
Recommended
Recommended
More Related Content
Similar to Impact of StakeholdersAs with any intervention, stakeholders mus
Similar to Impact of StakeholdersAs with any intervention, stakeholders mus (14)
More from MalikPinckney86
More from MalikPinckney86 (20)
Recently uploaded
Recently uploaded (20)
Impact of StakeholdersAs with any intervention, stakeholders mus
- 1. Impact of Stakeholders As with any intervention, stakeholders must be considered. For population health programs and interventions, the stakeholder group is large. If you are providing care to an individual patient, you may only consider the needs of the patient, family, and healthcare team. In population health, stakeholders may include the city, state, and national governments, along with the population and community impacted. In population health programs and interventions the goal is achieve the "greatest good for the greatest number" (Bentham, 1996). The focus of population health is broad and the needs of all stakeholders must be considered.Primary Prevention Primary prevention targets disease or disability prevention. These interventions focus on health promotion and address a universal population. Primary prevention interventions occur across settings, including healthcare organizations, school - based health clinics, complementary and alternative medicine (CAM) clinics, social media, as well as private homes (American Academy of Pediatrics, 2018). One example of a primary prevention intervention is a program to promote breastfeeding to reduce the occurrence of childhood obesity and comorbidities. Another example is vaccination programs to reduce the occurrence of infectious diseases.Secondary Prevention Secondary prevention focuses on identifying already occurring health problems or conditions prior to the onset of serious or long-term problems. These interventions address selected or targeted symptomatic populations. The objective of secondary prevention is early diagnosis and initial treatment or stabilization of disease in the early stages before it causes significant morbidity and mortality. These interventions can occur in all the some venues as primary interventions, as well as in emergency departments and retail-based clinics, such as Walgreen's (Moreland & Curran, 2018).Tertiary Prevention
- 2. Tertiary prevention aims to slow or stop the progression of disease. These interventions target individuals who are already diagnosed with a disease condition and work to restore function and reduce disease-related complications (Moreland & Curran, 2018). The third level of prevention is tertiary prevention, which is the act of managing a disease after diagnosis. Let's return to Kevin to see how this level of prevention relates to him. During Kevin's colonoscopy, the provider discovered polyps. The polyps were removed. And the pathology report reveals cancer. Tertiary prevention is the process of interventio n and treatment. It involves managing the disease post-diagnosis to slow or stop disease progression. Kevin's story illustrates an example of primary, secondary and tertiary prevention, including interventions for each level of prevention. Latest evidence suggests that therapeutic intervention strategies for Alzheimer's disease must be reconsidered as pathogenesis is now known to vary at different stages of the disease (Bu et al., 2016). What tertiary prevention intervention is helpful for the effective prevention and treatment of Alzheimer's disease? Preterm birth is a leading contributor of perinatal morbidity and mortality (Matei et al., 2019). What tertiary prevention intervention is needed to help reduce the occurrence of preterm birth?Population Health Interventions Population health interventions typically address one of the three levels of prevention and target the population as a whole. For example, an intervention may encompass individuals who are at risk for breast cancer, influenza, or impacted by a tornado. These interventions are not free. Funding plays a significant role in the creation and management of population health interventions, and health policy informs the type of interventions as well as the resource allocation.
- 3. After viewing “Lyft, Uber, and Sidecar” and the “EatWith” videos, predict the problems that will continue to plague innovators in the flexible workforce. Use at least two sources in addition to the text to support your position. Respond to at least two classmates’ posts. Course text: Weathington, B. L. & Weathington, J. G. (2020). Compensation and benefits: Aligning rewards with strategy, updated edition. Zovio. Eat with [Video segment]. (2014). In Reason TV, The sharing economy vs. the government . Retrieved from https://fod.infobase.com/OnDemandEmbed.aspx?token=93 730&wID=100753&loid=373417&plt=FOD&w=640&h=360&f Width=660&fHeight=410 Lyft, Uber and Sidecar [Video segment]. (2014). In Reason TV, The sharing economy vs. the government. Retrieved from https://fod.infobase.com/OnDemandEmbed.aspx?token=93730& wID=100753&loid=373417&plt=FOD&w=640&h=360&fWidth= 660&fHeight=410 Laws making workplaces, restaurants, and bars completely smoke-free can reduce heart attack hospitalizations by 8%–17% within a year.3,5,6 Federal laws that address U.S. air quality have contributed to a decrease of 54% of six common air pollutants since 1980.7 INTRODUCTION The health of the American public has improved on many fronts over the last decades—from decreasing incidence of lung cancer in
- 4. men to large reductions in the number of childhood lead poisoning cases. But as previous modules highlight, many diseases and illnesses are increasing in frequency. Though the reasons for these increases are often unknown, to the extent that the causes are recognized or suspected, preventive measures are desirable. Public health focuses on prevention of disease and health promotion rather than the diagnosis and treatment of diseases. WHAT IS PREVENTION? Prevention activities are typically categorized by the following three definitions: 1. Primary Prevention—intervening before health effects occur, through measures such as vaccinations, altering risky behaviors (poor eating habits, tobacco use), and banning substances known to be associated with a disease or health condition.8,9 2. Secondary Prevention—screening to identify diseases in the earliest stages, before the onset of signs and symptoms, through measures such as mammography and regular blood pressure testing.10 3. Tertiary Prevention—managing disease post diagnosis to slow or stop
- 5. disease progression through measures such as chemotherapy, rehabili- tation, and screening for complications.11 PREVENTION QUICK FACTS Actions such as the Clean Air Act as well as anti-smoking campaigns have had a significant preventive impact on public health.1,2,3 States play a crucial role in promoting both local and federal prevention efforts and also contrib- ute to prevention through their own initiatives.2,3 Beyond individual prevention efforts, local community actions can be particularly effective in bringing about changes that prevent or reduce environmentally-related illness and disease.4 PREVENTION PICTURE OF AMERICA2 3 Most prevention suggestions are primary or secondary prevention efforts for individuals. Yet, in the context of environmental health, prevention is much broader,
- 6. because exposure to many contaminants is beyond the control of individuals and historically has been most effectively reduced by government programs and regulations12 (e.g., Pollution Prevention Act13; Clean Air Act1). Traditionally, environmental public health has focused on reducing exposure to environ- mental hazards known to be related to disease. Increasing emphasis is placed on upstream inter- ventions—eliminating the source of the hazard rather than just preventing or reducing exposure.14 This type of elimination has often required action by individuals as well as governments at the federal, state, and local levels. THE PREVENTION FRAMEWORK LOCAL PREVENTION Beyond individual prevention efforts, local commu- nity actions can be particularly effective in bringing about changes that prevent or reduce environmen- tally-related illness and disease. Strategies ranging from community education to neighborhood aware- ness around an environmental health issue are some of the actions that can be taken at the local level. Zoning laws that provide incentives for the creation of bike paths or that reduce the number or density of liquor stores are actions taken by local govern- ments for the benefit of a community.15 Information sharing between neighborhood associations, faith communities, community-based organizations, and other local groups can highlight gaps in service and facilitate coordinated efforts to achieve public health outcomes. STATE PREVENTION States play an important role in promoting both local and federal prevention efforts and also contrib-
- 7. ute to prevention through their own initiatives. For example, inspections and regulation enforce- ment at food service establishments, swimming pools, hazardous waste disposal sites, and other locations help prevent illness and disease statewide. State-sponsored efforts support health screening programs, anti-smoking campaigns, and health education. As partners with federal agencies, states assist in implementation of programs such as the CDC’s Childhood Lead Poisoning Prevention Program and the CDC’s National Heart Disease and Stroke Prevention Program. Figure 1. The Spectrum of Prevention8 Influencing Policy and Legislation Mobilizing neighborhoods and communities Fostering coalitions and networks Changing internal practices and policies of agencies and institutions Educating healthcare providers and other professionals Promoting community education
- 8. Strengthening individual knowledge and skills PREVENTION 2 3 NATIONAL PREVENTION National prevention activities include initiatives, regulatory programs, and policies that establish nationwide programs to reduce both the presence of and exposure to harmful agents in the environ- ment (e.g., the Clean Water Act, National Tobacco Control Program, National Asthma Control Program). Many agencies are involved in activities that either directly or indirectly reduce public exposure. The Department of Health and Human Services, which includes the CDC and the U.S. Food and Drug Administration; the Environmental Protection Agency (EPA); the Department of Housing and Urban Development (HUD); and the Department of Agriculture (USDA) all have a hand in prevention efforts. KEY COMPONENTS OF PREVENTION16 Individual, local, state, and federal efforts to prevent environmentally-caused illness and disease have had some success, but a more comprehensive effort would be useful in meeting the overall environmental health challenges facing the United States. The following activities and initiatives can lead to understanding and reducing the nation’s incidence of environmentally- caused disease.
- 9. AWARENESS AND EDUCATION • Inform and educate decision-makers, public health practitioners, health care providers, and individuals about science-based health prevention approaches that will have the greatest benefit and impact on public health. • Provide information on effectiveness of interven- tions to inform policies. • Educate workers both in and out of the health field who may have daily contact with people at high risk for disease and injury. These individuals can encourage healthy behaviors, screen for certain health risks, and contribute to education of the community.17 • Provide the public with health education information. • Work with the media to highlight public health issues. PREVENTION PICTURE OF AMERICA4 5 • Establish programs to proactively distribute informa- tion to targeted groups—those at high risk for disease or injury. Research • Identify and support an environmental public health research agenda at the national level. This research would address knowledge gaps in suspected and emerging links between exposure to harmful environ- mental agents and health outcomes.
