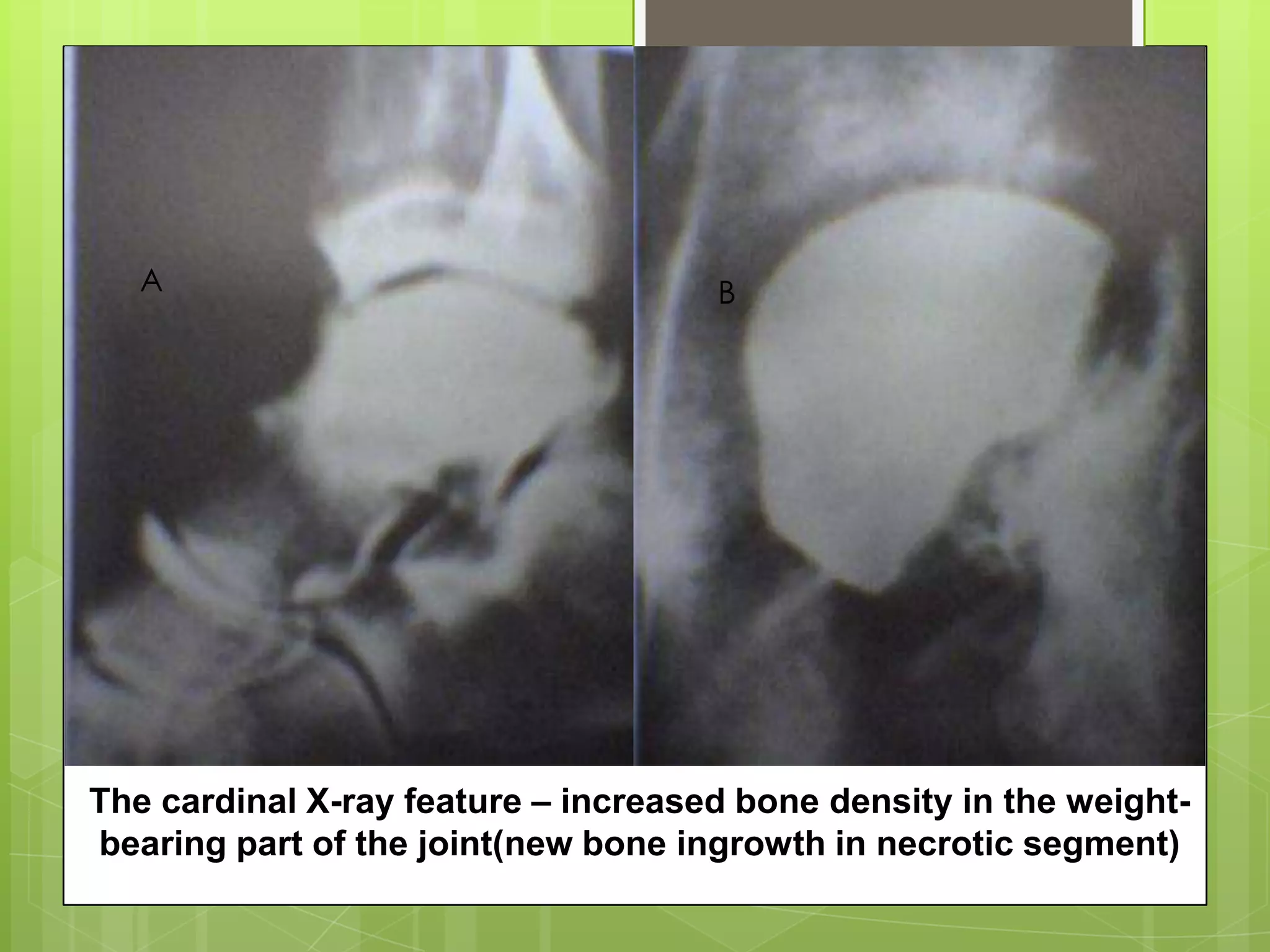
Consequences like avascular necrosis and osteoarthritis following fractures.
Common causes of joint stiffness after fractures and strategies for prevention.



































































![Mr. Kerengga [CPC]](https://cdn.slidesharecdn.com/ss_thumbnails/case1-110313121829-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



















