Download to read offline
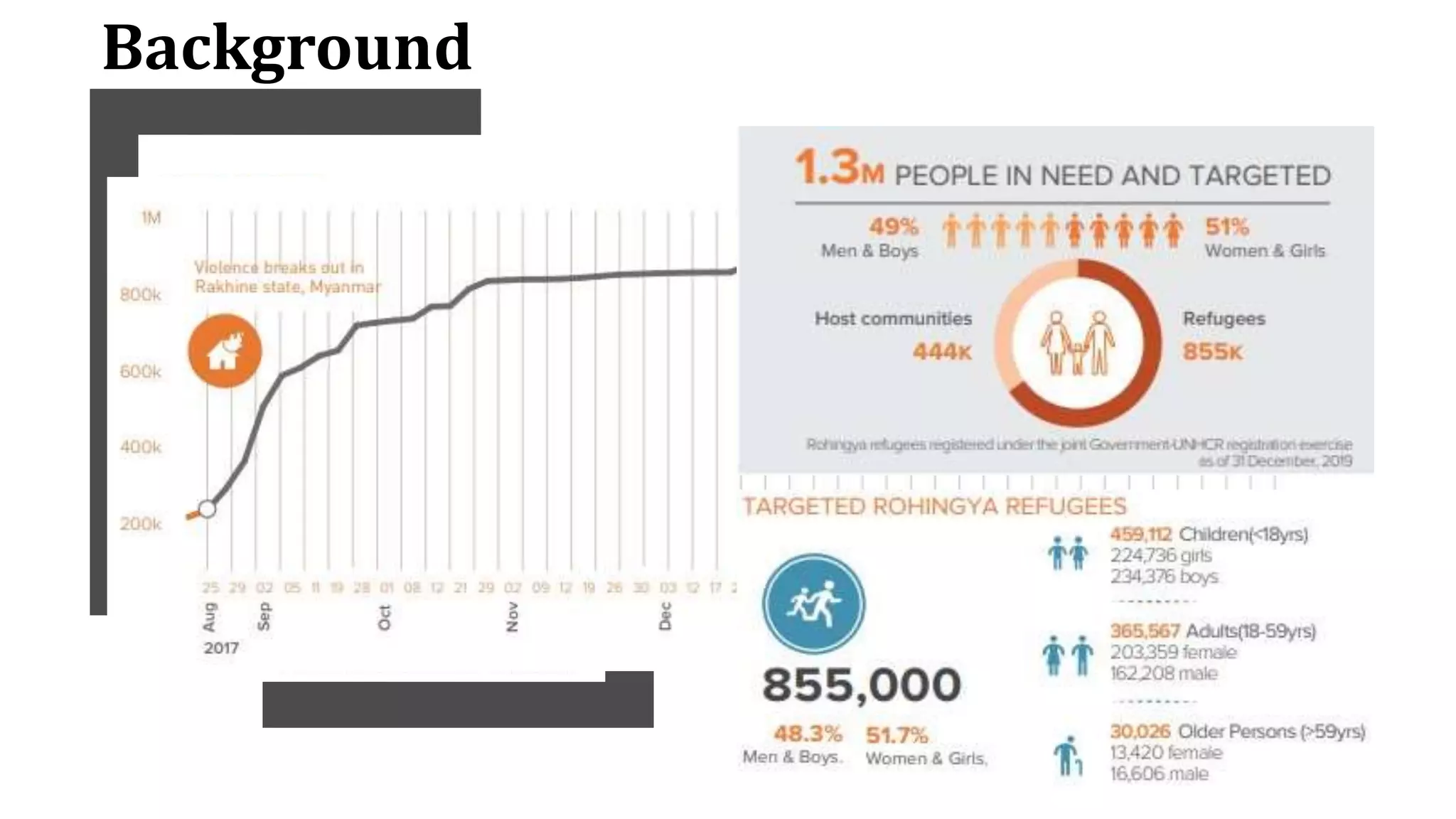
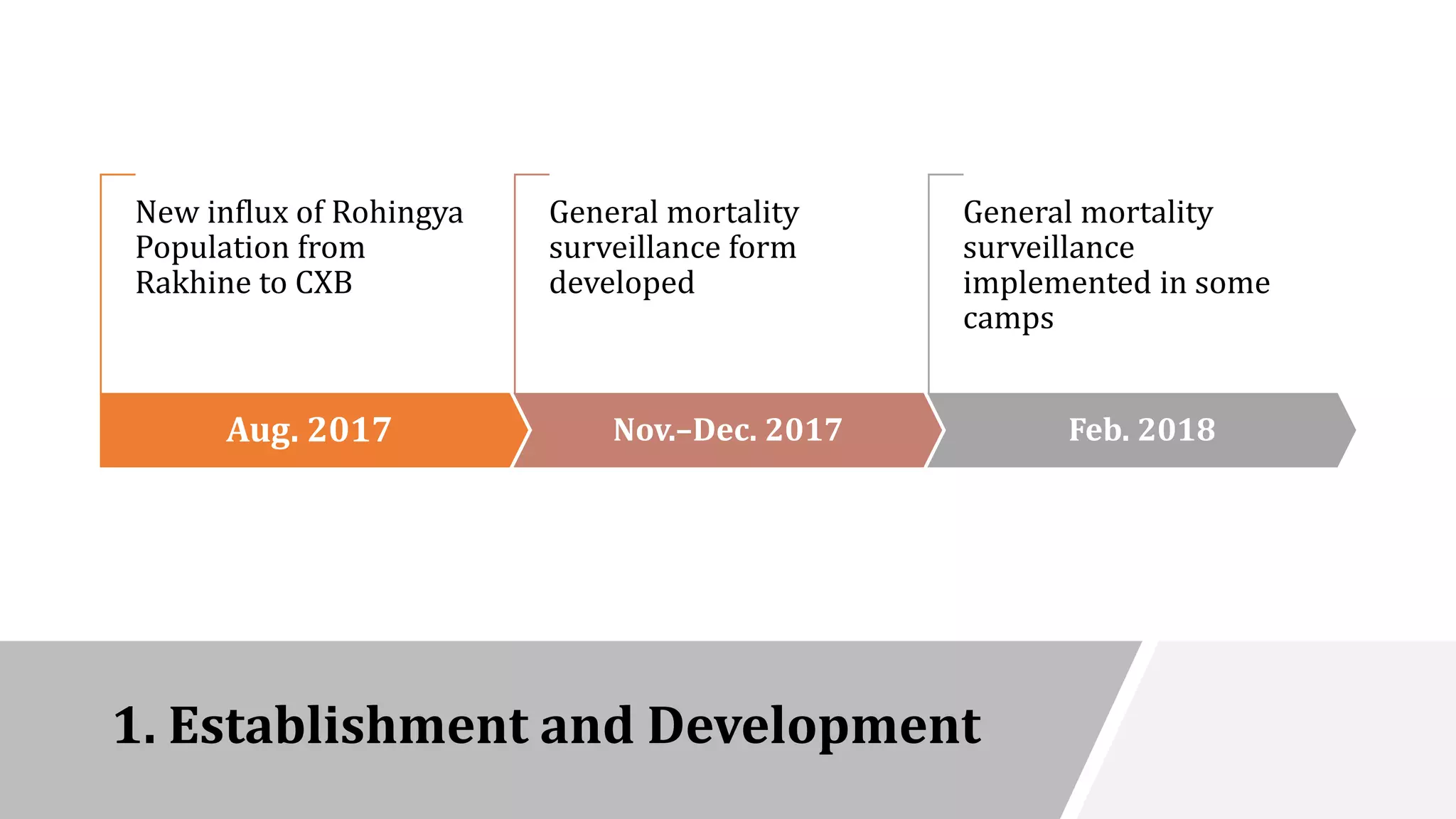
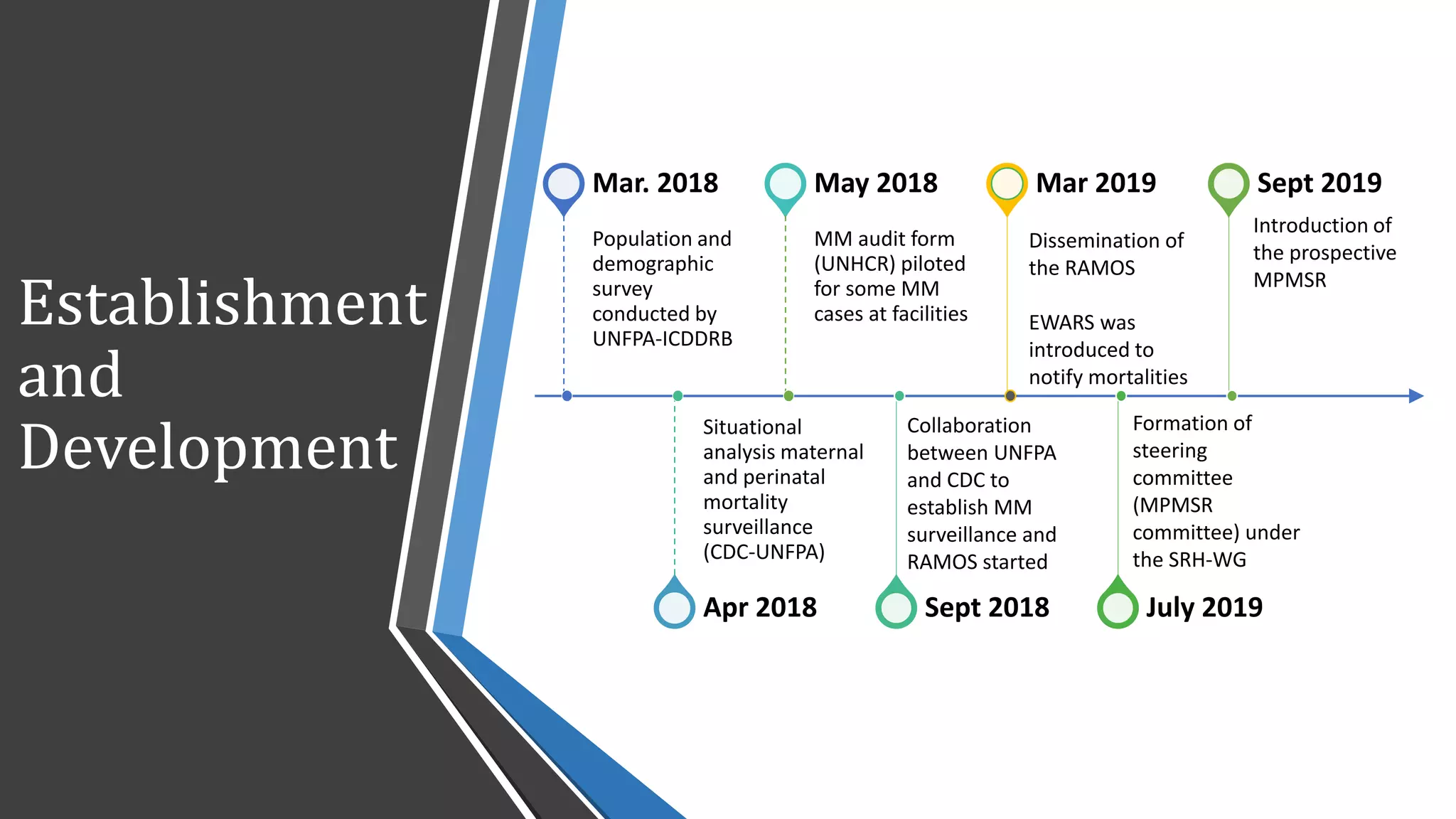
