

Recommended
More Related Content
What's hot
What's hot (19)
Viewers also liked
Viewers also liked (19)
Similar to Herpes Simplex RC
Similar to Herpes Simplex RC (20)
Recently uploaded
Recently uploaded (20)
Herpes Simplex RC
- 2. THE VIRUS Group: Group I (dsDNA) Order: Herpesvirales Family: Herpesviridae Subfamily: Alphaherpesvirinae Genus: Simplexvirus Species Herpes simplex virus 1 (HSV-1) Herpes simplex virus 2 (HSV-2)
- 3. The Virus Linear double stranded DNA molecule Enclosed in a regular icosahedral protein coat Lipid containing envelope covering it TEGUMENT: between layers
- 4. The Infection ● Step 1: Attachment ● Step 2: Entry into susceptible cells following attachment ● Step 3: Targeting of the virion to the site where it will reproduce ● Step 4: Uncoating of the virion— separation of protein coat from nucleic acid
- 5. The Infection ● Step 5: Synthesis of protein and replication ofStep 5: Synthesis of protein and replication of nucleic acidnucleic acid ● Step 6: Maturation of the viral particlesStep 6: Maturation of the viral particles ● Step 7: Cell lysisStep 7: Cell lysis ● Step 8: Spreading of the virusStep 8: Spreading of the virus within the hostwithin the host ● Step 9: Shedding of the infectious virions in salivaStep 9: Shedding of the infectious virions in saliva ● Step 10: Transmission to the next host, therebyStep 10: Transmission to the next host, thereby repeating the infectionrepeating the infection
- 6. The Dormancy ● Some viruses spread to axons ● Persist in latent stage in trigeminal ganglion ● Endogenous reactivation ● Viruses return to periphery ● Cause vesicular exanthem
- 7. The disease Virus Disease Mode of transmission Involved sites Herpes Simplex Virus 1 Stomatitis –CHILDREN ADULTS: gingivostomatitis, eczema,whitlow keratoconjunctivitis, esophagitis, pharyngotonsillitis, meningoencephalitis Infected saliva and oral and peri-oral lesions Pharynx, lips, eyes, skin above waist Herpes Simplex Virus 2 Herpes genitalis, neonatal herpes Sexual contact Genitalia, skin below waist
- 8. The Features – Herpetic gingivostomatitis ➢ Highly visible and acutely symptomatic primary infection ➢ Transmitted by droplet spreaddroplet spread or contact with lesions ➢ Age: Typically a childhood I infection seen between the ages of 2–4 years, but increasingly seen in the mouth and/or pharynx in older patients. ➢ Gender : M = F. ➢ Abrupt onset, with development of fever, irritability, headache, & pain on swallowing. ➢ Incubation period: 5 -20 days
- 9. The mucosal changes – Herpetic gingivostomatitis
- 10. The Features – Herpetic gingivostomatitis- Gingiva ● Distinctive punched out erosions along free gingival margins ● Enlarged, painful, erythematous gingiva
- 11. Recurrent oral Herpes Simplex Recurrent Herpes labialis AKA Cold Sores Recurrent Intra-oral Herpes Lips Palate/ maxillary gingiva/ lateral aspects of tongue
- 12. Histopathology : Epithelium ● The herpetic vesicle is an intra epithelial blister filled with fluid ● Infected cells are swollen with pale yellow eosinophilic cytoplasm and large nuclei ● AKA Ballooning Degeneration ● Acantholysis, Nuclear clearing, Nuclear Enlargement ● Cells are KA TZANCK CELLS
- 14. Histopathology :Epithelium : Alternate Pattern ● LIPSHUCTZ BODIES ● Eosiniphilic, ovoid, homogeneous structures within the nucleus. ● Displace nucleolus and chromatin peripherally ● C.T is infiltrated with inflammatory cells
- 15. Diagnosis - BIOPSY ● Excisional biopsy ● H/E ● Immunoflourescent stains
- 16. Diagnosis – Cytologic smear ● Puncturing an intact vesicle and expressing fluid on the slide ● Stained and examined for viral cytopathic effects ● Non specific for HSV
- 17. Diagnosis – Contd ● Culture ● Flourescent antibodies ● Serology ● Indirect tests
Editor's Notes
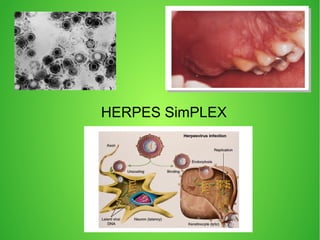
- Two basic types of herpes simplex infection. Lytic infections (right) commonly occur after endocytosis of herpes virus into keratinocyte. Replication and reassembly ensues that overwhelms host cell and causes it to burst, which releases large numbers of viruses. Latent infections (left) commonly occur in the cell body of neurons, where viral DNA remains dormant within the cytoplasm or nucleus until activated to replicate and migrate along a neural axis to an epithelial surface.
- HSV 1 and 2 genomes are antigenically related and similar HSV 2 is more neurovirulent and more resistant to antiviral drugs
- Capsid: 162 capsomeres Lipid envelope: derived from modified cell membrane Tegument: contains viral proteins
- PIC: only ENTRY of virus
- PIC: only RELEASE of virus Virus released via endoplasmic reticulum and golgi to cell surface (b) Electron micrograph of virus particles budding from the surface of a human cell. The virion on the left has completed the process.
- 3 rd point before : Pathogen remains permanently after primary infection subsides REACTIVATED BY PROLONED SUNLIGHT EXPOSURE, TRAUMA, FEVER, IMMUNOSUPPRESSION, STRESS AND ANXIETY Pathogen return via same route Exanthem = fever blisters
- Stomatitis = primary infection Top right – herpes stomatitis Bottom right – labialis [ vesicles ] Bottom left – gingivostomatitis
- Numerous pinhead yellow fluid-filled pinhead vesicles –COLLAPSE → small red lesions with an erythematous halo –ENLARGE → Central areas of ulceration covered by yellow fibrin –COALESCE → larger ulcers
- Recurrent infections occur at the site of inoculation or along distribution of the ganglion COLD SORES: occurs following upper respiratory tract infection Recurrent herpes labialis. A, Early stages consisting of fluid-filled viral vesicles. They ulcerate and resolve as B, Late stage demonstrating brownish crusted lesions. Intra oral Herpes: Punctate with red/ white bases that disappear
- Cells absorb fluid and swell
- Herpes simplex. Early and late stages of intraepithelial viral vesicle formation. A, Incipient vesicle formation early in prodromal stage before presence of a clinically visible vesicle exhibiting ballooning degeneration, nuclear margination, and multinucleation of the spinous layer of keratinocytes (viral cytopathic changes). B, Fully developed but intact intraepithelial viral vesicle that contains fluid, virally altered keratinocytes, large numbers of viruses, and necrotic debris. C, Photomicrograph of cytologic smear of viral vesicle contents that reveals enlarged and ballooned keratinocytes and associated leukocytes.
- SOME OTHER CELLS SHOW LIPSHCUTZ BODIES
- Diagnosis : based on cf IMMUNOSTAINS: use monoclonal abs to identify specific types and subtypes of Herpes.