Frontal and Parietal lobe signs explained
•Download as PPTX, PDF•
0 likes•696 views

1) The document discusses signs associated with lesions in the frontal and parietal lobes. Tests are described to assess functions localized to these regions like motor skills, memory, attention, and language abilities. 2) Parietal lobe signs include sensory deficits, agnosias like finger agnosia, and apraxias involving how to complete tasks. Tests evaluate two-point discrimination, graphesthesia, and stereognosis. 3) Both lobes are involved in executive functions and attention. Tests mentioned include the Wisconsin Card Sorting Test, Trail Making Test, and Stroop Test.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Frontal and Parietal lobe signs explained
Similar to Frontal and Parietal lobe signs explained (20)
More from Dr Fakir Mohan Sahu
More from Dr Fakir Mohan Sahu (20)
Recently uploaded
Recently uploaded (20)
Frontal and Parietal lobe signs explained
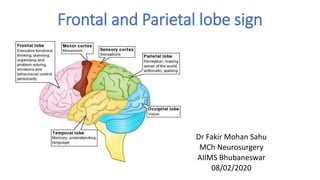
- 1. Frontal and Parietal lobe sign Dr Fakir Mohan Sahu MCh Neurosurgery AIIMS Bhubaneswar 08/02/2020
- 3. Functional region of the frontal lobe • I Primary motor area • II. Premotor area • III. Frontal eye fields • IV. Dorsolateral prefrontal cortex • V. Orbital and basal areas • VI. Supplementary motor area and anterior cingulated gyrus area
- 4. Clinical Assessment of frontal lobe sign • History, Examination and formal tests : Abnormal behavior, speech disorder, urinary incontinence, Frontal gait(magnetic gait) , weakness of limbs • Test sense of smell. • Frontal release reflexes Grasp reflex Sucking reflex (pout, snout, rooting) Palmo-mental reflex Glabellar tap reflex
- 5. Emotional make-up and personality is best assessed by history from family / friends & observation. •Abstraction and judgment are assessed by proverb interpretation and similarities. •E.g explain in your own words the meaning of •Don’t cry over spilled milk •Similarity between mango and orange, car and airplane.
- 6. Attentionand memory • Alternative sequence (e.g. copying MNMN)- Attention • Motor Luria’s ‘fist-edge-palm’ test • Go/no-go • Digit span test: Measure of short term memory
- 9. To assess perseveration and abstract thinking. Measure of executive function. Consists of four key cards and 128 response cards. Wisconsin Card Sorting Test(WCST)
- 10. Trail Making Test • Test for visual attention and task switching. . • In Part A, the circles are numbered 1 – 25 • In Part B, the circles include both numbers (1 – 13) and letters (A – L); (i.e., 1-A-2-B-3-C, etc.).
- 11. Trail Making Test A C1 2 7 3 D 5 B 4 6
- 12. Stroop test
- 14. • CORTICAL SENSORY SYNDROMES • ASOMATAGNOSIAS • APRAXIAS • VISUAL DISORDERS • AUDITORY NEGLECT Parietal lobe lesion and sign
- 15. Tests for cortical sensations A. Two point discrimination : Calipers or compass used. Sites – Palms (8-15 mm) Dorsum (2-3cm) Back (3-4 cm).
- 16. B. Graphesthesia : Done with pencil or swab stick. sites – palms, fingers and face. C. Stereognosis : • No preliminary visual demo given. • ex: key, pen or coin
- 17. ASOMATAGNOSIAS • Inability to feel, recognize, or be conscious of one’s own specific body parts or bodily conditions. ANOSAGNOSIA • Denial of illness HEMI NEGLECT • Neglect on one side of body in dressing and grooming.
- 18. GERSTMANN SYNDROME1. Finger agnosia 2. Right-left confusion 3. Acalculia 4. Dysgraphia
- 19. Tests for finger agnosia • Inability to name , point or recognize fingers on oneself or others. 1. Non verbal finger recognition 2. Verbal finger recognition
- 20. Tests for right – left confusion Identification on self . Crossed commands on self Identification on examiner Crossed commands on examiner .
- 21. Tests for calculations Components – Rote tables (add, multiply, etc) Recognition of signs (+ , - , * ) Basic arithmetic(carrying, borrowing) Spatial alignment of written calculations • Verbal rote examples : what is 4 plus 6 ? • Verbal complex examples : what is 21 / 5 ?
- 22. • Written complex examples : • Pt with rt. hemisphere lesion & left neglect. • Pt with rt. parietal hematoma – showing poor alignment and calculation errors.
- 23. APRAXIA AND PARIETAL LOBE • An inability to carry out a commanded task despite the retention of motor and sensory function
- 24. Types of apraxia 1. Ideomotor apraxia 2. Ideational apraxia 3. Bucco-facial apraxia 4. Constructional apraxia 5. Dressing apraxia
- 25. IDEOMOTOR APRAXIA (“how to do”) • Most common type of apraxia i. Buccofacial apraxia ii. Limb apraxia iii. Whole body apraxia
- 26. IDEATIONAL APRAXIA (“what todo”) • Able to do individual tasks, but cann't integrate them as a whole. • ‘Conceptual apraxia’ - inability to recognise the use of objects. (object agnosia)
- 27. CONSTRUCTIONAL APRAXIA • Constructional ability/praxis (visuoconstructive ability) • Non dominant parietal lobe • Area 17 IPL (kinesthetic analysis of visual patterns done here) Premotor area
- 28. DRESSING APRAXIA • Not a true apraxia. • Combination of spatial disorientation and visuospatial inattention.