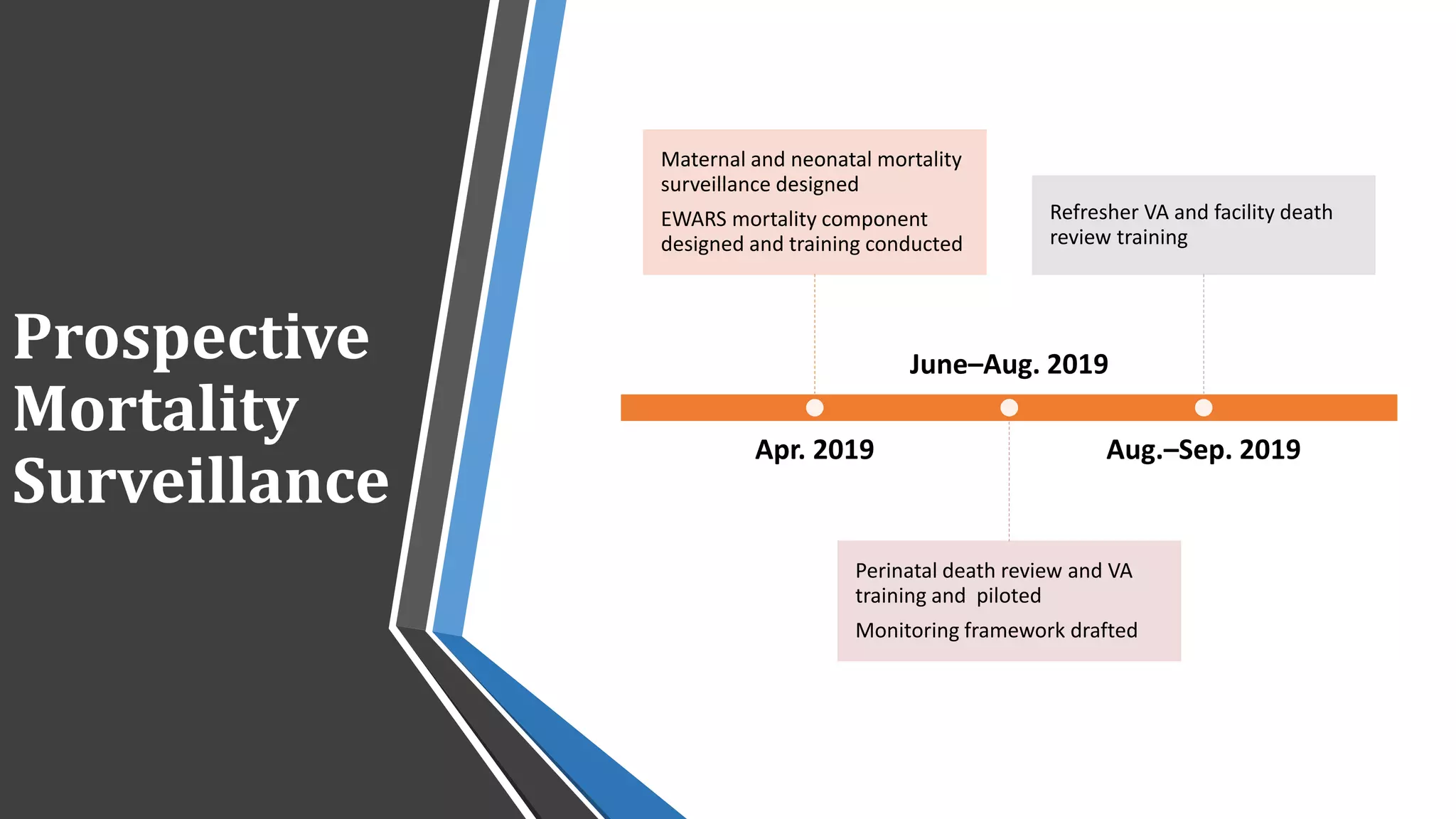
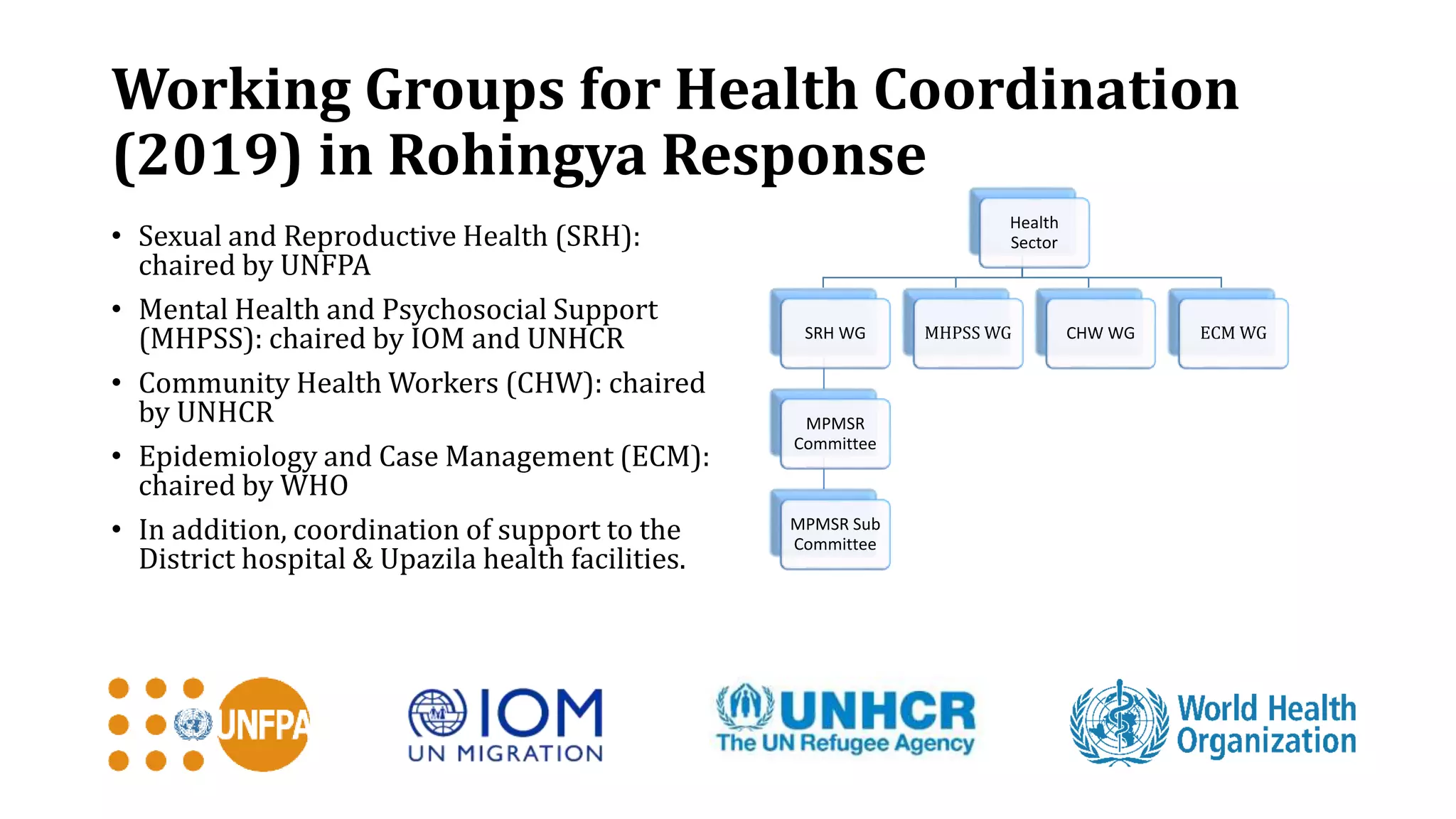
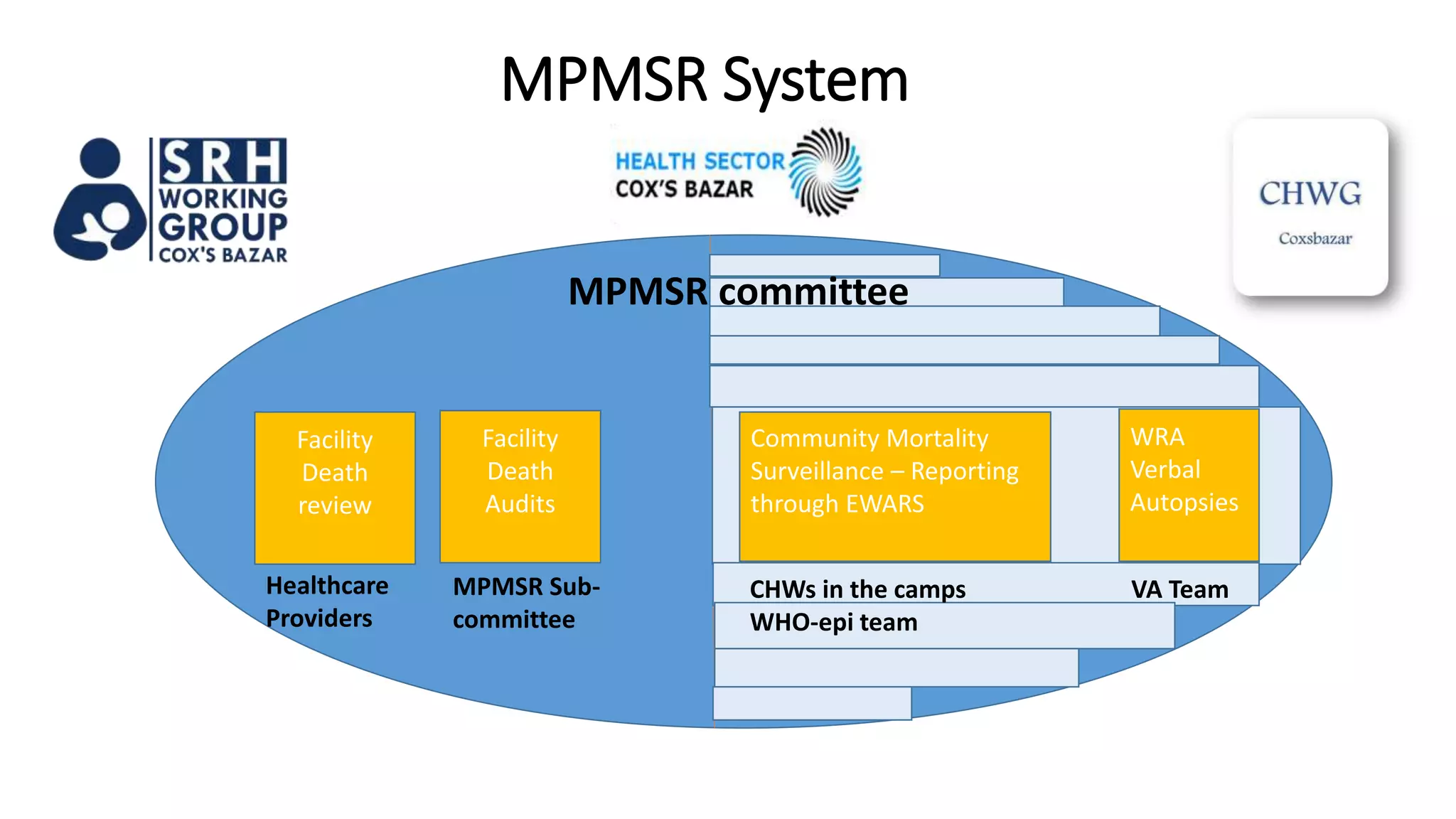
