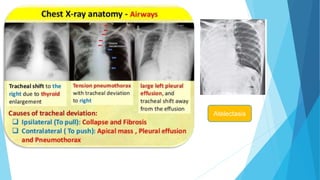
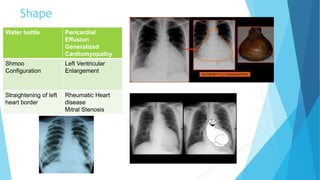
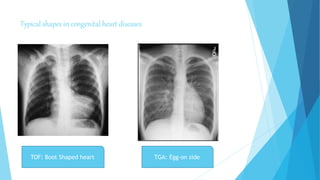
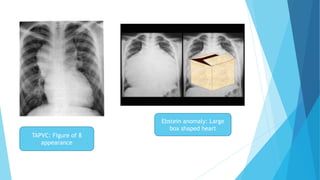
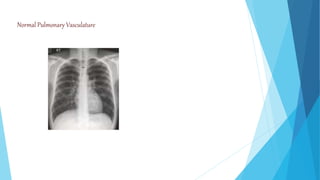
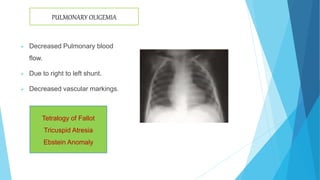
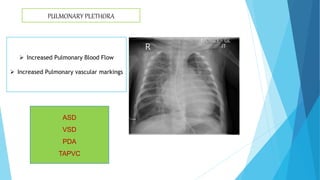
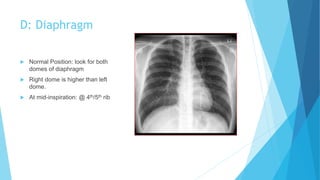
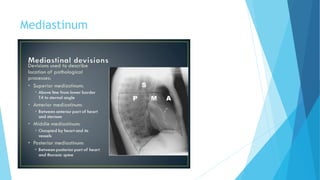
The document provides a comprehensive guide on chest X-ray interpretation authored by Dr. Manidipa Barman, covering key aspects such as patient details, imaging quality assessment, and a structured 'ABCDE' approach for interpretation. It details how to assess the airway, breathing, cardiac structures, diaphragm, and mediastinum, along with signs of various pulmonary and cardiac conditions. Additionally, it includes specific clinical indicators, conditions associated with radiographic findings, and references for further reading.






























































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)
















