
Recommended
More Related Content
Similar to Anorectal Malformation - A Guide to Imperforate Anus
Similar to Anorectal Malformation - A Guide to Imperforate Anus (20)
More from GrashiaBlessy1
More from GrashiaBlessy1 (20)
Recently uploaded
Recently uploaded (20)
Anorectal Malformation - A Guide to Imperforate Anus
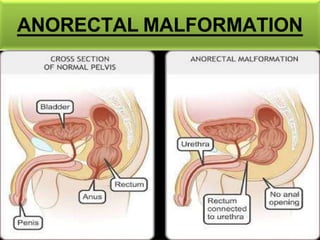
- 2. ANORECTAL MALFORMATION Definition: Anorectal malformation comprise a wide variety of defects involving distal anus and rectum as well as the urogenital tract. It involves an arrest of rectal descent resulting in absence of an anal opening which occurs during the 4th- 16th week of gestation.
- 3. INCIDENCE & ETIOLOGY: Minor abnormalities (1 in 500 live births) Major abnormalities (1 in 5000 live births) Boys commonly affected than girls. Etiology is unclear, Mutation in the genes responsible for this disorder.
- 4. PATHOPHYSIOLOGY: Resulting in Anorectal Anomaly Union of anus and rectum does not occur If the membrane that separates anus and rectum is not absorbed By the 7th week of gestation membrane separates the rectum from anus Genitourinary tract originates from the embryonic structure called CLOACA
- 5. CLASSIFICATION: There are basically 4 types of Anorectal anomalies: 1) ANAL STENOSIS 2) ANAL MEMBRANE ATRESIA 3) RECTAL ATRESIA 4) ANAL AGENESIS/ IMPERFORATE ANUS LOW IMPERFORATE ANUS INTERMEDIATE IMPERFORATE ANUS HIGH IMPERFORATE ANUS
- 7. DIAGNOSTIC EVALUATION: Detection of imperforate anus can be done at birth, on following findings: i. No anal opening ii. Gloved finger or thermometer cannot be inserted into infant rectum iii. No history of passage of meconium iv. Presence of abdominal distension v. Presence of meconium in urine, indicating rectovaginal fistula.
- 8. To find out the distance between blind end of rectum and anal dimple following investigation are done: 1) Invertogram 2) Abdominal ultrasound 3) Intravenous pyelogram (kidney, ureter, urinary bladder)
- 9. MANAGEMENT: Two aspect must be considered during the first 24- 28 hours of life: First is the presence of associated anomalies that may threaten the baby life. Severity of defect Surgical procedure depends on the types of anomaly Anoplasty Temporary colostomy Posterior sagittal anorectoplasty (PSARP) OR Pena’s procedure
- 10. NURSING MANAGEMENT: Pre- operative nursing care: i. After birth, as soon as the anomaly is noticed, oral feeding should be withheld. ii. I/V fluids are started to meet nutritional requirement iii. Abdominal girth should be measured. iv. Gastric compression should be done by nasogastric aspiration. v. Monitor vital signs, prepare the family psychologically for infant’s surgery.
- 11. Post- operative care: i. I/V fluids are to be continued. ii. Nasogastric suction is continued. iii. Oral feeding are started when peristalsis returns.