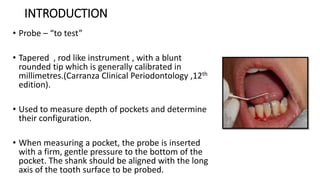
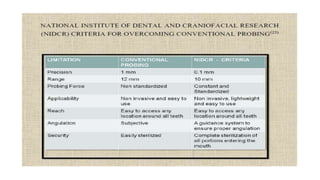
The document discusses the history and development of periodontal probes over several generations. It describes the key characteristics of 1st generation manual probes and 2nd generation pressure-sensitive probes. It then focuses on 3rd generation computer-assisted probes which standardize pressure and digitally record readings to reduce errors. Some examples provided are the Foster Miller Probe, Florida Probe, and True Pressure Sensitive probe. Overall the document traces the evolution of probes to become more precise, standardized, and integrated with digital systems.