Test bank for community public health nursing evidence for practice 4TH editi...
Liver cirrhosis
1.
2.
3. DEFINITION
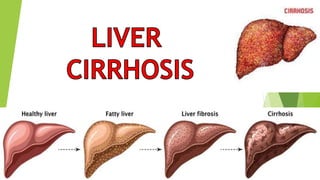
‘’Cirrhosis of liver is a chronic disease characterized by
replacement of normal liver tissue with diffuse fibrosis
that disrupts the structure and function of the liver.’’
4. REMEMBER THIS
Liver cirrhosis is a serious condition because
once the liver becomes cirrhotic, the damage to
the liver is irreversible. This leads to progressive
liver failure, complications of cirrhosis, liver
cancer and eventual death.
5.
6.
7.
8.
9.
10.
11. •Chronic alcohol abuse
•Chronic viral hepatitis (hepatitis B, C and D)
•Fat accumulating in the liver (nonalcoholic fatty liver disease)
•Iron buildup in the body (hemochromatosis)
•Cystic fibrosis
•Copper accumulated in the liver (Wilson's disease)
•Poorly formed bile ducts (biliary atresia)
•Alpha-1 antitrypsin deficiency
CAUSES AND RISK FACTORS
12. •Inherited disorders of sugar metabolism (galactosemia or glycogen storage disease)
•Genetic digestive disorder (Alagille syndrome)
•Liver disease caused by body's immune system (autoimmune hepatitis)
•Destruction of the bile ducts (primary biliary cirrhosis)
•Hardening and scarring of the bile ducts (primary sclerosing cholangitis
•Infection, such as syphilis or brucellosis
•Medications, including methotrexate or isoniazid
16. Hepatic insufficiency may result in the encephalopathy because in ability
of liver to detoxify the toxic substance the by products of metabolism.
Development of collateral blood vessels developed result of portal
hypertension allow elements of portal blood to enter in the systemic
circulation (So the liver cant get the nutrition because collateral vessels
direct bypass the liver).
Normally hepatic encephalopathy is characterized by the elevation of
ammonia level blood and in CSF.
17.
18. Ammonia is produced from the GI tract when the protein is breakdown from the
bacteria, by the liver, by gastric juices and peripheral tissues metabolism) and
another source of ammonia include the ammonia from the kidney in
hypokalaemia and increased dietary protein intake.
Normally the liver converts ammonia on to glutamate which stored in the
liver and later stage this glutamine converted in urea. (This urea excreted
through kidney)
Failure of liver to perform this function may be due to liver cell damage or
necrosis.
That will lead to increase in ammonia and ammonia is a CNS toxins that
affect the glia and nerve cell. It lead to altered CNS metabolism and
function.
25. MEDICAL MANAGEMENT
• Medical management is based on presenting symptoms.
• Treatment includes antacids, vitamins and nutritional supplements,
balanced diet; potassium-sparing diuretics (for ascites); avoidance of
alcohol.
• Colchicine may increase the length of survival in patients with mild
to moderate cirrhosis.
26. •Alcohol-related liver disease: Stop drinking alcohol. Recommendations for
alcohol addiction treatment programs.
•Hepatitis B or C: Several approved antiviral medications are available to treat
hepatitis types B and C.
•Nonalcoholic fatty liver disease: Management of nonalcoholic fatty liver disease
includes losing weight, following a healthy diet, getting physical exercise and
following your provider’s instructions for managing your diabetes.
•Inherited liver diseases: Treatment depends on the specific inherited disease.
Treatments are aimed at treating symptoms and managing complications.
Treatment of alpha-1 antitrypsin deficiency may include medicine to reduce
swelling in your abdomen and legs, antibiotics to treat infections and other
medicines for complications.
27. •Autoimmune hepatitis: Treatment includes medications to suppress your
immune system.
•Diseases that damage or block bile ducts in the liver: Treatments include
medications such as ursodiol (Actigall®) or surgery to open narrowed or
blocked bile ducts.
•Heart failure: Treatment depends on the cause and stage of your heart
failure. Medications include drugs to treat high blood pressure, reduce
cholesterol, remove excess fluids (edema) from your body and improve heart
pumping function. Other treatments include implantation of devices to help
pump blood or monitor heart rhythm, surgeries to unblock arteries or replace
or repair heart valves and transplant surgery to replace your heart.
28. NURSING MANAGEMENT
Promoting Rest
• Position bed for maximal respiratory efficiency; provide oxygen if needed.
• Initiate efforts to prevent respiratory, circulatory, and vascular disturbances.
• Encourage patient to increase activity gradually and plan rest with activity and
mild exercise.
Providing Skin Care
• Change patient’s position frequently.
•Avoid using irritating soaps and adhesive tape.
• Provide lotion to soothe irritated skin; take measures to prevent patient from scratching
the skin.
29. Improving Nutritional Status
• Provide a nutritious, high-protein diet supplemented by Bcomplex vitamins and others,
including A, C, and K.
• Encourage patient to eat: Provide small, frequent meals, consider patient preferences,
and provide protein supplements, if indicated.
• Provide nutrients by feeding tube or total PN if needed.
• Provide patients who have fatty stools (steatorrhea) with water-soluble forms of fat-
soluble vitamins A, D, and E, and give folic acid and iron to prevent anemia.
• Provide a low-protein diet temporarily if patient shows signs of impending or advancing
coma; restrict sodium if needed.
30. Reducing Risk of Injury
• Use padded side rails if patient becomes agitated or restless.
• Orient to time, place, and procedures to minimize agitation.
• Instruct patient to ask for assistance to get out of bed.
• Carefully evaluate any injury because of the possibility of internal bleeding.
• Provide safety measures to prevent injury or cuts (electric razor, soft toothbrush).
• Apply pressure to venipuncture sites to minimize bleeding.
31. • Administer oxygen if oxygen desaturation occurs; monitor for fever or abdominal
pain, which may signal the onset of bacterial peritonitis or other infection.
• Assess cardiovascular and respiratory status; administer diuretics, implement fluid
restrictions, and enhance patient positioning, if needed.
• Monitor intake and output, daily weight changes, changes in abdominal girth, and
edema formation.
• Monitor for nocturia and, later, for oliguria, because these states indicate increasing
severity of liver dysfunction.
Monitoring and Managing Complications
• Monitor for bleeding and hemorrhage.
• Monitor the patient’s mental status closely and report changes so that treatment of
encephalopathy can be initiated promptly.
• Carefully monitor serum electrolyte levels are and correct if abnormal.