- 10. Surveillance at all levels • Monitor environmental risk areas or situations and determine the prevalence of environmentally-linked health outcomes. Identify national, state, or commu- nity environmental health issues; develop measures to track those issues; and implement widespread surveillance to help identify relationships between environmental hazards and health concerns. Hazard evaluation at the national, state, and local levels • Implement hazard assessments as needed. Respond to high-risk situations, identify and quantify hazard- ous agents, and facilitate exposure reduction. Improvement of the public health system at the national, state, and local levels • Enhance and revitalize the environmental health system at all levels. Build and improve long-term strategic partnerships, commitments by all stakeholders, and additional resources, as well as collaboration with environmental regulatory agencies and development of a competent and effective environmental public health workforce.16 Proactive behavior by individuals • Make healthy lifestyle choices, choose environmental - ly-friendly products and services, and conscientiously try to minimize the environmental impact of yourself and your family. Become informed about the issues, and be proactive in prevention initiatives promoting
- 11. health and preventing illness and disease. PREVENTION 4 5 THE NATIONAL ENVIRONMENTAL PUBLIC HEALTH TRACKING NETWORK Many of the above activities are dependent on the availability of information to link diseases and environmental exposures. Laboratory studies contribute to our understanding, but without coordinated tracking of environmental hazards, exposures, and diseases, the picture is often fragmented and inconclusive. The CDC has responded to this need with the National Environ- mental Public Health Tracking Network.18 This Network has established information-system standards to facilitate integration of local, state, and national databases of environmental hazards, environmental exposures, and health effects. These data allow federal, state, and local agencies, among others, to monitor and distribute informa- tion about environmental hazards and disease trends. As trends and linkage between environmen- tal hazards and disease are uncovered, preventive actions can be taken to protect communities. SUCCESSFUL PREVENTION INITIATIVES Actions such as the Clean Air Act as well as anti- smoking campaigns have achieved a significant preventive impact on public health.1,2,3 The following success stories demonstrate how these initiatives relate to the advancement of environmental public health. CLEAN AIR PREVENTION INITIATIVES
- 12. One of the most substantial environmental pollution success stories has been the reduction in levels of air pollutants throughout the United States (see Outdoor Air Quality chapter). While national air quality has improved since the early 1990s, air quality problems still exist, presenting many challenges in protecting public health and the environment. Air pollution is a major problem that can affect every- one.19 Studies show links between air pollution and a number of health problems, such as an increased risk for heart attacks, and it can affect individuals with asthma and other lung conditions. Children and the elderly are often the most vulnerable to the effects of air pollution.20 1955 The Air Pollution Act of 1955 provides federal research funds for studying air pollution. 1963 The Clear Air Act of 1963 establishes a federal program authorizing research for ways to monitor and control pollution. 1967 The Air Quality Act of 1967 expands the federal government’s activities to begin enforcing areas subject to interstate pollution transport and conducting ambient air monitoring studies and industrial source inspections. 1970 The Clean Air Act of 1970 brings about a major shift in the government’s role in controlling air pollution. Comprehensive federal and state regulations are developed to reduce emissions from industrial and mobile sources. 1970 The U.S. Environmental Protection Agency (EPA) is
- 13. established to implement the require- ments of the 1970 Clean Air Act. 1977 and 1990 Major amendments are added to the 1970 Clean Air Act ensuring continuation of the Air Quality Standards, increasing the federal government’s air quality authority and responsibili- ties, and establishing new programs for acid rain and toxic air pollutants.19 Figure 2. Timeline of Key Federal Clean Air Initiatives PREVENTION PICTURE OF AMERICA6 7 Figure 2 provides a timeline that illustrates key fed- eral initiatives designed and implemented to reduce air pollution and related illnesses across the nation. The EPA has set national outdoor air quality stan- dards for the following six common air pollutants: • Particulate matter (PM) • Ozone (O3) • Carbon monoxide (CO) • Nitrogen dioxide (NO2) • Sulfur dioxide (SO2) • Lead (Pb) EPA monitors outdoor air quality concentrations of these pollutants and produces estimates of emis- sions based on monitored data plus calculations
- 14. of pollutants emitted by vehicles, factories, and other sources. EPA air quality trends show that air quality has improved nationally since 1980.7 Between 1980– 2007, while increases were seen in the gross domestic product, the number of vehicle miles traveled, over- all energy consumption, and the U.S. population, total emissions of these six common air pollutants decreased by 52%.7 Other significant improvements since 1970 include a 70% reduction of air toxics from large industrial sources, new cars that are more than 90% cleaner, and the end of the production of most ozone-depleting chemicals.20 The CDC Air Pollution and Respiratory Health Branch in the National Center for Environmental Health works to prevent environmentally-related respiratory illnesses and studies indoor and outdoor air pollution. This CDC program collects and analyzes respiratory health data, implements asthma interven- tions to ensure scientific information is translated into public health practice, establishes and maintains partnerships to control asthma, works to prevent car- bon monoxide poisoning, and studies the effects of forest fire smoke and other airborne contaminants.21 WHAT YOU CAN DO In addition to national legislation and programs regarding clean air, individuals can also take a proac- tive approach to reduce air pollution as well as their exposure to harmful air pollutants.20 Practice energy conservation – using less energy and recycling reduces air pollution generated by power generating and manufacturing facilities. • Recycle paper, plastic, glass bottles, cardboard,
- 15. and aluminum cans. • Conserve energy by turning off appliances and lights when not in use. • Buy ENERGY STAR products, such as energy- efficient lighting and appliances. • Connect outdoor lights to a timer or use solar lighting to reduce your use of electricity. • Use rechargeable batteries. • Lower the thermostat on the water heater to 120°F. Reduce your consumption of fossil fuels by driving less or using more efficient vehicles designed to burn less gasoline and oil. • Choose efficient, low-polluting vehicles. • Plan trips; save gasoline and reduce air pollution. • Keep tires properly inflated and aligned and get regular engine tune-ups and car maintenance to increase your fuel efficiency. • During summer, fill the gas tank during cooler evening hours to decrease evaporation and reduce the formation of ozone. • Avoid waiting in long drive-through lines; park your car and go in. • Use public transportation, walk, or ride a bike. • Join a carpool or vanpool to get to work.
- 16. Reduce your personal exposure to air pollutants. • Use low volatile organic compounds (VOC) or water-based paints, stains, finishes, and paint strippers. • Choose not to smoke inside the home; ask visitors to smoke outside. • Keep woodstoves and fireplaces well maintained. • Test the home for radon. • Avoid spilling gas; do not top off the tank and replace gas cap tightly. • Check daily air quality forecasts and associated health concerns. PREVENTION 6 7 SECONDHAND SMOKE PREVENTION INITIATIVES Secondhand smoke, also called environmental tobacco smoke (ETS), is the mixture of gases and particles given off by burning cigarettes, pipes, and cigars as well as the smoke exhaled by smokers.22 Breathing secondhand smoke, even in small amounts, is dangerous to human health and can cause lung cancer and an increased risk of heart disease, including heart attack, in adult nonsmokers22 (see Secondhand Smoke section in Homes chapter). Laws and policies for smoke-free environments have been initiated at the national, state, and
- 17. local levels. Nationally, several laws and policies restricting smoking in public places have been adopted.23 Federal law prohibits smoking on domestic airline flights and interstate buses. Smoking is also banned in most federally-owned buildings, and the Pro-Children Act of 1994 prohibits smoking in buildings where federally- funded services are provided to children.24 While these federal smoking restrictions are important, the most comprehensive smoke-free laws have originated at the local level. Local initia- tives engage communities in public education, raise awareness of the health risks of secondhand smoke, and increase public awareness of policies that provide protection from exposure risks.25 As increasing numbers of communities successfully implemented comprehensive laws making work- places, restaurants, and bars completely smoke-free, states began enacting similarly comprehensive laws.25 The first state laws restricting smoking in public places were passed in Arizona, Connecticut, and Minnesota between 1973–1975.26 Over the years a number of other states enacted limited smoking restrictions. In the 1990s, California became the first state to restrict smoking in most indoor work- places and places, including restaurants and bars.25 From 2002–2005, Delaware, New York, Massachu- setts, Rhode Island, and Washington state imple- mented comprehensive state smoke-free laws.25 By April of 2014, 24 states and the District of Columbia had comprehensive laws in effect requiring all private workplaces, restaurants, and bars to be smoke-free.27 According to the American Nonsmokers’ Rights Foundation, over 49%
- 18. of Americans live under comprehensive state In a 2006 report, the U.S. Surgeon General reached the following conclusions regarding control of secondhand smoke exposure:25 • The scientific evidence indicates that there is no risk-free level of exposure to second- hand smoke. • Only eliminating smoking in indoor spaces fully protects nonsmokers from secondhand smoke exposure; separating smokers from nonsmokers, cleaning the air, and ventilat- ing buildings cannot completely eliminate exposure. • Workplace smoking restrictions are effective in reducing secondhand smoke exposure and lead to less smoking among covered workers. • Establishing smoke-free workplaces is the only way to ensure secondhand smoke exposure does not occur in the workplace. • The majority of workers in the United States are covered by smoke-free policies. • Evidence from peer-reviewed studies shows that smoke-free policies do not have an adverse economic impact on the hospitality industry. PREVENTION PICTURE OF AMERICA8 9
- 19. or local smoke-free laws.27 The prevalence of U.S. nonsmokers’ exposure to secondhand smoke dropped by half between 1988–1991, when most Americans were exposed, and 2007–2008. This decline was likely driven in large part by the widespread adoption of state and local laws and voluntary business policies prohibiting smoking in indoor workplaces and public places.25 A number of studies conducted in a range of com- munities, states, regions, and countries have reported substantial and rapid reductions in heart attack hospitalizations following the implementation of smoke-free laws.28 In 2010, the Institute of Medi- cine, after reviewing these studies and related evidence, concluded that smoke-free laws reduce heart attacks.28 In addition, three meta-analyses of studies on this topic have estimated pooled effect sizes of 8%,3 10%,5 and 17%.6 WHAT YOU CAN DO There are steps individuals can take to protect themselves and their family from exposure to secondhand smoke25: • Make the home and car smoke-free. • Visit smoke-free restaurants and public places. • Ask people not to smoke around you and your children. • Use a smoke-free daycare center. CONTINUED PREVENTION SUCCESS Clean air and secondhand smoke prevention are just two examples of the many successes that have
- 20. occurred through the use of proactive preventive measures. Many more success stories will emerge as individuals, communities, and other stakeholders take on a more active role in environmental public health. PREVENTION 8 9 1. EPA. The Clean Air Act: Protecting human health and the environ- ment since 1970 as the U.S. economy has grown [online]. 2012. [cited 2013 May 8]. Available from URL: http://www.epa.gov/air/ sect812/economy.html. 2. CDC. State smoke-free laws for worksites, restaurants, and bars— United States, 2000—2010. MMWR 2011;60(15):472–5. 3. Meyers DG, Neuberger JS, He J. Cardiovascular effect of bans on smoking in public places. J Am Coll Cardiol 2009;54:1249– 55. 4. Institute of Medicine. The community. In:The Future of the Public’s Health in the 21st Century. Washington (D.C.): The National Academies Press, 2003. 5. Mackay DF, Irfan MO, Haw S, Pell JP. Meta-analysis of the effect of comprehensive smoke-free legislation on acute coronary events. Heart 2010;96(19):1525–30.
- 21. 6. Lightwood JM, Glantz SA. Declines in acute myocardial infarction after smoke-free laws and individual risk attributable to secondhand smoke Circulation 2009;120:1373–9. 7. EPA. Air trends. Basic information [online]. 2008 May 8. [cited 2010 Apr 13]. Available from URL: http://www.epa.gov/air/airtrends/ sixpoll.html. 8. Wallace RB. Primary prevention. In: Breslow L, Cengage G, editors. Encyclopedia of Public Health [online]. 2006. [cited 2010 Mar 30]. Available from URL: http://www.enotes.com/public- health- encyclopedia/primary-prevention. 9. Canadian Association of Physicians for the Environment. Primary prevention. Children’s Environmental Health Project [online]. 2000. [cited 2010 Mar 30]. Available from URL: http://www.cape.ca/ children/prev.html. 10. Wallace RB. Secondary prevention. In: Breslow L, Cengage G, editors Encyclopedia of Public Health [online]. 2006. [cited 2010 Mar 30]. Available from URL: http://www.enotes.com/public- health- encyclopedia/secondary-prevention. 11. Wallace RB. Tertiary prevention. In: Breslow L Cengage G, editors.
