Downloaded 156 times
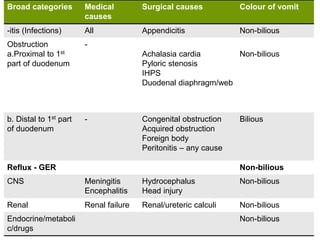



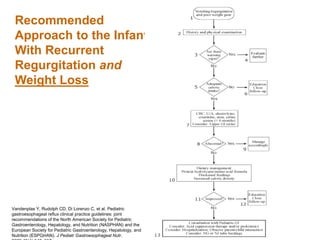
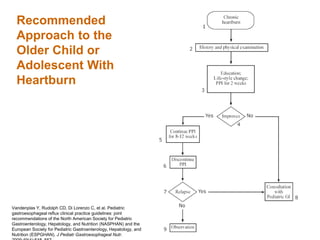



The document discusses causes and types of vomiting in children, categorizing them into medical and surgical causes, with emphasis on gastroesophageal reflux (GER) and gastroesophageal reflux disease (GERD). It details diagnostic approaches, management strategies including conservative and surgical options, and highlights the importance of lifestyle changes for controlling symptoms. The document also provides a framework for differentiating between physiological and pathological reflux in pediatric populations.











































































