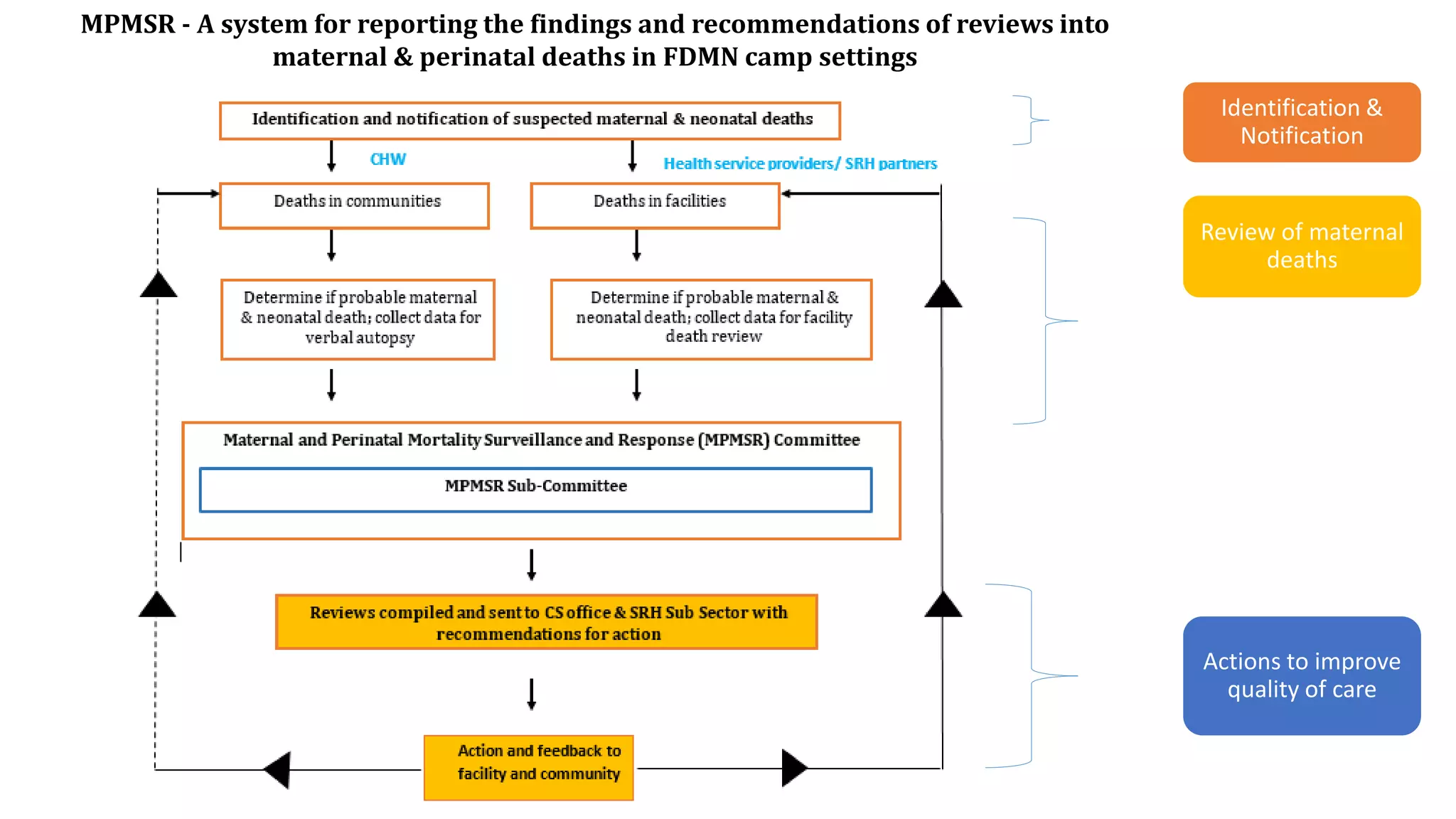
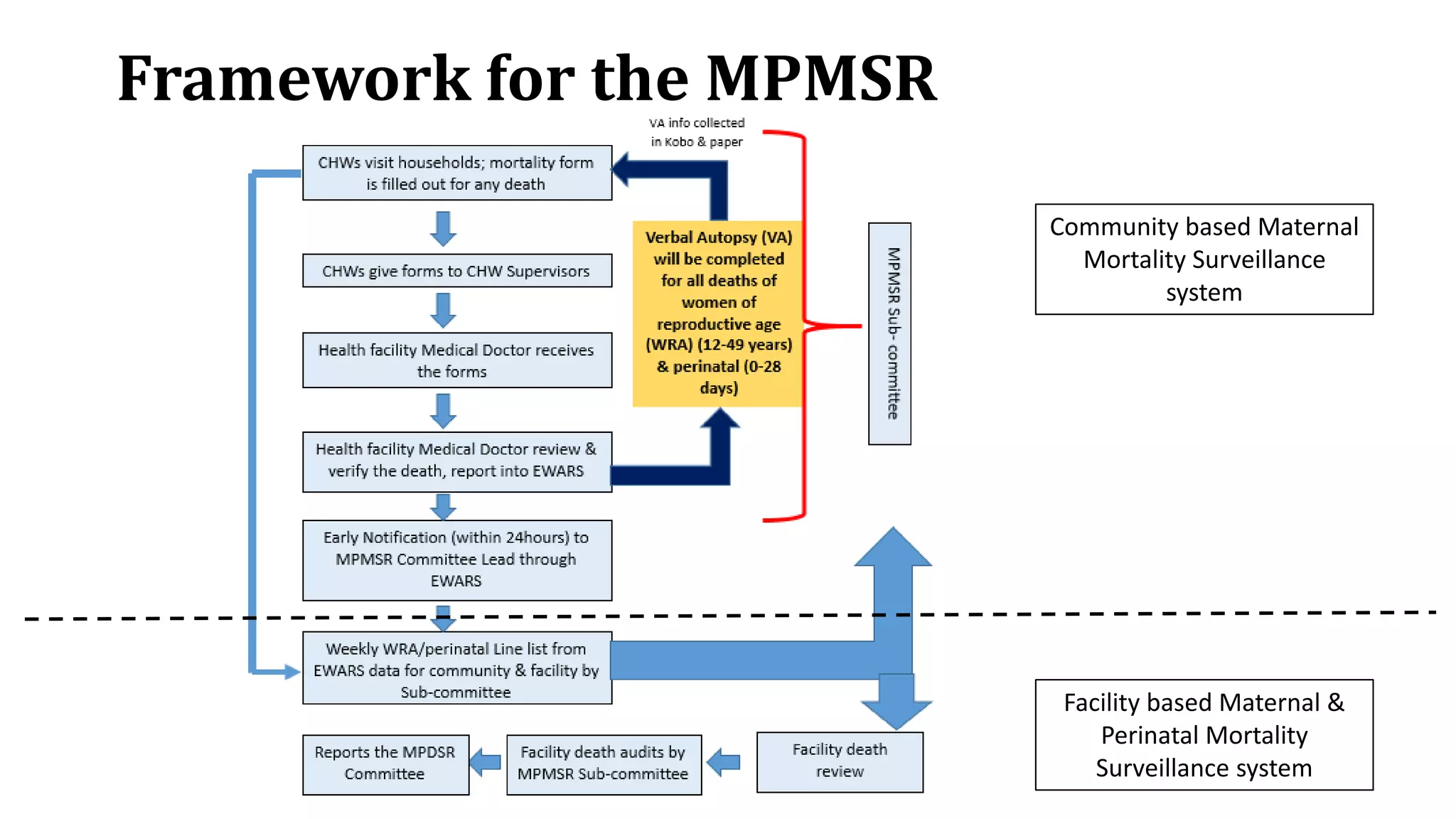
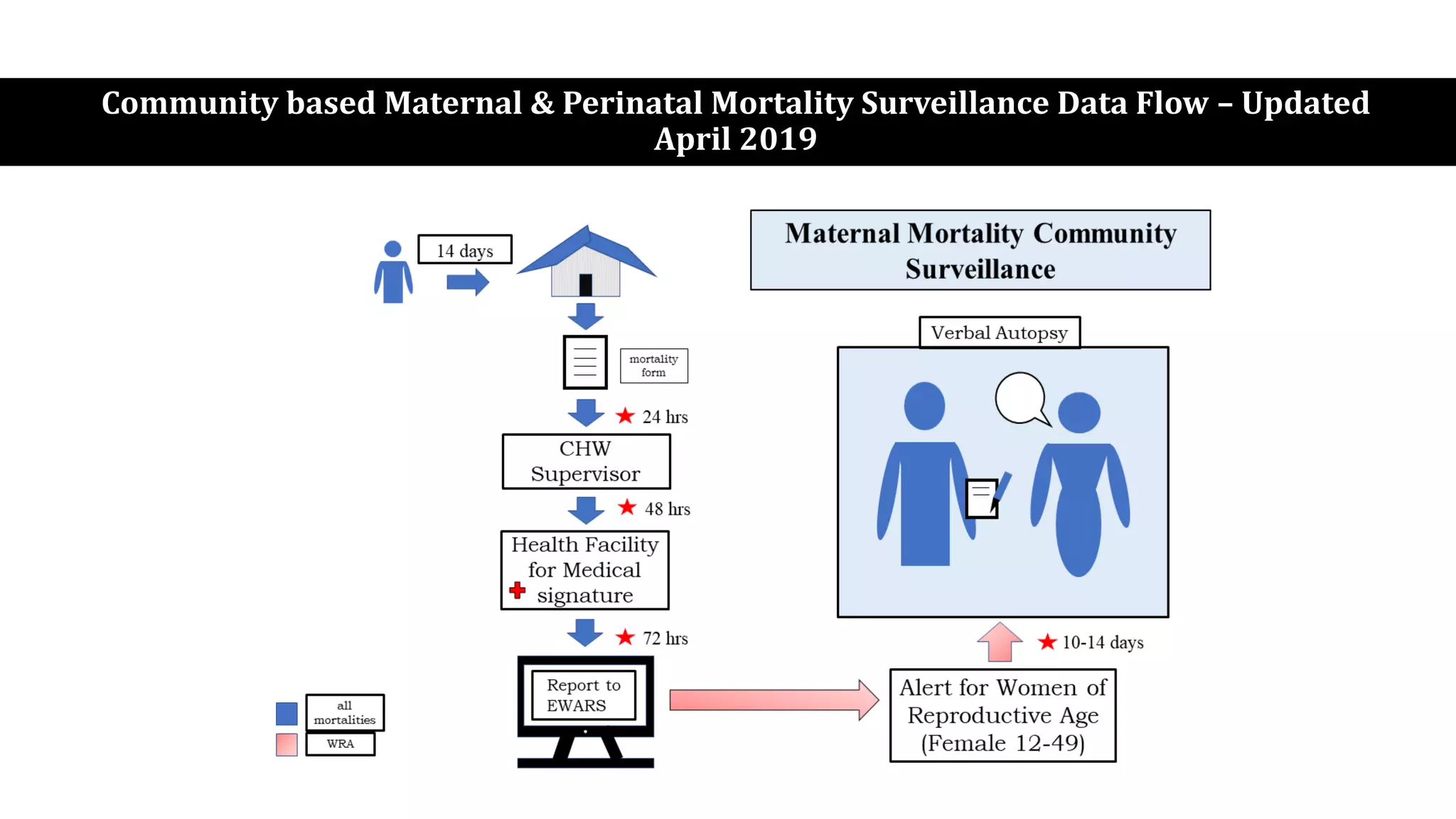
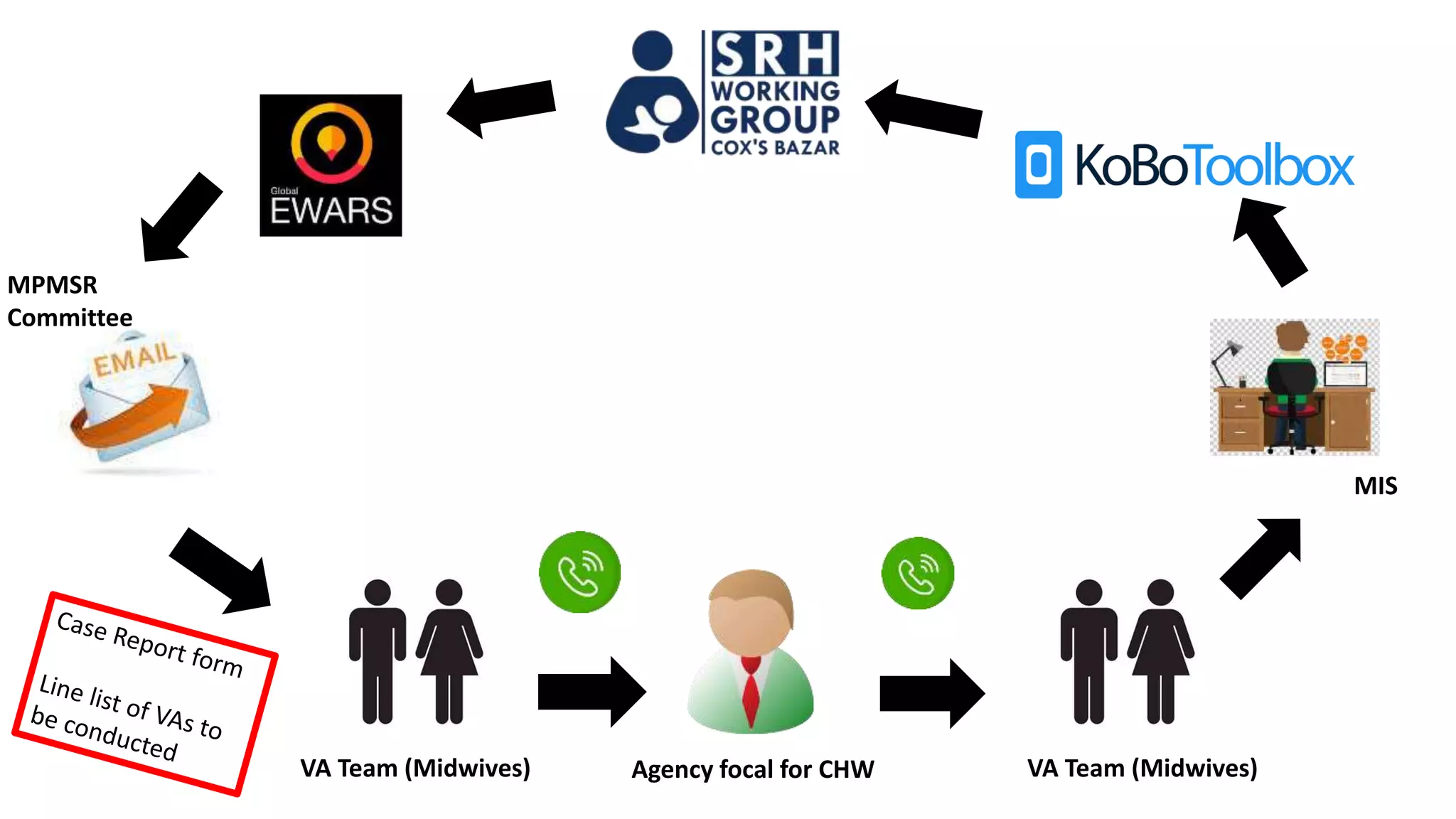