- 22. Encyclopedia of Public Health [online]. 2006. [cited 2010 Mar 30]. Available from URL: http://www.enotes.com/public-health- encyclo- pedia/tertiary-prevention. 12. EPA. Pollution Prevention Laws and Policy [online].2012 Feb 16.[cited 2013 May 8]. Available from URL: http://www.epa.gov/p2/ pubs/laws.htm. 13. Pollution Prevention Act of 1990, Pub. L. No. 101–508, 104 Stat. 1388–321 et seq (As Amended Through P.L. 107–377, December 31, 2002) [online]. 2002. [cited ]. Available from URL: http://www. epw.senate.gov/PPA90.pdf. 14. Cohen L, Chehemi S, Chavez V, editors. Prevention is primary: Strategies for community well-being. San Francisco (CA): Jossey- Bass; 2007. 15. Frieden, T. Government’s role in protecting health and safety. N Engl J Med 2013;368:1857–1859. 16. CDC. A national strategy to revitalize environmental public health services [online]. 2003. [cited 2010 Mar 31]. Available from URL: http://www.cdc.gov/nceh/ehs/Docs/nationalstrategy2003.pdf.
- 23. 17. Rattray T, Brunner W, Freestone J. The new spectrum of prevention: a model for public health practice.Contra Costa Health Services [online] 2002 Apr [cited 2010 Mar 30]. Available from URL: http:// www.cchealth.org/topics/prevention/pdf/new_spectrum_of_ prevention.pdf. 18. CDC. National Environmental Public Health Tracking Program. Background [online]. 2009 July 13. [cited 2010 Mar 31]. Available from URL: http://www.cdc.gov/nceh/tracking/background.htm. 19. EPA History of the Clean Air Act [online]. 2008 Jul 7. [cited 2010 Apr13]. Available from URL: http://www.epa.gov/air/caa/caa_ history.html. 20. EPA. The plain English guide to the Clean Air Act [online]. 2007. [cited 2010 Apr 13]. Available from URL: http://www.epa.gov/air/ caa/peg/peg.pdf. 21. CDC. Air pollution and respiratory health [online]. 2009 May. [cited 2010 Apr 14]. Available from URL: http://www.cdc.gov/nceh/ airpollution/about.htm. 22. EPA. Smoke-free homes and cars program. Health effects of expo- sure to secondhand smoke [online]. 2008 Feb 29. [cited 2010 Apr 14]. Available from URL: http://www.epa.gov/smokefree/health
- 24. effects.html. 23. CDC Smoking and Tobacco Use, Secondhand Smoke (SHS) Facts [online]. 2013 Jun 10. [cited http://www.cdc.gov/tobacco/data_ statistics/fact_sheets/secondhand_smoke/general_facts/index.ht m. 24. National Cancer Institute. Fact sheet: Secondhand smoke: questions and answers [online]. 2007 Aug 01.[cited 2010 Apr14]. Available from URL: http://www.cancer.gov/cancertopics/factsheet/ Tobacco/ETS. 25. CDC. The health consequences of involuntary exposure to tobacco smoke: a report of the Surgeon General. Secondhand smoke what it means to you [online].2006. [cited 2010 Apr 14]. Available from URL: http://www.surgeongeneral.gov/library/secondhandsmoke/ secondhandsmoke.pdf. 26. DHHS. Reducing the Health Consequences of Smoking: 25 Years of Progress. A Report of the Surgeon General. DHHS Publication No. (CDC) 89-8411 [online]. 1989. [Accessed 13 May 2013]. Available from URL: http://profiles.nlm.nih.gov/ps/access/NNBBXS. pdf. 27. American Nonsmokers’ Rights Foundation. Summary of 100% smokefree state laws and population protected by 100% U.S.
- 25. smokefree laws [online]. July 3, 2014 [cited 2014 Jul 8]. Available from URL: http://www.no- smoke.org/pdf/SummaryUSPopList.pdf. 28. Institute of Medicine. Secondhand smoke exposure and cardiovas- cular effects: making sense of the evidence. Washington (D.C.): The National Academies Press, 2010. REFERENCES http://www.epa.gov/air/sect812/economy.html http://www.epa.gov/air/sect812/economy.html http://www.epa.gov/air/airtrends/ sixpoll.html http://www.epa.gov/air/airtrends/ sixpoll.html http://www.enotes.com/public-health- encyclopedia/primary- prevention http://www.enotes.com/public-health- encyclopedia/primary- prevention http://www.cape.ca/children/prev.html http://www.cape.ca/children/prev.html http://www.enotes.com/public-health-encyclopedia/secondary- prevention http://www.enotes.com/public-health-encyclopedia/secondary- prevention http://www.enotes.com/public-health-encyclopedia/tertiary- prevention http://www.enotes.com/public-health-encyclopedia/tertiary- prevention http://www.epa.gov/p2/pubs/laws.htm http://www.epa.gov/p2/pubs/laws.htm http://www.epw.senate.gov/PPA90.pdf http://www.epw.senate.gov/PPA90.pdf http://www.cdc.gov/nceh/ehs/Docs/nationalstrategy2003.pdf http://www.cchealth.org/topics/prevention/pdf/new_spectrum_of
- 26. _ prevention.pdf http://www.cchealth.org/topics/prevention/pdf/new_spectrum_of _ prevention.pdf http://www.cchealth.org/topics/prevention/pdf/new_spectrum_of _ prevention.pdf http://www.cdc.gov/nceh/tracking/background.htm http://www.epa.gov/air/caa/caa_ history.html http://www.epa.gov/air/caa/caa_ history.html http://www.epa.gov/air/caa/peg/peg.pdf http://www.epa.gov/air/caa/peg/peg.pdf http://www.cdc.gov/nceh/airpollution/about.htm http://www.cdc.gov/nceh/airpollution/about.htm http://www.epa.gov/smokefree/health effects.html http://www.epa.gov/smokefree/health effects.html http://www.cdc.gov/tobacco/data_ statistics/fact_sheets/secondhand_smoke/general_facts/index.ht m http://www.cdc.gov/tobacco/data_ statistics/fact_sheets/secondhand_smoke/general_facts/index.ht m http://www.cancer.gov/cancertopics/factsheet/Tobacco/ETS http://www.cancer.gov/cancertopics/factsheet/Tobacco/ETS http://www.surgeongeneral.gov/library/secondhandsmoke/secon dhandsmoke.pdf http://www.surgeongeneral.gov/library/secondhandsmoke/secon dhandsmoke.pdf http://profiles.nlm.nih.gov/ps/access/NNBBXS.pdf http://profiles.nlm.nih.gov/ps/access/NNBBXS.pdf http://www.no-smoke.org/pdf/SummaryUSPopList.pdf PU36CH31-Kolodny ARI 11 February 2015 9:9 The Prescription Opioid and Heroin Crisis: A Public
- 27. Health Approach to an Epidemic of Addiction Andrew Kolodny,1,2,3 David T. Courtwright,4 Catherine S. Hwang,5,6 Peter Kreiner,1 John L. Eadie,1 Thomas W. Clark,1 and G. Caleb Alexander5,6,7 1 Heller School for Social Policy and Management, Brandeis University, Waltham, Massachusetts 02454; email: [email protected], [email protected], [email protected], [email protected] 2 Phoenix House Foundation, New York, NY 10023 3 Global Institute of Public Health, New York University, New York, NY 10003 4 Department of History, University of North Florida, Jacksonville, Florida 32224; email: [email protected] 5 Center for Drug Safety and Effectiveness, 6 Department of Epidemiology, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland 21205; email: [email protected] 7 Division of General Internal Medicine, Department of Medicine, Johns Hopkins Medicine, Baltimore, Maryland 21205; email: [email protected] Annu. Rev. Public Health 2015. 36:559–74 First published online as a Review in Advance on January 12, 2015 The Annual Review of Public Health is online at publhealth.annualreviews.org This article’s doi: 10.1146/annurev-publhealth-031914-122957
- 28. Copyright c© 2015 by Annual Reviews. All rights reserved Keywords prescription drug abuse, heroin, overdose deaths, chronic pain, opioid, addiction Abstract Public health authorities have described, with growing alarm, an unprece- dented increase in morbidity and mortality associated with use of opioid pain relievers (OPRs). Efforts to address the opioid crisis have focused mainly on reducing nonmedical OPR use. Too often overlooked, however, is the need for preventing and treating opioid addiction, which occurs in both medical and nonmedical OPR users. Overprescribing of OPRs has led to a sharp increase in the prevalence of opioid addiction, which in turn has been asso- ciated with a rise in overdose deaths and heroin use. A multifaceted public health approach that utilizes primary, secondary, and tertiary opioid addic- tion prevention strategies is required to effectively reduce opioid-related morbidity and mortality. We describe the scope of this public health crisis, its historical context, contributing factors, and lines of evidence indicating
- 29. the role of addiction in exacerbating morbidity and mortality, and we provide a framework for interventions to address the epidemic of opioid addiction. 559 A nn u. R ev . P ub li c H ea lt h 20 15 .3 6: 55 9- 57
- 32. :a 89 o n 05 /2 2/ 21 . F or p er so na l us e on ly . PU36CH31-Kolodny ARI 11 February 2015 9:9 INTRODUCTION
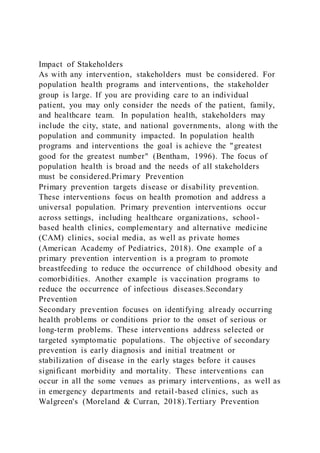
- 33. Over the past 15 years, the rate of opioid pain reliever (OPR) use in the United States has soared. From 1999 to 2011, consumption of hydrocodone more than doubled and consumption of oxycodone increased by nearly 500% (42). During the same time frame, the OPR-related overdose death rate nearly quadrupled (15). According to the United States Centers for Disease Control and Prevention (CDC), the unprecedented increase in OPR consumption has led to the “worst drug overdose epidemic in [US] history” (58). Given the magnitude of the problem, in 2014 the CDC added opioid overdose prevention to its list of top five public health challenges (13). Overdose mortality is not the only adverse public health outcome associated with increased OPR use. The rise in opioid consumption has also been associated with a sharp increase in emergency room visits for nonmedical OPR use (69) and in neonatal abstinence syndrome (57). Moreover, from 1997 to 2011, there was a 900% increase in individuals seeking treatment for addiction to OPRs (66, 68). The correlation between opioid sales, OPR-related overdose deaths, and treatment seeking for opioid addiction is striking (Figure 1). Addiction is defined as continued use of a drug despite negative consequences (1). Opioids are highly addictive because they induce euphoria (positive reinforcement) and cessation of chronic use produces dysphoria (negative reinforcement). Chronic exposure to opioids results in structural and functional changes in regions of the brain that mediate
- 34. affect, impulse, reward, and motivation (83, 91). The disease of opioid addiction arises from repeated exposure to opioids and can occur in individuals using opioids to relieve pain and in nonmedical users. Another important feature of the opioid addiction epidemic is the relationship between OPR use and heroin use. According to the federal government’s National Survey on Drug Use and Health (NSDUH), 4 out of 5 current heroin users report that their opioid use began with OPRs (54). Many of these individuals appear to be switching to heroin after becoming addicted to OPRs because heroin is less expensive on the black market. For example, in a recent sample of 0 1 2 3 4 5 6 7 8 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
- 35. 2010 R at e Year Opioid sales kg/10,000 Opioid deaths/100,000 Opioid treatment admissions/10,000 Figure 1 Rates of OPR sales, OPR-related unintentional overdose deaths, and OPR addiction treatment admissions, 1999–2010. Abbreviation: OPR, opioid pain reliever. Source: 10. 560 Kolodny et al. A nn u. R ev . P ub li c H
- 39. l us e on ly . PU36CH31-Kolodny ARI 11 February 2015 9:9 Non-Hispanic white Non-Hispanic black 50 40 30 20 10 0 Pe rc en t o f a ll
- 40. h er o in a d m is si o n s ag ed 1 2 an d o ve r 2001 2003 2005 2007 2009 2011 2001 2003 2005 2007 2009 2011 12–19 years
- 41. 20–34 years 35–44 years 45 years or older Year Figure 2 Heroin admissions, by age group and race/ethnicity: 2001–2011. Source: 68. opioid-addicted individuals who switched from OPRs to heroin, 94% reported doing so because OPRs “were far more expensive and harder to obtain” (16, p. 24). The increased prevalence of opioid addiction has also been associated with increases in heroin- related morbidity and mortality. For example, since 2001, heroin addiction treatment admissions for whites ages 20–34 have increased sharply (Figure 2). During this time frame, heroin overdose deaths among whites ages 18–44 increased by 171% (14). HISTORY OF OPIOID ADDICTION IN THE UNITED STATES The current opioid addiction crisis is, in many ways, a replay of history. America’s first epidemic of opioid addiction occurred in the second half of the nineteenth century. In the 1840s, the estimated national supply of opium and morphine could have supported a maximum of 0.72 opioid-addicted individuals per 1,000 persons (18). Over the next 50 years, opioid consumption soared by 538%.
