2. JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
It is the most common cyanotic heart defect, and the
most common cause of blue baby syndrome
It was described in 1672 by Niels Stensen, in 1773 by
Edward Sandifort, and in 1888 by the French physician
Étienne-Louis Arthur Fallot, after whom it is named.
3. TOF is the most common type of cyanotic congenital heart
disease. There are several forms of this defect, the
common ones are :
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
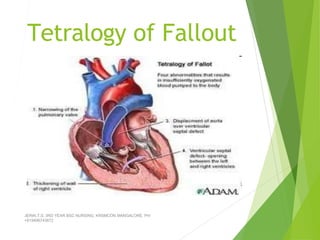
1) Obstruction to right ventricular outflow (pulmonary
stenosis)
Ventricular septal defect ( VSD )
Dextral position of the aorta with septal override/
overriding of aorta
Right ventricular hypertrophy
2)
3)
4)
4. Pathophysiology
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
► Pulmonary stenosis and VSD are the
most vital abnormalities in TOF. The
defect largely depends on the stenosis
of pulmonary artery, VSD size,
pulmonary & systemic resistance to
the blood flow.
► If pulmonary artery resistance is more
than systemic, right to left shunt.
► If systemic vascular resistance is more
than pulmonary artery resistance, left
to right shunt.
5. Blood from systemic circulation
Right atrium
Right ventricle ( through VSD)and pulmonary artery resistance
Left ventricle and Aorta
Right to left shunt
Cyanosis
Polycythemia ( compensation)
Increased viscosity of the blood
Slowing down of circulation
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
CVA
+919496743672
6. Clinical features
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Cyanosis:
Neonates may not be cyanotic if the defects are very small ( because of
PDA)
Cyanosis becomes evident after the ductus closes during the 1stmonth
of life.
Its evident in mucus membrane of mouth, lips, fingernails, & toe nails.
Initially it is seen only during crying and exertion later seen even at rest
Clubbing occurs by 1- 2 yrs
7. JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Severe dyspnoea on exertion or exercise
Rest in between the activities ( as compensation to reduce demand for 02)
(they sit or lie down after a brief active play)
Knee chest position by infants
Squatting position by older children
9. Paroxysmal dyspnoic attack
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
( anoxic “blue” spells) ( TET spells) (hypercyanotic spell)
➢ An episode of intense cyanosis that occurs
predominantly in morning after awakening from
sleep, during or after crying, during or after
defecation, during or following feeding
➢ Child starts crying becomes Dyspnoic & restless
➢ Gasps for breath
➢ Weak cry followed by sleep
Some times may cause convulsions and
unconsciousness
11. ► Prolonged episodes may
lead to
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
➢
➢
➢
➢
Unconsciousness
Convulsions
Hemiparesis
Death
12. JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Slow growth and development
Slow mental development because of tissue hypoxia of brain
On auscultation murmurs heard
Radiography shows enlarged ventricles on right side, large aorta &
decrease size of pulmonary artery.
Cardiac catheterization shows hypertension in right ventricle
13. Diagnostic measures
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
1.
2.
3.
4.
5.
6.
Hematocrit increased-Polycythemia
ECG: shows right axis deviation
2D Echocardiography, color flow mapping & doppler
Cardiac catheterization
Ventriculography
Chest X-ray: reveals oligemic lung fields (poorly vascularized lungs) a
small boot shaped heart with the tip of the boot turned up above the
diaphragm.
15. Medical Management
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
1. Prostaglandin E (0.05-0.20 g/kg/min) IV to
maintain the patency of ductus
2. Management of spells, mild sedative like
promethazine reduces the frequency of spells,
provided it is given regularly.
3. Oral propranolol 0.5-1mg/kg oral every 6hrly
4. Treatment of iron deficiency anemia and
dehydration
5. Antibiotic therapy for bacterial infection
16. Management of TETspells
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
1)Treated with beta-blocker such as
propranolol, but acute episodes may
require rapid intervention with morphine
to reduce ventilatory drive and a
vasopressor such as epinephrine,
phenylephrine, or norepinephrine to
increase blood pressure.
2)Oxygen (100%) is effective in treating
spells because it is a potent pulmonary
vasodilator and systemic vasoconstrictor.
This allows more blood flow to the lungs.
17. Conti………
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
There are also simple procedures such as squatting and the
knee chest position which increases aortic wave
reflection, increasing pressure on the left side of the
heart, decreasing the right to left shunt thus decreasing
the amount of deoxygenated blood entering the
systemic circulation.