- 29. VISUAL DISORDERS • Optic radiation passes through Inferior part of the parietal lobe – incongruous homonymous hemianopia or an inferior quadrantanopia. • Rt. angular gyrus - Left sided visual neglect.
- 30. AUDITORY NEGLECT • In right parietal lesions are initially unresponsive to voices or noises on the left side. • Main lesion - right superior lobule.
- 31. Thank you
Editor's Notes
- The dorsolateral frontal cortex is concerned with planning, strategy formation, and executive function. The frontal operculum contains the centre for expression of language. The orbitofrontal cortex is concerned with response inhibition Broca's area: expressive language, i.e. language production. Frontal eye field area :Voluntary eye movements
- The primitive reflexes are present in normal babies. As the CNS matures, frontal lobe cells develop and begin to inhibit these reflexes. They may reappear with brain damage or disease
- Attention is the patient’s ability to attend to a specific stimulus without being distracted by external, internal or environmental stimuli. An example is to ask the patient to tap the knee when the examiner says "Stop" and not to tap when the examiner says "Go" “repeat 3-5; 7-5-8; 3-9-4-8..” N: >5 increasing sequence of no A two year child has a digit span of 2, 3yr- 3, 4yr- 4, 5yr- 5, 6yr-6 and 7yr to adult- 7
- Using A F S normal individual more than 10 also check for repitation no less than 8 abnrmal
- Trail Making Test consist of 25 circles distIn Part A, the circles are numbered 1 – 25, and the patient should draw lines to connect the numbers in ascending order. ributed over a sheet of paper In Part B, the circles include both numbers (1 – 13) and letters (A – L); as in Part A, the patient draws lines to connect the circles in an ascending pattern, but with the added task of alternating between the numbers and letters (i.e., 1-A-2-B-3-C, etc.).
- Test of inhibition response Patients are asked to state the color in which words are printed rather than the words themselves failed inhibition
- PRIMARY SOMASTHETIC AREA Body image representation SOMASTHETIC ASSOCIATION AREA Body in space and Tactile discrimination SUPERIOR PARIETAL LOBULE connections with all lobes) Visual spatial properties Visual attention, 3 D analysis of body space interactions cingulate gyrus and prefrontal cortex . Therefore they mediate influence of emotion, attention and motivation INFERIOR PARIETAL LOBULE reading , calculations Angular gyrus & Supra marginal gyrus- they have interconnections with visual, auditory, somasthetic, supr. colliculus, LGB and other lobes
- Cortical defect is essentially to one of sensory discrimination i.e impaired ability to integrate and localize stimuli. Inability to recognize part of one’s body.
- Ask pt. to close both eyes – respond as ‘one’ or ‘two’. Single and double points to be differentiated Compare with other side Tongue 1mm Lips-4 mm
- Digits like 1-9 , or shapes/symbols used. abnormal side done first and then normal side.
- (perception of one’s body and the relations of bodily parts to one another) Even when patients are told that the body part belongs to them, many will deny the reality and remain firm in their belief that it is not a part of them. It’s the lack of awarence or insight in pt to understand that suffered from any disease, refuse medication and trt. Shave only one side or use only one sleeve of shirt. Fail to use one side of body, even though paralysis is not present Denial and neglect - non-dominant parietal lesions.
- Parietal lobe is – “ Lobe of hand ”. Hand is extensively represented Parietal lobe gathers information regarding various objects through hand An example of bilateral asomatognosia and is due to lesion in left dominant. inferior parietal lobule (angular gyrus).
- with pt eyes closed, touch one of his fingers. Ask him to touch the same finger of examiner, with eyes open. Examiner places hand in some irregular position and asks pt – “ point to my middle finger”
- ex : show your left foot ex : with your right hand touch your left ear ex : point my right elbow ex : with your left hand point my right foot
- Lt parietal lesions – inability to understand and carry out numericals. Severe acalculia = Anarithmetria.
- Rt parietal lesions – inability to align numbers and to do complex computations (borrowing, carrying, etc). But, pt can do problems in his head.
- Defect - unable to show, but uses the object. – unable to do whole task, but does individual tasks.
- Constructional apraxia – visuospatial orientation,
- Inability to perform a single purposeful movement ( blowing a match ) ( flip a coin , comb hair ) ( stand like boxer )
- Inability to do complex motor planning of a higher sequence of order . ex: pt attempts to light a candle by striking it on matchbox
- high level non verbal cognitive function Parietal lobes are principle areas of visual – motor integration draw a clock with 10:20 time
- Dressing apraxia – form of sensory extinction and loss of extra personal space.