- 42. It reached its peak in the mid-1890s, when the supply could have supported a maximum of ∼4.59 opioid-addicted individuals per 1,000 persons. The ceiling rate then began to decline, and by 1920 there were no more than 1.97 opioid-addicted individuals per 1,000 persons in the United States. The epidemic had diverse origins. Mothers dosed themselves and their children with opium tinctures and patent medicines. Soldiers used opium and morphine to treat diarrhea and painful injuries. Drinkers alleviated hangovers with opioids. Chinese immigrants smoked opium, a practice that spread to the white underworld. But the main source of the epidemic was iatrogenic morphine addiction, which coincided with the spread of hypodermic medication during 1870–1895. The model opioid-addicted individual was a native-born white woman with a painful disorder, often of a chronic nature. Nineteenth-century physicians addicted patients—and, not infrequently, themselves—because they had few alternatives to symptomatic treatment. Cures were scarce and the etiology of painful conditions was poorly understood. An injection of morphine almost magically alleviated symptoms, pleasing doctors and patients. Many patients continued to acquire and inject morphine, the sale of which was poorly controlled. The revolutions in bacteriology and public health, which reduced diarrheal and other diseases commonly treated with opium; the development of alternative analgesics such as aspirin; stricter
- 43. www.annualreviews.org • The Opioid Addiction Epidemic 561 A nn u. R ev . P ub li c H ea lt h 20 15 .3 6: 55 9- 57 4. D ow
- 46. n 05 /2 2/ 21 . F or p er so na l us e on ly . PU36CH31-Kolodny ARI 11 February 2015 9:9 prescription laws; and admonitions about morphine in the lay and professional literature stemmed the addiction tide. One important lesson of the first narcotic epidemic is that physicians were educable. Indeed, by 1919, narcotic overprescribing was the hallmark of older, less-competent
- 47. physicians. The younger, better-trained practitioners who replaced them were more circumspect about administering and prescribing opioids (5). For the rest of the twentieth century, opioid addiction epidemics resulted from transient in- creases in the incidence of nonmedical heroin use in urban areas. After World War II, these epidemics disproportionately affected inner-city minority populations, such as the large, heavily publicized increase in ghetto heroin use and addiction at the end of the 1960s (24, 37). THE SHARP RISE IN PRESCRIPTION OPIOID CONSUMPTION In 1986 a paper describing the treatment of 38 chronic pain patients concluded that OPRs could be prescribed safely on a long-term basis (61). Despite its low- quality evidence, the paper was widely cited to support expanded use of opioids for chronic non-cancer pain. Opioid use increased gradually in the 1980s. In 1996, the rate of opioid use began accelerating rapidly (38). This acceleration was fueled in large part by the introduction in 1995 of OxyContin, an extended release formulation of oxycodone manufactured by Purdue Pharma. Between 1996 and 2002, Purdue Pharma funded more than 20,000 pain-related educational programs through direct sponsorship or financial grants and launched a multifaceted campaign to encourage long-term use of OPRs for chronic non-cancer pain (86). As part of this campaign, Purdue provided financial support to the American Pain Society,
- 48. the American Academy of Pain Medicine, the Federation of State Medical Boards, the Joint Commission, pain patient groups, and other organizations (27). In turn, these groups all advocated for more aggressive identification and treatment of pain, especially use of OPRs. For example, in 1995, the president of the American Pain Society introduced a campaign en- titled “Pain is the Fifth Vital Sign” at the society’s annual meeting. This campaign encouraged health care professionals to assess pain with the “same zeal” as they do with vital signs and urged more aggressive use of opioids for chronic non-cancer pain (9). Shortly thereafter, the Veterans’ Affairs health system, as well as the Joint Commission, which accredits hospitals and other health care organizations, embraced the Pain is the Fifth Vital Sign campaign to increase the identi- fication and treatment of pain, especially with OPRs. Similarly, the American Pain Society and the American Academy of Pain Medicine issued a consensus statement endorsing opioid use for chronic non-cancer pain (31). Although the statement cautioned against imprudent prescribing, this warning may have been overshadowed by assertions that the risk of addiction and tolerance was low, risk of opioid-induced respiratory depression was short-lived, and concerns about drug diversion and abuse should not constrain prescribing. Prior to the introduction of OxyContin, many physicians w ere reluctant to prescribe OPRs on a long-term basis for common chronic conditions because of their concerns about addiction, tolerance, and physiological dependence (80). To overcome
- 49. what they claimed to be “opiopho- bia,” physician-spokespersons for opioid manufacturers published papers and gave lectures in which they claimed that the medical community had been confusing addiction with “physical dependence.” They described addiction as rare and completely distinct from so-called “physical dependence,” which was said to be “clinically unimportant” (60, p. 300). They cited studies with serious methodological flaws to highlight the claim that the risk of addiction was less than 1% (28, 45, 52, 59, 62). In addition to minimizing risks of OPRs, the campaign advanced by opioid manufacturers and pain organizations exaggerated the benefits of long-term OPR use. In fact, high-quality, 562 Kolodny et al. A nn u. R ev . P ub li c H ea
- 53. us e on ly . PU36CH31-Kolodny ARI 11 February 2015 9:9 long-term clinical trials demonstrating the safety and efficacy of OPRs for chronic non-cancer pain have never been conducted. Surveys of patients with chronic non-cancer pain receiving long-term OPRs suggest that most patients continued to experience significant chronic pain and dysfunction (25, 76). The CDC and some professional societies now warn clinicians to avoid prescribing OPRs for common chronic conditions (29). Although increased opioid consumption over the past two decades has been driven largely by greater ambulatory use for chronic non-cancer pain (8), opioid use for acute pain among hospitalized patients has also increased sharply. A recent study found that physicians prescribed opioids in more than 50% of 1.14 million nonsurgical hospital admissions from 2009 to 2010, often in high doses (34). The Joint Commission’s adoption of the Pain is the Fifth Vital Sign campaign and federally mandated patient satisfaction surveys asking patients to rate how often hospital staff did “everything they could to help you with your pain” are noteworthy, given the
- 54. association with increased hospital use of OPRs. REFRAMING THE OPIOID CRISIS AS AN EPIDEMIC OF ADDICTION Policy makers and the media often characterize the opioid crisis as a problem of nonmedical OPR abuse by adolescents and young adults. However, several lines of evidence suggest that addiction occurring in both medical and nonmedical users, rather than abuse per se, is a key driver of opioid-related morbidity and mortality in medical and nonmedical OPR users. Opioid Harms Are Not Limited to Nonmedical Users Over the past decade, federal and state policy makers have attempted to reduce OPR abuse and OPR-related overdose deaths. Despite these efforts, morbidity and mortality associated with OPRs have continued to worsen in almost every US state (10). Thus far, these efforts have focused primarily on preserving access to OPRs for chronic pain patients while reducing nonmedical OPR use (89), defined as the use of a medication without a prescription, in a way other than as prescribed, or for the experience or feeling it causes. However, policy makers who focus solely on reducing nonmedical use are failing to appreciate the high opioid-related morbidity and mortality in pain patients receiving OPR prescriptions for medical purposes. The incidence of nonmedical OPR use increased sharply in the late 1990s, peaking in 2002 with 2.7 million new nonmedical users. Since 2002, the
- 55. incidence of nonmedical use has gradually declined to ∼1.8 million in 2012 (64, 70) (Figure 3). Although the number of new nonmedical users has declined, overdose deaths, addiction treatment admissions, and other adverse public health outcomes associated with OPR use have increased dramatically since 2002. A comparison of age groups of nonmedical OPR users to age groups suffering the highest rates of opioid-related morbidity and mortality suggests that strategies focused exclusively on reducing nonmedical OPR use are insufficient (Figure 4). Although past- month nonmedical use of OPRs is most common in teenagers and young adults between the ages of 15 and 24 (65), OPR overdose deaths occur most often in adults ages 45–54, and the age group that has experienced the greatest increase in overdose mortality over the past decade is 55–64 (15), an age group in which medical use of OPRs is common. Opioid overdoses appear to occur more frequently in medical OPR users than in young nonmedical users. For example, in a study of 254 unintentional opioid overdose decedents in Utah, 92% of the decedents had been receivi ng legitimate OPR prescriptions from health care providers for chronic pain (39). Middle-aged women and the elderly are more likely than other groups to visit doctors with complaints of pain (4). The development of iatrogenic opioid addiction in these groups may explain why they have experienced the largest increase in hospital stays resulting from opioid user www.annualreviews.org • The Opioid Addiction Epidemic 563
- 59. 05 /2 2/ 21 . F or p er so na l us e on ly . PU36CH31-Kolodny ARI 11 February 2015 9:9 3,000 2,500 2,000 1,500
- 60. 1,000 500 0 1991 1993 1995 1997 1999 2001 2003 2005 2007 2009 2011 N u m b er o f n ew u se rs (i n t h o u sa n
