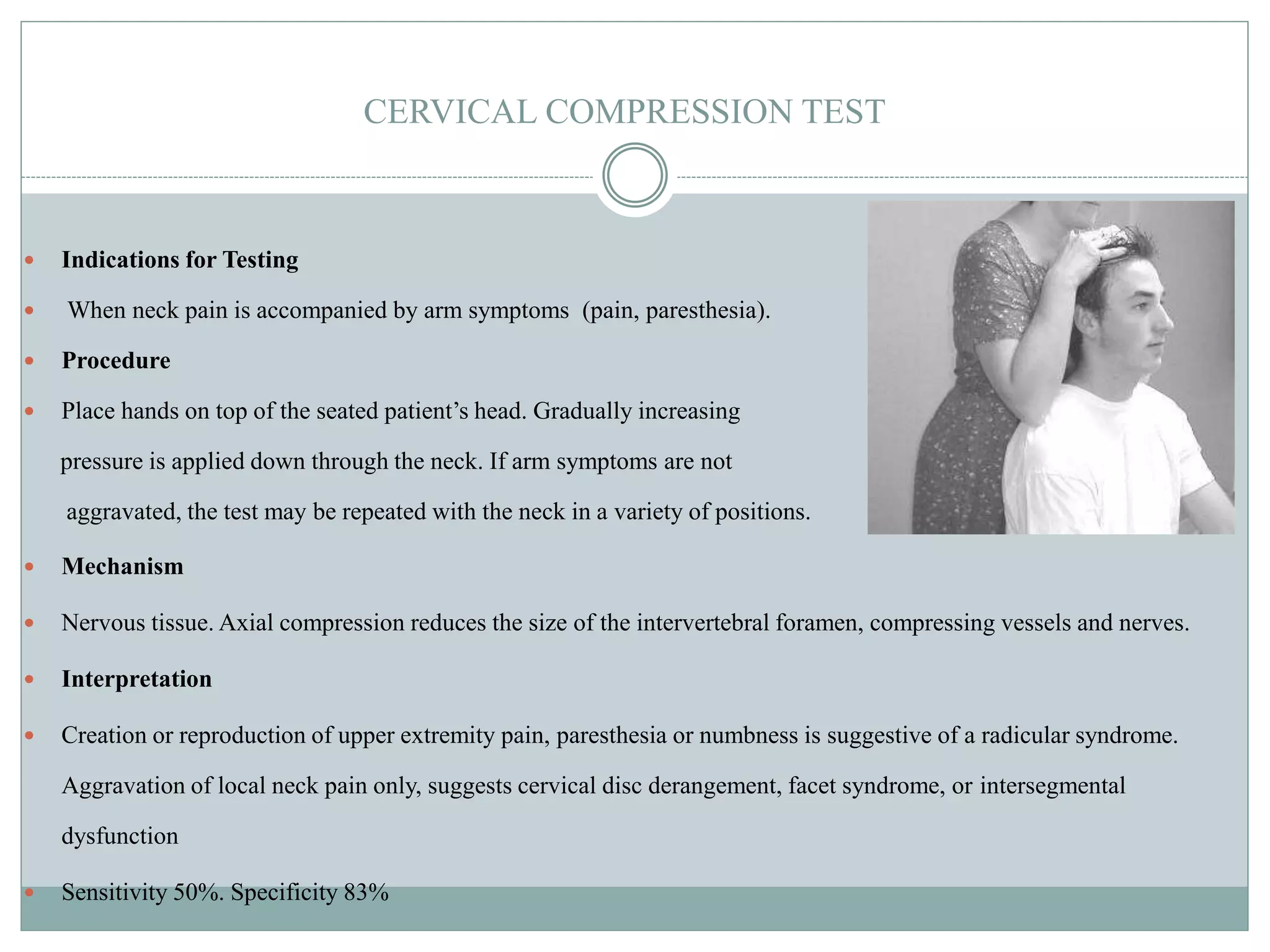
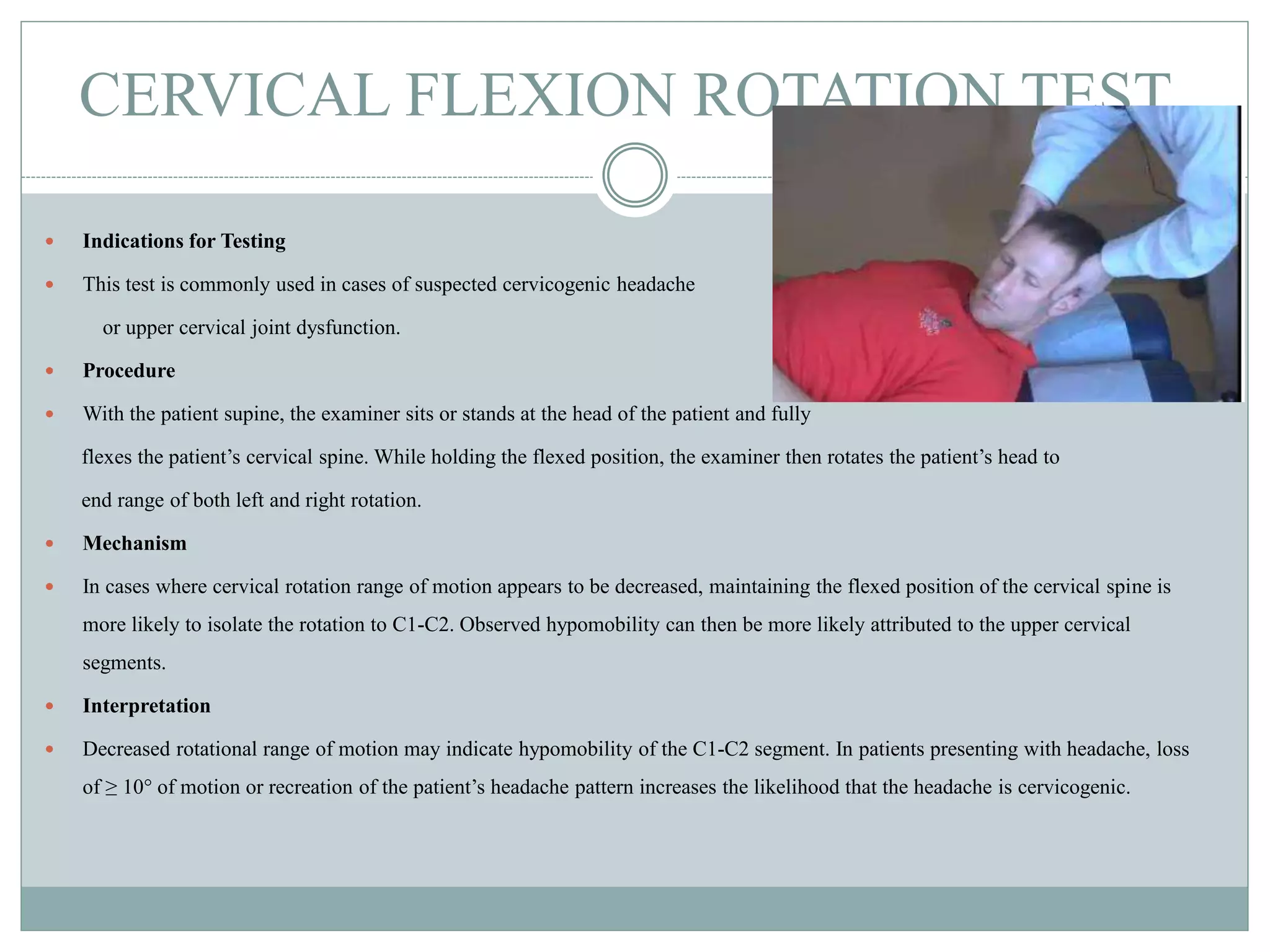
This document provides descriptions of various orthopedic tests of the cervical spine. It describes tests such as cervical compression, flexion, distraction, and resisted muscle tests. For each test, it provides the indications for use, procedures, mechanisms, and interpretations. The tests are used to evaluate patients with neck and arm pain, particularly to identify conditions like radiculopathy or nerve root irritation.