
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Cirrhosis of liver ppt
Similar to Cirrhosis of liver ppt (20)
Recently uploaded
Recently uploaded (20)
Cirrhosis of liver ppt
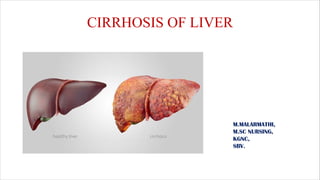
- 1. CIRRHOSIS OF LIVER M.MALARMATHI, M.SC NURSING, KGNC, SBV.
- 3. • The liver is located in the upper right-hand portion of the abdominal cavity, beneath the diaphragm, and on top of the stomach, right kidney, and intestines. • Shaped like a cone, the liver is a dark reddish-brown organ that weighs about 1.5 kg. • The liver consists of 2 main lobes. Both are made up of 8 segments that consist of 1,000 lobules (small lobes). These lobules are connected to small ducts (tubes) that connect with larger ducts to form the common hepatic duct. • The common hepatic duct transports the bile made by the liver cells to the gallbladder and duodenum (the first part of the small intestine) via the common bile duct.
- 4. • Production of bile, which helps carry away waste and break down fats in the small intestine during digestion • Production of certain proteins for blood plasma • Production of cholesterol and special proteins to help carry fats through the body • Conversion of excess glucose into glycogen for storage (glycogen can later be converted back to glucose for energy) and to balance and make glucose as needed. • Regulation of blood levels of amino acids, which form the building blocks of proteins. • Processing of hemoglobin for use of its iron content (the liver stores iron) • Conversion of poisonous ammonia to urea (urea is an end product of protein metabolism and is excreted in the urine) • Clearing the blood of drugs and other poisonous substances
- 5. DEFINITION Cirrhosis of liver is a chronic, progressive disease characterized by widespread fibrosis (scaring) & nodule formation. Cirrhosis occurs when the normal flow of blood, bile, & hepatic metabolites is altered by fibrosis.
- 6. ETIOLOGY Chronic alcohol intake Hepatitis B and C Autoimmune hepatitis Wilson’s disease Haemochroma tosis Alpha 1 antitrypsin. Glycogen storage diseases cystic fibrosis Biliary obstruction ETIOLOGY
- 7. TYPES OF CIRRHOSIS OF LIVER Alcoholic cirrhosis Postnecrotic cirrhosis Biliary cirrhosis Cardiac cirrhosis
- 8. Alcoholic cirrhosis (Laennec’s cirrhosis, micronodular, portal cirrhosis) • Most common, due to chronic alcoholism. First stage alcohol intake is an accumulation of fat in the liver cells. If the alcohol abuse continues, widespread scar formation occurs throughout the liver.
- 9. Postnecrotic cirrhosis • There are broad bands of scar tissue due to late results of toxic, autoimmune or viral hepatitis. Broad bands of scar tissue from within the liver
- 10. Biliary cirrhosis • Scaring occurs around bile duct in liver, Results from chronic biliary obstruction & infection. There is diffuse fibrosis of the liver with jaundice main feature. Cardiac cirrhosis • Associated with severe right sided long term heart failure, fairly rare.
- 11. PATHOPHYSIOLOGY Due to etiological causes Primary event is injury to hepatocellular elements Initiates inflammatory response with cytokine release->toxic substances Destruction of hepatocytes, bile duct cells, vascular endothelial cells
- 12. Repair through cellular proliferation and regeneration Formation of fibrous scar Clinical features
- 13. STAGES OF LIVER DAMAGE
- 15. DIAGNOSTIC EVALUATION History collection Physcial examination Liver biopsy CT scan Liver ultrasound Gastroscopy
- 16. History collection. • History collection findings shows that previous history of viral, toxic, or idiopathic hepatitis, chronic biliary obstruction and infection, severe right sided heart failure • Functional health patterns any history of chronic alcoholism, weakness, fatigue. • Elimination dark urine,decrease urine output,flatulence, changes in bowel habits. • Cognitive perceptual Dull, right upper quadrant or epigastric pain.etc one history reveals Cirrhosis of liver.
- 17. Physcial examination • In the abdomen in chronic liver disease include: collateral circulation of the abdominal wall around the umbilicus, bruising, hepatomegaly, splenomegaly, abdominal distension (particularly in the flanks) with shifting dullness and fluid thrill secondary to ascites, hepatic bruit, • S p i d e r n e v i , p a l m a r e r t h y e m a , c a p u t medusa,mehrcke nails, terry nails reveals cirrhosis of liver.
- 18. Lab findings • The following findings are typical in cirrhosis: Aminotransferases - AST and ALT are moderately elevated, with AST > ALT. However, normal aminotransferases do not preclude cirrhosis. • Alkaline phosphatase - usually slightly elevated. GGT -- correlates with AP levels. Typically much higher in chronic liver disease from alcohol. Bilirubin - may elevate as cirrhosis progresses. • Albumin - levels fall as the synthetic function of the liver declines with worsening cirrhosis since albumin is exclusively synthesized in the liver. • Prothrombin time- increases since the liver synthesizes clotting factors. • Globulins - increased due to shunting of bacterial antigens away from the liver to lymphoid tissue. Serum sodium - hyponatremia due to inability to excrete free water resulting from high levels of ADH and aldosterone. • Thrombocytopenia - due to both congestive splenomegaly as well as decreased thrombopoietin from the liver. However this rarely results in platelet count < 50,000/mL. • Leukopenia and neutropenia- due to splenomegaly with splenic margination. • Coagulation defects - the liver produces most of the coagulation factors and thus coagulopathy correlates with worsening liver disease.