- 61. d s) Year Figure 3 First-time nonmedical use of pain relievers. Source: 64, 70. disorders since 1993 (56) (Figure 5). Over the past decade, white women ages 55–64 have also experienced the largest increase in accidental opioid overdose deaths (12, 15). Opioid Addiction Is a Key Driver of Morbidity and Mortality Accidental opioid overdose is a common cause of death in individuals suffering from opioid ad- diction (36). Although overdoses do occur in medical and nonmedical OPR users who are not 1,400 1,200 1,000 800 600 400 200 0
- 62. 1,600 15–24 25–34 35–44 45–54 55–64 65+ 15–24 25–34 35–44 45– 54 55–64 65+ N u m b er s in t h o u sa n d s D ea th r at
- 64. Age group (2011) Age group (2011) a Past month nonmedical OPR use by age b OPR-related unintentional overdose deaths by age Figure 4 (a) Past month nonmedical OPR use by age versus (b) OPR- related unintentional overdose deaths by age. Abbreviation: OPR, opioid pain reliever. Sources: 58, 68. 564 Kolodny et al. A nn u. R ev . P ub li c H ea lt h 20 15
- 68. . PU36CH31-Kolodny ARI 11 February 2015 9:9 400 350 300 250 200 100 50 0 150 R at e o f s ta ys p
- 69. er 1 00 ,0 00 p o p u la ti o n 188.6 70.7 66.6 46.0 51.1 221.8 312.3 338.1 230.8 265.3 18–24 25–44
- 70. 45–64 65–84 85+ 1993 2012 Year Figure 5 Rate of hospital inpatient stays related to OPR use by adult age group, 1993 and 2012. Source: 56. opioid-addicted, consistent findings in samples of OPR overdose decedents show that deaths are most common in individuals likely to be suffering from opioid addiction. A study of 295 unin- tentional OPR overdose deaths in West Virginia found that four out of five decedents (80%) had a history of a substance use disorder (33). Another study found that among 254 opioid overdose decedents in Utah, about three-fourths (76%) had relatives or friends who were concerned about the decedent’s misuse of opioids prescribed for pain (39). The sharp increase in the prevalence of opioid addiction is a key driver of opioid-related morbidity and mortality. The misattribution of the opioid crisis to nonmedical use or abuse rather than to addiction has stymied efforts to address this crisis because it has led to a focus on policies to prevent such nonmedical use at the expense of greater resources committed to preventing and treating opioid addiction in both medical and nonmedical users. PREVENTION STRATEGIES This section organizes strategies for curbing the epidemic of
- 71. opioid addiction into primary, sec- ondary, and tertiary prevention. Although some specific interventions are discussed, we do not provide an exhaustive list. Rather, our purpose is to demonstrate that prevention strategies em- ployed in epidemiologic responses to communicable and noncommunicable disease epidemics apply equally well when the disease in question is opioid addiction. Interventions should focus on preventing new cases of opioid addiction (primary prevention), identifying early cases of opioid addiction (secondary prevention), and ensuring access to effective addiction treatment (tertiary prevention). Primary Prevention The aim of primary prevention is to reduce the incidence of a disease or condition. Opioid addiction is typically chronic, life-long, difficult to treat, and associated with high rates of morbidity and mortality. Thus, bringing the opioid addiction epidemic under control requires effort to prevent new cases from developing. www.annualreviews.org • The Opioid Addiction Epidemic 565 A nn u. R ev . P
- 75. p er so na l us e on ly . PU36CH31-Kolodny ARI 11 February 2015 9:9 Preventing addiction caused by medical exposure to OPRs. The incidence of iatrogenic opioid addiction in patients treated with long-term OPRs is unknown because adequately designed prospective studies have not been conducted. However, opioid use disorders appear to be highly prevalent in chronic pain patients treated with OPRs. A survey performed by Boscarino et al. of 705 chronic pain patients treated in specialty and primary care outpatient centers found that 26% met the Diagnostic and Statistical Manual of Mental Disorders (DSM) IV criteria for opioid dependence, and 35% met DSM V criteria for an opioid use disorder (6, 7). A systematic review of studies utilizing opioids for low back pain found that aberrant drug abuse–related behaviors suggestive of addiction occurred in up to 24% of patients on
- 76. long-term OPRs (50). Many patients on long-term OPRs worry about dependence and addiction and express a desire to taper or cease opioid therapy (76). To reduce the incidence of iatrogenic opioid addiction, health care professionals must prescribe opioids more cautiously for both acute and chronic pain. Unfortunately, the campaign to encourage OPR prescribing has left many health care providers with a poor appreciation of opioid risks, especially the risk of addiction, and an overestimation of opioid benefits. Despite these risks and the lack of evidence supporting long-term efficacy, OPR prescribing for chronic non-cancer pain increased over the past decade while use of nonopioid analgesics decreased (20). This pattern highlights the need for prescriber education that explicitly corrects misperceptions about OPR safety and efficacy. If clinicians treating pain more often substituted nonopioid analgesics and nonpharmaceutical approaches for OPRs, evidence suggests the incidence of opioid addiction would decline and outcomes for patients with chronic non- cancer pain would improve. Many prescribers are unaware that evidence of long-term effectiveness for OPRs is lacking and that risks, in addition to addiction, include respiratory depression leading to unintentional overdose death; serious fractures from falls (71, 77); hypogonadism and other endocrine effects that can cause a spectrum of adverse effects (88); increased pain sensitivity (2); chronic constipation and serious fecal impaction (81); and chronic dry mouth, which can lead to tooth decay (79).
- 77. Providing prescribers with accurate information about opioid risks and benefits could result in more informed risk/benefit appraisals. Indeed, one of the lessons learned from the nineteenth- century opioid addiction epidemic was that physicians were educable. By the early 1900s, aggressive opioid prescribing had become the hallmark of older, less- competent physicians (5). Several states, including Iowa, Kentucky, Massachusetts, Ohio, Tennessee, and Utah, have passed mandatory prescriber education legislation (89). In addition, the US Food and Drug Admin- istration (FDA) is requiring manufacturers of extended release and long-acting OPRs to sponsor educational programs for prescribers. Unfortunately, some of these educational programs, includ- ing those required by the FDA, imply that OPRs are safe and effective for chronic non-cancer pain instead of offering prescribers accurate information about OPR risks and benefits (84). It remains unclear whether or not educational programs such as these will reduce OPR prescribing for common conditions where risks of use are likely to outweigh benefits. Some opioid manufacturers have reformulated OPRs to make them more difficult to misuse through an intranasal or injection route. These so-called abuse- deterrent formulations (ADFs) may offer safety advantages over easily snorted and injected OPRs, but they do not render them less addictive. Opioid addiction, in both medical and nonmedical OPR users, most frequently develops through oral use (85). Some opioid-addicted individuals may transition to intranasal or
- 78. injection use, but most continue to use OPRs orally (47). Thus, ADFs should not be considered a primary prevention strategy for opioid addiction. In 2013, the New York City Department of Health and Mental Hygiene released emergency room guidelines on OPR prescribing (55). Recommendations included in the guidelines call for substituting nonopioid analgesics when possible, avoiding use of extended-release OPRs, and 566 Kolodny et al. A nn u. R ev . P ub li c H ea lt h 20 15 .3
- 82. PU36CH31-Kolodny ARI 11 February 2015 9:9 limiting the supply to three days. Reducing patient exposure to OPRs and reducing the supply of excess OPRs in the homes of discharged patients may be effective strategies for preventing opioid addiction that can occur from both medical and nonmedical OPR use. Preventing addiction caused by nonmedical exposure to OPRs. Individuals who use OPRs nonmedically are at risk for developing opioid addiction. Thus, efforts to reduce nonmedical use are an important primary prevention strategy. Adolescents and young adults who experiment with nonmedical use are most likely to obtain OPRs for free from friends or family members who had received a legitimate prescription (70). This information suggests that more cautious prescribing is required to prevent nonmedical use of excess OPRs. Unused OPRs in medicine chests should be immediately discarded or returned to a pharmacy, which became permissible in October 2014 after the Drug Enforcement Administration made a federal regulatory change (82). Although OPRs have an abuse liability similar to that of heroin (17), they are commonly per- ceived as less risky. Seventy-three percent of eighth graders surveyed in 2013 perceived occasional use of heroin without a needle as high risk, but only 26% perceived occasional use of Vicodin as high risk (41). Eighth graders also perceived occasional Vicodin
- 83. use as less risky than occasional marijuana use, less risky than smoking 1–5 cigarettes per day, and less risky than moderate alcohol use. Individuals who perceive the risk of nonmedical OPR use to be low may be more likely to misuse OPRs. A 2004 survey found that college students w ho perceive a low level of risk from OPRs were 9.6 times more likely to use OPRs nonmedically, as compared with those who perceive these medications as harmful (3). Although the ability for causal inference from this type of cross- sectional survey is limited, this finding suggests that social marketing campaigns designed to increase perceived harmfulness of OPRs may be an effective prevention strategy. Secondary Prevention The aim of secondary prevention is to screen for a health condition after its onset but before it causes serious complications. Efforts to identify and treat opioid-addicted individuals early in the course of the disease are likely to reduce the risk of overdose, psychosocial deterioration, transition to injection opioid use, and medical complications. Physicians are frequently the source of OPRs for opioid- addicted medical and nonmedical users (43). Contacts with medical professionals present valuable opportunities for early identi- fication of opioid addiction. However, detection of opioid addiction in OPR users can be very difficult. Opioid-addicted chronic pain patients may demonstrate aberrant drug-related behaviors,
