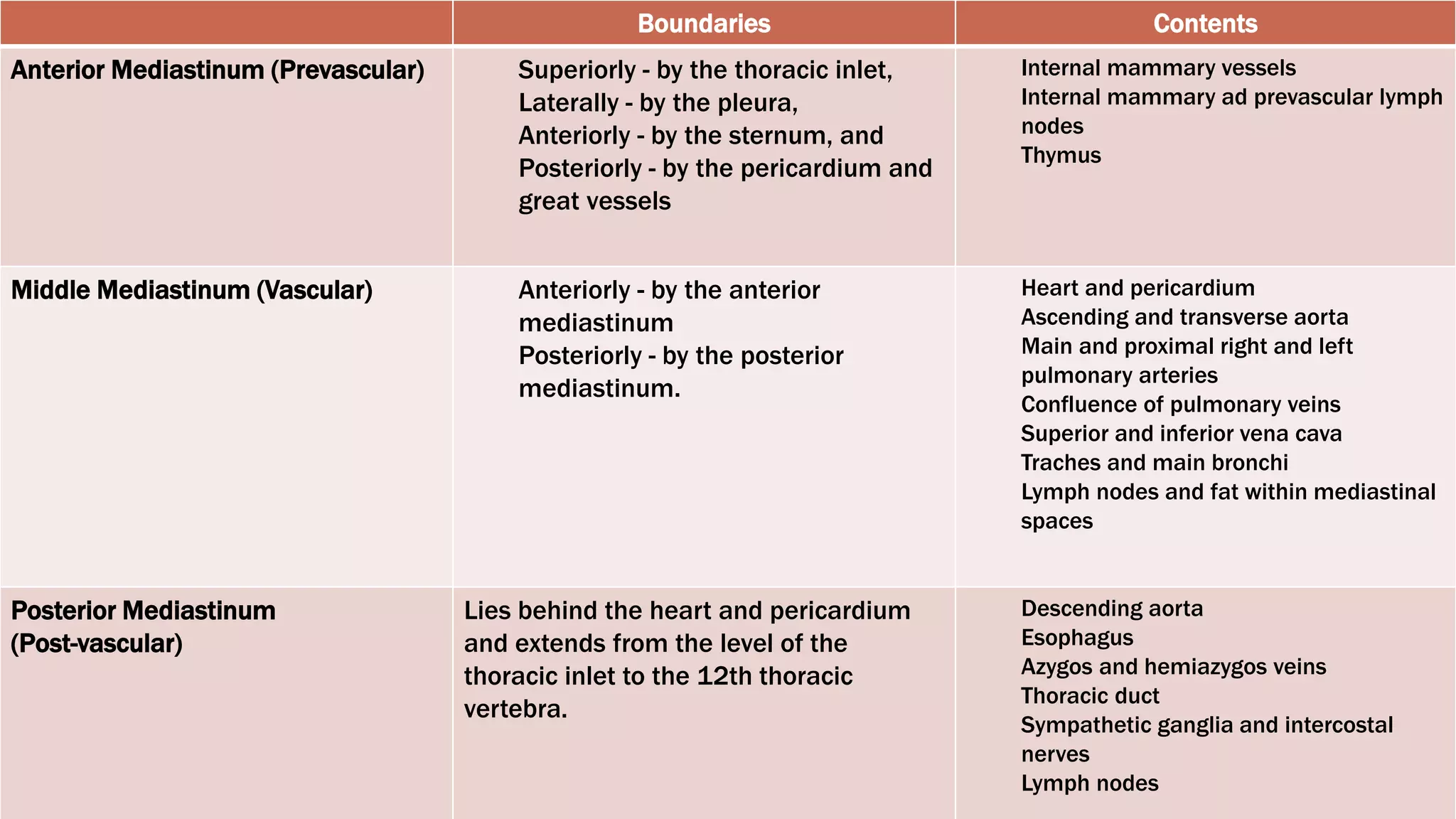
The document defines and describes the mediastinum and its boundaries, divisions, and contents. It also discusses the normal radiographic appearance of structures within the mediastinum, including the heart and vasculature. Key points include that the mediastinum is the central compartment of the thorax bounded by the sternum, vertebrae, and pleura. It is divided into the superior, anterior, middle, and posterior mediastinum and contains structures like the heart, great vessels, trachea and esophagus.