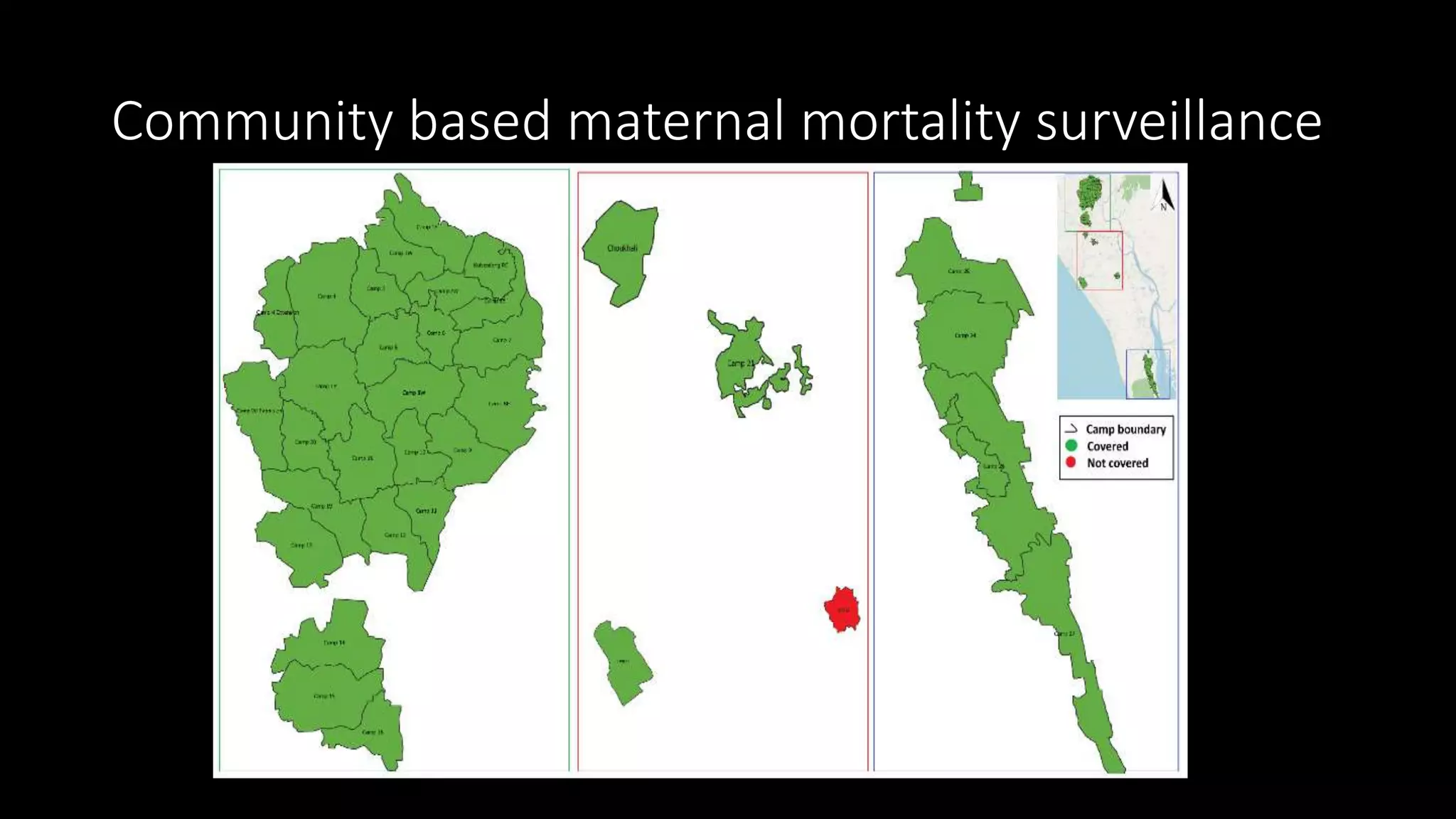


This case study explores the establishment and implementation of a maternal and perinatal mortality surveillance and response system (MPMSR) in the Rohingya refugee crisis, highlighting efforts by NGOs to improve public health infrastructure. Data collected through interviews and document reviews from 2017 to 2019 reveal the development process and challenges faced, including the need for better follow-up on recommendations and integration with existing national systems. Overall, the surveillance system is regarded as effective and is supported by a strong commitment from stakeholders.























































