- 84. such as presenting for early refills. However, some opioid- addicted pain patients, especially those prescribed high doses, may not demonstrate drug-seeking behavior. Opioid-addicted individuals receiving OPR prescriptions are often reluctant to disclose their concerns about addiction with prescribers because they fear being judged, being cut off from a legitimate supply, or being labeled as malingerers for feigning pain. The difficulty of diagnosing opioid addiction in individuals motivated to conceal their condi- tion suggests that prescribers should seek collateral information before prescribing OPRs. Urine toxicology can be used to verify a patient’s self-reported drug ingestion history (53). However, urine toxicology of patients on long-term OPRs is not a reliable strategy for identifying opioid addiction. Urine toxicology cannot determine if a patient is taking extra doses or if a patient is using OPRs by an intranasal or injection route. Opioid-addicted individuals may receive OPR prescriptions from multiple providers, a prac- tice referred to as “doctor shopping.” Doctor shoppers can be identified through use of state www.annualreviews.org • The Opioid Addiction Epidemic 567 A nn u. R ev
- 88. or p er so na l us e on ly . PU36CH31-Kolodny ARI 11 February 2015 9:9 prescription drug monitoring programs (PDMPs). Some state PDMPs send unsolicited reports to the medical providers of doctor shoppers. Research suggests that unsolicited reports increase prescribers’ ability to detect opioid addiction, sometimes prompting actions such as coordinating care with other providers and modifying their own prescribing practices, as well as screening and referring for addiction treatment (78). Prescribers in most states can consult their state PDMP before prescribing OPRs. PDMPs may be especially useful in emergency rooms and other settings where opioid-addicted individuals feign pain to obtain OPRs. Too often, however, patients identified as
- 89. doctor shoppers are simply turned away, without hospital staff attempting to link these patients to addiction treatment services. Efforts must be made to help these clinicians understand that drug- seeking patients are suffering from the chronic, life-threatening disease of opioid addiction. One challenge to PDMP effectiveness has been the low rate of provider use of these data (48). To increase prescriber utilization, Kentucky, Tennessee, and New York passed legislation mandating that prescribers check the PDMP before prescribing controlled substances. Data from these states indicate that PDMP utilization increased rapidly subsequent to the mandate, which correlated with declines in opioid prescribing (KY, TN, NY) and a sharp drop in visits to multiple providers (TN, NY) (35). Tertiary Prevention Tertiary prevention strategies involve both therapeutic and rehabilitative measures once a disease is firmly established. The goal of tertiary prevention of opioid addiction is to prevent overdose deaths, medical complications, psychosocial deterioration, transition to injection drug use, and injection-related infectious diseases. Doing so is accomplished mainly by ensuring that opioid- addicted individuals can access effective and affordable opioid addiction treatment. Opioid addiction treatment. The need for opioid addiction treatment is great and largely unmet. According to the NSDUH, an estimated 2.1 million Americans are addicted to OPRs, and 467,000
- 90. are addicted to heroin (70). Unfortunately, these estimates exclude many opioid-addicted pain patients because NSDUH participants are told by surveyors that “we are only interested in your use of prescription pain relievers that were not prescribed for you or that you used only for the experience or feeling they caused” (67, p. 124). In 2005, there were an estimated 10 million chronic pain patients receiving daily, long-term treatment with OPRs (8). The continuing increase in opioid consumption from 2005 to 2011 (42) suggests that the number may now exceed 10 million. Applying the prevalence estimates of DSM IV opioid dependence found by Boscarino et al. (6) in pain patients taking long-term opioids would indicate that an additional 2.5 million chronic pain patients may be opioid-addicted. Thus, the total number of Americans suffering from opioid addiction may exceed 5 million. Treatment of opioid addiction includes pharmacotherapies and psychosocial approaches, in- cluding residential treatment, mutual-help programs (e.g., Narcotics Anonymous), and 12-Step treatment programs. These modalities may be used as stand- alone interventions or in combination with pharmacotherapy. Psychosocial opioid addiction treatment approaches show value and are an important treatment option (63). However, research with greater specificity and consistency is needed to better evaluate outcomes. Pharmacotherapies for opioid addiction include agonist maintenance with methadone and partial-agonist maintenance with buprenorphine and antagonist
- 91. treatment with naltrexone, which is available in a monthly injection. Methadone and buprenorphine work by controlling cravings. Naltrexone works by preventing opioid-addicted individuals from feeling the effects of opioids. 568 Kolodny et al. A nn u. R ev . P ub li c H ea lt h 20 15 .3 6: 55 9-
- 94. 58 :a 89 o n 05 /2 2/ 21 . F or p er so na l us e on ly . PU36CH31-Kolodny ARI 11 February 2015 9:9
- 95. Naltrexone may be helpful in highly motivated and carefully selected patients. However, patients treated with naltrexone may be at increased risk of overdose death should relapse occur (23). Multiple well-designed randomized controlled trials provide strong evidence that buprenor- phine maintenance and methadone maintenance are safe and effective treatments for opioid ad- diction (30, 40, 46, 49, 74, 75). Both buprenorphine and methadone treatment are associated with reduced overdose risk and improved maternal and fetal outcomes in pregnancy (19, 44, 51, 72). Despite strong evidence supporting the use of buprenorphine and methadone, fewer than 1 million Americans are receiving these treatments (87). Methadone poses a substantially greater risk of respiratory depression than does buprenorphine and can be obtained only from licensed opioid treatment programs (OTPs). The lack of OTPs in many communities presents a major challenge to expanding access to methadone. In contrast, buprenorphine, a partial opioid agonist, has a better safety profile than does methadone and can be prescribed in an office-based setting (26). Barriers to accessing buprenorphine include federal lim- its on the number of patients a physician may treat, ineligibility of nurse practitioners to prescribe it, and inadequate integration of buprenorphine into primary care treatment. Access to buprenor- phine treatment could be expanded if the federal government eased or remove regulatory barriers. Harm-reduction approaches. Tertiary prevention strategies also include harm-reduction ap-
- 96. proaches to improving health outcomes and reducing overdose deaths. In the subset of opioid- addicted individuals who are heroin injection drug users, evidence suggests that access to syringe exchange programs can prevent HIV infection (22). These efforts have been less effective at pre- venting hepatitis C infection, which is increasing rapidly in young, white IDUs (32). Expanding access to naloxone, an opioid overdose antidote, can prevent overdose deaths by reversing life-threatening respiratory depression. In the 1990s, syringe exchange programs began distributing naloxone to injection drug users for the purpose of rescuing peers. Evidence shows that clients of syringe exchange programs demonstrated the ability to successfully reverse overdoses when they had been provided with naloxone and training (73). In addition, providing family members of opioid-addicted individuals and nonparamedic first responders with naloxone may be an effective strategy for rescuing overdose victims (21, 90). At present, there are more than 188 community-based naloxone distribution programs in 15 states and the District of Columbia (11). CONCLUSION The increased prevalence of opioid addiction, caused by overprescribing of OPRs, has led to a parallel increase in opioid overdose deaths. Efforts to address this crisis that focus exclusively on reducing nonmedical OPR use have been ineffective. Middle- aged and elderly individuals commonly exposed to OPRs for pain treatment have experienced the largest increase in rates of
- 97. opioid-related morbidity and mortality. Recognition that opioid addiction in both medical and nonmedical users is a key driver of opioid-related morbidity and mortality will result in a more effective response to this public health crisis. Just as public health authorities would approach other disease outbreaks, efforts must be made to reduce the incidence of opioid addiction, identify cases early, and ensure access to effective treatment. Preventing opioid addiction requires strategies that foster more cautious and selective OPR prescribing. However, if prescribing is reduced without also ensuring access to addiction treatment, the opioid overdose death rate may remain at a historically high level and the use of heroin may continue to increase. Coordinated efforts from federal agencies, state agencies, health care insurers, and health care providers are required to address the needs of millions of Americans now struggling with this chronic, life-threatening disease. www.annualreviews.org • The Opioid Addiction Epidemic 569 A nn u. R ev . P ub li
- 101. so na l us e on ly . PU36CH31-Kolodny ARI 11 February 2015 9:9 DISCLOSURE STATEMENT Dr. Alexander is Chair of the FDA’s Peripheral and Central Nervous System Advisory Committee, serves as a paid consultant to IMS Health, and serves on an IMS Health scientific advisory board. This arrangement has been reviewed and approved by Johns Hopkins University in accordance with its conflict of interest policies. Ms. Hwang is a current ORISE Fellow at the FDA. LITERATURE CITED 1. Angres DH, Bettinardi-Angres K. 2008. The disease of addiction: origins, treatment, and recovery. Dis. Mon. 54:696–721 2. Angst MS, Clark JD. 2006. Opioid-induced hyperalgesia: a qualitative systematic review. Anesthesiology 104:570–87