18. Stepwise management of
hypercyanotic spells
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
1) Put the child in knee chest position
2) Provide humidified O2-6-8L/min
3) Inject Morphine 0.1-0.2mg/kg S/C
4) Obtain arterial pH. If less than 7.3,
administer NaHCO3 1ml/kg diluted 1:1 in
distilled H2O IV
5) Give propranolol 0.1mg/kg IV during spell,
followed by 1mg/kg/day orally
6) Correct anemia by packed cell transfusion.
Start the child on long term oral iron
therapy.
19. Surgical management
palliative surgeries
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
To increase the pulmonary blood circulation
1. Waterson shunt: a side to side anastomosis of the
ascending aorta and right pulmonary artery in
neonates
Blalock taussig procedure: for older infants and
children, in which an artificial ductus is created by
anastomosis of a branch of the aorta ( subclavian
artery) to the pulmonary artery.
2.
20. Modified Blalock-Taussig Shunt:by using Gortex Graft.
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Avoid BP measurements and venipunctures in the affected arm after a
Blalock-Taussig shunt. Pulse will not be palpable in that arm because of
use of the subclavian artery for the shunt.
21. 3.
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Potts procedure: anastomosis of the upper descending aorta and left
pulmonary artery
4. Brock procedure: is a direct operation, pulmonary valvotomy or
infundibular resection, for the pulmonary stenosis. This operation
increases pulmonary blood flow but does not correct the ventricular
septal defect.
23. Total surgical repair
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Surgery is now often carried out in
infants one year of age or younger with
less than 5% perioperative mortality.
► The open-heart surgery is designed
(1) to relieve the right ventricular outflow
tract stenosis by careful resection of
muscle and
(2) to repair the VSD with a Gore-Tex patch
or a homograft. Additional reparative or
reconstructive surgery may be done on
patients as required by their particular
cardiac anatomy.
24. Corrective surgery
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Aims:
To close the VSD
To correct the pulmonary artery stenosis by
valvotomy
To close the already created shunts
monitor for ventricular arrhythmias after corrective
repair.
26. Transposition of the Great
Arteries
TGA
TGA occurs when the pulmonary artery originates from the
left ventricle and the aorta originates from right
ventricle.
Accounts for 5% of total CHD
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
27. Hemodynamics
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
► The defect results in 2 separate
circulations
► The right side of the heart manages the
systemic circulation
► The left side of the heart manages
pulmonary circulation
► To sustain life there must be
accompanying defects (shunts) where
oxygenated blood mixes with
deoxygenated blood like ASD, VSD, OR
PDA
28. Pathophysiology
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Blood from the systemic circulation
Rt atrium, & Rt ventricle
Aorta
Deoxygenated blood supplied to the body
Cyanosis
Polycythemia
Thrombi
CVA
29. Oxygenated blood from the lungs
Lt Atrium, Lt Ventricle
Pulmonary artery
Again circulates to the lung
But
when there is Shunt for mixing of oxygenated & deoxygenated blood
Delays cyanosis
But
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
these associated defects can lead to increased pulmonary blood flow that
increases pressure in the pulmonary circulation
CCF
30. Clinical features
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Depends upon the inter circulatory
mixing
► Cyanosis
► Clubbing
► CCF
► Easy fatigability
► Slow weight gain
► Failure to thrive
► Frequent chest infections
► Tachypnea
► Cardiomegaly
31. Diagnosis
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Auscultation- systolic murmur
Chest X-ray- cardiomegaly with a typical egg-on-side
shaped heart. Pulmonary vascular markings are
increased
ECG shows right axis deviation, right or biventricular
hypertrophy
Cardiac catheterization shows O2 saturation
2D`echo reveals transpositions
33. Nursing measures
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Administer prostaglandins to maintain the open state of
the ductus arteriosus, which will allow the mixing of
poorly oxygenated blood with well oxygenated blood
Monitor for rapid respiration and cyanosis
Administer oxygen as needed preoperatively.
Treat CCF timely
34. Surgical management
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
►Palliative – by balloon atrial septotomy
Is done soon after diagnosis to enlarge
the atrial septum. And it is successful
only when done within 6-12 weeks.
► Definitive- by arterial switch operation
or by redirecting the blood flow
Mustard or Senning procedure:in which
pulmonary venous blood is redirected
to the right ventricle and systemic
venous blood is redirected to the left
ventricle.
35. 2) Jantene’s switch operation: the pulmonary artery and aorta are
transected. The distal aorta is anastomosed to the proximal pulmonary
stump and the pulmonary artery to the proximal aortic stump. The
coronary arteries are shifted to aorta. This surgery is preferred over other
surgery.
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
36. Complications
JERIN.T.S, 3RD YEAR BSC NURSING, KRSMCON MANGALORE. PH:
+919496743672
Infective endocarditis
Brain abscess and CVA due to thrombi or severe hypoxia