2. Introduction
• It is an abnormally increased concentration of
hemoglobin in the blood, either through
reduction of plasma volume or increase in red
cell numbers.
• People with polycythemia have an increase in
hematocrit, hemoglobin or red blood cell count
above the normal limits.
• The term is used when the hematocrit is
elevated (more than 55% in males, more than
50% in females).
3. • An increase in the no of red blood cells = absolute polycythemia
• Due to decrease in the volume of plasma = relative polycythemia
Relative Polycythemia:
• It is an apparent rise of the erythrocyte level in
the blood.
• The underlying cause is reduced blood plasma.
• Relative polycythemia is often caused by loss of
body fluids, such as through burns, dehydration
and stress.
4. Absolute Polycythemia
• Overproduction of RBC may be due to a primary process in the bone
marrow= myeloproliferative syndrome
• May be a reaction to chronically low oxygen levels.
• Over transfusion
5.
6. Relative polycythemia (hemoconcentration) is a high
red cell count due to a decrease in plasma volume
instead of an absolute increase in the number of red
cells.
•Potential causes of relative polycythemia include:
•Isosmotic volume contraction (i.e. diarrhea,
vomiting)
•Hyposmotic volume contraction (i.e. diuretic use,
adrenal insufficiency).
7. • Absolute polycythemia is an abnormally high red cell count
due to an absolute increase in the number of red cells – further
divided into primary and secondary polycythemia.
• Absolute primary polycythemia is due to an abnormality of
hematopoietic precursors. Potential causes of primary
polycythemia include:
• Polycythemia vera (most common)
• Erythropoietin receptor mutations
8. Absolute secondary polycythemia is due to increased secretion of
erythropoietin (EPO) – further divided
into compensatory and abnormal polycythemia.
•Compensatory (appropriate) polycythemia occurs when there is an
increase in EPO in response to tissue hypoxia. Some causes of
compensatory polycythemia include:
•Cyanotic heart disease (right-to-left shunts)
•Pulmonary disease
•Abnormal hemoglobin function
•Altitude sickness (low partial pressure of O2
9. •Abnormal (inappropriate) polycythemia occurs when there is an
increase in EPO in the absence of tissue hypoxia.
•Inappropriate polycythemia can be seen in paraneoplastic
syndromes of the following EPO-secreting pathologies:
•Hemangioblastoma
•Hepatocellular carcinoma
•Leiomyoma (Benign smooth muscle tumor usually in the
uterus)
•Pheochromocytoma
•Renal cell carcinoma
•Hydronephrosis
10.
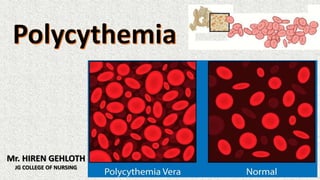
11. • Polycythemia Vera (PV) is a chronic myeloproliferative
disorder characterized by increased RBC volume, and
hyperviscosity syndrome.
• A mutation in the JAK-2 gene causes constant stimulation of
the erythropoietin-receptor in erythrocyte progenitors.
• All cell lines are increased, but erythrocytosis is the most drastic.
Polycythemia Vera
12. • Patients typically have a ruddy complexion and splenomegaly.
• The symptoms are due to the increased blood volume (headache,
dizziness, tinnitus, fatigue, paresthesias, and blurred vision) or to
increased blood viscosity (angina, claudication, dyspnea, and
thrombophlebitis).
• Blood pressure and uric acid are often elevated, and pruritus is another
common and bothersome complication.
• Erythromelalgia (a burning sensation in the fingers and toes) may be
reported.
CLINICAL MANIFESTATION
13. DIAGNOSTIC EVALUATION
• Diagnosis is based on an elevated erythrocyte mass, a normal oxygen saturation level,
and often an enlarged spleen.
• Other factors useful in establishing the diagnosis include elevated leukocyte and
platelet counts.
• The mutation of the enzyme JAK2 causes an
erythrocyte hypersensitivity to the effects of
erythropoietin.
• Although a mutation in JAK2 is found in the
majority of people with polycythemia vera, it
is not specific for the disease
14. Medical Management
The objective of management is to reduce the high red blood
cell mass.
• Phlebotomy is performed repeatedly to keep the hemoglobin
within normal range; iron supplements are avoided.
• Chemotherapeutic agents are used to suppress marrow
function (may increase risk for leukemia).
• Anagrelide (Agrylin) may be used to inhibit platelet
aggregation and control the thrombocytosis related to
polycythemia.
15. • Interferon alpha-2b (Intron-A) is the most effective treatment
for managing the pruritus associated with polycythemia vera.
• Antihistamines may be administered to control pruritus (not
very effective).
• Allopurinol is used to prevent gouty attacks when the uric
acid level is elevated.
16. Nursing Management
• Assess risk factors for thrombotic complications and teach patient to
recognize signs and symptoms of thrombosis.
•Discourage sedentary behavior, crossing the legs, and wearing tight
or restrictive clothing (particularly stockings) to reduce the likelihood
of DVT.
• Advise patient to avoid aspirin and medications containing aspirin (if
patient has a history of bleeding).
• Advise patient to minimize alcohol intake and avoid iron and
vitamins containing iron.
• Suggest a cool or tepid bath for pruritus, along with cocoa butter–
based lotions and bath products to relieve itching.