- 102. 3. Arria AM, Caldeira KM, Vincent KB, O’Grady KE, Wish ED. 2008. Perceived harmfulness predicts nonmedical use of prescription drugs among college students: interactions with sensation-seeking. Prev. Sci. 9:191–201 4. Blackwell DL, Lucas JW, Clarke TC. 2014. Summary Health Statistics for U.S. Adults: National Health Interview Survey, 2012. Vital Health Stat. 10(260). Hyattsville, MD: Natl. Cent. Health Stat., U.S. Dept. Health Hum. Serv. 5. Blair T. 1919. Is opium the “sheet-anchor of treatment”? Am. J. Clin. Med. 26:829–34 6. Boscarino JA, Rukstalis M, Hoffman SN, Han JJ, Erlich PM, et al. 2010. Risk factors for drug dependence among out-patients on opioid therapy in a large US health-care system. Addiction 105:1776–82 7. Boscarino JA, Rukstalis MR, Hoffman SN, Han JJ, Erlich PM, et al. 2011. Prevalence of prescription opioid-use disorder among chronic pain patients: comparison of the DSM-5 versus DSM-4 diagnostic criteria. J. Addict. Dis. 30:185–94 8. Boudreau D, Von Korff M, Rutter CM, Saunders K, Ray GT, et al. 2009. Trends in long-term opioid therapy for chronic non-cancer pain. Pharmacoepidemiol. Drug Saf. 18:1166–75 9. Campbell JN. 1996. APS 1995 presidential address. Pain Forum 5:85–88 10. CDC (Cent. Dis. Control Prev.). 2011. Vital signs: overdoses of prescription opioid pain relievers—United
- 103. States, 1999–2008. MMWR 60:1487–92 11. CDC (Cent. Dis. Control Prev.). 2012. Community-based opioid overdose prevention programs providing naloxone—United States, 2010. MMWR 6:101–5 12. CDC (Cent. Dis. Control Prev.). 2013. Vital signs: overdoses of prescription opioid pain relievers and other drugs among women—United States, 1999–2010. MMWR 62:537–42 13. CDC (Cent. Dis. Control Prev.). 2014. CDC’s Top Ten: 5 Health Achievements in 2013 and 5 Health Threats in 2014. Atlanta, GA: CDC. http://blogs.cdc.gov/cdcworksforyou24-7/2013/12/cdc’s- top-ten-5-health-achievements-in-2013-and-5-health-threats-in- 2014/ 14. CDC (Cent. Dis. Control Prev.). 2014. QuickStats: rates of drug poisoning deaths involving heroin,∗ by selected age and racial/ethnic groups—United States, 2002 and 2011. MMWR 63:595 15. Chen LH, Hedegaard H, Warner M. 2014. Drug-Poisoning Deaths Involving Opioid Analgesics: United States, 1999–2011. NCHS Data Brief No. 166. Hyattsville, MD: Natl. Cent. Health Stat. 16. Cicero TJ, Ellis MS, Surratt HL, Kurtz SP. 2014. The changing face of heroin use in the United States: a retrospective analysis of the past 50 years. JAMA Psychiatry 71:821–26 17. Comer SD, Sullivan MA, Whittington RA, Vosburg SK, Kowalczyk WJ. 2008. Abuse liability of pre-
- 104. scription opioids compared to heroin in morphine-maintained heroin abusers. Neuropsychopharmacology 33:1179–91 18. Courtwright DT. 2001. Dark Paradise: A History of Opiate Addiction in America. Cambridge, MA: Harvard Univ. Press. Revis. ed. 19. Coyle MG, Salisbury AL, Lester BM, Jones HE, Lin H, et al. 2012. Neonatal neurobehavior effects following buprenorphine versus methadone exposure. Addiction 107:63–73 20. Daubresse M, Chang HY, Yu Y, Viswanathan S, Shah ND, et al. 2013. Ambulatory diagnosis and treatment of nonmalignant pain in the United States, 2000–2010. Med. Care 51:870–78 570 Kolodny et al. A nn u. R ev . P ub li c H ea
- 108. us e on ly . http://blogs.cdc.gov/cdcworksforyou24-7/2013/12/cdc's-top-ten- 5-health-achievements-in-2013-and-5-health-threats-in-2014/ http://blogs.cdc.gov/cdcworksforyou24-7/2013/12/cdc's-top-ten- 5-health-achievements-in-2013-and-5-health-threats-in-2014/ PU36CH31-Kolodny ARI 11 February 2015 9:9 21. Davis CS, Ruiz S, Glynn P, Picariello G, Walley AY. 2014. Expanded access to naloxone among firefight- ers, police officers, and emergency medical technicians in Massachusetts. Am. J. Public Health 104:e7–9 22. Des Jarlais DC, Perlis T, Arasteh K, Torian LV, Beatrice S, et al. 2005. HIV incidence among injection drug users in New York City, 1990 to 2002: use of serologic test algorithm to assess expansion of HIV prevention services. Am. J. Public Health 95:1439–44 23. Digiusto E, Shakeshaft A, Ritter A, O’Brien S, Mattick RP. 2004. Serious adverse events in the Australian National Evaluation of Pharmacotherapies for Opioid Dependence. Addiction 99:450–60 24. DuPont RL, Greene MH. 1973. The dynamics of a heroin addiction epidemic. Science 181:716–22 25. Eriksen J, Sjøgren P, Bruera E, Ekholm O, Rasmussen NK. 2006. Critical issues on opioids in chronic
- 109. non-cancer pain: an epidemiological study. Pain 125:172–79 26. Fareed A, Vayalapalli S, Byrd-Sellers J, Casarella J, Drexler K. 2011. Safety and efficacy of long-term buprenorphine maintenance treatment. Addict. Dis. Treat. 10:123–30 27. Fauber J. 2012. Painkiller boom fueled by networking: doctors, researchers with financial ties to drug makers set stage for surge in prescriptions. Milwaukee- Wisconsin Journal Sentinel, Feb. 18, p. A1 28. Fishbain DA, Cole B, Lewis J, Rosomoff HL, Rosomoff RS. 2008. What percentage of chronic nonmalig- nant pain patients exposed to chronic opioid analgesic therapy develop abuse/addiction and/or aberrant drug-related behaviors? A structured evidence-based review. Pain Med. 9:444–59 29. Franklin GM. 2014. Opioids for chronic noncancer pain: a position paper of the American Academy of Neurology. Neurology 83:1277–84 30. Fudala PJ, Bridge TP, Herbert S, Williford WO, Chiang CN, et al. 2003. Office-based treatment of opiate addiction with a sublingual-tablet formulation of buprenorphine and naloxone. N. Engl. J. Med. 349:949–58 31. Haddox JD, Joranson D, Angarola RT, Brady A, Carr DB, et al. 1997. The use of opioids for the treatment of chronic pain: a consensus statement from the American Academy of Pain Medicine and the American Pain Society. Clin. J. Pain 13:6–8
- 110. 32. Hagan H, Pouget ER, Williams IT, Garfein RL, Strathdee SA, et al. 2010. Attribution of hepatitis C virus seroconversion risk in young injection drug users in 5 US cities. J. Infect. Dis. 201:378–85 33. Hall AJ, Logan JE, Toblin RL, Kaplan JA, Kraner JC, et al. 2008. Patterns of abuse among unintentional pharmaceutical overdose fatalities. JAMA 300:2613–20 34. Herzig SJ, Rothberg MB, Cheung M, Ngo LH, Marcantonio ER. 2014. Opioid utilization and opioid- related adverse events in nonsurgical patients in US hospital s. J. Hosp. Med. 9:73–81 35. Hopkins D, Dreyzehner JJ, O’Leary T. 2014. Lessons learned from mandating prescriber compliance. Presented at Natl. Prescr. Abuse Sum., April 22–23, Atlanta 36. Hser YI, Hoffman V, Grella CE, Anglin MD. 2001. A 33- year follow-up of narcotics addicts. Arch. Gen. Psychiatry 58:503–8 37. Hughes PH, Barker NW, Crawford GA, Jaffe JH. 1972. The natural history of a heroin epidemic. Am. J. Public Health 62:995–1001 38. INCB (Int. Narc. Control Board). 2007. The Report of the International Narcotics Control Board for 2007. Vienna: INCB 39. Johnson EM, Lanier WA, Merrill RM, Crook J, Porucznik CA, et al. 2013. Unintentional prescription opioid-related overdose deaths: description of decedents by next of kin or best contact, Utah, 2008–2009. J. Gen. Intern. Med. 28:522–29
- 111. 40. Johnson RE, Chutuape MA, Strain EC, Walsh SL, Stitzer ML, Bigelow GE. 2000. A comparison of levomethadyl acetate, buprenorphine, and methadone for opioid dependence. N. Engl. J. Med. 343:1290– 97 41. Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. 2014. Monitoring the future National Survey Results on Drug Use: 1975–2013. Overview, key findings on adolescent drug use. Ann Arbor, MI: Inst. Soc. Res., Univ. Mich. 42. Jones CM. 2013. Trends in the distribution of selected opioids by state, US, 1999–2011. Presented at Natl. Meet. Safe States Alliance, June 6, Baltimore, MD 43. Jones CM, Paulozzi LJ, Mack KA. 2014. Sources of prescription opioid pain relievers by frequency of past-year nonmedical use: United States, 2008–2011. JAMA Intern. Med. 174:802–3 www.annualreviews.org • The Opioid Addiction Epidemic 571 A nn u. R ev . P ub li c
- 115. na l us e on ly . PU36CH31-Kolodny ARI 11 February 2015 9:9 44. Jones HE, Kaltenbach K, Heil SH, Stine SM, Coyle MG, et al. 2010. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N. Engl. J. Med. 363:2320–31 45. Juurlink DN, Dhalla IA. 2012. Dependence and addiction during chronic opioid therapy. J. Med. Toxicol. 8:393–99 46. Kakko J, Svanborg KD, Kreek MJ, Heilig M. 2003. 1-year retention and social function after buprenorphine-assisted relapse prevention treatment for heroin dependence in Sweden: a randomised, placebo-controlled trial. Lancet 361:662–68 47. Katz N, Dart RC, Bailey E, Trudeau J, Osgood E, Paillard F. 2011. Tampering with prescription opioids: nature and extent of the problem, health consequences, and solutions. Am. J. Drug Alcohol Abuse 37:205–17 48. Kreiner P, Nikitin R, Shields TP. 2014. Bureau of Justice
- 116. Assistance Prescription Drug Monitoring Program Performance Measures Report: January 2009 through June 2012. Waltham, MA: PDMP Cent. Excell., Brandeis Univ. 49. Ling W, Charuvastra C, Collins JF, Batki S, Brown LS, et al. 1998. Buprenorphine maintenance treatment of opiate dependence: a multicenter, randomized clinical trial. Addiction 93:475–86 50. Martell BA, O’Connor PG, Kerns RD, Becker WC, Morales KH, et al. 2007. Systematic review: opioid treatment for chronic back pain: prevalence, efficacy, and association with addiction. Ann. Intern. Med. 146:116–27 51. McCarthy JJ, Leamon MH, Parr MS, Anania B. 2005. High- dose methadone maintenance in pregnancy: maternal and neonatal outcomes. Am. J. Obstet. Gynecol. 193:606–10 52. Medina JL, Diamond S. 1977. Drug dependency in patients with chronic headache. Headache 17:12–14 53. Monte AA, Heard KJ, Hoppe JA, Vasiliou V, Gonzalez FJ. 2015. The accuracy of self-reported drug ingestion histories in emergency department patients. J. Clin. Pharmacol. 55:33–38 54. Muhuri PK, Gfroerer JC, Davies MC. 2013. Associations of nonmedical pain reliever use and initia- tion of heroin use in the United States. CBHSQ Data Rev. Aug.: http://www.samhsa.gov/data/sites/ default/files/DR006/DR006/nonmedical-pain-reliever-use- 2013.htm