- 19. Liver biopsy Is a medical procedure in which a small amount of liver tissue is surgically removed so it can be analyzed in the laboratory by a pathologist. Liver biopsies are usually done to detect the presence of abnormal cells in the liver, like cancer cells, or to evaluate disease processes such as cirrhosis.
- 20. • CT scan This procedure combines special x-ray equipment with sophisticated computers to produce multiple, digital images or pictures of the liver. It can help determine the severity of cirrhosis as well as other liver diseases. See "Radiation Dose in X-Ray and CT Exams" for more information.
- 21. • Liver ultrasound Is a type of imaging exam that uses sound waves to create pictures of the inside of the abdomen and/or pelvis, including images of the liver. Doppler ultrasound allows for evaluation of blood flow to and from the liver.
- 22. Gastroscopy • Endoscopic examination of the esophagus, stomach and duodenum is performed in patients with established cirrhosis to exclude the possibility of esophageal varices. If these are found, prophylactic local therapy may be applied (sclerotherapy or banding) and beta blocker treatment may be commenced. Rarely diseases of the bile ducts, such as as primary sclerosing, can be causes of cirrhosis. Imaging of the bile ducts, such as ERCP or MRCP (MRI of biliary tract and pancreas) can show abnormalities in these patients, and may aid in the diagnosis.
- 23. Non pharmacological management Ø Rest Ø Avoidance of alcohol and anticoagulants management of ascites Ø Administration of 300 calorie, high carbohydrate, protein, low fat diet, low sodium diet for ascites.
- 24. Diuretic therapy is an important part of management. • Spironolactone • A high potency loop diuretic. • Chlorothiazide may be used.
- 25. Needle puncture of the abdominal cavity may be performed to remove ascitic fluid.
- 26. Peritoneovenous shunt is a surgical procedure that provides continous reinfusion of ascitic fluid.
- 27. Non pharmacological management • Fist step is initated stabilize the patient and manage the airway. • Iv therapy is initated and may include administration of blood products. pharmacological management • B- Blockers • Octreotide • Vasopressin • Vitamin K
- 28. BALLOON TAMPONADE: Balloon tamponade controls the h e m o r r h a g e b y m e c h a n i c a l compression of the varices. It may be used in patients with acute esophageal or gastric variceal hemorrhage that can not be controlled on initial endoscopy.
- 29. Endoscopic sclerotherapy SCLEROTHERAPY: It involves injection of a sclerosant solution into the varices through an injection needle that is placed through the endoscope.
- 30. ENDOSCOPIC BAND LIGATION Endoscopic variceal ligation or banding is performed by placing a small rubber band around the base of the varix(enlarged vein).
- 31. • Non Pharmacological management • The goal of management of hepatic encephalopathy is the reduction of ammonia. • With improvement of mental function, dietary protein content is increased gradually over days. • Electrolytes and acid imbalance should as be treatment.
- 32. • Lactulose • Antibiotics • B- Blockers • Octreotide • Vasopressin • Vitamin K • Spironolactone • Furosemide • Chlorothiazide.
- 33. Liver transplantation may be considered in patient with recurrent hepatic encephalopathy and end stage liver disease.
- 34. Nursing management • Monitor the hemodynamic parameter • Monitor I/O, daily weight • Monitor prothrombin time, bleeding time • Provide adequate rest. • Patient level of conscious • Restrict fluids & sodium if there is edema or ascites • Provide adequate nutrition & hydration • Fluid and eletrolyte imbalance • Acid base balance • Monitor the respiratory status • Provide adequate intake of nutrients • Maintenance of normal body weight • Maintenance of skin integrity • Advice the patient cessation of alcohol.
- 35. • Provide comfort measures such as back rubbing &changing position to relieve pain • Teach the patient relaxation techniques like deep breathing • Provide quiet and calm environment. • Give analgesics to relieve form pain and fever. • Evaluate pt’s current activity tolerance and adjust activity and reduce intensity of task that may cause undesired physiological changes. • Help and encourage patients to eat,Feed the patient when fatigue or let someone nearby to help patients.
- 36. • Keep head of bed elevated to facilitates breathing by reducing pressure on the diaphragm • Restrict intake of caffeine, gas-producing or spicy and excessively hot or cold foods to aids in reducing gastric irritation &abdominal discomfort that may impair oral intake /digestion. • Protect pt. from bleeding, monitor urine, stool, gums, skin for signs of bleeding/ bruising • Teach pt. to use soft toothbrush,avoid constipation • Administer Vit. K as ordered.
- 37. THANK YOU