- 117. 55. N.Y. City Dep. Health Ment. Hyg. 2013. New York City Emergency Department Discharge Opioid Prescrib- ing Guidelines. Long Island City, NY: NYC Health. http://www.nyc.gov/html/doh/downloads/pdf/ basas/opioid-prescribing-guidelines.pdf 56. Owens PL, Barrett ML, Weiss AJ, Washington RE, Kronick R. 2014. Hospital inpatient utiliza- tion related to opioid overuse among adults, 1993–2012. HCUP Stat. Brief No. 177, Agency Healthc. Res. Quality (AHRQ), Rockville, MD. http://www.hcup- us.ahrq.gov/reports/statbriefs/sb177- Hospitalizations-for-Opioid-Overuse.pdf 57. Patrick SW, Schumacher RE, Benneyworth BD, Krans EE, McAllister JM, Davis MM. 2012. Neonatal abstinence syndrome and associated health care expenditures: United States, 2000–2009. JAMA 307:1934– 40 58. Paulozzi LJ. 2010. The epidemiology of drug overdoses in the United States. Presented at Promis. Leg. Re- sponses to the Epidemic of Prescr. Drug Overdoses in the U.S., Maimonides Med. Cent. Dep. Psychiatry, Dec. 2, Grand Rounds, Brooklyn 59. Perry S, Heidrich G. 1982. Management of pain during debridement: a survey of U.S. burn units. Pain 13:267–80 60. Portenoy RK. 1996. Opioid therapy for chronic nonmalignant pain: clinicians’ perspective. J. Law Med. Ethics 24:296–309 61. Portenoy RK, Foley KM. 1986. Chronic use of opioid analgesics in non-malignant pain: report of 38
- 118. cases. Pain 25:171–86 62. Porter J, Jick H. 1980. Addiction rare in patients treated with narcotics. N. Engl. J. Med. 302:123 63. Reif S, George P, Braude L, Dougherty RH, Daniels AS, et al. 2014. Residential treatment for individuals with substance use disorders: assessing the evidence. Psychiatr. Serv. 65:301–12 64. SAMHSA (Substance Abuse Ment. Health Serv. Adm.). 2003. Results from the 2002 National Survey on Drug Use and Health: National Findings. Off. Appl. Stud., NHSDA Ser. H-22, DHHS Publ. No. SMA 03-3836. Rockville, MD: SAMHSA 65. SAMHSA (Subst. Abuse Ment. Health Serv. Adm.). 2009. Trends in Nonmedical Use of Prescription Pain Relievers: 2002 to 2007. NSDUH Rep. Rockville, MD: SAMHSA 572 Kolodny et al. A nn u. R ev . P ub li c
- 122. na l us e on ly . http://www.samhsa.gov/data/sites/default/files/DR006/DR006/n onmedical-pain-reliever-use-2013.htm http://www.samhsa.gov/data/sites/default/files/DR006/DR006/n onmedical-pain-reliever-use-2013.htm http://www.nyc.gov/html/doh/downloads/pdf/basas/opioid- prescribing-guidelines.pdf http://www.nyc.gov/html/doh/downloads/pdf/basas/opioid- prescribing-guidelines.pdf http://www.hcup-us.ahrq.gov/reports/statbriefs/sb177- Hospitalizations-for-Opioid-Overuse.pdf http://www.hcup-us.ahrq.gov/reports/statbriefs/sb177- Hospitalizations-for-Opioid-Overuse.pdf PU36CH31-Kolodny ARI 11 February 2015 9:9 66. SAMHSA (Subst. Abuse Ment. Health Serv. Adm.). 2010. Center for Behavioral Health Statistics and Quality. Treatment Episode Data Set (TEDS): 2007. Discharges from Substance Abuse Treatment Services. DASIS Ser.: S-51, HHS Publ. No. (SMA) 10-4479. Rockville, MD: SAMHSA 67. SAMHSA (Subst. Abuse Ment. Health Serv. Adm.). 2011. CAI Specifications for Programming in English: 2012 National Survey on Drug Use and Health. Rockville, MD:
- 123. SAMHSA. https://www.icpsr.umich.edu/ icpsrweb/DSDR/studies/34933?keyword%5B0%5D=drug+depen dence&q=ANLNDMOR&= groupResults=false 68. SAMHSA (Subst. Abuse Ment. Health Serv. Adm.). 2013. Center for Behavioral Health Statistics and Quality. Treatment Episode Data Set (TEDS): 2001–2011. National Admissions to Substance Abuse Treatment Services. BHSIS Ser. S-65, DHHS Publ. No. SMA 13-4772. Rockville, MD: SAMHSA 69. SAMHSA (Subst. Abuse Ment. Health Serv. Adm.). 2013. Drug Abuse Warning Network, 2011: National Estimates of Drug-Related Emergency Department Visits. DHHS Publ. No. SMA 13-4760, DAWN Ser. D-39. Rockville, MD: SAMHSA 70. SAMHSA (Subst. Abuse Ment. Health Serv. Adm.). 2013. Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings. NSDUH Ser. H-46, DHHS Publ. No. SMA 13-4795. Rockville, MD: SAMHSA 71. Saunders KW, Dunn KM, Merrill JO, Sullivan MD, Weisner CM, et al. 2010. Relationship of opioid use and dosage levels to fractures in older chronic pain patients. J. Gen. Intern. Med. 25:310–15 72. Schwartz RP, Gryczynski J, O’Grady KE, Sharfstein JM, Warren G, et al. 2013. Opioid agonist treatments and heroin overdose deaths in Baltimore, Maryland, 1995–2009. Am. J. Public Health 103:917–22 73. Seal KH, Thawley R, Gee L, Bamberger J, Kral AH, et al. 2005. Naloxone distribution and cardiopul-
- 124. monary resuscitation training for injection drug users to prevent heroin overdose death: a pilot intervention study. J. Urban Health 82:303–11 74. Sees KL, Delucchi KL, Masson C, Rosen A, Clark HW, et al. 2000. Methadone maintenance for opioid dependence. JAMA 284:694–95 75. Strain EC, Bigelow GE, Liebson IA, Stitzer ML. 1999. Moderate versus high-dose methadone in the treatment of opioid dependence: a randomized trial. JAMA 281:1000–5 76. Sullivan MD, Von Korff M, Banta-Green C, Merrill JO, Saunders K. 2010. Problems and concerns of patients receiving chronic opioid therapy for chronic non-cancer pain. Pain 149:345–53 77. Takkouche B, Montes-Martı́nez A, Gill SS, Etminan M. 2007. Psychotropic medications and the risk of fracture: a meta-analysis. Drug Saf. 30:171–84 78. Thomas CP, Kim M, Nikitin RV, Kreiner P, Clark TW, Carrow GM. 2014. Prescriber response to unsolicited prescription drug monitoring program reports in Massachusetts. Pharmacoepidemiol. Drug Saf. 23:950–57 79. Thomson MW, Poulton R, Broadbent MJ, Al-Kubaisy S. 2006. Xerostomia and medications among 32-year-olds. Acta. Odontol. Scand. 64:249–54 80. Turk DC, Brody MC, Okifuji EA. 1994. Physicians’ attitudes and practices regarding the long-term prescribing of opioids for non-cancer pain. Pain 59:201–8
- 125. 81. Tuteja AK, Biskupiak J, Stoddard GJ, Lipman AG. 2010. Opioid-induced bowel disorders and narcotic bowel syndrome in patients with chronic non-cancer pain. Neurogastroenterol. Motil. 22:424–30 82. US Drug Enforc. Admin. (DEA). 2014. Disposal of controlled substances. Fed. Regist. 79(174):53520–70 83. Upadhyay J, Maleki N, Potter J, Elman I, Rudrauf D, et al. 2010. Alterations in brain structure and functional connectivity in prescription opioid-dependent patients. Brain 133:2098–114 84. US FDA (Food Drug Admin.). 2011. Comment from Physicians for Responsible Opioid Prescribing on the Food and Drug Administration (FDA) Notice: Draft blueprint for prescriber education; availability: long- acting/extended-release opioid class-wide risk evaluation and mitigation strategy. Phys. Responsib. Opiod Pre- scr. (PROP), FDA-2011-D-0771-0069, Regulations.gov, Washington, DC. http://www.regulations. gov/#!documentDetail;D=FDA-2011-D-0771-0069 85. US FDA (Food Drug Admin.). 2013. Guidance for Industry: Abuse-Deterrent Opioids— Evaluation and Labeling. Silver Spring, MD: US FDA. http://www.fda.gov/downloads/Drugs/ GuidanceComplianceRegulatoryInformation/Guidances/UCM33 4743.pdf 86. US GAO (Gen. Account. Off.). OxyContin Abuse and Diversion and Efforts to Address the Problem. GAO- 04-110. Washington, DC: GAO. http://www.gao.gov/new.items/d04110.pdf www.annualreviews.org • The Opioid Addiction Epidemic 573
- 130. http://www.regulations.gov/#!documentDetail;D=FDA-2011-D- 0771-0069 http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegu latoryInformation/Guidances/UCM334743.pdf http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegu latoryInformation/Guidances/UCM334743.pd f http://www.gao.gov/new.items/d04110.pdf PU36CH31-Kolodny ARI 11 February 2015 9:9 87. Volkow ND, Frieden TR, Hyde PS, Cha SS. 2014. Medication-assisted therapies—tackling the opioid- overdose epidemic. N. Engl. J. Med. 370:2063–6 88. Vuong C, Van Uum SH, O’Dell LE, Lutfy K, Friedman TC. 2010. The effects of opioids and opioid analogs on animal and human endocrine systems. Endocr. Rev. 31:98–132 89. White House ONDCP (Off. Natl. Drug Control Policy). 2014. National Drug Control Strategy. Washington, DC: ONDCP. http://www.whitehouse.gov/sites/default/files/ndcs_2014.pdf 90. Williams AV, Marsden J, Strang J. 2014. Training family members to manage heroin overdose and administer naloxone: randomized trial of effects on knowledge and attitudes. Addiction 109:250–59 91. Younger JW, Chu LF, D’Arcy NT, Trott KE, Jastrzab LE, Mackey SC. 2011. Prescription opioid anal- gesics rapidly change the human brain. Pain 152:1803–10 574 Kolodny et al.
- 134. 05 /2 2/ 21 . F or p er so na l us e on ly . http://www.whitehouse.gov/sites/default/files/ndcs_2014.pdf PU36-FrontMatter ARI 25 February 2015 11:17 Annual Review of Public Health Volume 36, 2015Contents Symposium: Strategies to Prevent Gun Violence
- 135. Commentary: Evidence to Guide Gun Violence Prevention in America Daniel W. Webster � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 1 The Epidemiology of Firearm Violence in the Twenty-First Century United States Garen J. Wintemute � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 5 Effects of Policies Designed to Keep Firearms from High-Risk Individuals Daniel W. Webster and Garen J. Wintemute � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �21 Cure Violence: A Public Health Model to Reduce Gun Violence Jeffrey A. Butts, Caterina Gouvis Roman, Lindsay Bostwick, and Jeremy R. Porter � � � � �39 Focused Deterrence and the Prevention of Violent Gun Injuries: Practice, Theoretical Principles, and Scientific Evidence Anthony A. Braga and David L. Weisburd � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �55 Epidemiology and Biostatistics Has Epidemiology Become Infatuated With Methods? A Historical Perspective on the Place of Methods During the Classical
- 136. (1945–1965) Phase of Epidemiology Alfredo Morabia � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �69 Statistical Foundations for Model-Based Adjustments Sander Greenland and Neil Pearce � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �89 The Elusiveness of Population-Wide High Blood Pressure Control Paul K. Whelton � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 109 The Epidemiology of Firearm Violence in the Twenty-First Century United States Garen J. Wintemute � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 5 Focused Deterrence and the Prevention of Violent Gun Injuries: Practice, Theoretical Principles, and Scientific Evidence Anthony A. Braga and David L. Weisburd � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �55 vii A nn
- 140. 2/ 21 . F or p er so na l us e on ly . PU36-FrontMatter ARI 25 February 2015 11:17 Unintentional Home Injuries Across the Life Span: Problems and Solution s Andrea C. Gielen, Eileen M. McDonald, and Wendy Shields �